
Abstract
Objective
There was no study aimed at evaluating the effect of muscle function on SLE patients' quality of life using the Sarcopenia Quality of Life (SarQoL) questionnaire.
Methods
This cross-sectional study recruited 61 women with SLE consecutively, muscle function was measured with Jamar handheld-dynamometer and 6-meter walk test, HRQoL was measured with Sarcopenia Quality of Life (SarQoL) questionnaire. The cut-off point for low muscle strength (<18 kg) and low gait speed (<1.0 m/s) was according to the Asian Working Group on Sarcopenia 2019 criteria. Statistical analysis was conducted with a t-test for mean difference, and linear regression was used to adjust confounders (age, protein intake, physical exercise, and disease activity).
Results
The subjects' mean muscle strength was 19.54 kg (6.94), and 44.3% (n = 27) was found to have low muscle strength. The subjects' mean gait speed was 0.77 m/s (0.20), and 90.3% (n = 55) was found to have low gait speed. The difference of total SarQoL score in subjects with normal and low muscle strength was found to be significant; 74.86 (9.48) vs. 65.49 (15.51) (p = 0.009), and still statistically significant after adjustments with age, protein intake, physical exercise level, and disease activity [B 0.56; 95% CI 0.08–1.03; p = 0.022]. The difference of total SarQoL score in subjects with normal and low physical performance was found to be not significant, 70.67 (11.08) vs. 70.72 (13.56) (p = 0.993).
Conclusion
There was a significant difference in SarQoL's total score in normal compared with low muscle strength groups of Indonesian women with SLE.
Keywords
Introduction
Lupus mainly affects women of productive age, with the mean age of onset in Asia ranging from 25.7 to 34.5 years old. 1 The improvement in early diagnosis and medical management has resulted in increased survival, especially in rich countries where the ten-year survival rates could achieve 94%. 1 Unfortunately, this was not followed by improved functional status and quality of life; indeed, lupus subjects reported lower physical and emotional function compared with the general population. 2
Muscle function and mass disturbances, also known as sarcopenia, has been studied in the elderly population as an essential factor affecting health-related quality of life (HRQoL). 3 This process was shown not only affecting the elderly but also in younger population, 4 especially those with chronic underlying conditions, such as autoimmunity and cancer. 5 Indeed, several studies have shown lower muscle function in individuals with lupus, 6 , 7 and it was associated with lower quality of life and functional status. 8 , 9
Recently, to be able to specifically evaluated health-related quality of life in subjects with sarcopenia, a new HRQoL tool called SarQoL was developed and validated. 10 , 11 SarQoL was found to be better than generic HRQoL tools, such as SF-36, EQ5D, and EuroQoL, in evaluating and predicting changes in quality of life in relation to muscle function. 12 SarQol has been shown to give a better responsivity in 2 years observation than SF-36 (p = 0.005); EQ-5D (p < 0.001) and Euro-QoL (p = 0.003). Furthermore SarQoL also shown a correlation to gait speed (r = 0.50), SPPB (r = 0.47) and chair stand test (r = 0.42), whereas the other generic HRQoL tools does not. 12 Nevertheless, according to our knowledge, there was no study evaluating the impact of low muscle function in subjects with lupus. The present study was conducted to assess the frequency of low muscle function and its' impact on HRQoL, according to SarQoL, in Indonesian women with lupus.
Materials and methods
Patients and settings
A cross-sectional study was conducted in the outpatient clinic of the Allergy and Clinical Immunology Division, Cipto Mangunkusumo National Referral Hospital, Jakarta, in March 2020. The study was approved by the Medical Research Ethics Committee of the Faculty of Medicine of Universitas Indonesia, Jakarta. Subjects has been given an adequate explanation and agreed to participate in the research.
Consecutive patients with SLE were included in the study, and all patients met the Systemic Lupus International Collaborating Clinics (SLICC) criteria for the classification of SLE. We excluded patients with another autoimmune disease and anatomical dysfunction that disturbs with the measurement. The sample size was calculated considering an α of 0.05, power of 80%, and the mean SarQoL score of individuals with sarcopenia (X1 67.8), an effect size of 8.5 and standard deviation of 8.5, a sample size of 32 patients was estimated.
Data collection and assessment
The data obtained from the interview include age; age at the moment of diagnosis; body mass index; muscle mass measurements using Tanita MC-780 MAP Body Impedance Analysis; SLE activity index using MEX-SLEDAI; Numerical Rating Scale for Pain; the medication used; International Physical Activity Questionnaire for weekly physical exercise; protein intake using three days Food Record; and functional status using Activity of Daily Living Questionnaire.
Determination of muscle strength was done by calibrated Jamar handheld dynamometer, 13 and physical performance by 6-meter gait speed test 14 as described elsewhere. Low muscle strength was defined as handheld dynamometer measurement of ≤18 kg. Low gait speed was defined as 6-meter walking speed ≤1.0 meter/second (Asian Working Group on Sarcopenia 2019). 15 HRQoL measurements were conducted using the SarQoL questionnaire validated before 11 and then formally translated into the Indonesian language (data on file).
Statistical analysis
Analysis was done using SPSS 20.0 (SPSS Inc., Chicago, IL, USA). Mean difference analysis was done using the t-test to evaluate muscle strength and gait speed relation to SarQoL total score. Multivariate analysis by linear regression was done to adjust with confounders: age (less or more than 40 years old), protein intake (more or less than 0.8 g/kg BW daily), activity level (more or less than 350 minutes of physical exercise weekly, IPAQ) and disease activity (mild-moderate or severe, MEX-SLEDAI). P-value cut-off of <0.25 was used as the threshold for multivariate analysis. Analysis of muscle function and the components of SarQoL (7 areas) was done with the t-test for further exploration and helped with results explanation. Any p-values < 0.05 were considered significant.
Results
We recruited 61 subjects consecutively; two subjects were excluded because of anatomical abnormalities, six subjects refused to participate because of time constraints. Regarding weekly physical activities, it was found that 45.9% (n = 28) subjects did not participate at all in the last week. Low appendicular muscle mass index [appendicular muscle mass (kg)/height (m) 2 ] was only found in 4.9% of subjects (n = 3). Most of the subjects had deficient vitamin D levels [25(OH)D < 20 ng/ml] (77.1%; n = 47) and only 6.6% (n = 4) of subjects had sufficient levels [25(OH)D > 30 ng/ml].
Musculoskeletal involvement was found on 78.6% of subjects (n = 48) and 36.1% of them (n = 22) reported moderate-severe pain (VAS >4). Muscular pain was found on 34.4% of subjects (n = 21), but no subjects reported increased creatine kinase enzymes. Lupus nephritis was found on 22% of subjects (n = 14) and severe kidney function (eGFR < 30 ml/1.73m3) affected 4.4% of subjects (n = 2). Most subjects were diagnosed with SLE less than five years (54.1%; n = 33) and classified as having moderate lupus activity (MEX SLEDAI 2–5; 47.5%; n = 29). Routine corticosteroid usage in the last month was found on 83.6% of subjects (n = 51), and most of them use low dose corticosteroid (<7.5 mg prednisone daily; 67.2%; n = 41). Detailed demographic, anthropometric, nutrition, and clinical characteristics could be seen in Table 1.
Relevant characteristics of study subjects.
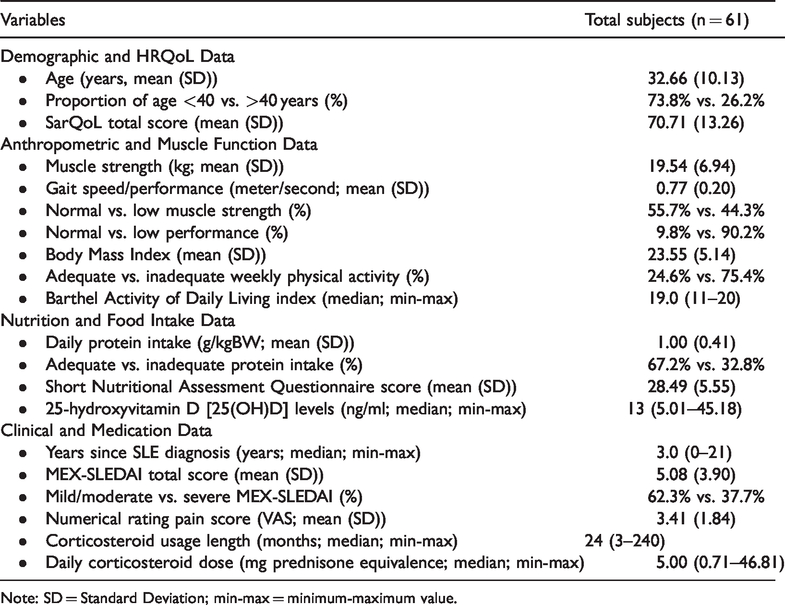
Note: SD = Standard Deviation; min-max = minimum-maximum value.
Table 2 described the analysis of the relationship between muscle function and the SarQoL total score. After adjusting to age, MEX-SLEDAI score, protein intake adequacy, and physical activity variables, muscle strength was independently associated with SarQoL total score [B 0.56; 95% CI 0.23–1.03; p = .022]. Colinearity analysis did not found any significant interaction between variables in multivariate analysis. The final linear regression model showed crude R2 of 0.175, adjusted R2 of 0.101, and R2 change of 0.175 (p = 0.054). SarQoL's components analysis, according to muscle strength grouping, could be seen in Table 3. Table 4 gives a comparison of relevant characteristics between normal and low muscle strength groups.
Analysis of muscle function and mean SarQoL total score.

Bolded values denotes a significant result (p-value <0.05).
SarQoL components analysis according to muscle strength.
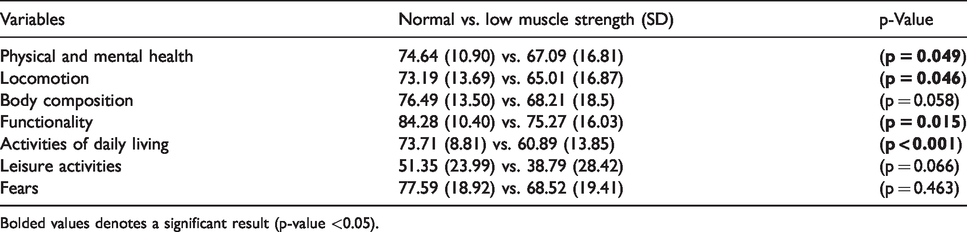
Bolded values denotes a significant result (p-value <0.05).
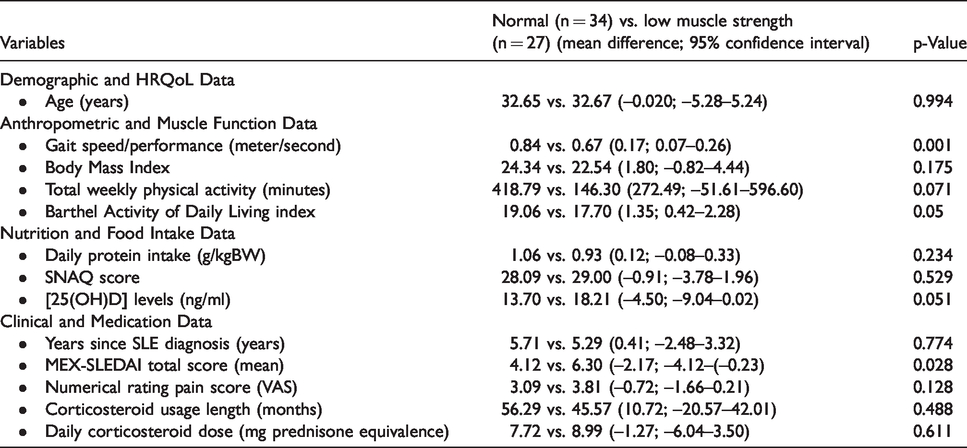
Comparison of subjects with normal and low muscle strength.
Discussion
Our SLE subjects showed a mean age of 32.66 (10.126) years, and most had SLE less than five years (54.1%). This result was generally consistent with other SLE populations in Asia, that generally had a younger age and shorter SLE duration. 1 Musculoskeletal involvement was found in 78.6% of subjects and moderate-severe pain (VAS < 4) in 36.1% of subjects, again generally consistent with regional 1 and local data. 16 Clinical activity according to MEX-SLEDAI (mean 5.08, SD 3.9) was generally lower than other local data in another center, although they used SLEDAI descriptor for the assessment (median 7; min−max 0−14). 16
Measurements of muscle function in our subjects resulted in generally low muscle strength (mean 19.54 kg; SD 6.94) and physical performance (gait speed mean 0.77 m/s; SD 0.20). Currently, there was no data regarding muscle strength and physical performance normal range in Indonesian young adults. Data from neighboring countries showed a higher muscle strength in Chinese (median 28 kg) and Malays (median 23 kg) of comparable age and gender. 17 There was no data regarding normal gait speed values in Asian young adults; Bohannon et al. 14 data on young Caucasian women revealed a normal gait speed range of 1.39−1.46 m/s. Though no normal data in Indonesia, we could safely assume that our subjects' low muscle strength and physical performance are clinically significant. Data from studies in healthy elderly (>60 years old) Indonesian woman in the community revealed mean muscle strength of 19.8 kg (5.1) 18 and median gait speed of 0.84 m/s (min−max 0.18−2.0). 19
Low muscle function that appears in our study subjects warrants further evaluation. Andrews et al., 8 in a study of 146 women with SLE, have shown that dysfunction in muscle strength was related to a further decrease in physical function in 2 years. They showed that every 10 N-m reductions of peak knee flex torsion were correlated with a 0.84 point reduction of short physical performance battery (SPPB) score. 8 This association remains significant, even after adjusting to covariates such as age, length of SLE diagnosis, SLE activity, physical activity, steroid use, body composition, and depression. Furthermore, Andrews et al. 8 also shown that the impact of low muscle strength and future physical dysfunction was strongest in the weakest individuals. Indeed, in our study, we found that only disease activity (SLEDAI score mean 4.12 vs. 6.30 (−2.17; −4.12-(−0.23)); p = 0.029) might contribute to low muscle function; this warrants further longitudinal study to evaluate the longterm relationship between these variables in our population.
Evaluating physical performance using gait speed is a convenient and reliable way to evaluate individuals' complex systems because gait speed resulted from the complex interaction of muscle, neuro-cognitive, balance and cardio-respiratory, and personal habits exercise routines. 14 There was only one other study that evaluates gait speed in SLE subjects; Fernandes et al. 20 compared 33 SLE subjects with 26 healthy control, they found that women with SLE have lower gait speed than the healthy control. They also found higher percentages of subjects with low gait speed (<0.8 m/s) in the SLE groups (57.7%) than the healthy control groups (38.5%). The higher proportion of our study subjects with low gait speed could be caused by the higher cut-off points recommended by the AWGS 2019 guidelines. This warrants further study to evaluate the appropriate cut-off for low gait speed in the SLE population, as low gait-speed has been proven as a predictor of survival, where a meta-analysis of 34,485 elderly subjects has shown an improved rate of survival with every 0.1 m/s gait speed increment. 21 Furthermore, our study also showed that individuals with low muscle strength also had a significantly lower gait speed compared to normal muscle strength (0.84 vs. 0.67 (0.17; 0.07–0.26); p = 0.001).
Subjects with low muscle strength in our study were shown to have a lower total SarQoL score [65.49 (15.51) vs. 74.86 (9.48)], which still significant after adjustment with confounders such as low protein intake and inadequate physical activity (p=.022). There was no difference in total SarQoL score in subjects with low gait speed than normal, although this might be because of general lack of fitness in SLE subjects compared to healthy young adult 22 or higher cut-off points recommended by the AWGS 2019 guidelines. 15 These make it difficult to conclude the relationship between gait speed and total SarQoL score in our subjects, and further research is needed to compare the relative fitness of our SLE patients compared to healthy young adults and to determine the population cut-off points in gait speed.
There was no other study, according to our knowledge, that evaluates the SarQoL total score in SLE subjects with low muscle function. Several studies showed that low muscle strength was consistently related to lower quality of life (SF-36), 9 life satisfaction (value-added activity, VLA), 9 fatigue, 23 and depression 6 in SLE subjects. Improvement of quality of life in SLE subjects with low muscle function through physical exercise and nutritional intervention, although promising, still marred with several limitations, such as small sample size, no reasonable control, contradictive results, short monitoring time, and unspecific health-related quality of life tools used.24–26 These difficulties highlighted the need for specific HRQoL tools in diagnosing, evaluating, and monitoring SLE subjects' therapeutic intervention with low muscle function. Indeed, through validation 11 and longitudinal responsiveness study, 12 using SarQoL as a tool to evaluate individuals with low muscle function and mass (sarcopenia) has been proven to be more reliable, consistent, and responsive than generic questionnaire (SF-36, EQ5D, and EuroQoL).
Furthermore, analysis of low muscle strength relation with specific SarQoL components in our study subjects revealed a consistent description of the relationship between physical strength, locomotion, functionality, and activities of daily living (Tables 3 and 4). Suppose we see the construct of the SarQoL questionnaire. In that case, we will see a coherent step between components of muscle function (i.e., upper or lower body strength), performance (i.e., walking speed, time, and distance), subsequent integration to the more complex activities (i.e., exercise, shopping, household tasks) and complications of low muscle function (i.e., falls, loss of flexibility and physical capacity). 10 SarQoL also is shown to be more sensitive in the change of muscle function than muscle mass, 27 a feature of muscle disturbances in subjects with SLE as shown by Andrews et al. 9 and also with the low prevalence of low muscle mass in our study (4.9%; n = 3) despite the high numbers of low muscle function.
Based on these findings, we argued that SarQoL could be used to evaluate, diagnose, and monitor intervention results in SLE patients with low muscle function. The use of SarQoL in SLE subjects with low muscle function could help eliminate inconsistencies and difficulties in evaluating intervention in future research. We acknowledge that there are several limitations of this study that need further research, especially to answer several important questions, such as the cut-off points and factors related to the development of low muscle function in subjects with SLE, especially in individuals with lupus nephritis and severe renal dysfunction. The inclusion of healthy subjects as control could also provide us with crucial clinical comparison. We also need longitudinal validation of SarQoL to evaluate changes in muscle function and HRQoL over time, and finally, an intervention study to evaluate whether a medical, physical, and nutritional intervention will improve muscle function and HRQoL in SLE.
Conclusions
We found there was a significant difference in SarQoL's total score of female Indonesian SLE subjects with normal compared to low muscle function. There was no difference in SarQoL's total score according to the subject's physical performance, but this was probably due to SLE's subjects' general lack of fitness or inappropriate cut-off points for our population. The SarQoL questionnaire showed promise to be used in SLE subjects, with similar characteristics as our study subjects, as evaluation tools and also intervention target, but further research is needed to evaluate SarQoL performance over time and to prove whether improving muscle function will lead to better HRQoL of SLE subjects in a consistent manner.
Footnotes
Disclaimer
The views represented in this article are the authors' point of view and not the institution's official position and funder.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article: This research was partially funded by a research grant provided by Universitas Indonesia.