
Abstract
Objective
To investigate the mechanism underlying systemic lupus erythematosus (SLE)-related bone loss by evaluating the bone mineral density (BMD) and bone turnover markers (BTMs) in premenopausal patients with new-onset SLE without any treatment.
Methods
BMD and BTMs of 106 premenopausal patients with new-onset SLE and 64 gender-, age- and body mass index (BMI)-matched healthy controls were analyzed. BMD was determined using dual energy X-ray absorptiometry (DXA). Serum BTMs were measured.
Results
Hip and lumbar spine BMD in premenopausal patients with new-onset SLE was significantly decreased compared with healthy controls. Higher rate of osteoporosis was observed in new-onset SLE patients (25% vs. 1%). Moreover, uncoupled bone remodeling evidenced by an increase in bone resorption marker β-CTX (685.9 ± 709.6 pg/mL vs. 395.4 ± 326.0 pg/mL, P < 0.05) and decrease in bone formation markers PINP (37.4 ± 33.0 ng/mL vs. 46.1 ± 20.9 ng/mL, P < 0.05) and OC (11.4 ± 9.8 ng/mL vs. 18.2 ± 8.6 ng/mL, P < 0.05) was observed in premenopausal patients with new-onset SLE compared with healthy controls. Univariate correlation analyses showed negative correlations between OC and SLE Disease Activity Index (SLEDAI), and positive correlations between β-CTX and SLEDAI. SLE patients positive for dsDNA, nucleosome showed lower OC and higher β-CTX.
Conclusion
Premenopausal patients with new-onset SLE had decreased BMD and abnormal bone metabolism with increased β-CTX and decreased OC and P1NP levels, indicating uncoupled bone remodeling in new-onset SLE patients. Disease activity and abnormal immunity, especially the amount of antibodies in SLE patients, were strongly associated with abnormality of bone metabolism.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease involving multiple organs and systems with high incidence in patients of child-bearing age. 1 The outcome of SLE patients has improved with 5-year survival rates up to 95% with increased treatment level. 2 Therefore, focus has increased on complications that develop as the survival time extends which increases the rate of disability and decreases the quality of life in SLE patients. 3
Osteoporosis is a common complication of SLE and has a negative effect on the long-term prognosis and quality of life in SLE patients. The incidence rate of osteopenia and osteoporosis in patients with SLE were reportedly 25–74% and 1.4–68%, respectively. 4 Furthermore, approximately 29% of SLE patients suffer at least one fracture in their life, which is higher than healthy controls of equal age. 5 Various factors contribute to bone loss in SLE patients. First, age, body mass index (BMI), and menolipsis are traditional factors that contribute to bone loss in SLE patients similar to primary osteoporosis patients. 6 Second, glucocorticoid (GC) treatment is associated with the development of osteoporosis in SLE because GCs reduce the proliferation, differentiation, and function of osteoblasts leading to bone loss in SLE patients. 7 Jardinet et al. 8 found that premenopausal SLE patients showed lower bone mineral density (BMD) and more than 7 mg per day of GC use aggravated bone loss in premenopausal SLE patients. Third, chronic inflammation, renal injury, avoidance of sun light, combined with joint and muscle dysfunction caused by SLE, are associated with bone loss in SLE patients.
Bone homeostasis is based on balanced bone remodeling and comprises bone formation and bone resorption. The biochemical markers of bone formation and bone resorption are important in understanding the pathophysiologic basis for bone metabolic diseases. 9 Assessing bone turnover may add valuable information for the management of patients with lower BMD and prediction of fracture risk. The non-collagen protein osteocalcin (OC) and precursor molecules of collagen I, amino-terminal propeptide of type I procollagen (PINP), which are produced by osteoblasts during osteogenesis, are commonly used to assess osteoblastic activity. Osteoclasts dissolve bone matrix by secreting proteolytic enzymes and then produce β-carboxy-terminal cross-linking telopeptide of type I collagen (β-CTX), which is also used to evaluate the activity of osteoclasts. 10 Excessive bone resorption and an inadequate formation response to increased resorption during bone remodeling both result in decreased bone mass and microarchitectural deterioration of the skeleton. Whether decreased bone mass is primarily due to increased bone resorption or decreased bone formation remains unknown, especially in secondary osteoporosis found in inflammatory disease.
In the present study, BMD and bone turnover markers (BTMs) were investigated in premenopausal patients with new-onset SLE who did not receive GC treatment. In addition, the risk factors contributing to the bone loss and disrupted bone homeostasis in premenopausal patients with new-onset SLE were analyzed.
Methods
Patients and healthy controls
The present study included 106 premenopausal patients with new-onset SLE recruited from the Department of Rheumatology and Immunology of the First Affiliated Hospital at Xi’an Jiao Tong University from September 2016 to September 2018. All patients were diagnosed based on the 1997 American College of Rheumatology criteria for SLE. The exclusion criteria included creatinine clearance rate < 60 mL/min, pregnancy, suffering from severe heart disease, or pulmonary dysfunction. Premenopausal status was confirmed based on the presence of menstrual cycles or premenopausal levels of gonadotropins. SLE patients who had symptoms associated with SLE for < 6 months without any treatment were defined as new-onset SLE patients. Clinical parameters of SLE patients were collected, including height, weight, BMI, inflammatory index, and patient disease activity, which was assessed using SLE Disease Activity Index (SLEDAI). In addition, 64 healthy controls with matched demographic features were recruited for the study. All participants were Han Chinese, which is a predominant ethnic population in China. Percentage of 106 patients who take the BTMs and BMD test in spring were as 40%, in summer 17%, in autumn 22% and in winter 21%. Moreover, more than 90% patients come from Shaanxi Province from 31 to 39 degrees north latitude. All participants read and signed the informed consent.
BMD and BTMs
BMD (g/cm2) of lumbar spine (vertebrae L1–L4) and left hip (total hip and femoral neck) were measured using dual energy X-ray with the same equipment (DEXA, DMS, France). Z-score represented the comparison of patients with the age-matched population. According to World Health Organization (WHO), osteoporosis in premenopausal patients was identified as Z-score ≤-2 and osteopenia as Z < −1 but > −2.
Serum levels of BTMs including OC, PINP, β-CTX, 25-hydroxy vitamin D (25(OH)D), and parathormone (PTH) were measured. Fasting blood samples were collected between 8 a.m. and 10 a.m. and assayed for serum 25(OH)D using mass spectrometry, PTH using Immulite 2000, and PINP and β-CTX using electrochemiluminescence immunoassays (Elecsys 1010 Analytics, Roche Diagnostics, Germany), with coefficient of variation (CV) of 3–8%. The normal premenopausal ranges for PTH is 15–65 pg/ml, 25(OH)D > 20 ng/ml, OC 11–43 ng/ml, PINP 15–58 ng/ml, β-CTX ≤573 pg/ml.
Statistical analysis
Values were expressed as mean ± standard deviation (SD). The differences in BTMs between patients and healthy controls were analyzed using the independent sample t-test. Pearson correlation was used to calculate the correlation between BMD, BTMs, and related clinical parameters. P-values < 0.05 were considered statistically significant. All statistical analyses were performed using the IBM SPSS 23.0 statistical software.
Results
Characteristics of recruited SLE patients
The present study included 106 premenopausal patients with new-onset SLE. Characteristics of all premenopausal SLE patients, including age, BMI, and SLEDAI are shown in Table 1. The mean age of premenopausal patients with new-onset SLE was 31 ± 8 years and the mean BMI was 20.6 ± 3.3 kg/m2. In addition, 64 demographic feature-matched healthy controls were recruited (mean age 32 ± 6 years, mean BMI 21.5 ± 2.6 kg/m2).
Characteristics of recruited new-onset SLE patients.
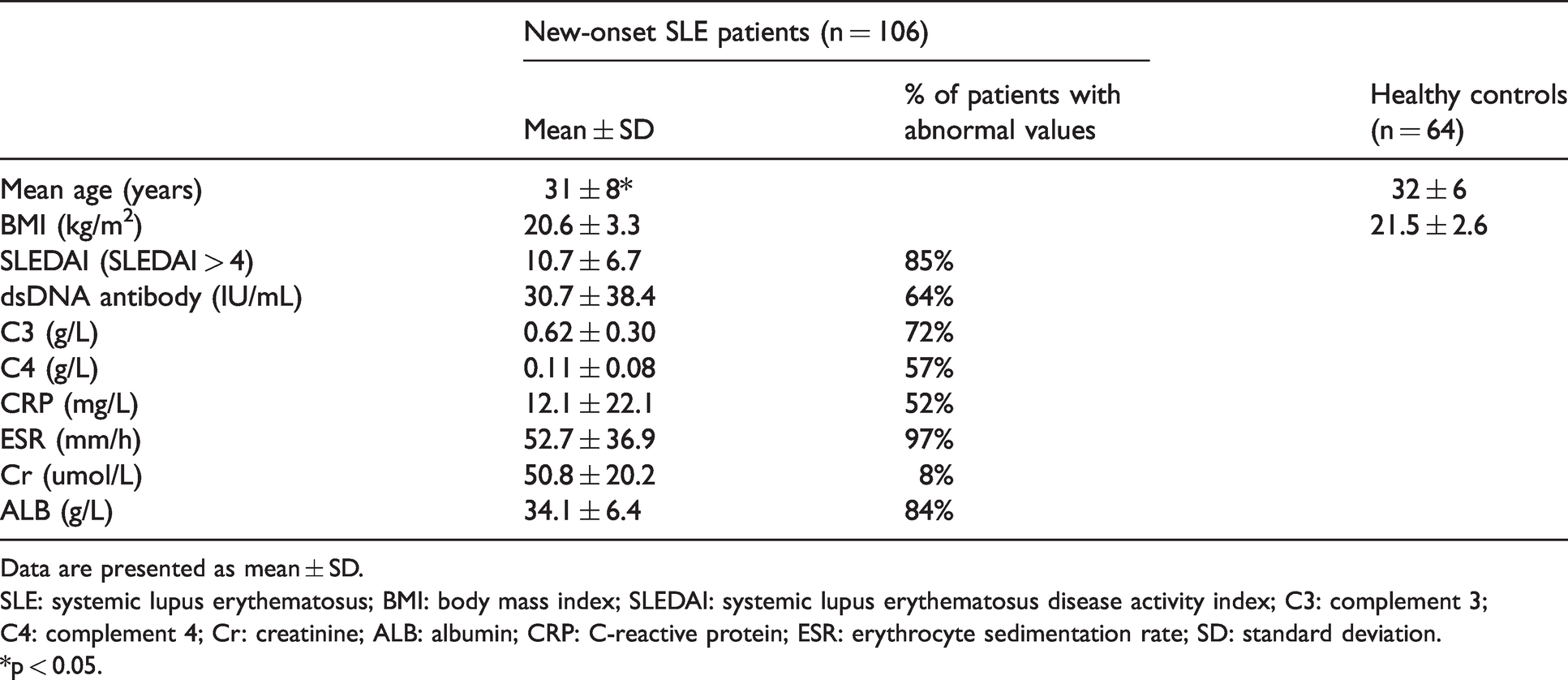
Data are presented as mean ± SD.
SLE: systemic lupus erythematosus; BMI: body mass index; SLEDAI: systemic lupus erythematosus disease activity index; C3: complement 3; C4: complement 4; Cr: creatinine; ALB: albumin; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; SD: standard deviation.
*p < 0.05.
Comparison of BMD and BTMs between premenopausal patients with new-onset SLE and healthy controls
The rate of osteoporosis in the recruited 106 premenopausal patients with new-onset SLE was 25%, which was significantly higher than in healthy controls (1%) (Table 2). None of the patients had osteomalacia. Notably, abnormalities were also observed in BMD and BTMs in premenopausal patients with new-onset SLE who received no treatment. A significant decrease was observed in hip BMD (0.871 ± 0.140 g/cm2 vs. 0.940 ± 0.114 g/cm2, P < 0.05) and lumbar spine BMD (0.861 ± 0.151 g/cm2 vs. 0.941 ± 0.099 g/cm2, P < 0.01) of premenopausal patients with new-onset SLE who did not receive GC treatment compared with healthy controls.
Comparison of BMD and BTMs between premenopausal patients with new-onset SLE and healthy controls.
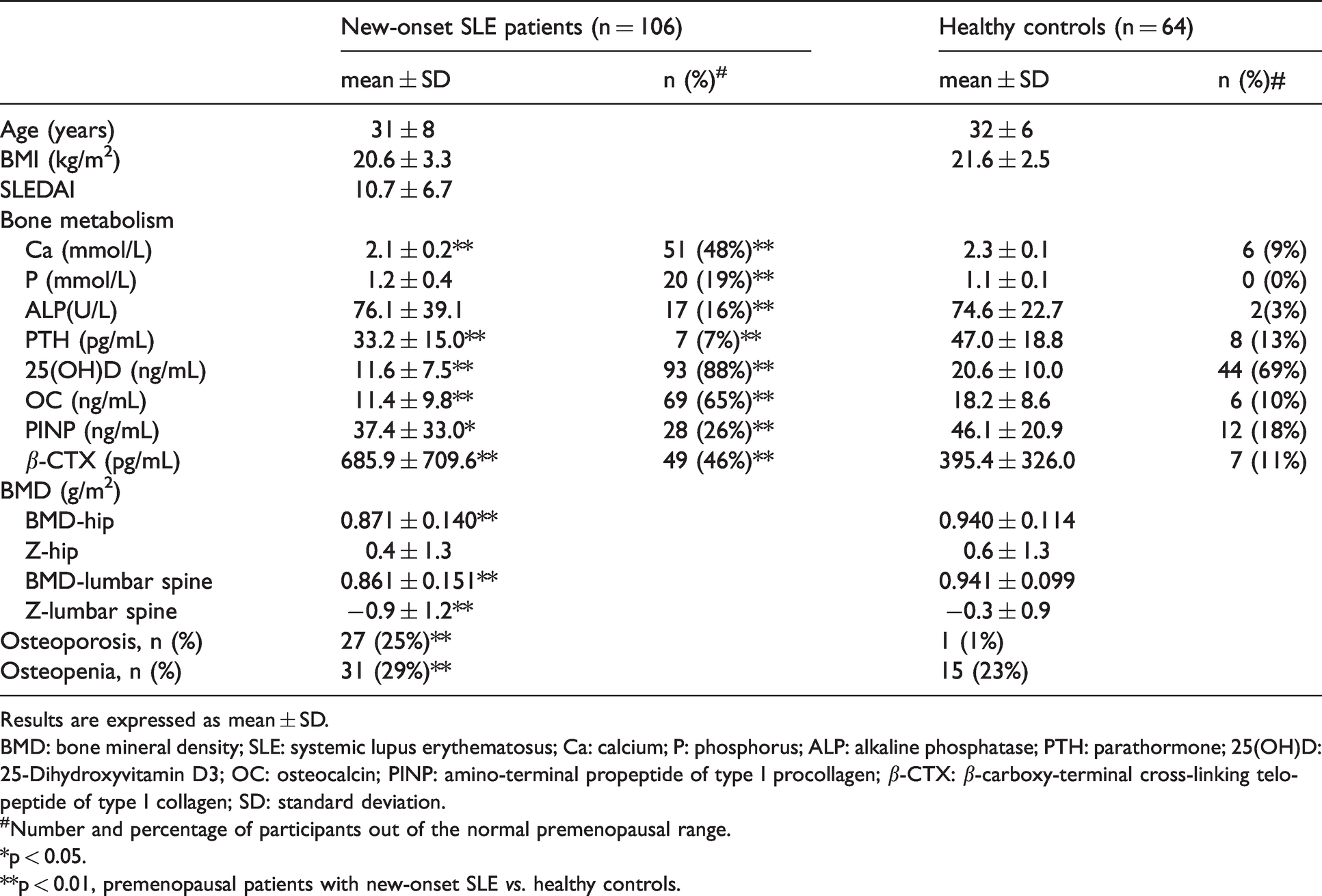
Results are expressed as mean ± SD.
BMD: bone mineral density; SLE: systemic lupus erythematosus; Ca: calcium; P: phosphorus; ALP: alkaline phosphatase; PTH: parathormone; 25(OH)D: 25-Dihydroxyvitamin D3; OC: osteocalcin; PINP: amino-terminal propeptide of type I procollagen; β-CTX: β-carboxy-terminal cross-linking telopeptide of type I collagen; SD: standard deviation.
#Number and percentage of participants out of the normal premenopausal range.
*p < 0.05.
**p < 0.01, premenopausal patients with new-onset SLE vs. healthy controls.
Furthermore, premenopausal patients with new-onset SLE showed significantly reduced OC (11.4 ± 9.8 ng/mL vs. 18.2 ± 8.6 ng/mL, P < 0.01) and PINP levels (37.4 ± 33.0 ng/mL vs. 46.1 ± 20.9 ng/mL, P < 0.05) and increased β-CTX (685.9 ± 709.6 pg/mL vs. 395.4 ± 326.0 pg/mL, P < 0.05) levels compared with healthy controls.
In addition, a significantly lower 25(OH)D (11.6 ± 7.5 ng/mL vs. 20.6 ± 10.0 ng/mL, P < 0.05), PTH (33.2 ± 15.0 pg/mL vs. 47.0 ± 18.8 pg/mL, P < 0.01) and Ca (2.1 ± 0.2 mmol/L vs. 2.3 ± 0.1 mmol/L, P < 0.01) in premenopausal patients with new-onset SLE were observed (Table 2). We have discovered a positive correlation between 25(OH)D and OC (r = 0.38, P < 0.01), positive correlation between 25(OH)D and PINP (r = 0.26, P < 0.01), and negative correlation between 25(OH)D and β-CTX (r = −0.27, P < 0.01), while no correlation has been found between 25(OH)D and BMD.
Univariate correlation analyses of SLEDAI compared with bone turnover abnormality
Univariate correlation analyses showed negative correlation between OC and SLEDAI (r = −0.3, P < 0.01). A significant positive correlation was observed between OC and complement 3 (C3) and C4 (C3: r = 0.3, P < 0.01, C4: r = 0.3, P < 0.01). OC was negatively correlated with erythrocyte sedimentation rate (ESR) (r = −0.2, P < 0.05).
A positive correlation was observed between β-CTX and SLEDAI (r = 0.3, P < 0.01). β-CTX was positively associated with CRP (r = 0.2, P < 0.05).
In addition, a negative correlation between 25(OH)D and SLEDAI was observed in premenopausal patients with new-onset SLE (r = −0.3, P < 0.01). Positive correlation between 25(OH)D and C3 and C4 (C3: r = 0.2, P < 0.05, C4: r = 0.2, P < 0.05) was observed in new-onset SLE patients (Table 3).
Correlation coefficients between BTMs and disease-related factors.
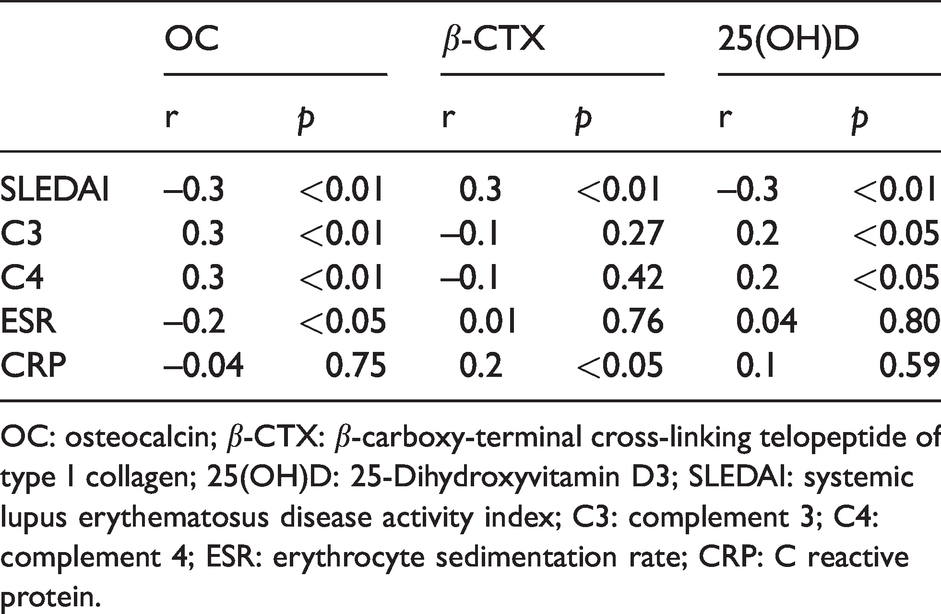
OC: osteocalcin; β-CTX: β-carboxy-terminal cross-linking telopeptide of type I collagen; 25(OH)D: 25-Dihydroxyvitamin D3; SLEDAI: systemic lupus erythematosus disease activity index; C3: complement 3; C4: complement 4; ESR: erythrocyte sedimentation rate; CRP: C reactive protein.
Correlations between autoantibodies and BTMs
Correlations between BTMs and autoantibodies were investigated to better understand SLE-associated osteoporosis. SLE patients positive for dsDNA, nucleosome, histone, and ribosomal P protein antibodies showed significantly decreased OC compared with patients negative for antibodies.
However, higher β-CTX levels were observed in SLE patients positive for anti-nucleosome, anti-histone, and anti-ribosomal P proteins (Figure 1).
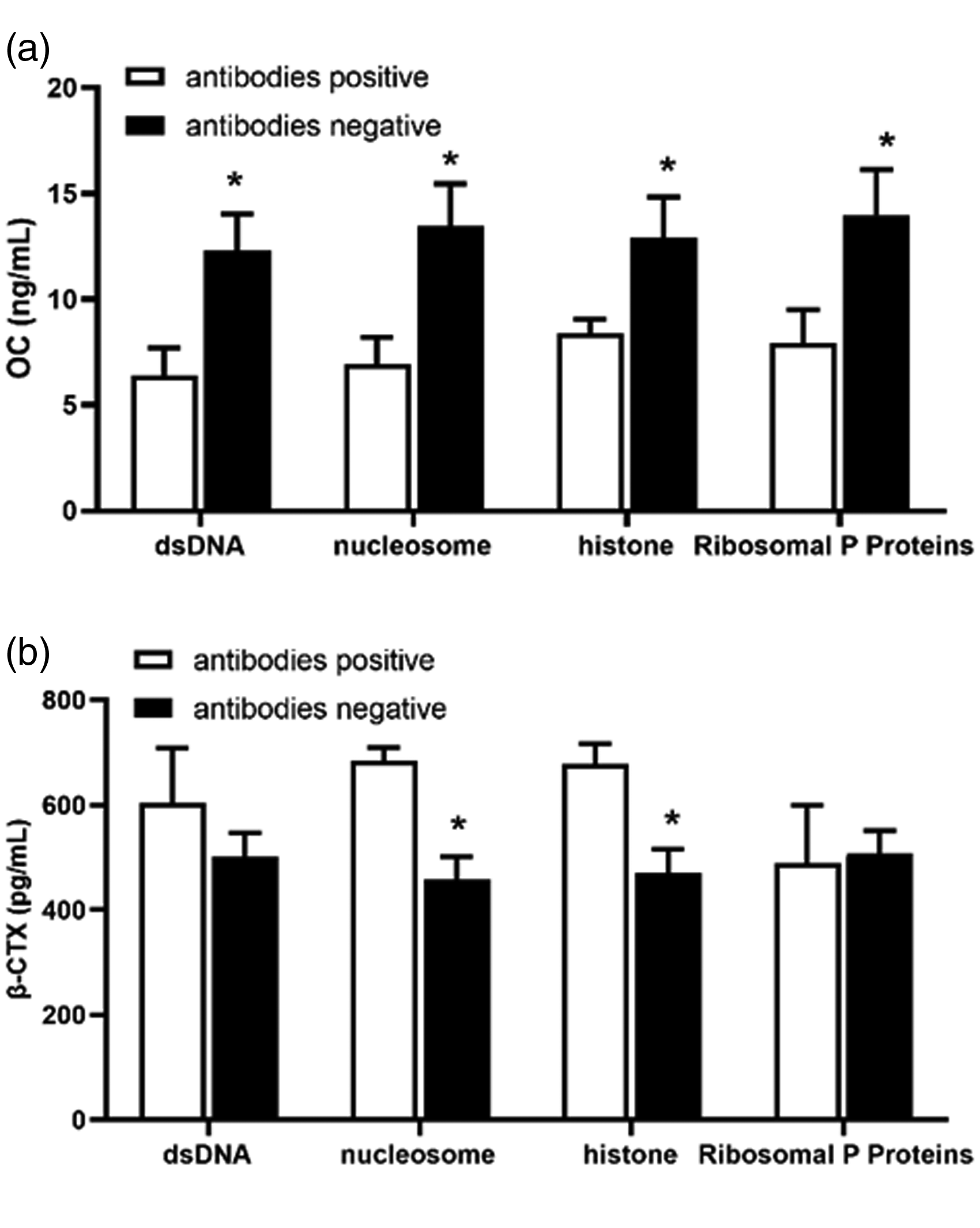
Comparison of bone turnover markers (BTMs) between antibody-positive and antibody-negative premenopausal patients with new-onset systemic lupus erythematosus (SLE). (a) osteocalcin (OC); (b) β-carboxy-terminal cross-linking telopeptide of type I collagen (β-CTX).*P < 0.05 premenopausal patients with antibodies positive vs. premenopausal patients with antibodies negative.
Discussion
Although decreased BMD and abnormal bone turnover in SLE patients has been confirmed in numerous studies, consensus regarding bone health in premenopausal SLE patients is lacking.4,11,12 Various risk factors contribute to bone loss in SLE patients, however, the risk remains controversial in premenopausal women. 13 To date, GCs are the main treatment for the management of SLE patients. However, the use of GCs for an extended period of time is also associated with bone loss. The estimated GC-induced osteoporosis rate is 50% for patients treated with GCs for more than 6 months. 14 To exclude the influence of GC treatment, the effects of SLE on bone homeostasis were comprehensively evaluated in premenopausal patients with new-onset SLE compared with gender-, age- and BMI-matched healthy controls in the present study. Young premenopausal women with SLE at the time of diagnosis exhibited osteopenia or osteoporosis as evidenced by reduced BMD based on DXA. Hip and lumbar spine BMD in premenopausal patients with new-onset SLE were significantly decreased compared with healthy controls. Higher rates of osteoporosis (25%) were observed in premenopausal patients with new-onset SLE, which is in agreement with several previous studies.15,16
Notably, abnormal bone turnover was observed in premenopausal patients with new-onset SLE, including an increase in bone absorption marker β-CTX and decrease in bone formation markers OC and PINP. These results indicated that SLE itself may contribute to abnormal bone remodeling in premenopausal SLE patients, resulting in osteopenia and osteoporosis in the end. BTMs are biochemical markers that reflect the metabolic activity of bone and provide information complementing to BMD in predicting fracture risk. 17 Bone resorption and bone formation are highly coupled in the normal physiological state that increased bone resorption is often accompanied by an appropriate increase of bone formation to maintain bone homeostasis. However, BTMs in premenopausal women with SLE have been assessed in only a few cross-sectional studies.18,19 In the present study, although premenopausal patients with new-onset SLE showed an increase in β-CTX compared with gender-, age- and BMI-matched healthy controls, a decrease in OC and P1NP was observed, indicating an apparent uncoupling of bone remodeling in SLE patients that leads to bone loss and lower BMD.
Studies on the relationship between SLE and bone metabolism are limited. In the present study, increased β-CTX level in premenopausal patients with new-onset SLE and positive correlation between β-CTX and SLEDAI confirmed that the disease activity is the main cause of bone resorption enhancement. β-CTX is recommended as a sensitive and specific marker of bone resorption by the International Osteoporosis Foundation and the International Federation of CLINICAL Chemistry and Laboratory Medicine, 20 which can be used to evaluate the risk of bone loss and bone fracture risk. In studies with postmenopausal women, high bone resorption predicted low BMD and high fracture risk, however, studies with premenopausal women are lacking. 21
Bone formation and bone resorption are highly coupled to maintain bone health. Osteoporosis is caused by abnormal bone remodeling, including excessive bone resorption and inadequate formation response. 22 However, the effects of disease activity on bone formation are unclear. The results of the present study showed a negative correlation between OC level and SLEDAI, indicating SLE may affect bone formation. OC is a bone matrix protein synthesized by mature osteoblasts with a compact, calcium-dependent, alpha helical conformation. OC constitutes approximately 15% of the non-collagenous bone matrix proteins, in which the gamma-carboxyglutamic acid (GLA) residues bind and promote absorption to hydroxyapatite in the bone matrix. Serum OC is a valid marker of bone turnover when the resorption and formation are coupled and a specific marker of bone formation when uncoupled. 23 Reportedly, higher tumor necrosis factor (TNF) and low-density lipoprotein (LDL) levels were found in active SLE patients and increased LDL induced activation of T cells and production of receptor activator of NF-kB ligand (RANKL) to enhance the maturation and activation of osteoclasts. 24 DC Lacey et al. discovered that TNF-α inhibited the differentiation of mature osteoblasts by inhibiting the expression of OC, alkaline phosphatase, Runx2 25 and stimulating production of Dickkopf-1 (DKK-1), which suppresses bone formation by inhibiting WNT-mediated osteoblast development and function. 26
In recent studies, the complex integration of the skeletal system with the immune system was reported.27,28 Here, we show a positive correlation between OC and C3 levels. Complement is an important component of innate and adaptive immunity. Serum complement plays an important role in the clearance of immune complexes in the body, thus, the decrease of serum complement level is an important biomarker for SLE diagnosis and a classical biological indicator for SLE disease activity. Studies have shown that C3 and C5 can directly promote the differentiation of mesenchymal stem cells into osteoblasts by binding to receptors C3aR and C5aR. 29 Moreover, complement is an important transmitter of the inflammatory response and inflammatory factors such as IL-6, MCP-1, and IL-8 can promote osteoclast differentiation and formation.30,31 Therefore, complement, as an important predictor of SLE disease activity, also plays an important role in regulating bone metabolism. An abnormal complement system in SLE patients may aggravate the chaos of bone metabolism, which in turn leads to lower BMD.
Overactivation of the immune system, the production of autoantibodies, formation of immune complexes, activation of complement, and the release of various inflammatory cytokines caused by systemic chronic inflammation are closely associated with the uncoupling of bone remodeling. 32 The results of our study showed that autoantibody-positive patients had decreased OC levels and increased β-CTX levels. Autoantibodies are produced by B cells, which are reportedly involved in bone loss in rheumatoid arthritis.33–35 Physiologically, B cells secrete osteoprotegerin (OPG), a potent anti-osteoclastogenic factor that preserves bone mass. However, activated B cells secrete pro-osteoclastogenic factors including RANKL, interleukin (IL)-17A, and TNF-α, promoting bone loss in inflammatory states.36,37 So decreased OC and increased β-CTX in autoantibody-positive patients may be caused by activated B cells. Besides, it has been reported that anti-citrullinated protein antibody (ACPA) directly induced differentiation of monocytes into osteoclasts resulting in bone loss in rheumatoid arthritis (RA) patients, 38 indicating that autoantibodies could induce bone loss independent of B cells. We have incubated RAW264.7 cells (precursor cell of osteoclast) with colony-stimulating factor, RANKL, and serum of SLE patients with positive dsDNA and antibodies. Our results showed increased TRAP, NFATC1, and s-Src mRNA expression in RAW264.7 cells incubated with the serum of SLE patients containing higher dsDNA and ANA titers (data not shown), which further confirmed the effect of autoantibodies on bone metabolism. Results in our study only indicate that antibodies may affect the bone health of SLE patients, but the mechanism underlying the correlation remains need for further research.
In the present study, we also found that 25(OH)D in premenopausal SLE patients was significantly lower than BMI- and age-matched healthy controls. Furthermore, 25(OH)D was positively correlated with bone formation and negatively correlated with bone resorption in our study, indicating that lower 25(OH)D may contribute to the uncoupling of bone remodeling in SLE. Vitamin D plays an important role in bone homeostasis by increasing intestinal absorption of calcium and phosphate, increasing bone mineralization, and stimulating osteoclast differentiation. 39 Deficiency of 25(OH)D caused secondary hyperparathyroidism and high bone turnover, then leading to bone lose. Study included 1436 healthy individuals in China revealed a negative linear correlation between PTH and 25(OH)D, and the breakpoint of 25(OH)D was 18.21 ng/mL, below which the PTH level rapidly increased. 40 However, no correlation between 25(OH)D and PTH, 25(OH)D and BMD was found in our study, indicating that SLE is far more complicated that the immune microenvironment may intervene both 25(OH)D and BMD. The etiology of reduced vitamin D plasma levels in SLE is multifactorial and includes a variety of intrinsic factors related to the disease itself. We also discovered that 25(OH)D was negatively associated with SLEDAI and positively associated with serum complement in SLE patients, indicating a correlation between 25(OH)D and immune function. Recently, various studies have focused on the immunological actions of Vitamin D. The vitamin D receptor (VDR) is expressed in almost all immune cells. 41 Colotta et al. 42 found that Vitamin D upregulated anti-inflammtory pathways in immune cells. So vitamin D insufficiency was associated with both bone loss and immunologic derangement in SLE patients. The exact mechanism that how vitamin D affect bone in SLE needs further research. Whether vitamin D deficiency is a pathogenic factor of SLE or the result of SLE is inconclusive. Based on the extensive immunomodulatory effects of active vitamin D and the results of improved disease and immunological indicators obtained by patients with vitamin D supplementation shown by limited prospective studies, it is more likely that vitamin D deficiency may be an SLE environmental pathogenic factor.
In summary, systemic inflammation has been found to have a widespread effect on the bone over the past 20 years. However, the mechanism of bone injury in some specific states has not been fully elucidated because of the complexity of systemic diseases like SLE with a variety of factors that affect bone biology. Whether premenopausal SLE bone injuries or GC treatment have a greater effect on the disease has been controversial. In the present study, weight, age, and GC factors were excluded, confirming that disease activity was a major factor resulting in BMD decline and abnormal bone turnover in premenopausal patients with new-onset SLE. These results show that significant bone loss is present in the early stages of Lupus in Chinese premenopausal patients. BMD and BMT should be promptly assessed after SLE diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the China National Foundations of Natural Sciences Foundation (No. 81702119) and the Shaanxi Province National Natural Science Foundation (No. 2018JQ8031).
Contributorship
All authors have a role in conducting the research and writing the manuscript. The final version of this manuscript is approved by all authors.