
Abstract
Objective
To determine longitudinal associations between Physician Global Assessment (PGA) and patient-reported outcomes (PROs) in patients with systemic lupus erythematosus (SLE).
Methods
Patients attending a rheumatology clinic between 2013 and 2017 completed specific (SLEQOL) and generic (SF36) health-related quality of life (HRQoL) surveys and rated their global rating of change (GRC) at each visit. PGA, SLEDAI-2K and SLE Flare Index (SFI) were also captured on all visits. Generalised estimating equations (GEE) methods were used to examine longitudinal associations of PGA with PROs and clinical indicators.
Results
337 patients were followed for a median [IQR] of 3.2 [1.6, 3.4] years (2,059 visits). High PGA (>1) was strongly associated with high SLEDAI-2K scores, the presence of flares and poor PROs. Odd ratios (OR) [95% CI] of PGA > 1 in patients with SLEDAI-2K >4 & <10 and SLEDAI-2K ≥10, compared to SLEDAI-2K ≤ 4, were 3.46 [2.36, 5.08], p < 0.001 and 6.39 [4.30, 9.49], p < 0.001, respectively. OR [95% CI] of PGA > 1 in patients with mild-to-moderate or severe flares were 2.09 [1.62, 2.71], p < 0.001 and 4.42 [3.21, 6.07], p < 0.001, respectively. Mental components of both SLEQOL (mood, self-image) and SF36 (MCS) surveys demonstrated significant associations with high PGA. After adjusting for SLEDAI-2K, one-point increase in PGA was associated with reductions in SLEQOL total score and SF36-MCS by 2.33 (regression coefficient (RC) [95% CI] = −2.33 [−3.77, −0.88], p = 0.002), and 4.16 (RC [95% CI] = −4.16 [−5.19, −3.13], p < 0.001) points, respectively. Associations of some physical components (SLEQOL-symptoms, and SF36-PCS) with PGA attenuated when adjusted for SLEDAI-2K. Patients who rated low scores of GRC, which indicate health deterioration, were twice as likely to have PGA > 1 (OR [95%CI] 1.99 [1.25, 3.16], p = 0.004).
Conclusion
High PGA was strongly associated with poor mental health, high disease activity and flares. This study confirms the value of PGA as an efficient assessment tool for SLE.
Keywords
Background
Systemic lupus erythematosus (SLE) is a chronic, heterogeneous, multi-system autoimmune disease with a substantial burden of morbidity. Patients suffer considerable physical, psychological and social challenges throughout their clinical course. 1 The impact of the disease on health-related quality of life (HRQoL) has been documented as worse than for several other chronic conditions.2–5
Ideally, assessment of an SLE patient should be a holistic evaluation from both the physician and patient. 6 However, the points of view between physician and patient often differ. Physicians usually assess the activity and severity of the disease based on factors that include patients’ symptoms, physical signs and laboratory findings. Several validated instruments have been developed for physicians to use as assessments of SLE disease activity in clinical practice and research trials, such as the Systemic Lupus Erythematosus Disease Activity Index −2000 (SLEDAI-2K). The physician global assessment (PGA) is often used in addition, to ensure capture of overall disease activity, especially bearing in mind the omission from standard instruments of several organ domains. 7 On the other hand, SLE patients usually perceive their disease and its impact on their quality of life not only by physical but also by psychological factors, as well as their past experience with the disease.8–11 There is increasing awareness of the difference between the perspective of physicians and patients, and consequently an increased interest in utilizing patient reported outcomes (PROs). Both generic instruments (e.g. SF36 12 or EQ-5D 13 ) and lupus-specific instruments (e.g. SLEQOL, 14 LupusQoL, 15 and LupusPRO 16 ) have been used to assess HRQoL in SLE. Many studies illustrate the discrepancies between physician- vs. patient-assessed health status in SLE,8–11 but the relationship between physician-measured disease activity using the PGA and patient-reported HRQoL outcomes has been sparsely explored. With the emerging requirement for clinical trials to include patient reported outcomes, 17 and inconsistent results of several clinical trials, mainly due to study design and outcome measurements, 18 understanding the relationship between an easily utilized, clinical assessment tool such as PGA and patient-reported HRQOL outcomes is important.
Recently, we published our experience in comparing the generic HRQoL survey, SF36, with SLE-specific HRQoL survey, SLEQOL, in lupus patients, and showed that these two instruments were broadly equivalent in assessing HRQoL. 2 In the current study, we have examined how the PGA was associated with patient-reported HRQoL, assessed using both generic and specific instruments.
Patients and methods
Adult, consenting SLE patients who attended the rheumatology clinic at Chiang Mai University Hospital, Thailand were prospectively followed from October 2013 to June 2017. All patients met either the 1997 American College of Rheumatology (ACR), 19 or the 2012 Systemic Lupus International Collaborating Clinics (SLICC) classification criteria for SLE. 20 This study was performed in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study was approved by the Research Ethics Committee of Faculty of Medicine, Chiang Mai University (no. 202/2013). All of the participants gave their written informed consent prior to entering the study.
Disease activity was assessed by using the SLEDAI-2K, 21 and SLE Flare Index (SFI) 22 at 3-6 monthly routine visits, while irreversible organ damage was determined annually using the SLICC-ACR SLE Damage Index (SDI). 23 Lupus Low Disease Activity State (LLDAS) was determined according to the definition of Franklyn et al., 24 and SLE disease severity was classified according to Abrahamowicz ‘s definition. 25 The PGA was determined on a 0-3 scale representing the range from none to severe lupus activity. 22 Each patients’ PGA was assessed by the same clinician (WL or NK) throughout the study.
Patients completed SLEQOL and SF36 (version 2.0) surveys at each routine visit. Both SLEQOL and SF36 surveys have been translated into Thai, validated,26,27 and used in many clinical studies in Thailand.28,29 In addition, Global Rating of Change (GRC), in which patients rated their global health status compared to previous visit on a 7-point Likert scale (from −7 [a very great deal worse] to +7 [a very great deal better]) was captured. Visits were grouped into either ‘no change’ (−1 to +1), ‘deterioration’ (−2 to −7) or ‘improvement’ (+2 to +7) categories based on GRC scores. 30
SF36 surveys were scored using the QualityMetric Health Outcomes Scoring Software 5.0 (Optum, Lincoln, Rhode Island, USA) to derive the final summary scores, physical component summary (PCS) and mental component summary (MCS) as well as eight domain specific scores: physical functioning (PF), role physical (RP), role emotional (RE), social functioning (SF), mental health (MH), energy/vitality (VT), bodily pain (BP), and general health (GH). High SF36 scores mean better HRQoL. In the SLEQOL survey, the overall score was derived from six domain-specific (physical functioning, activities, symptoms, treatment, mood and self-image) scores. In contrast to SF36, high SLEQOL scores mean poor HRQoL; therefore, we used the processes of re-scoring and standardization as previously described, in order to compare SLEQOL with SF36 results.2,31
Statistical analysis
Statistical analyses were performed using Stata version 15.1 (StataCorp, College Station, Texas, USA). Firstly, differences in patient characteristics between PGA-high (PGA > 1) and PGA-low (PGA ≤ 1) were examined. Continuous variables were summarized as median (interquartile range [IQR], range) and compared using Mann-Whitney U tests, while categorical variables were described as frequency (%) and compared using Chi-squared tests. Time-adjusted mean (TAM) values were derived for variables including PGA, SLEDAI-2K, SF36, and SLEQOL scores to estimate the average values accounting for varying time intervals between visits.
Generalised estimating equations (GEE) methods were used to examine longitudinal associations of PGA with other disease activity indicators, including SLEDAI-2K and flare, wherein PGA was considered as the outcome variable. The same statistical methods were used to examine the associations between PGA and HRQoL in which, HRQoL assessments were treated as the outcomes. We used PGA in both continuous and categorical forms to assess associations; using Gaussian distribution along with link identity for continuous and binomial distribution with logit link for binary outcomes. Exchangeable correlation matrices were used in all models and robust standard errors were derived adjusting for patient clustering. Results are reported as either mean change (regression coefficients) or odds ratio (OR) with corresponding 95% confidence interval (95% CI); negative mean changes indicate poorer HRQoL and vice versa. A p-value <0.05 was considered statistically significant.
Results
This study included 337 SLE patients and 2,059 visits; SF36 and SLEQOL data were available from 2,054 and 2,055 visits, respectively. The median [interquartile range (IQR)] duration of follow-up in this study was 3.2 [1.6, 3.4] years. Since GRC measures inter-visit changes, GRC status was available for 1,722 visits.
Patient characteristics
Characteristics of this study population have previously been published. 2 In brief, the majority of patients (n = 325 [96%]) were female with a median [IQR] age at diagnosis of 26 [19, 38] years, age at enrolment of 37 [28, 48] years and disease duration of 7 [3, 13] years. About 95% (n = 319) of patients were treated with glucocorticoids at least once during the observation period with a median [IQR] TAM prednisolone of 5.8 [3.7, 9.3] mg/day. Additionally, 84% (n = 284) of patients received immunosuppressive treatment and 38% (n = 129) received anti-malarials during the study period. The median [IQR] TAM-SLEDAI-2K of the whole study group was 3.4 [2.0, 5.6]. The median [IQR] TAM-PGA was 0.4 [0.3, 0.6] (Figure 1); PGA was >1 at 246 visits (12%), and 110 (33%) patients had PGA >1 at least once. Regarding flares, about 56% (n = 189) of patients had experienced mild/moderate or severe flare at least once during the study period.
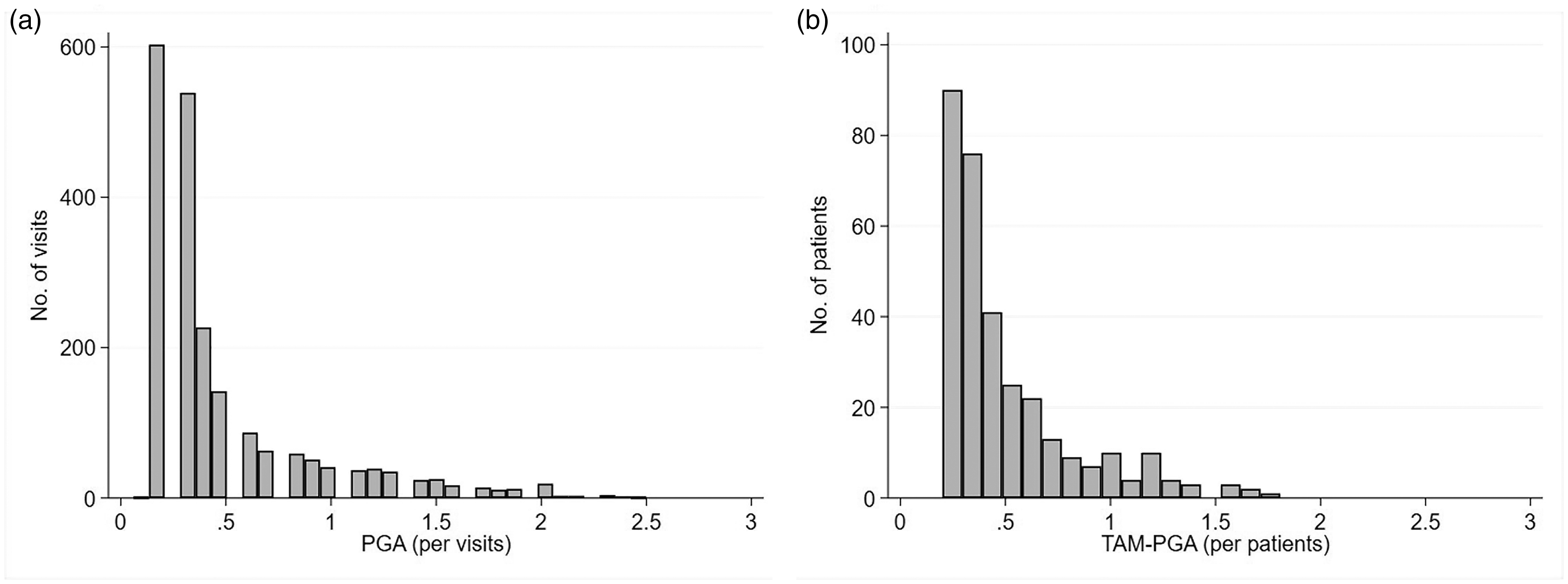
Distribution of (a) PGA by visits; (b) TAM-PGA by patients.
Disease characteristics in patients categorised by PGA
We examined clinical characteristics in patients categorised by high versus low PGA, using a cut-off of PGA > 1 for assignment as ‘high’ (including moderate and high disease activity). We categorised patients in two ways; whether PGA > 1 was ever observed, and based on TAM-PGA >1. Patients in high PGA groups were younger at disease diagnosis and study enrolment, with a shorter study observation period. High PGA group patients also had significantly higher tertiary educational level, SLEDAI-2K and had received higher mean prednisolone doses (Table 1). In addition a high PGA ever was associated with higher likelihood of glucocorticoid and immunosuppressant use and flare. Association with other disease indicators were similar between the PGA and TAM-PGA.
Patient characteristics, stratified by PGA.
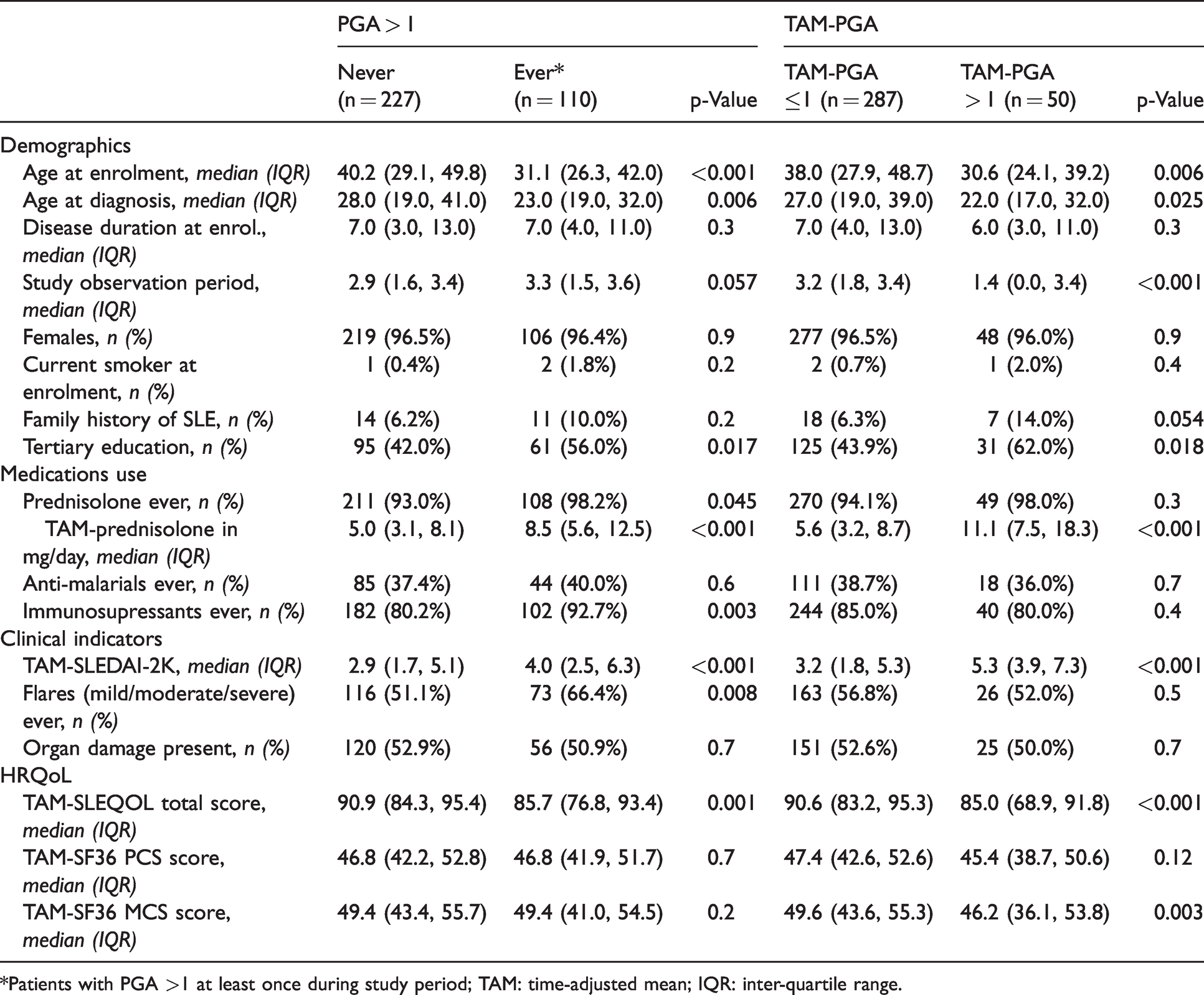
*Patients with PGA >1 at least once during study period; TAM: time-adjusted mean; IQR: inter-quartile range.
Longitudinal associations of PGA with disease activity indicators
We first sought to confirm associations of PGA with other measures of SLE disease activity. Measured over time, PGA demonstrated strong positive associations with other SLE disease activity measures. In GEE analysis, PGA was significantly higher in patients with active SLE defined by SLEDAI-2K >4, (Table 2). Each increase of one point in SLEDAI-2K was associated with a significant increase in mean PGA of 0.05 (95% CI: 0.04, 0.06, p < 0.001). When assessed by SLEDAI-2K categories, we observed that if the SLEDAI-2K was >4 & <10, the odds of PGA being >1 was more than three times greater than in patients with SLEDAI-2K ≤ 4 (OR [95%CI] =3.46 [2.36, 5.08], p < 0.001). Similarly, in patients with SLEDAI-2K ≥ 10, the odds ratio of PGA >1 was 6.39 [4.30, 9.49], p < 0.001). PGA was also higher in those who experienced flares. The differences in estimated mean PGA (RC [95%CI]) between patients with and without mild/moderate flares was 0.24 [0.18, 0.30], and between those with and without severe flares was 0.43 [0.35, 0.51].
Longitudinal associations of PGA with SLE disease activity indicators.
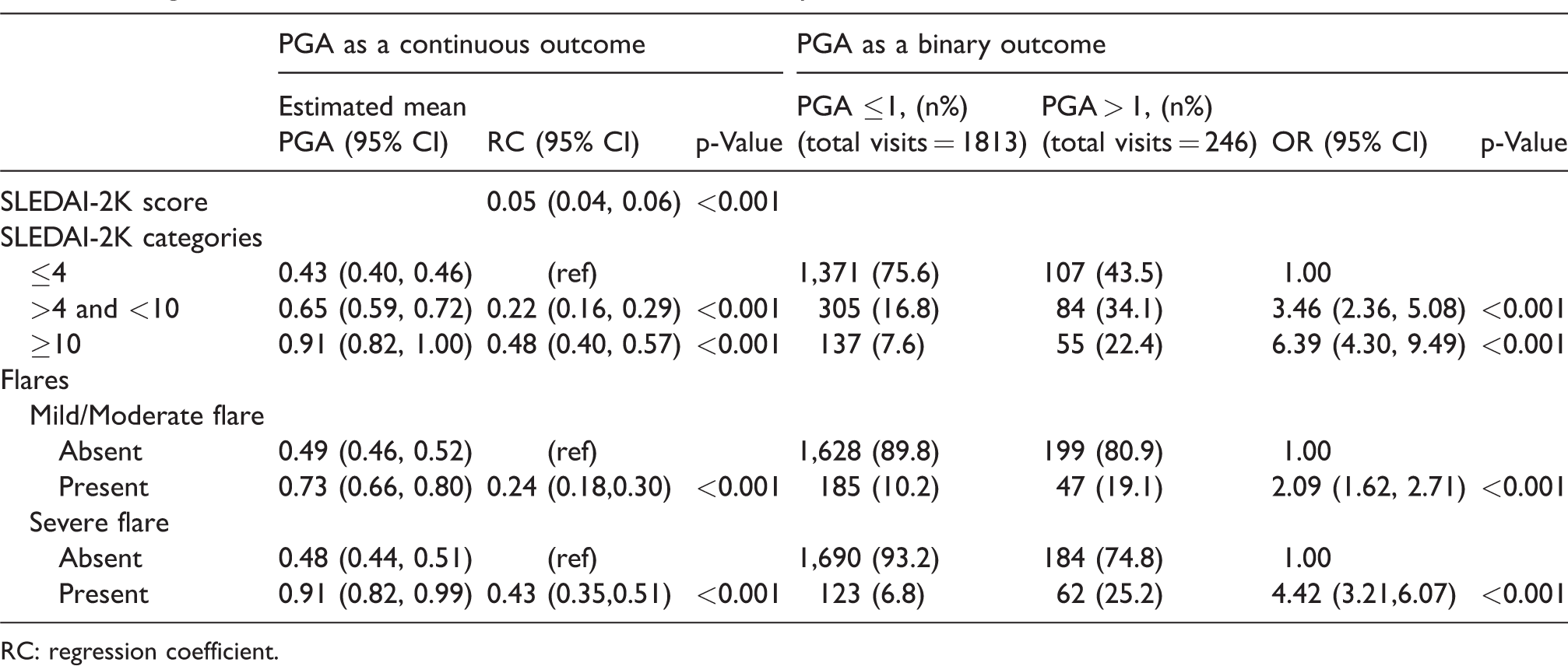
RC: regression coefficient.
Associations between PGA and HRQoL indicators
We next examined univariable longitudinal associations of PGA with both generic (SF36) and SLE-specific (SLEQOL) HRQoL surveys. PGA was significantly associated with both SLEQOL and SF36 summary scores (Supplementary Table 1). An increase of one point in PGA was associated with a significant reduction in SLEQOL total score (OR [95% CI] −3.47 [−4.85, −2.09] p < 0.001). Similarly, one-point increase in PGA was associated with reduction in each of SF36-PCS and SF36-MCS, by −1.45 [−2.31, −0.58], p < 0.001) and −4.02 [−4.98, −3.06], p < 0.001), respectively. We further examined associations of PGA > 1 with specific domains, and except for SF36-PH (physical functioning), all other domains were negatively associated with statistical significance (Supplementary Table 1 and Figure 2). Interestingly, domains that contribute more towards mental health such as SLEQOL-mood and SF36-RE (role emotional) and SF36-SF (social functioning) demonstrated stronger associations than physical health domains.
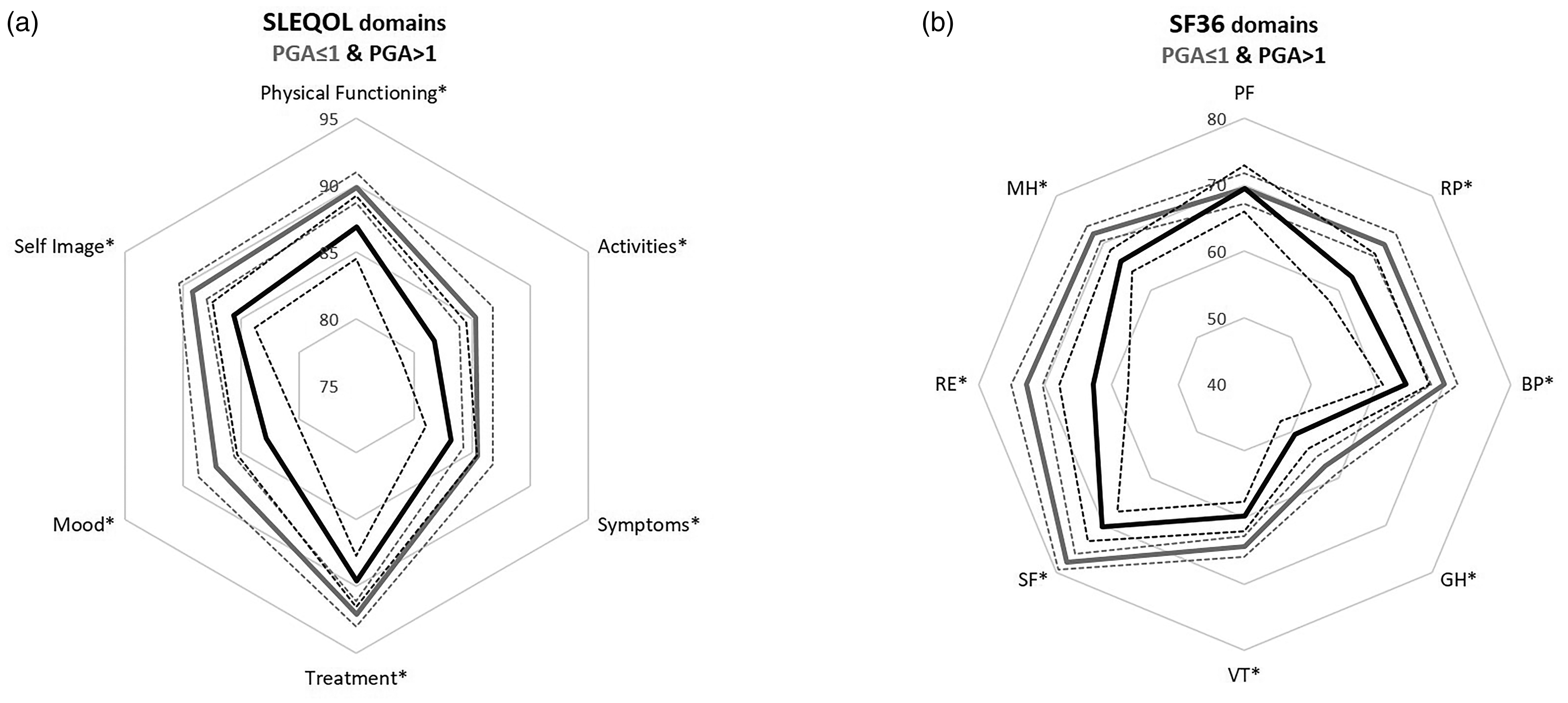
Radar charts showing comparison of estimated means (solid lines) and corresponding 95% CIs (dotted lines) of (a) SLEQOL and (b) SF 36 survey domains between SLE patient visits with PGA≤ 1 and PGA > 1.
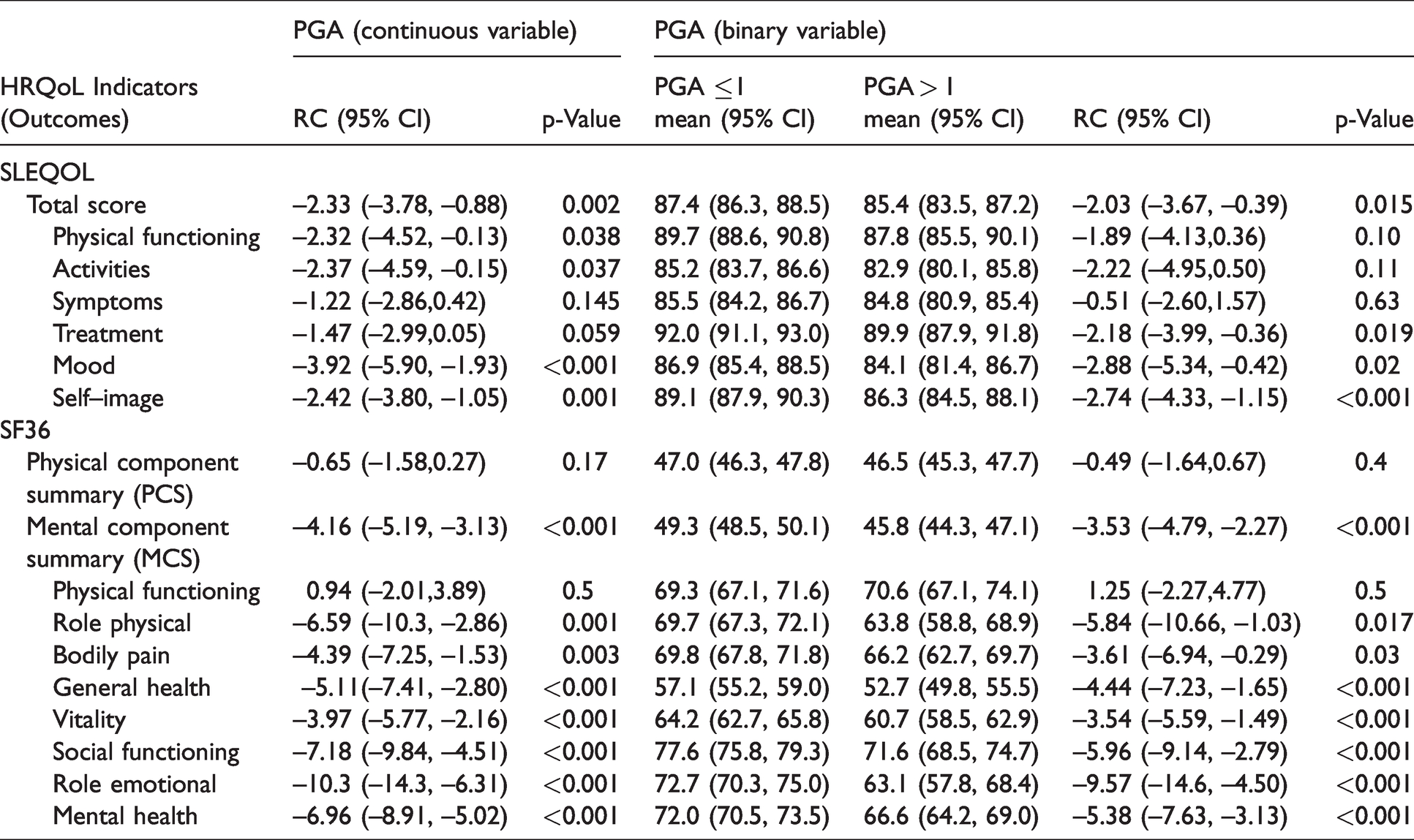
We next examined the independence of the association of PGA with HRQoL by adjusting for disease activity measured by SLEDAI-2K. PGA remained strongly associated with most domains of both SLEQOL and SF36 surveys after adjustment (Table 3). Domains related to mental health remained statistically significantly associated, while some domains related to physical health attenuated. After adjustment, an increase in one point in PGA was associated with a significant reduction in SLEQOL total score of 2.33 points (RC [95%CI] −2.33 [−3.78, −0.88] p = 0.002). However, the association of some specific SLEQOL domains, namely ‘symptoms’ and ‘treatment’, attenuated when adjusted for SKEDAI-2K. Similarly, after adjustment, an increase in one point in the PGA remained significantly associated with a reduction in SF36-MCS by 4.16 points (RC [95%CI] −4.16 [−5.19, −3.13] p < 0.001). In contrast, no associations of SF36-PCS and SF36-PF (physical functioning) domain with PGA was observed after adjusting for SLEDAI-2K (Table 3).
Longitudinal associations of PGA with HRQoL measures, adjusted for disease activity (SLEDAI-2K score).
We further examined the associations between the PGA and HRQoL outcomes in patients with moderate-to-high active disease, i.e., SLEDAI-2K ≥ 6, and the results are summarised in Supplementary Table 2. Overall, PGA was significantly associated with overall summary scores (SLEQOL-total score; SF36-PCS; SF36-MCS), and most domain-specific scores, in both SLEQOL and SF36 surveys in these patients. Domains that were not associated with PGA in this active disease group include SLEQOL-symptoms; SLEQOL-treatment, and SF36-PF (Supplementary Table 2).
Finally, we examined the associations between GRC and PGA. In contrast to the relative stability of PGA across the study, patients’ GRC ratings fluctuated considerably (Supplementary Figure 1). GRC-defined deterioration was significantly associated with PGA. When compared to patients who rated GRC as ‘no change’ in HRQoL, those who rated deterioration were nearly as twice as likely to have PGA > 1 than PGA ≤ 1 (OR [95%CI] 1.99 [1.25, 3.16], p = 0.004). In contrast, no association with PGA was shown for GRC rated improvement (OR [95%CI] 0.99 [0.67, 1.45], p = 0.9) (Figure 3).
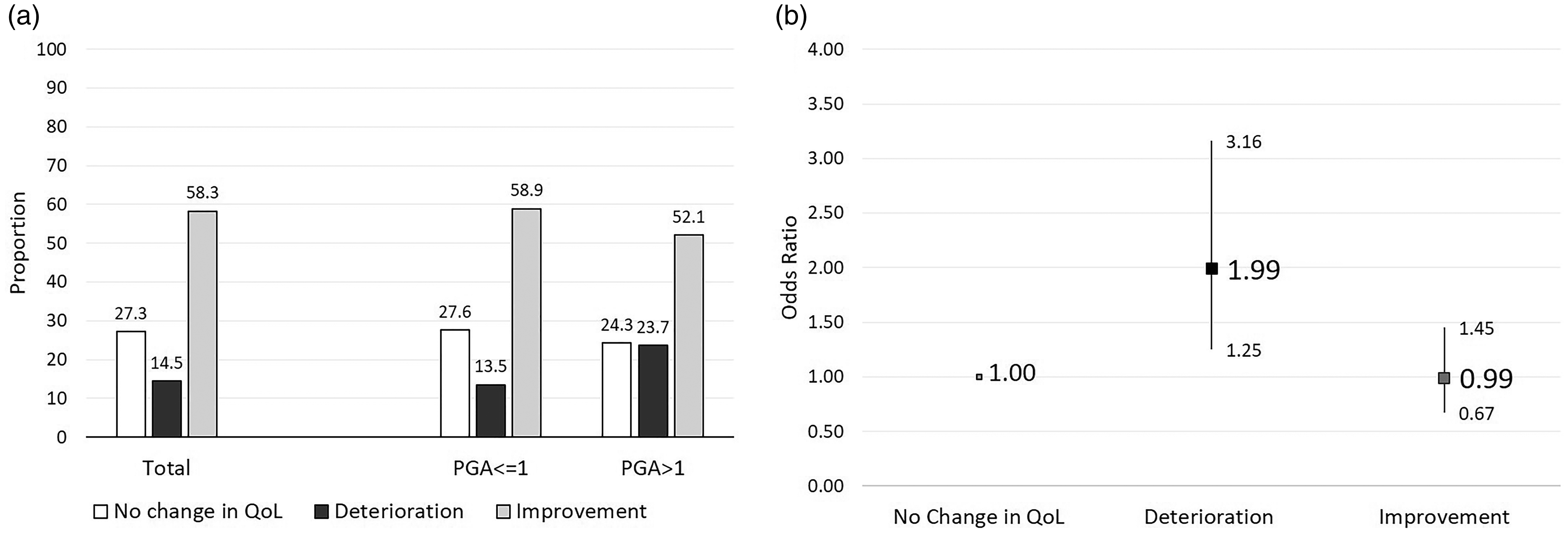
(a) Proportions of patients in GRC categories stratified by PGA (≤1 vs. >1), and (b) Odds ratios and 95% CIs of patients reporting deterioration or improvement if PGA was >1, compared to patients with PGA < 1.
Discussion
In the absence of an ideal measure of disease activity and treatment response in SLE, the composite endpoints currently used in clinical trials, the SLE responder index (SRI) and BILAG-based Composite Lupus Assessment (BICLA), both include a physician global assessment.32,33 However, none of these endpoints directly capture how patients feel and function, issues recently identified as critical to trial treatment response measures. 17 Patient-reported HRQoL may be a concept closer to this goal in SLE, but correlations between physician-measured disease activity and HRQoL measures remain incompletely understood.
In this study, we examined the associations of physician-assessed disease activity captured with the PGA with patient-reported HRQoL in a prospectively followed SLE patient cohort. High PGA was significantly associated with poor HRQoL, captured using both generic (SF36) and SLE-specific (SLEQOL) instruments. These negative associations were more prominent in mental health domains than physical domains, regardless of instrument. In addition, using GRC, we found that patients who had high PGA (>1) were more likely to indicate deterioration than no change or improvement in HRQoL. This finding was in line with our previous observation that patients who rated their GRC as deterioration had poorer HRQoL. 2
Several studies examining the associations between PGA and HRQoL in SLE have been previously published. For instance, Chaigne et al., 34 in their cross-sectional study, reported significant, negative association between PGA and all domains of the SF36 instrument. Another cross-sectional study by Kaya et al., 35 reported a modest but significant negative association between PGA and all domains of the Turkish LupusPro instrument, except that of the cognition domain. These two studies were in line with our observations. In a large prospective multicenter cross-sectional study, Golder et al., 4 also reported a significant negative association between PGA and SF36 survey results. In contrast, other studies have shown weak or no associations between disease activity measures, including PGA, and patient-reported HRQoL. 36
Importantly alongside associations with measures of HRQoL, we found that PGA was significantly associated with other SLE disease activity indicators such as SLEDAI-2K and flare index, supporting the utility of PGA as a disease activity instrument in SLE. A direct association between PGA and validated SLE disease activity instruments is not well described; indeed inclusion of PGA in the SRI and BICLA clinical trial endpoints in order to capture disease activity missed by these measures comports with the idea that they may measure things. Aranow et al. performed two studies determining the correlation between PGA and SLE disease activity instruments: the first study was performed in an out-patient rheumatology clinic using the SELENA-SLEDAI instrument, 7 and the second study was based on 50 real-life cases, assessed by 60 rheumatologists around the world, using SLEDAI-2K. 37 Both studies showed very good correlations between PGA and the disease activity instrument. Furthermore, the authors reported that PGA determined with knowledge of patients’ laboratory results showed better correlation than when determined without laboratory results.7,37 A separate study by Chaigne et al. found that active disease defined by SELENA-SLEDAI ≥4 was associated with high PGA. 34
PGA assessment is by definition subjective, and relates to the physician’s experience and other factors impacting on his/her judgment at the time of evaluation. Some physicians may assess SLE disease activity based only on clinical findings and laboratory results and pay little or no attention to the patients’ symptoms. For example, for a patient who has arthritis in several joints and complains about difficulty in performing daily activities/household chores, a physician may rate the PGA as moderate because of the involvement of several joints, while another may rate the PGA higher due to patient’s difficulty in performing daily activities. Similar scenarios can easily be imagined where physicians with different levels of experience may rate PGA differently for a patient with lupus nephritis with a given degree of proteinuria. In this study, PGA was assessed by the same physicians throughout the study, each with >15 years of experience of caring for lupus, which we consider as a strength of this study.
The lack of association between PGA and the SF36 physical functioning domain was interesting. This might be explained by the low prevalence of musculoskeletal symptoms in the study cohort. This was a single center study and therefore, generalizability of the findings to a wider population may be limited, although the instruments used are widely used and validated across languages and cultures. We did not collect a patient rating of global disease activity (PtGA), which may be conceptualized differently to physician ratings of disease activity. However, previous studies have shown at best moderate correlation between PGA and PtGA.8–10,38,39 It also should be noted that approximately two-third of the patients in this study had low disease activity at enrollment. This could be explained that they had a long disease duration prior to enrollment (median 7 years), as although majority of SLE patients have remitting-relapsing disease activity, the proportion of those with long quiescent disease increases over time.40,41
Conclusion
Herein, we report the results from one of the largest studies examining the longitudinal associations between PGA and patient-reported HRQoL. PGA correlated well with conventional measures of disease activity, and was significantly negatively associated with HRQoL measured by generic or lupus-specific HRQoL instruments, and in particular high PGA was a strong indicator of poor mental health HRQoL scores in SLE. Hence, we conclude that PGA is a useful tool to capture SLE disease state. Since PGA is a simple and a less time-consuming instrument than other measures used in research settings, this supports the value of PGA being routinely used in lupus patient care.
Supplemental Material
sj-pdf-1-lup-10.1177_09612033211027943 - Supplemental material for Associations between physicians’ global assessment of disease activity and patient-reported outcomes in patients with systemic lupus erythematosus: A longitudinal study
Supplemental material, sj-pdf-1-lup-10.1177_09612033211027943 for Associations between physicians’ global assessment of disease activity and patient-reported outcomes in patients with systemic lupus erythematosus: A longitudinal study by Worawit Louthrenoo, Nuntana Kasitanon, Eric Morand and Rangi Kandane-Rathnayake in Lupus
Supplemental Material
sj-pdf-2-lup-10.1177_09612033211027943 - Supplemental material for Associations between physicians’ global assessment of disease activity and patient-reported outcomes in patients with systemic lupus erythematosus: A longitudinal study
Supplemental material, sj-pdf-2-lup-10.1177_09612033211027943 for Associations between physicians’ global assessment of disease activity and patient-reported outcomes in patients with systemic lupus erythematosus: A longitudinal study by Worawit Louthrenoo, Nuntana Kasitanon, Eric Morand and Rangi Kandane-Rathnayake in Lupus
Supplemental Material
sj-pdf-3-lup-10.1177_09612033211027943 - Supplemental material for Associations between physicians’ global assessment of disease activity and patient-reported outcomes in patients with systemic lupus erythematosus: A longitudinal study
Supplemental material, sj-pdf-3-lup-10.1177_09612033211027943 for Associations between physicians’ global assessment of disease activity and patient-reported outcomes in patients with systemic lupus erythematosus: A longitudinal study by Worawit Louthrenoo, Nuntana Kasitanon, Eric Morand and Rangi Kandane-Rathnayake in Lupus
Supplemental Material
sj-pdf-4-lup-10.1177_09612033211027943 - Supplemental material for Associations between physicians’ global assessment of disease activity and patient-reported outcomes in patients with systemic lupus erythematosus: A longitudinal study
Supplemental material, sj-pdf-4-lup-10.1177_09612033211027943 for Associations between physicians’ global assessment of disease activity and patient-reported outcomes in patients with systemic lupus erythematosus: A longitudinal study by Worawit Louthrenoo, Nuntana Kasitanon, Eric Morand and Rangi Kandane-Rathnayake in Lupus
Footnotes
Availability of data and materials
The datasets used and/or analyzed in this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Asia Pacific Lupus Collaboration (APLC), which is funded by unrestricted educational grants from Janssen, Eli Lilly, Bristol Myers Squibb and Merck Serono.
Acknowledgements
We thank Mrs. Waraporn Sukitawut, Ms. Saowanee Pantana and Ms. Phimwalan Konkaeo for their secretarial assistance.
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.