
Abstract
Background
Systemic lupus erythematosus (SLE) and Primary Antiphospholipid Syndrome (PAPS) overlap clinical and immunological features. Therefore, misclassification of PAPS patients as SLE is a concern. The ACR/EULAR 2019 SLE classification has never been studied in PAPS.
Objective
To verify if the ACR/EULAR 2019 SLE classification can correctly classify a PAPS patient as not having SLE and compare its performance with the SLICC 2012 SLE classification. Methods: One-hundred thrombotic PAPS patients who fulfilled the Sidney criteria were consecutively screened and those who attended the inclusion criteria were submitted to ACR/EULAR 2019 and SLICC 2012 classifications.
Results
Sixty-seven PAPS patients were included in this study. The majority was female (89.6%) with median age at study inclusion of 45 years (35–53) and median PAPS disease duration of 13 years (8–19). PAPS correct classification was observed more often with ACR/EULAR 2019 than SLICC 2021 criteria (94.0% vs. 64.2%; p < 0.001). The 4 misclassified patients in ACR/EULAR 2019 were also misclassified in SLICC 2012. The comparison of misclassified patients to those correctly not classified as SLE resulted, for both criteria, in higher frequencies of hematological domain [ACR/EULAR 2019 (100% vs. 28.6%, p = 0.010) and SLICC 2012 (95.8% vs. 11.6%, p < 0.001)]. Further analysis of hematological manifestations revealed that for the ACR/EULAR 2019 leukopenia (100% vs. 22.2%, p = 0.004) and for the SLICC 2012 leukopenia/lymphopenia (91.7% vs. 7%, p < 0.001) were more frequent in misclassified group. Proteinuria (20.8% vs. 0%, p = 0.004) and low complement (45.8% vs. 20.9%, p = 0.033) were also more often observed in the incorrectly SLICC 2012 classified patients.
Conclusion
ACR/EULAR 2019 had high accuracy for distinguishing PAPS from SLE, whereas the SLICC 2012 incorrectly classified more than one third of the PAPS patients as having SLE.
Keywords
Introduction
Antiphospholipid syndrome (APS) is classified according to the updated Sidney criteria, which requires the presence of one thrombotic or one obstetric criterion, associated with at least one persistently positive antiphospholipid antibody (aPL), namely lupus anticoagulant (LA), anticardiolipin (aCL), and/or anti-ß2 glycoprotein I antibodies (aß2GPI). 1 Up to 50% of cases are associated with other autoimmune diseases, mainly systemic lupus erythematosus (SLE). The other half is considered as primary APS (PAPS). 2
Misclassification of PAPS as SLE remains a challenge in spite of the fact that the existing SLE classification criteria were reported to have both high specificity (which is the main characteristic of American College of Rheumatology (ACR) 1997 classification) 3 and high sensitivity (which is the main characteristic of Systemic Lupus International Collaborating Clinics (SLICC) 2012 classification). 4 In fact, PAPS and SLE share many clinical and immunological features such as hematological manifestations, proteinuria, seizures and antinuclear antibodies (ANA) positivity. This overlap of criteria may justify the misclassification of some PAPS patients as SLE, which is a critical concern. 6
Recently, Aringer et al. validated new SLE classification criteria that were endorsed by the ACR and the European League against Rheumatism (EULAR) (ACR/EULAR) 2019 classification, with 96.1% of sensitivity and 93.4% of specificity. The inclusion of a positive ANA as the main entry criterion was a critical step to improve accuracy. Moreover, this is the first classification to attribute weights to each criterion. 5 These new ACR/EULAR 2019 classification criteria were not tested in the setting of PAPS.
The main objective of the present study was to compare the performance of the ACR/EULAR 2019 and the SLICC 2012 criteria according to their rates of misclassification of PAPS patients as SLE.
Patients and methods
Study cohort
Data were obtained from an electronic database from 2000 (when our standard electronic protocol was introduced) to 2020. All PAPS patients regularly followed in the specialized APS Clinical Unit of the Rheumatology Division, Hospital das Clínicas HCFMUSP, Faculdade de Medicina, Universidade de São Paulo, Brazil, were included for screening. One hundred consecutive PAPS were identified and retrospectively studied.
The main inclusion criterion for screening was the previous diagnosis of thrombotic primary APS (with or without obstetric APS) according to current APS classification criteria (Sidney). 1 All thrombotic manifestations were documented with imaging or histopathological studies. Positivity to aPL was confirmed on two or more occasions, at least 12 weeks apart. LA was detected according to the guidelines of the International Society on Thrombosis and Haemostasis. 7 aCL (IgG and/or IgM) in serum or plasma was considered positive if present in medium or high titers (>40 GPL or MPL), and aβ2GPI (IgG and/or IgM) was considered positive if titers were >20 U/mL as measured by standardized ELISA. 1 Anti-Sm and anti-dsDNA were performed by ELISA and anti-dsDNA was confirmed by Crithidia luciliae immunofluorescence test. Values of anti-dsDNA 2-fold or higher than the upper reference limit were considered high titers. 4
Exclusion criteria for analysis were suspicion of other autoimmune diseases, especially SLE or missing data that could jeopardize the SLE classifications.
The study was approved by our Local Ethics committee, number 37149820.2.0000.0068 (ICHC/USP).
Evaluation of SLE classification criteria
All PAPS patients included were submitted to the two current SLE classification criteria (SLICC 2012 and ACR/EULAR 2019). Patients were classified as SLE if they met 4 criteria in the SLICC 2012 or scored 10 points or more in the ACR/EULAR 2019 (which requires a positive ANA with titers ≥1:80 as an entry criteria). Descriptions of both SLE classification criteria are reported elsewhere.4,5
Statistical analysis
Categorical variables were presented as numbers and percentages and were analyzed by Pearson Chi-square or two-tailed Fisher’s exact test. Continuous variables were expressed as mean and standard deviation (SD) if normally distributed or median and interquartile range if asymmetrically distributed. Normality was analyzed by the Kolmogorov-Smirnov test. Student’s t-test was used for normally distributed continuous variables, and Mann-Whitney U test for asymmetrical continuous variables. The difference between classification criteria were assessed by McNemar’s test. Statistical analysis was performed using SPSS Version 23 (Chicago, Illinois). A p-value of <0.05 was considered as statistically significant.
Results
One-hundred PAPS patients were initially screened. A total of 33 patients were excluded due to: lupus-like presentation (n = 3); lack of important laboratory data, such as anti-Sm, anti-dsDNA, complement and proteinuria (n = 16). We also excluded patients who did not perform the direct Coombs test and fulfilled 3 points in SLICC 2012 (n = 14).
After considering these exclusion criteria, 67 PAPS patients were included in this study and were then classified according to SLICC 2012 and ACR/EULAR 2019 criteria (Figure 1).
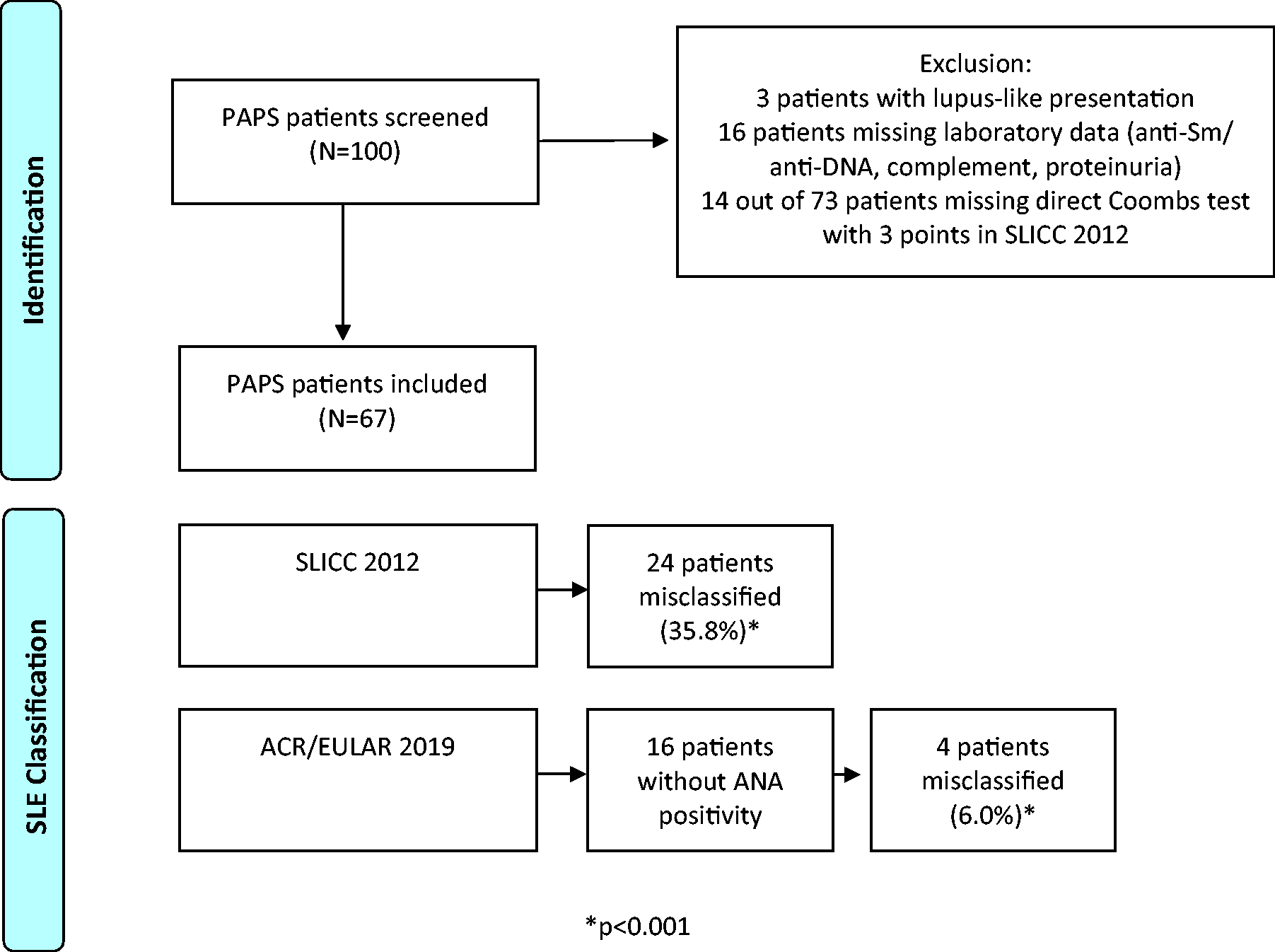
Flowchart of thrombotic PAPS patients submitted to SLE classifications.
Patient’s characteristics
All patients had thrombotic PAPS and 49.0% also had obstetric manifestations. Venous and arterial thromboses were detected in 71.6% and 38.8% of these patients, respectively. The great majority were female (89.6%) with median age at study inclusion of 45 years (35–53) and median PAPS duration of 13 years (8–19). Regarding laboratory criteria, ANA was the most common immunological criteria (76.1%) and LA was the most frequent aPL (95.5%). Three patients had drug related leukopenia, one with mycophenolate mofetil 8 and two with hydroxyurea 9 and, therefore, did not score in the hematological criteria in both SLE classifications. Main characteristics of the studied patients are shown in Table 1.
General characteristics of the 67 thrombotic PAPS patients.
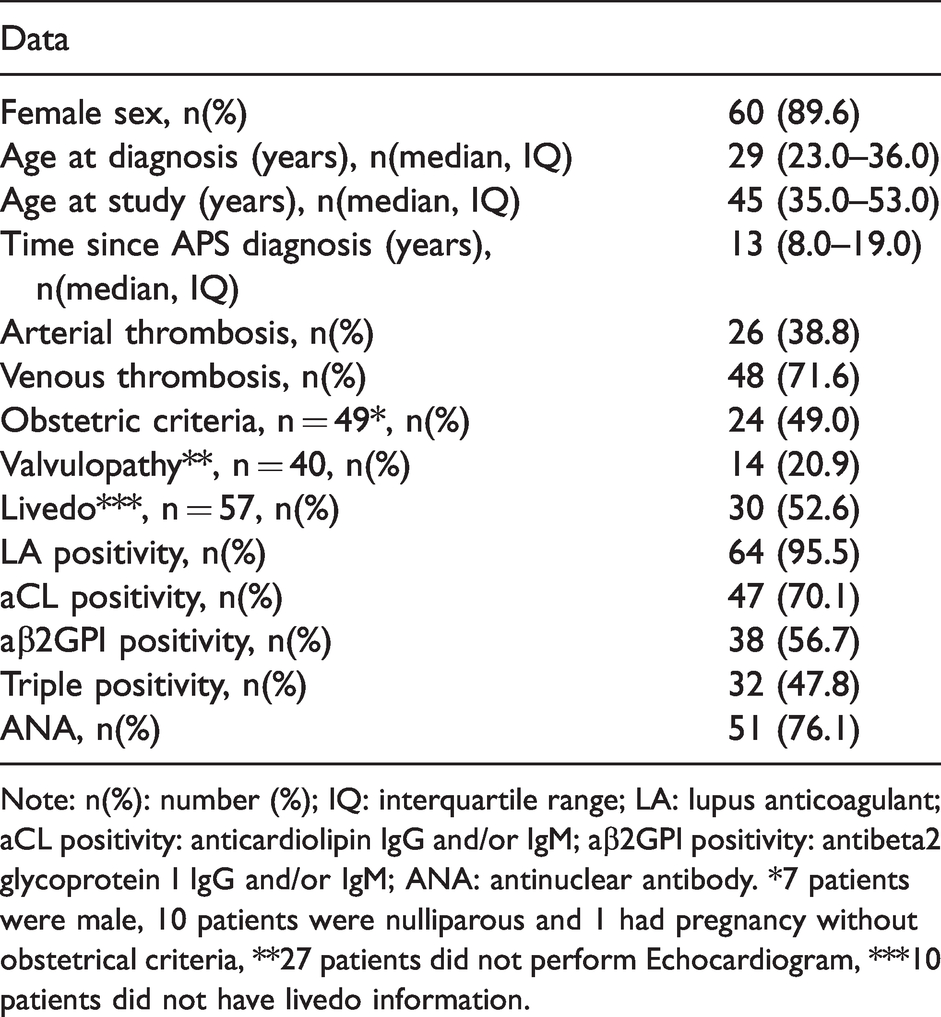
Note: n(%): number (%); IQ: interquartile range; LA: lupus anticoagulant; aCL positivity: anticardiolipin IgG and/or IgM; aβ2GPI positivity: antibeta2 glycoprotein I IgG and/or IgM; ANA: antinuclear antibody. *7 patients were male, 10 patients were nulliparous and 1 had pregnancy without obstetrical criteria, **27 patients did not perform Echocardiogram, ***10 patients did not have livedo information.
Misclassification rates according to the two different SLE classification criteria
Applying the ACR/EULAR 2019 criteria in our PAPS cohort, 94.0% of the studied patients were correctly classified as not having SLE. On the other hand, only 64.2% of the studied patients were correctly classified as not having SLE according to SLICC 2012 criteria. Misclassification rate was therefore only 6.0% in ACR/EULAR 2019 vs. 35.8% in SLICC 2012 (p < 0.001). Importantly, all 4 patients misclassified in ACR/EULAR 2019 were also misclassified in SLICC 2012.
Factors contributing to misclassification in this cohort
The comparison between misclassified patients and those correctly not classified resulted in higher frequencies of hematological domain for both criteria [ACR/EULAR 2019 (100% vs. 28.6%, p = 0.010) and SLICC 2012 (95.8% vs. 11.6%, p < 0.001)] (Table 2). Further analysis of hematological manifestations revealed that leukopenia (100% vs. 22.2%, p = 0.004 - for the ACR/EULAR 2019), and leukopenia/lymphopenia (91.7% vs. 7%, p < 0.001 - for the SLICC 2012) were more frequent in misclassified group (Tables 2 and 3).
Comparison of 67 thrombotic PAPS patients misclassified as SLE or correctly not classified as SLE according to the SLICC 2012 classification.
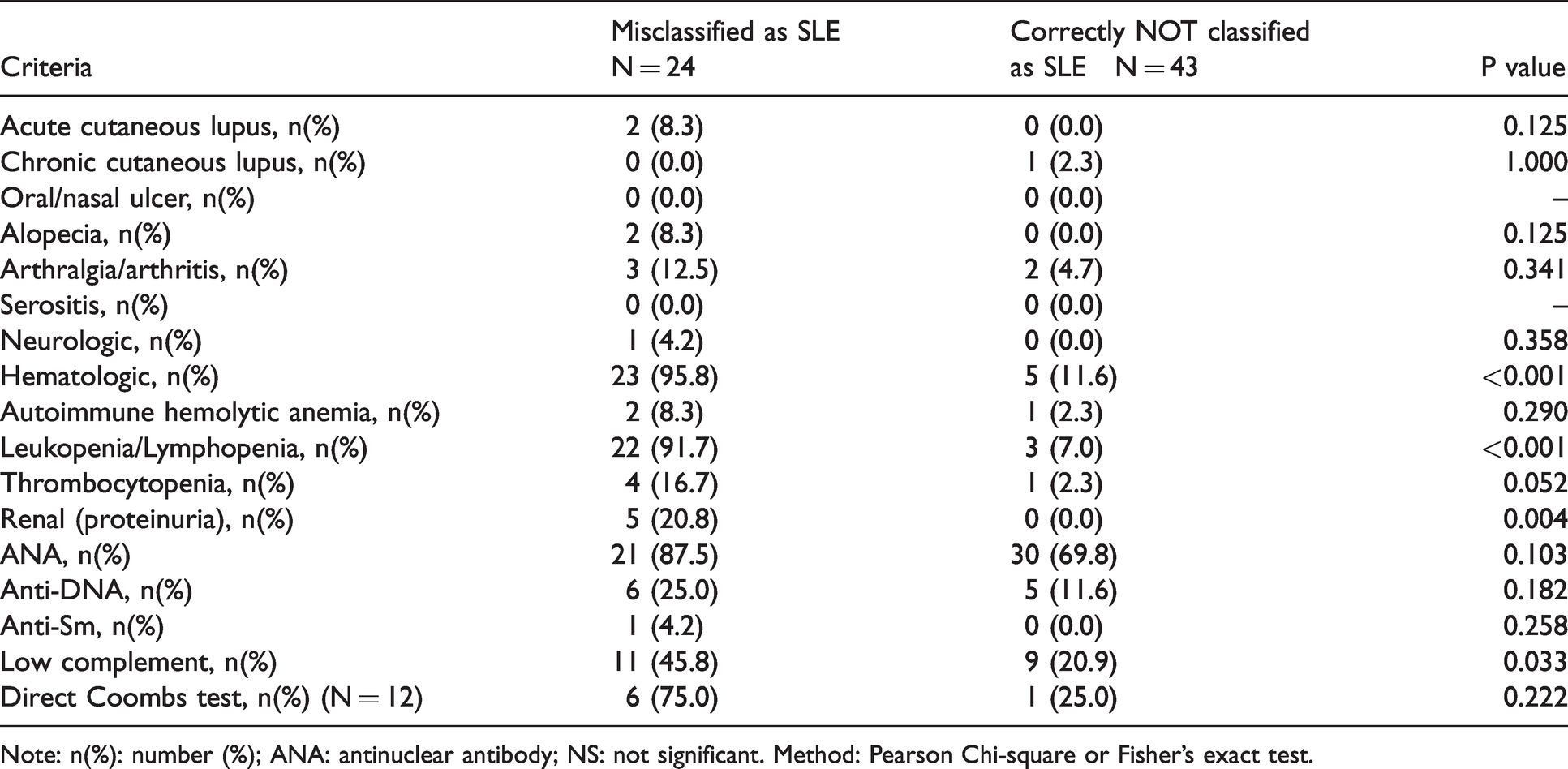
Note: n(%): number (%); ANA: antinuclear antibody; NS: not significant. Method: Pearson Chi-square or Fisher’s exact test.
Comparison of 67 thrombotic PAPS patients misclassified as SLE or correctly not classified as SLE according to the ACR/EULAR 2019 classification.
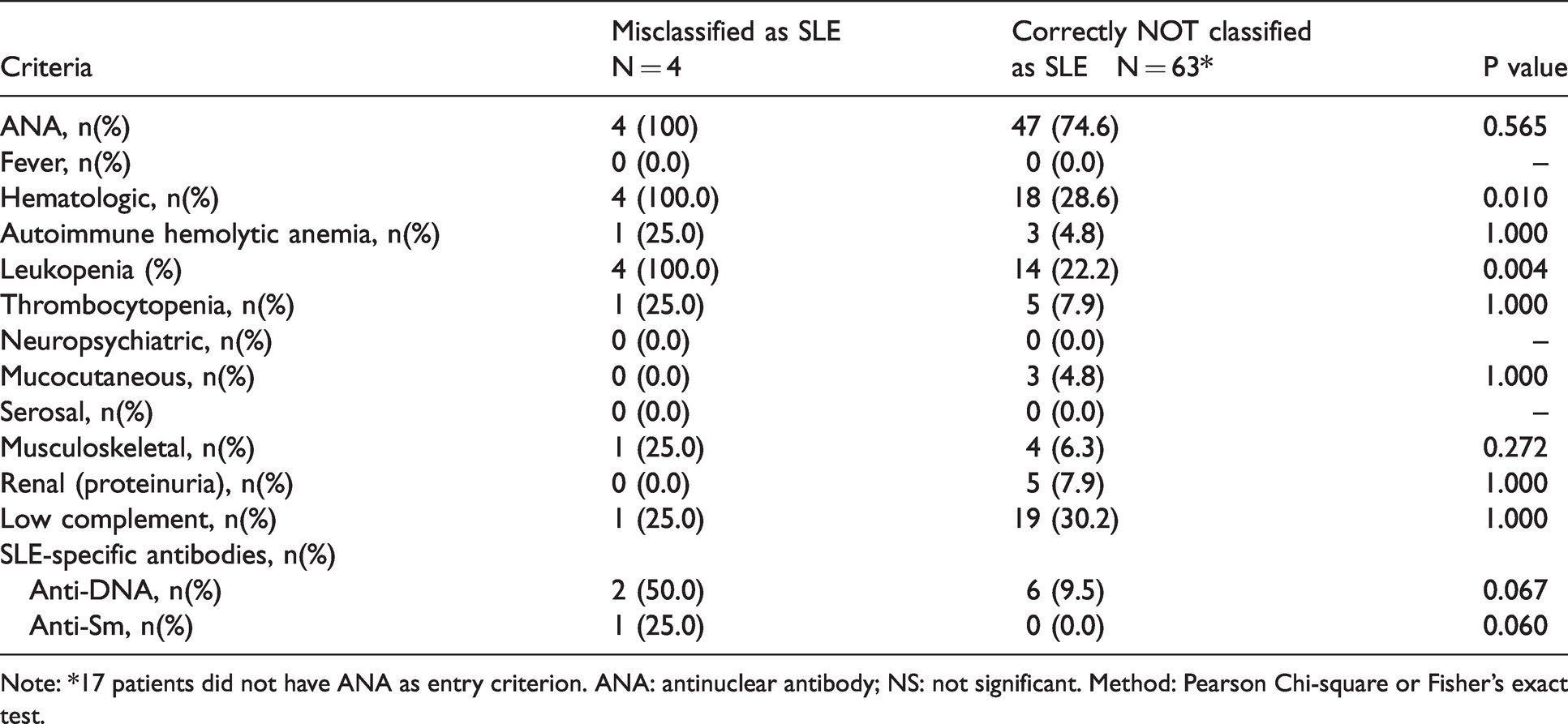
Note: *17 patients did not have ANA as entry criterion. ANA: antinuclear antibody; NS: not significant. Method: Pearson Chi-square or Fisher’s exact test.
The impact of hematological criteria in misclassification was evaluated in 11 patients who marginally fulfilled the SLICC 2012 criteria (4 points). All patients had one point due to hematological criteria and 10 of these 11 patients had leukopenia and/or lymphopenia.
In addition, the presence of proteinuria was more frequent in PAPS patients misclassified as SLE by the SLICC 2012 vs. those correctly classified as not having SLE (20.8% vs. 0%, p = 0.004) (Table 2). The highest value of proteinuria registered was 1.16 g/g. Proteinuria was elevated only once in 3 patients, without any identifiable cause. On the other hand, proteinuria was persistent in two patients, and both of them had biopsy-proven aPL-nephropathy. None of them had anti-dsDNA or anti-Sm antibodies, and 3 had positive ANA. Of note, these patients had a long median disease duration of 10 years (5–21.5).
Immunological criteria revealed that only low complement contributed to misclassification. Indeed, low complement was present more frequently in misclassified patients in SLICC 2012 than in those correctly not classified (45.8% vs. 20.9%, p = 0.033) (Table 2).
Lupus specific antibodies in PAPS patients misclassified as SLE
Anti-Sm was observed in only one patient that was misclassified in SLICC 2012 (criteria: lymphopenia, aPL, anti-Sm and ANA) and also in ACR/EULAR 2019. The median disease duration for this patient was 13 years.
Eleven patients were positive for anti-dsDNA measured by ELISA; of them, nine had persistently positive tests with high titers and eight had a positive Crithidia luciliae immunofluorescence confirmation test. Six patients were misclassified in SLICC 2012 with only 4 criteria, and 5 of them also had leukopenia. Two patients were misclassified in ACR/EULAR 2019. The median disease duration for patients with anti-dsDNA positivity was 13 years (7–19).
Description of misclassified patients in ACR/EULAR 2019
Four patients were both misclassified in ACR/EULAR 2019 and in SLICC 2012. All of them were anticoagulated with warfarin and Patient 1 was also treated with hydroxychloroquine as add-on therapy due to stroke recurrence. Characteristics of these patients are shown in Table 4.
Characteristics of the 4 patients misclassified in ACR/EULAR 2019.
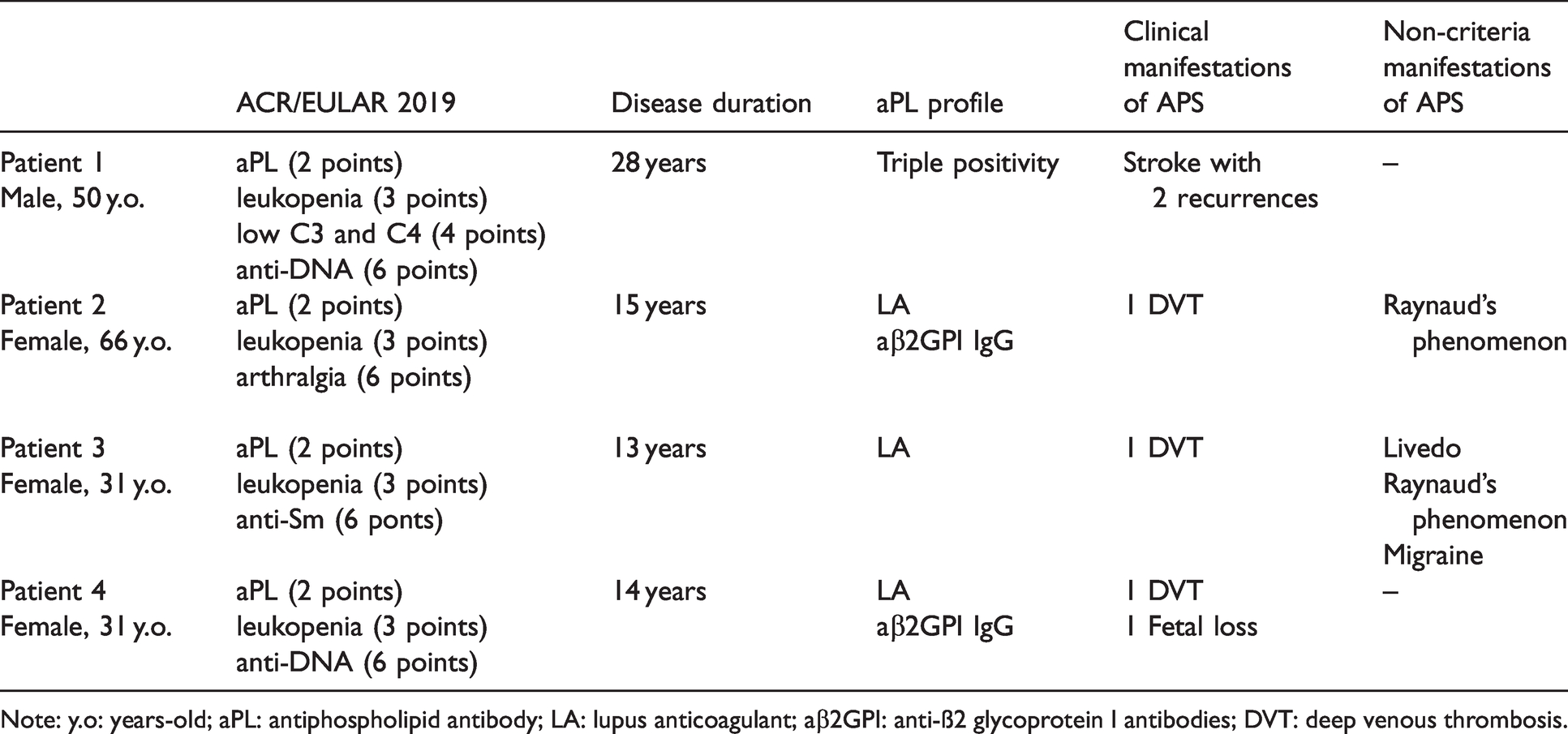
Note: y.o: years-old; aPL: antiphospholipid antibody; LA: lupus anticoagulant; aβ2GPI: anti-ß2 glycoprotein I antibodies; DVT: deep venous thrombosis.
Discussion
We found a significantly higher misclassification rate for the SLICC 2012 compared to the ACR/EULAR 2019 (p < 0.001). SLICC 2012 is well known for its high sensitivity (97%) and low specificity (84%). 4 Therefore, we should expect that SLICC 2012 should perform considerably worse than the ACR/EULAR 2019. Due to the highly heterogeneous spectrum of SLE manifestations, Adamichou et al. suggested that combining the two classification criteria could maximize SLE diagnostic assertiveness. 10 However, our data did not support this statement, since all 4 patients misclassified using ACR/EULAR 2019 were also misclassified with SLICC 2012.
Because both diseases may share clinical and immunological features, misclassification of PAPS patients as SLE in real life scenarios is troublesome. In fact, PAPS patients can meet up to 10 criteria in SLICC 2012 6 and up to 24 points in ACR/EULAR 2019. 5 The aPL positivity present in our patients automatically fulfilled one criterion in SLICC 2012 and 2 points in ACR/EULAR 2019. Our 4 misclassified patients in ACR/EULAR were well characterized as thrombotic PAPS with a long disease duration and follow-up. None of them had SLE clinical manifestations, but a 66 years-old woman with arthralgias not observed by examinator and without elevated acute-phase proteins. The Euro-phospholipid cohort had reported 8.1% of arthralgias and 2.8% of arthritis in PAPS, meanwhile another study had identified 41.0% of arthralgia and arthritis in PAPS. 11
ACR/EULAR 2019 criteria have never been validated in PAPS patients. Recently, Assan et al. validated this classification criteria in a Primary Sjögren Syndrome (PSS) cohort. They compared 49 SLE patients with 49 PSS and 26 overlap SLE/PPS. The criteria were met by 97.9% of patients with SLE and only by 4.2% with PSS, suggesting ACR/EULAR 2019 is a valid tool for distinguishing both diseases. 12 Our results also corroborate that ACR/EULAR 2019 is a valid tool to discriminate PAPS from SLE.
Hematologic manifestations were the most commonly observed clinical criteria in SLICC 2012 and ACR/EULAR 2019. Importantly, hematologic criteria comprise autoimmune hemolytic anemia, leukopenia, lymphopenia (not included in ACR/EULAR 2019) and thrombocytopenia.4,5 For the ACR 1997, hematologic criteria consisted of one clinical criterion 3 that was split into 3 different categories for the SLICC 2012. 4 This could be a reasonable explanation for those differences found in the aforementioned frequencies, as it may have increased SLICC 2012 sensitivity.
Based on the high frequency of hematological manifestations in patients misclassified as SLE, we should assume that hematologic criteria are the most important contributor factor to misclassification. When analyzing leukopenia/lymphopenia in SLICC 2012, we found 91.7% of misclassified patients present with either of these criteria vs. 7.0% of correctly not classified as SLE (p < 0.001). Interestingly, all eleven patients with a borderline score of 4 points in SLICC 2012 had one point from hematological criteria, of which 10 had leukopenia and/or lymphopenia. Besides, the 4 misclassified patients in ACR/EULAR 2019 had 3 points of leukopenia.
Renal criterion characterized by proteinuria was also an important item for misclassification in SLICC 2012, but not in ACR/EULAR 2019. This is a good example of clinical and laboratory overlap between SLE and PAPS. In terms of classification, this parameter has a high weight since proteinuria encompasses 4 points of the 10 needed to fulfill ACR/EULAR 2019 criteria, and one of the 4 required for classification using SLICC 2012. Two patients out of 5 patients had persistent proteinuria and both were diagnosed as aPL nephropathy on biopsy. This finding reinforces the importance of kidney biopsy for the correct diagnosis of lupus nephritis, especially in the setting of aPL positivity, since aPL nephropathy is an important differential diagnosis in this scenario.
Regarding immunological criteria, low complement was a contributor to misclassification in SLICC 2012, but not in ACR/EULAR 2019. The discrimination of ‘C3 and C4’ with 4 points and ‘C3 or C4’ with 3 points in ACR/EULAR 2019 may have improved specificity to this criterion. Paule et al. excluded from their analysis PAPS patients with immunological criteria considered SLE-specific, such as anti-dsDNA, anti-Sm, and with ANA values >1:320. 6 We chose to consider all consecutive patients diagnosed and classified as thrombotic PAPS, irrespective of their immunological data taking into consideration that even these antibodies are not 100% specific and they can be truly positive in patients without clinically manifested SLE. Ehrenstein et al. detected anti-dsDNA antibodies in 2 out of 30 PAPS patients (6.7%) using Crithidia luciliae immunofluorescence test. 13 Eleven patients (16.4%) of our study had anti-dsDNA positivity, and only 1 patient (1.5%) had isolated anti-Sm positivity without any clinical manifestations of SLE. Autoantibodies development is known to occur years before a clinical diagnosis 14 and, therefore, we cannot exclude that these patients will evolve to lupus diagnosis; however, the long term follow up of the PAPS patients evaluated herein minimizes this possibility.
To the best of our knowledge, this is the first paper to analyze the performance of ACR/EULAR 2019 classification criteria in a cohort of PAPS patients. Additionally, our cohort is composed of well-characterized thrombotic PAPS patients, which ensures a highly homogenous sample. Another strength of our study is the median PAPS duration of 13 years. Patients with recent SLE diagnosis usually perform worse in classification criteria than those with long standing disease, as it can take time for a patient to accrue enough items. 15 Therefore, based on the long-term follow-up of our studied patients, the risk of missing a diagnosis of SLE in our cohort was drastically minimized, besides the fact that SLE patients evolve to APS more frequently than the opposite. 16 On the other hand, we had some limitations mainly related to its retrospective design with potential missing data. Direct Coombs test was the main reason for laboratory exclusion. PAPS patients do not perform this test routinely unless there is clinical suspicion of hemolytic anemia.
In conclusion, the present study identified that ACR/EULAR 2019 has high accuracy in differentiating PAPS from SLE, whereas the SLICC 2012 incorrectly classified more than one third of the PAPS patients as having SLE. A correct classification of PAPS patients as not having SLE may impact proper management, avoiding unnecessary therapy and damage.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq #305242/2019-9 to EB and #306879/2018-2 to EFB) and Fundação de Amparo à Pesquisa do Estado de Sao Paulo (FAPESP 2015/03756-4 to EB).