
Abstract
Introduction
Lupus is a systemic condition fraught with health disparities. In the United States, patients with skin of color (P-SOC) experience lower quality health care and worse health outcomes compared to white patients. 1 Lupus occurs two-to-three times more often among women of color, and minorities develop symptoms at younger ages with more serious complications. 2 African-American ethnicity, malar rashes, and discoid lesions can predict long-term organ damage and mortality, 3 making it essential that clinicians accurately diagnose and promptly treat lupus in P-SOC.
Medical education contributes to the health disparities experienced among P-SOC with lupus. Educational materials underrepresent P-SOC, 4 a bias extending to resources specific to lupus, 5 and training programs contain few curricula dedicated to cutaneous findings in P-SOC. 6 These resources and learning experiences prepare practitioners to care for patients, and they impart unconscious biases while creating deficiencies in clinical skills when they exclude P-SOC.7,8 This can delay diagnosis for patients, can expose them to misdiagnosis, and can promote their distrust in the health care system. 9
Given the importance of recognizing lupus among P-SOC and the consequences of biases in education, we investigated practitioners’ confidence assessing lupus-related rashes in P-SOC. Secondarily, we analyzed which predictors are associated with greater clinical confidence and whether practitioners would like more teaching about these rashes in P-SOC.
Methods
We developed an anonymous survey to measure providers’ confidence assessing lupus-related rashes in P-SOC as well as practitioners’ characteristics that might influence confidence. Questions addressed career specialty, type and duration of practice, and practitioner race and ethnicity as well as the frequency of patients’ race and ethnicity encountered in clinical practice. We included factors that previous studies indicated may contribute to provider confidence when caring for P-SOC (9, 10, and 11). On a four-point Likert scale (1 (“none”), 2 (“very little”), 3 (“moderate”), and 4 (“a lot”)), providers ranked their confidence, experience, and previous training assessing any rash, any lupus-related rash, lupus-related rashes in patients with fair skin, and lupus-related rashes in P-SOC. We used the term “lupus-related rash” to reflect the variety of skin manifestations within the domain of cutaneous lupus as well as cutaneous findings associated with lupus not specifically classified as cutaneous lupus (e.g. urticaria). We also intended “lupus-related rash” to be a descriptive term for participants who may not be well-versed in the study of cutaneous lupus. We defined training as “education (such as nursing, physician assistant, or medical school, residency, fellowship, or continuing medical education) that included tools such as reading, image reviews, or lectures that assisted practitioners in diagnosing lupus-related rashes in P-SOC.” Our final question asked if providers would like more education in assessing lupus-related rashes.
In February and March 2020, we invited health professionals in the fields of rheumatology, dermatology, and internal medicine from the greater St. Louis area (Missouri, United States) to complete the survey. We shared surveys electronically via email listservs of rheumatology fellows and providers, dermatology residents and practitioners, primary care providers, and internal medicine residents affiliated with Washington University School of Medicine and its community network as well as in-person at rheumatology continuing medical education conferences. We instructed practitioners to take the survey once if they received multiple invitations. We planned to invite additional providers in primary and hospitalist care, but the onset of the COVID-19 pandemic ended recruitment. Of the 480 invited providers, 132 (27.5%) answered the survey. This value underestimates the response rate as the anonymity of our study precluded reviewing the names of invitees and correcting for duplicate requests. Responses were stored in the Qualtrics survey platform (Seattle, Washington). The study protocol was in compliance with the World Medical Association Declaration of Helsinki, and the Washington University School of Medicine Institutional Review Board approved our study with waived informed consent (approval 202001144).
A linear mixed effects model compared practitioners’ mean confidence levels among any rash, any lupus-related rash, lupus-related rashes in fair skin, and lupus-related rashes in P-SOC. This model accounted for correlated ratings of confidence from the same practitioner and assumed missing data at random; incomplete data was used in the mixed model analysis. Linear contrasts compared mean confidence level pairwise. A univariate linear regression model assessed the association between confidence assessing lupus-related rashes in various skin tones and the other potential predictors. Predictors with p-values smaller than 0.2 in the univariate analysis were incorporated in the multivariate linear regression model analysis. We used analysis of covariance (ANCOVA) with a backward selection method to construct the final model. We examined for multicollinearity with variance inflation factors and condition indices. Last, we determined least squares confidence means for each Likert scale level of experience (i.e., “none,” “very little,” “moderate,” and “a lot”) in diagnosing lupus-related rashes in P-SOC and calculated the difference of least squares confidence means between pairwise comparisons of experience levels. All the statistical tests were two-sided, and analyses were performed with SAS 9.4 (SAS Inc, Cary, NC).
Results
Practitioners’ personal and practice characteristics.
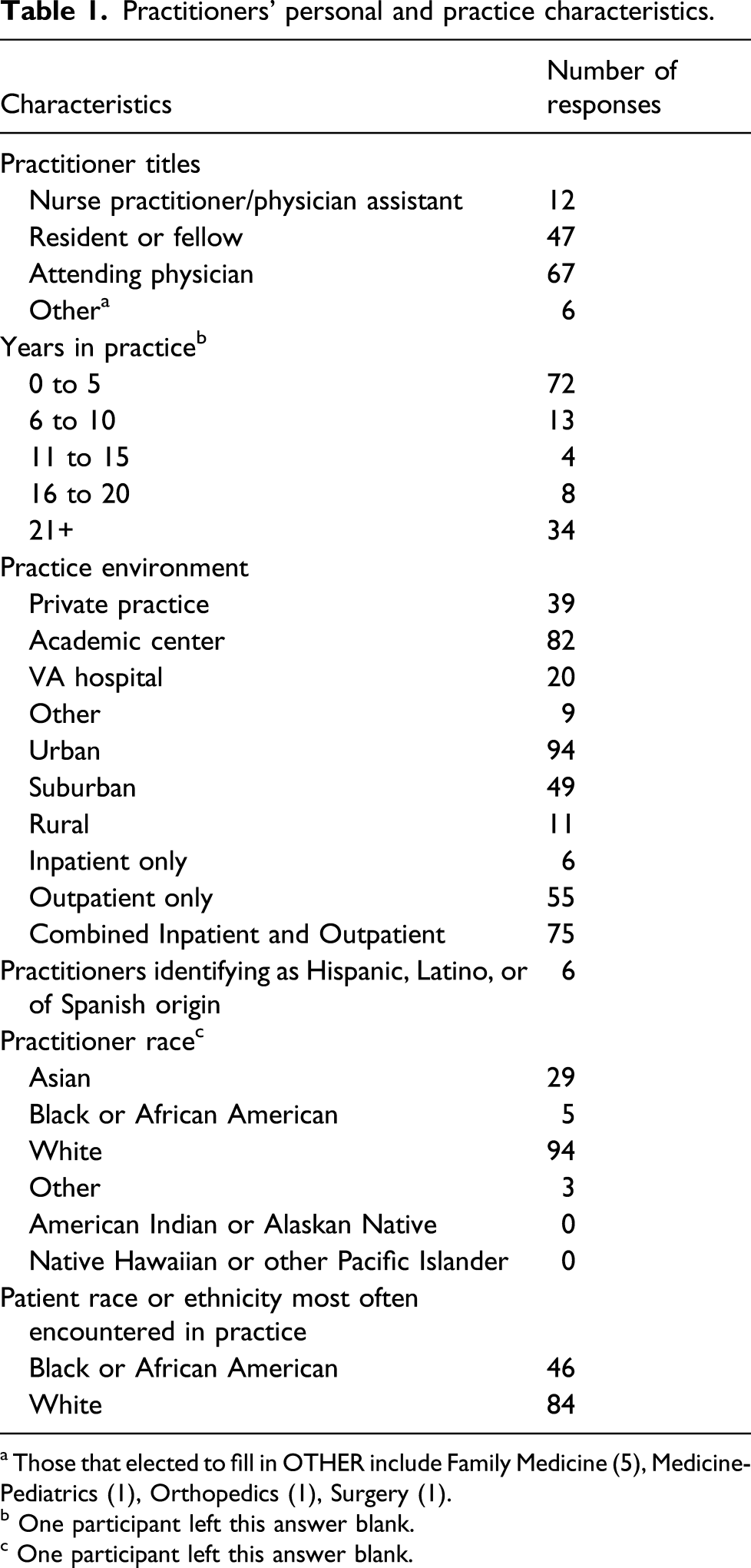
a Those that elected to fill in OTHER include Family Medicine (5), Medicine-Pediatrics (1), Orthopedics (1), Surgery (1).
b One participant left this answer blank.
c One participant left this answer blank.
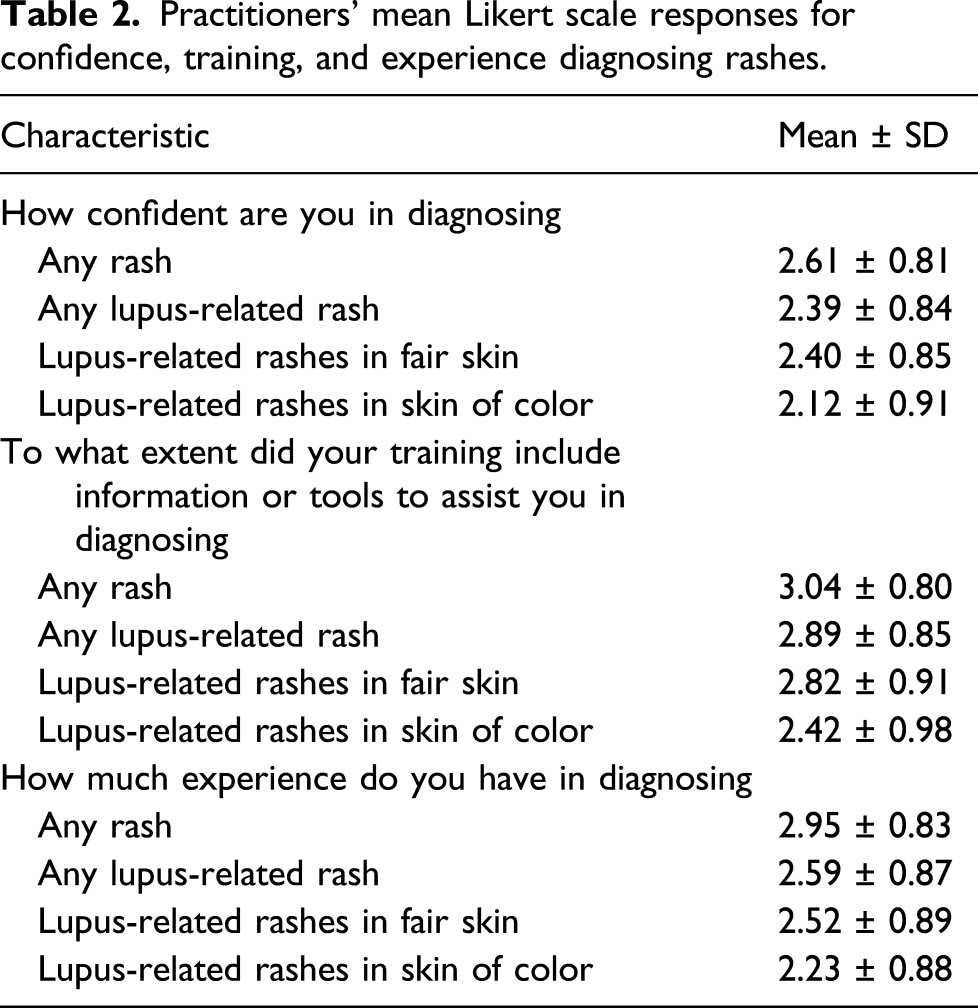
Practitioners’ mean Likert scale responses for confidence, training, and experience diagnosing rashes.
Univariate association analysis with provider confidence assessing lupus-related rashes in patients with skin of color (P-SOC).
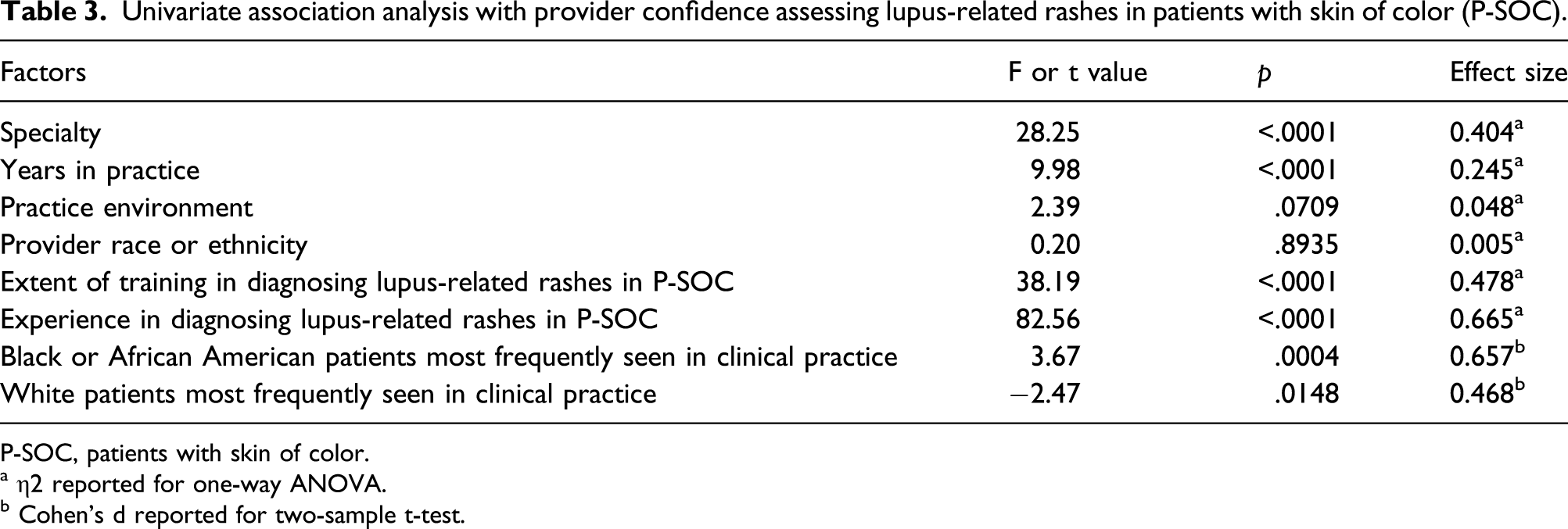
P-SOC, patients with skin of color.
a η2 reported for one-way ANOVA.
b Cohen’s d reported for two-sample t-test.
The difference of least squares confidence means between pairwise comparisons of levels of experience showed that for every iterative increase in experience, there is an associative rise in confidence with assessing lupus-related rashes in P-SOC, indicating a dose–response relationship between experience and confidence: the larger the increase in experience, the greater the gain in confidence (supplement).
When asked about more training to diagnose lupus-related rashes in P-SOC, 93% of participants (N = 132) indicated interest in additional education.
Discussion
Our study demonstrates that practitioners have lower confidence diagnosing lupus-related rashes in P-SOC than in patients with fair skin. Clinicians reported the least amount of confidence assessing rashes in patients with lupus and skin of color compared to those with any rash, any lupus-related rash, or lupus-related rashes in patients with fair skin. Univariate analysis demonstrated associations between several predictors and confidence, and experience with patients of color and lupus-related rashes uniquely correlated with provider confidence in the multivariate model. These findings represent the first investigation of practitioners’ confidence assessing rashes specific to lupus in P-SOC and of predictive factors that may influence provider confidence.
Our results complement prior research that highlights practitioners’ low confidence and clinical skills diagnosing cutaneous disorders in P-SOC. Dermatology providers previously reported less confidence evaluating common skin diseases among P-SOC,8,11 and an assessment of medical students’ clinical abilities revealed less skill naming squamous cell carcinoma, urticaria, and contact dermatitis in P-SOC. 12 These findings suggest that practitioners lack both confidence and clinical skill when caring for P-SOC, highlighting provider-specific deficiencies that contribute to poor health outcomes.
The intersection of skin color and a diagnosis of lupus holds clinical importance. Our findings indicate that practitioners have the least confidence assessing rashes in patients with a diagnosis of lupus and skin of color compared to any rash or lupus-related rash in patients with fair skin. P-SOC with lupus experience delays in diagnosis, more severe complications, and worse health outcomes compared to white patients.2,3 Therefore, it is critical that providers are exposed to learning experiences that develop their clinical confidence and acumen in recognizing the manifestations of lupus among P-SOC.
Previous research has shown that curricular modules can improve clinicians’ confidence in diagnosing rashes in P-SOC. 7 In our study, educational tools from practitioners’ training predicted confidence in the univariate model but were not associated with confidence in the multivariate model. This implies that educational materials dispensed during an initial training period insufficiently prepare clinicians for treating lupus-related rashes in P-SOC in long-term practice.
On the other hand, we found that continued experience improved confidence. This factor represents more than years in practice or clinical specialty because neither career duration nor specialty was associated with practitioners’ confidence in the multivariate model. Instead, it may more accurately reflect the types of patient experiences encountered in clinical practice. Trainees reflect that spending time in dermatology clinics dedicated to the care of P-SOC improves their diagnostic acumen in assessing cutaneous findings in P-SOC. 13 Additionally, clinics specialized in the care of patients with lupus also improve patients’ satisfaction, trust in health care providers, and health outcomes.9,10,14 In combination with dedicated didactic teaching, such clinical experiences increase trainees’ exposure to less common patient populations and conditions, thereby consolidating their learning and enhancing their training. Independently practicing clinicians likely would appreciate similar opportunities in continuing medical education as more than 90% of survey respondents voiced interest in additional education about lupus-related rashes in P-SOC.
We included representatives from multiple specialties, namely, rheumatology, dermatology, and internal medicine, to strengthen the results of our study. We selected these specialties because they frequently treat patients with lupus and because it improves the generalizability of our results. Furthermore, our regression analyses measured the association of practitioner confidence with factors previous studies indicated might predict confidence in diagnosing lupus-related rashes in P-SOC, thereby grounding our methods in previous research.9–11
Our study has several limitations. It was underpowered to detect an association between practitioner race and ethnicity with clinical confidence. We planned to recruit additional providers in hospital medicine and primary care but were limited by the COVID-19 pandemic. Additionally, internal medicine resident trainees comprised almost one-third of participants. With limited knowledge and insight into their abilities, novices can overestimate their skills, 15 which may have influenced their survey responses. Last, this study evaluated confidence, which does not equate to clinical skill.
In future research, our approach should be applied to dermatologic manifestations of other autoimmune rheumatic diseases where P-SOC suffer worse outcomes than white patients. Educators should develop assessment tools to quantify practitioners’ competence assessing rashes in P-SOC to facilitate education and training. Also, medical educators should investigate which educational and clinical training interventions best prepare providers and trainees to care for P-SOC with lupus, paying close attention to clinics that specialize in the care of lupus and P-SOC where these approaches most fertilely intersect.
These findings show that a significant difference exists in provider confidence diagnosing lupus-related rashes in patients with fair skin compared to P-SOC among rheumatologists, dermatologists, and internists. Medical resources and training experiences that favor fair skin contribute to this finding as additional clinical experience with P-SOC is associated with greater confidence. Therefore, a combination of instructional teaching as well as clinical experiences with patients of color could improve practitioners’ confidence and patients’ health outcomes. In devising strategies to enhance practitioners’ experience with lupus and P-SOC, the profession of medicine can reduce the health inequities experienced by this vulnerable patient population.
Footnotes
Acknowledgments
We thank Drs. Aisling Doyle, MD, Iris Lee, MD, Muithi Mwanthi, MD, PhD, and Andrea Ramirez-Gomez, MD for helping us develop our survey. We thank Drs. Dominique Cosco, MD, Heather Jones, MD, and Prabha Ranganathan, MD, MSCI for supporting survey distribution.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Washington University in St Louis Mentors in Medicine Program [grant number 2020].