
Abstract
Background
Early diagnosis and treatment of myocardial affection in patients with systemic lupus erythematosus (SLE) are crucial.
Objectives
To evaluate the ventricular systolic function in juvenile-onset systemic lupus erythematosus (j-SLE) patients by 3-D speckle tracking echocardiography (3D-STE) and to determine the predictors of left ventricular (LV) dysfunction if present.
Methods
Twenty-six SLE patients without heart failure and 21 healthy controls were studied by standard echocardiogram and 3D-STE. Conventional parameters included LV ejection fraction (EF), fractional shortening (FS), and mitral annular plane systolic excursion (MAPSE). Global LV strain (GLS) and global area strain (GAS) were obtained by 3D-STE. Medical records, including diagnosis criteria, duration of disease, and SLE disease activity index (SLEDAI) were evaluated.
Results
The mean age was similar in patients and controls 11.42 vs 11.48 years p = 0.93. The mean duration of the disease was 1.87 ± 1.02 years and SLEDAI ranged from 0 to 9. By conventional and tissue Doppler imaging echocardiography, only MAPSE was significantly lower in SLE patients compared to controls (14.56 vs 18.46 mm, p < 0.001). By 3D speckle tracking echocardiography, GLS and GAS were significantly reduced in SLE patients compared to controls (−15.07 vs −19.9.4%, −34.6% vs −39.7%, respectively, p < 0.001). Multiple linear regression and ROC analyses indicated that the SLEDAI score was the only predictive factor for the left ventricular remodeling.
Conclusions
These results indicate that early subclinical LV dysfunction occur in jSLE patients even with normal EF and SLE disease activity might be a potential driver for LV deformation.
Key Points
jSLE had low LV GLS and GAS by 3-D STE. SLEAI is the best predictor for low LV GLS in jSLE.
Introduction
Systemic lupus erythematosus (SLE) is a multisystem autoimmune connective tissue disease, it is characterized by the production of autoantibodies against nuclear antigens and deposition of immune-complexes in several tissues particularly the kidneys, the central nervous system (CNS), cardiovascular system, and hematopoietic system. 1 Approximately 20% of cases occur in childhood. 2 The clinical presentation and prognosis of jSLE is frequently more severe than adult-onset disease and cardiac involvement is estimated to occur in more than 50% of cases and may involve the conduction system, pericardium, coronary arteries, and valves.3,4 The clinical symptoms are non-specific, standard transthoracic echocardiography (TTE) often lacks the sensitivity to detect subclinical ventricular dysfunction 5 and traditional echocardiographic methods that rely on geometric model assumptions to estimate systolic function are often imprecise. 6 As the left ventricular myofibers have a complex spatial orientation and contract simultaneously in different directions, addition of the third dimension for myocardial deformation analysis is required. 7 Tissue Doppler and two- and three-dimensional speckle tracking echocardiography (STE) are valuable techniques that allow the evaluation of ventricular and atrial myocardial deformation by dimensionless parameters without the need of any geometrical assumption. Therefore, it is considered to be a very promising tool for assessment of regional and global atrial and ventricular systolic and diastolic functions. 8 Since tissue Doppler methodology is known to be angle-dependent and 2-D STE can only track motion within the imaging plane, this adversely affects tracking when speckles move out of the imaging plane. 9 Three-dimensional STE allows accurate and faster analysis of deformation when compared with 2-D STE and might represent a viable alternative in the evaluation of global LV function. 10 The current study aimed to evaluate myocardial functions in patients with juvenile-onset SLE who had no cardiac symptoms using conventional, tissue Doppler imaging and three dimensional STE.
Patients and methods
This is a cross-sectional case-controlled study for children diagnosed as juvenile-onset SLE who have been followed in Rheumatology Clinic, Cairo University Specialized Pediatric Hospital during the period from June 2017 to June 2019. All patients of both gender younger than 18 years who fulfilled at least four of the updated revised criteria of the American College of Rheumatology for SLE diagnosis 11 and New York heart association (NYHA) functional class I (no cardiac symptoms and without limitation of physical activity) were included in the study. Twenty-one age and sex healthy matched controls were selected. Each participant who fulfilled the inclusion criteria was subjected to a detailed examination and medical history was taken concerning steroids and immunomodulators therapy, as well as the frequency of relapses. The general examination included body weight, height, body surface area, heart rate, and systemic blood pressure. An informed consent was obtained from each participant. Collecting data included different recent laboratory investigations and medications; anti-inflammatory or immunomodulators, from patient’s files. Disease activity have been defined on the basis of SLEDAI scores: no activity on remission (SLEDAI = 0), mild activity (SLEDAI = 1–5), moderate activity (SLEDAI =6 –10), high activity (SLEDAI = 11–19), and very high activity (SLEDAI ≥ 20). 12 Echocardiographic examination was performed by a pediatric cardiologist familiar with TDI and 3D-STE for all cases in supine and left lateral positions using General Electric (Vivid-7, Horten, Norway) machine with a 3 and 5 MHz transducers according to the age of the patient and having tissue velocity imaging capabilities specification. The ECG cable was connected to the ultrasound machine to define and to time the cardiac cycle events; the beginning of QRS complexes was used as a reference point. Conventional echocardiography and Doppler velocities were performed according to American guidelines of echocardiography. 13 Mitral annular plane systolic excursion (MAPSE) was performed at lateral mitral annulus in apical four chamber view. Tissue Doppler imaging (PW-TDI) was done and care was taken to increase the frame rate to more than 180 frames/s to improve temporal resolution; moreover, care was taken also to align the ultrasound beam parallel to the target wall during measurements. To reduce the effect of respiration on tissue velocities, three cardiac cycles were recorded and the average velocity was calculated. The following parameters were measured: Systolic (S’) and diastolic (E’, A’, E’/A’ ratio) myocardial velocities at the basal segments of the lateral LV wall, septal wall. As the left ventricle contracts in systole, it shortens in the longitudinal direction (negative strain) and this change in length is called the strain or deformation. Longitudinal shortening is responsible for 60% of the left ventricular ejection and is the most important component of systolic function. Global longitudinal strain (GLS) is more reliable for assessing the systolic function. Myocardial deformation is expressed as strain, which represents the fractional or percent change of a region of interest from its original dimension (change in length between two points). This global longitudinal shortening varies from −15% to −30% from base to apex.14,15 3-D STE was obtained through a full volume acquisition of the LV to avoid the foreshortening which is a major problem for apical imaging and may underestimate ejection fraction. The depth and volume size were adjusted to obtain a temporal resolution higher than 30 volumes/s. All data sets were analyzed off-line using commercially available software (Echo PAC version 11; GE). The software automatically identified the LV cavity endocardial border in 3D and provided the LV volumes and EF. Subsequently, an automatic trace of the epicardial border was displayed to set the region of interest required to calculate the LV 3D myocardial deformation parameters. The 3D GLS and global area strain at end-systole was calculated. If three or more segments were rejected, global strain values were not calculated, and these patients were excluded from any further analysis. 16
Statistical analysis of the data
Data were fed to the computer and analyzed using IBM SPSS software package version 20.0. (IBM Corp, Armonk, NY) Qualitative data were described using number and percent. Quantitative data were described using range, mean, standard deviation, and median. Significance of the obtained results was judged at the 5% level. The used tests were chi-square test for categorical variables, to compare between different groups. Student t-test for normally distributed quantitative variables, to compare between two studied groups, Mann–Whitney test for abnormally distributed quantitative variables, to compare between two studied groups and Pearson coefficient to correlate between two normally distributed quantitative variables. Ordinal data are presented as number and percentages and intergroup differences are compared with the chi-squared test for trend. Univariate and multivariate linear regression analyses were used to investigate possible associations between echocardiographic parameters on the 3D-STE and other studied variables. At first step, the linear correlation was performed in order to detect the impact of the most common variables as age of disease onset, SLEDAI, hemoglobin level and estimated systolic pulmonary artery pressure as well as duration of steroid and hydroxychloroquine therapy on the left ventricular performance in SLE patients by non-conventional echocardiography study. Then multivariate regression models were selected based on the statistical positive findings with linear correlation. Receiver-operating characteristic curve (ROC) is generated by plotting sensitivity (TP) on Y axis versus 1-specificity (FP) on X axis at different cut off values. The area under the ROC curve denotes the diagnostic performance of the test. Area more than 50% gives acceptable performance and area about 100% is the best performance for the test.
Results
Clinical and laboratory characteristics of the study population
Comparison of clinical, laboratory, conventional, and tissue Doppler echocardiographic parameters of SLE and controls (mean ± SD) (min-max).
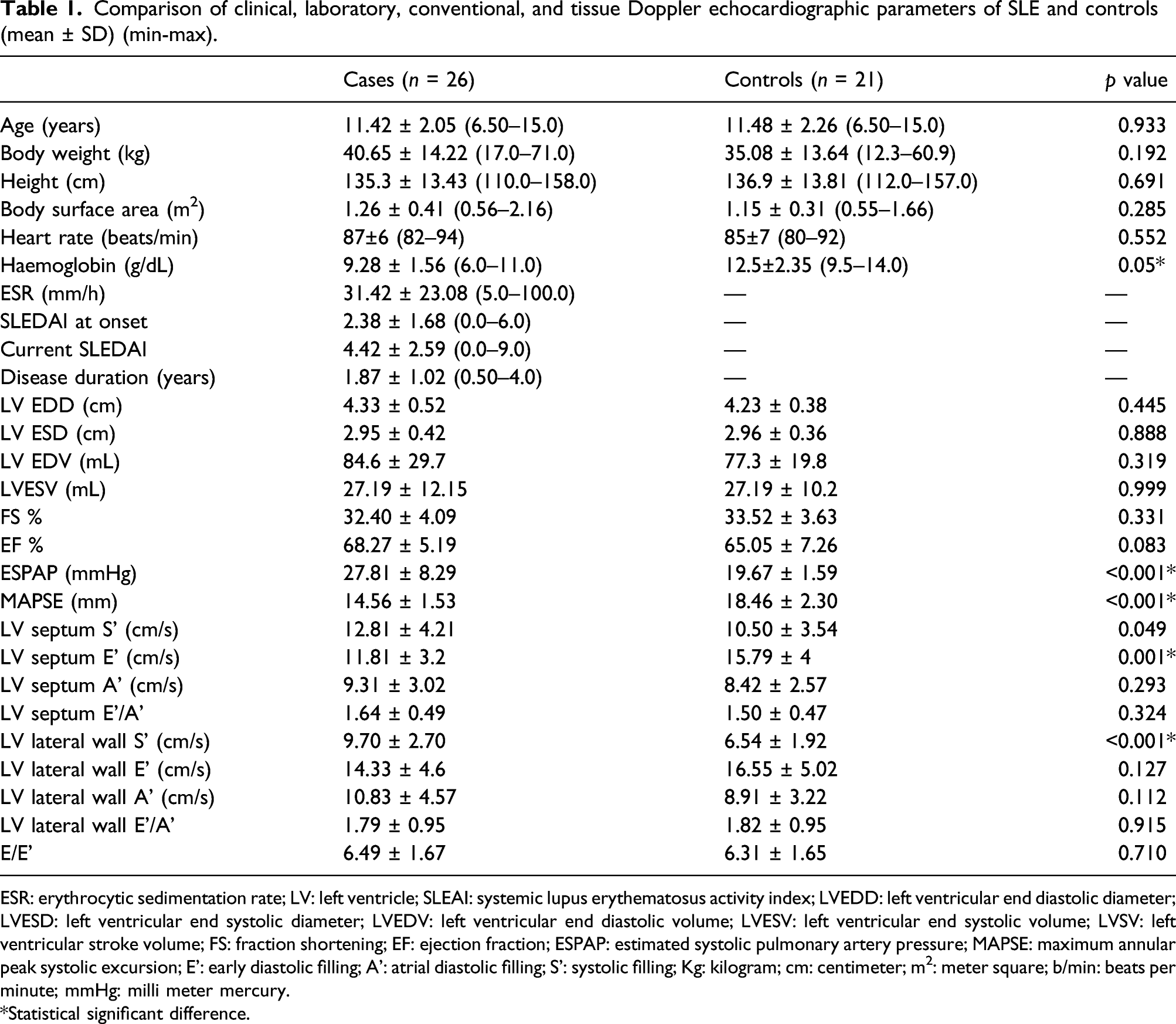
ESR: erythrocytic sedimentation rate; LV: left ventricle; SLEAI: systemic lupus erythematosus activity index; LVEDD: left ventricular end diastolic diameter; LVESD: left ventricular end systolic diameter; LVEDV: left ventricular end diastolic volume; LVESV: left ventricular end systolic volume; LVSV: left ventricular stroke volume; FS: fraction shortening; EF: ejection fraction; ESPAP: estimated systolic pulmonary artery pressure; MAPSE: maximum annular peak systolic excursion; E’: early diastolic filling; A’: atrial diastolic filling; S’: systolic filling; Kg: kilogram; cm: centimeter; m2: meter square; b/min: beats per minute; mmHg: milli meter mercury.
*Statistical significant difference.
Comparison of body mass index (BMI) and blood pressure centiles of SLE and controls.
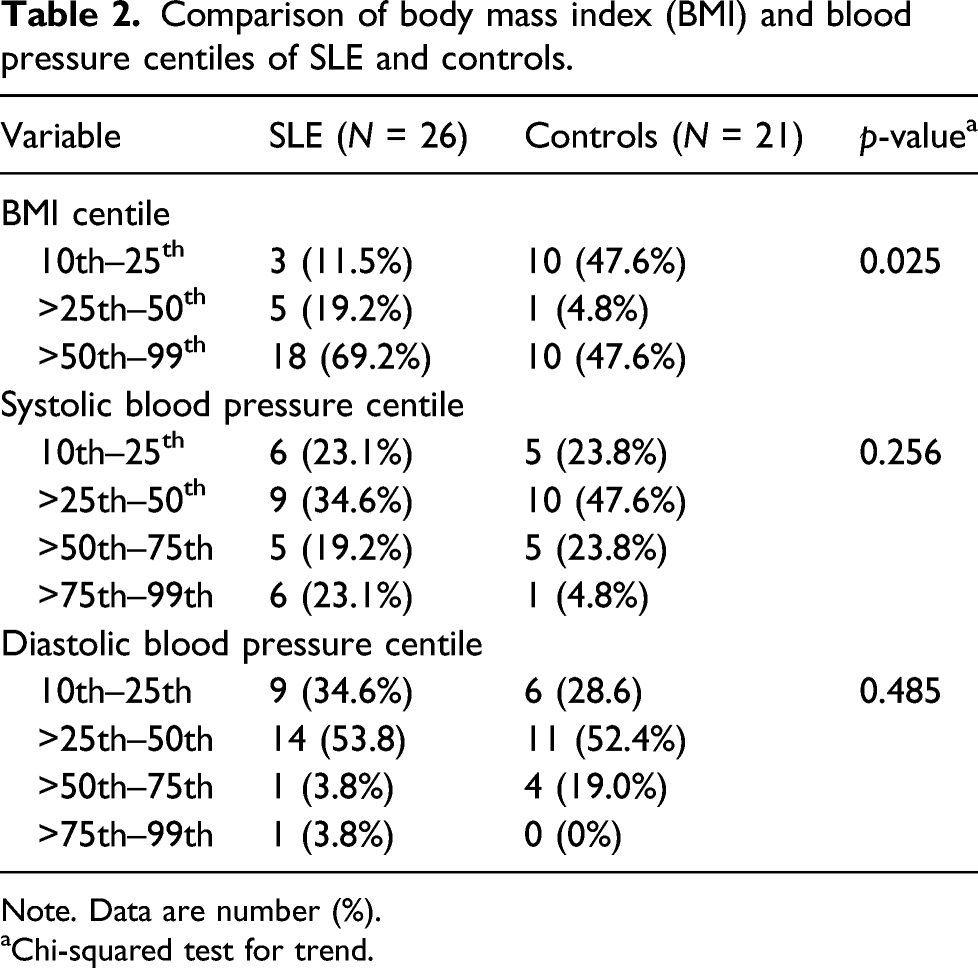
Note. Data are number (%).
aChi-squared test for trend.
Conventional and tissue Doppler echocardiographic parameters of left ventricle
There was no statistically significant difference between patients and controls regarding conventional LV dimensions and systolic function by M-mode. On the other hand, mitral valve excursion from base to apex assessed by MAPSE was lower than controls’ (p< 0.001). There was mild LV diastolic dysfunction affecting septum more than lateral wall as septal E’ was lower than controls (p < 0.001) (Table 1).
3D volumetric study, global longitudinal, and area strains of jSLE patients and controls (mean ± SD) (non-conventional echocardiographic parameters).
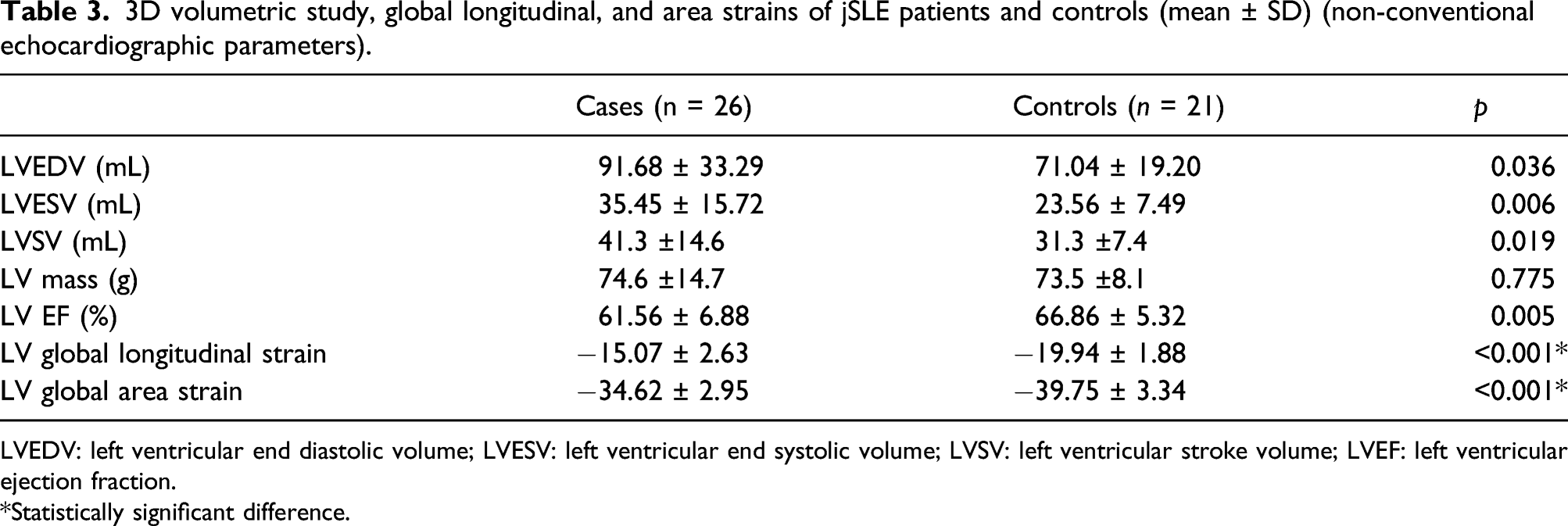
LVEDV: left ventricular end diastolic volume; LVESV: left ventricular end systolic volume; LVSV: left ventricular stroke volume; LVEF: left ventricular ejection fraction.
*Statistically significant difference.
Clinical correlations
By univariate analysis
SLE disease activity index at the onset of the illness was significant negative correlated with the age of the onset of the disease and with LV fraction shortening assessed by conventional method. On the other hand, higher disease activity correlated with decreased (less negative) myocardial deformation as global left ventricular systolic strain (GLS) and global area strain (GAS) were impaired (Figure 1). Various correlations with SLE activity index: (a) SLEAI at onset of the disease with the age at disease onset, (b) SLEAI at onset of the disease with left ventricular fraction shortening assessed by conventional method, (c) SLE activity at current status with left ventricular global longitudinal strain (GLS), and (d) SLE at current with left ventricular global area strain (GAS). SLE disease activity index (SLEDAI).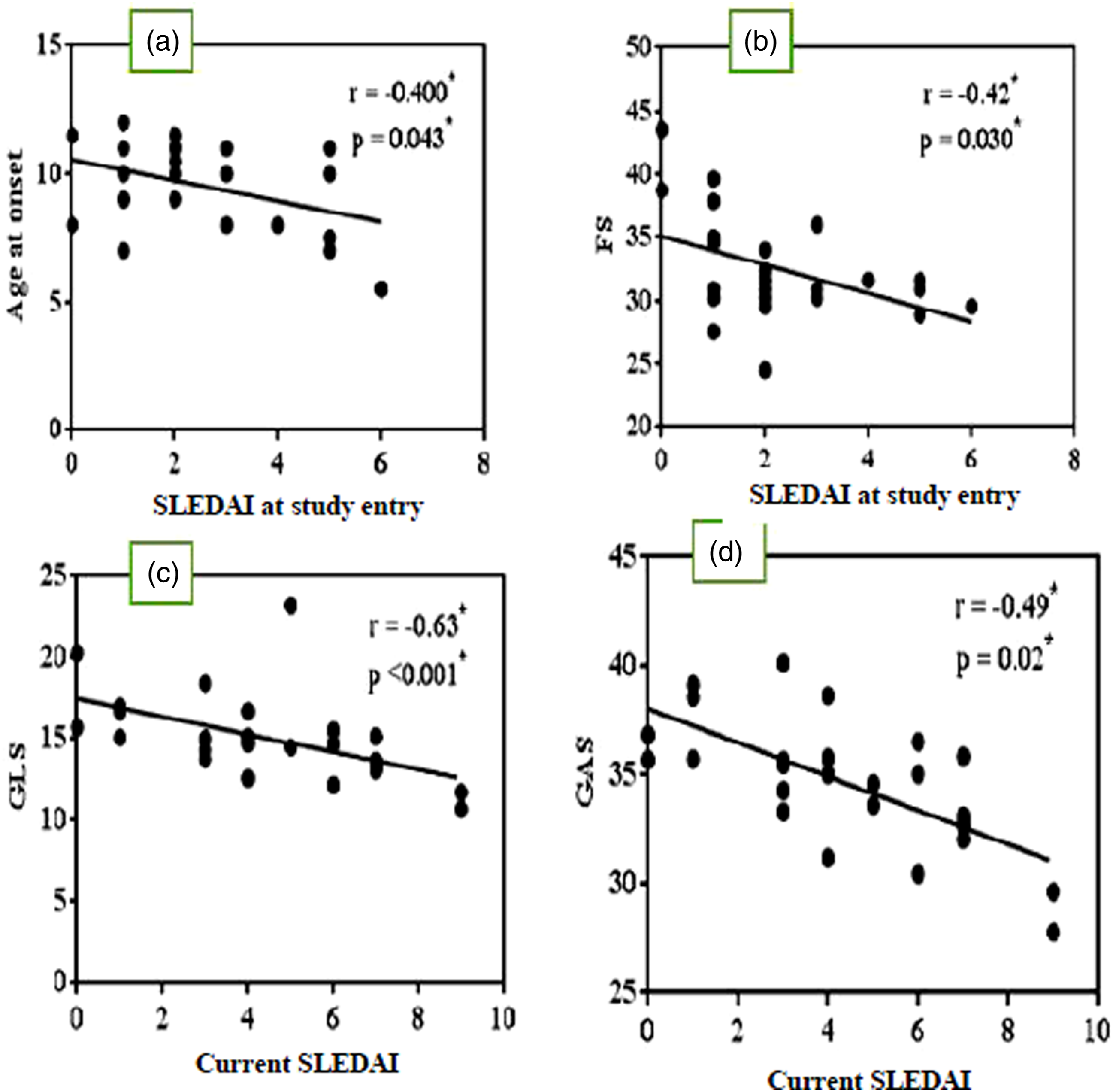
By multivariate analysis
Multiple regression analysis for identifying factors influencing left ventricular function assessed by 3-dimensional speckle tracking echocardiography.
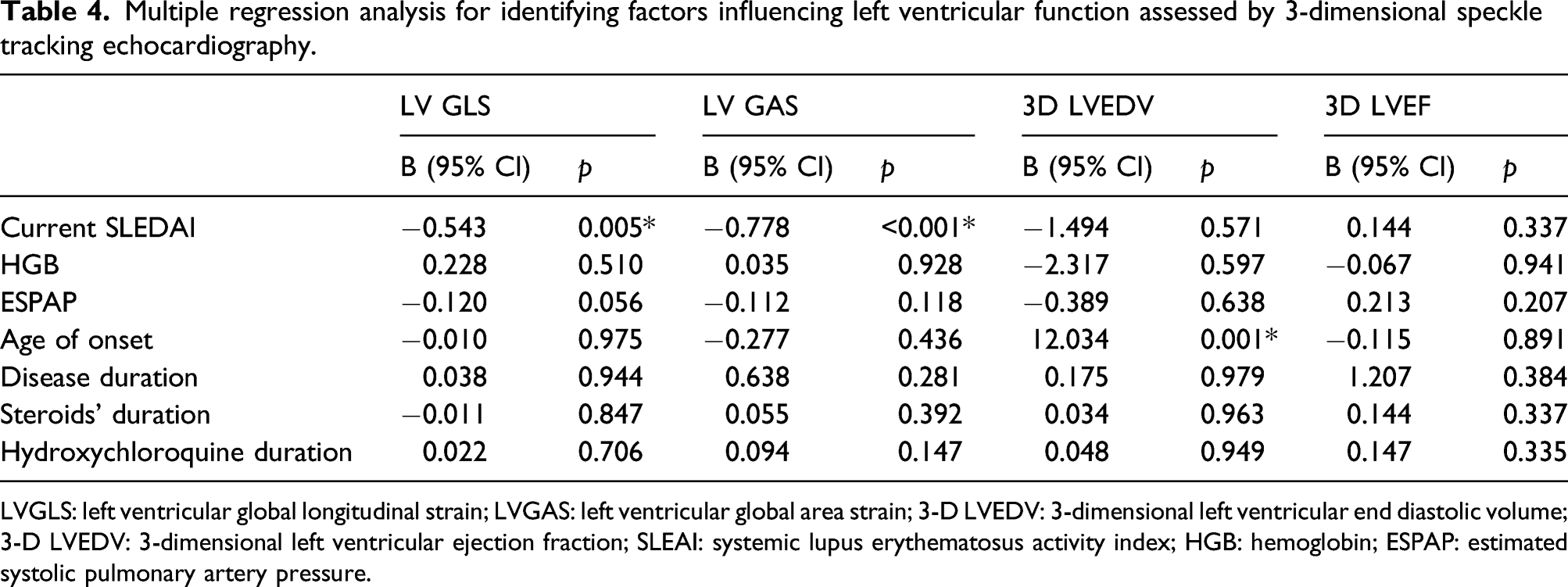
LVGLS: left ventricular global longitudinal strain; LVGAS: left ventricular global area strain; 3-D LVEDV: 3-dimensional left ventricular end diastolic volume; 3-D LVEDV: 3-dimensional left ventricular ejection fraction; SLEAI: systemic lupus erythematosus activity index; HGB: hemoglobin; ESPAP: estimated systolic pulmonary artery pressure.
Predictors of left ventricular deformation in jSLE
Predictors of LV Global longitudinal strain (GLS) affection assessed by 3-D STE at a cutoff value < −14.
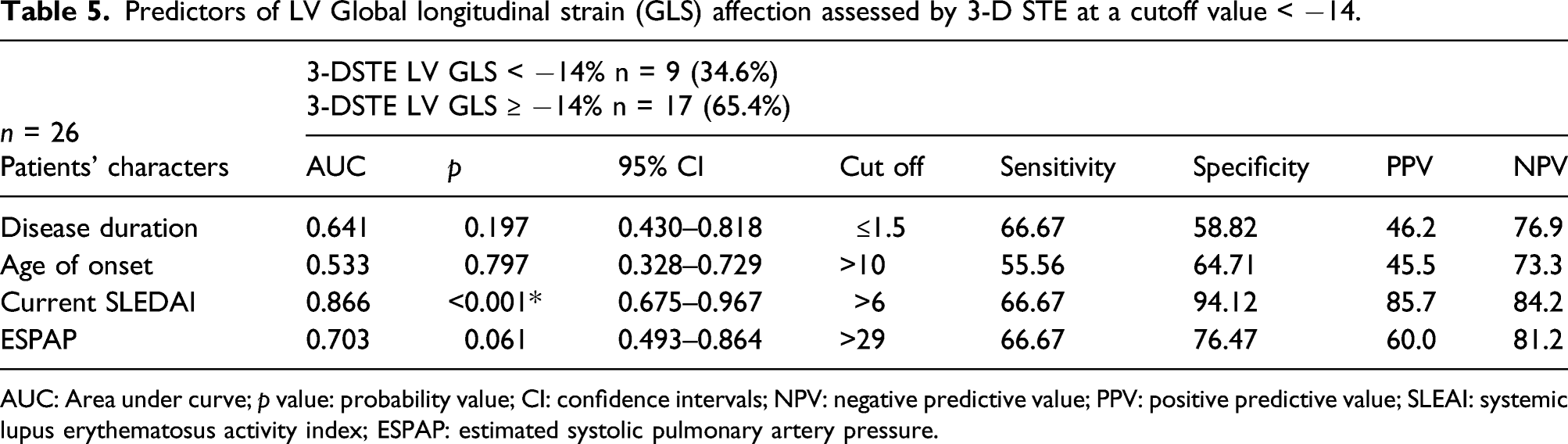
AUC: Area under curve; p value: probability value; CI: confidence intervals; NPV: negative predictive value; PPV: positive predictive value; SLEAI: systemic lupus erythematosus activity index; ESPAP: estimated systolic pulmonary artery pressure.
*signifies “Statistically significant”.
Predictors of LV Global area strain (GAS) affection in jSLE with a cutoff value < −35%.
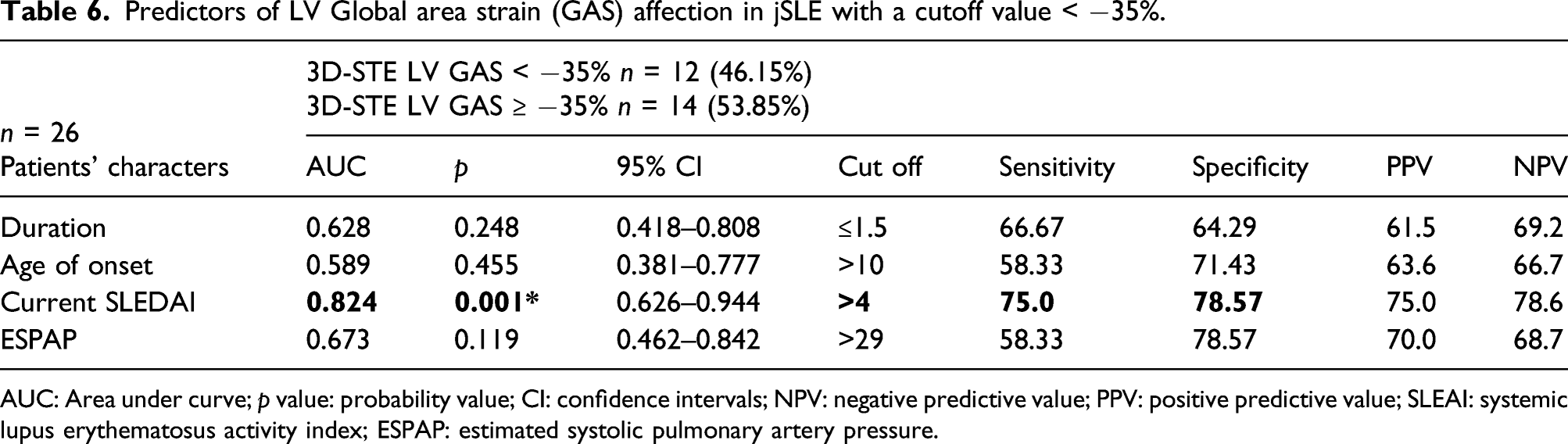
AUC: Area under curve; p value: probability value; CI: confidence intervals; NPV: negative predictive value; PPV: positive predictive value; SLEAI: systemic lupus erythematosus activity index; ESPAP: estimated systolic pulmonary artery pressure.
*signifies “Statistically significant”.
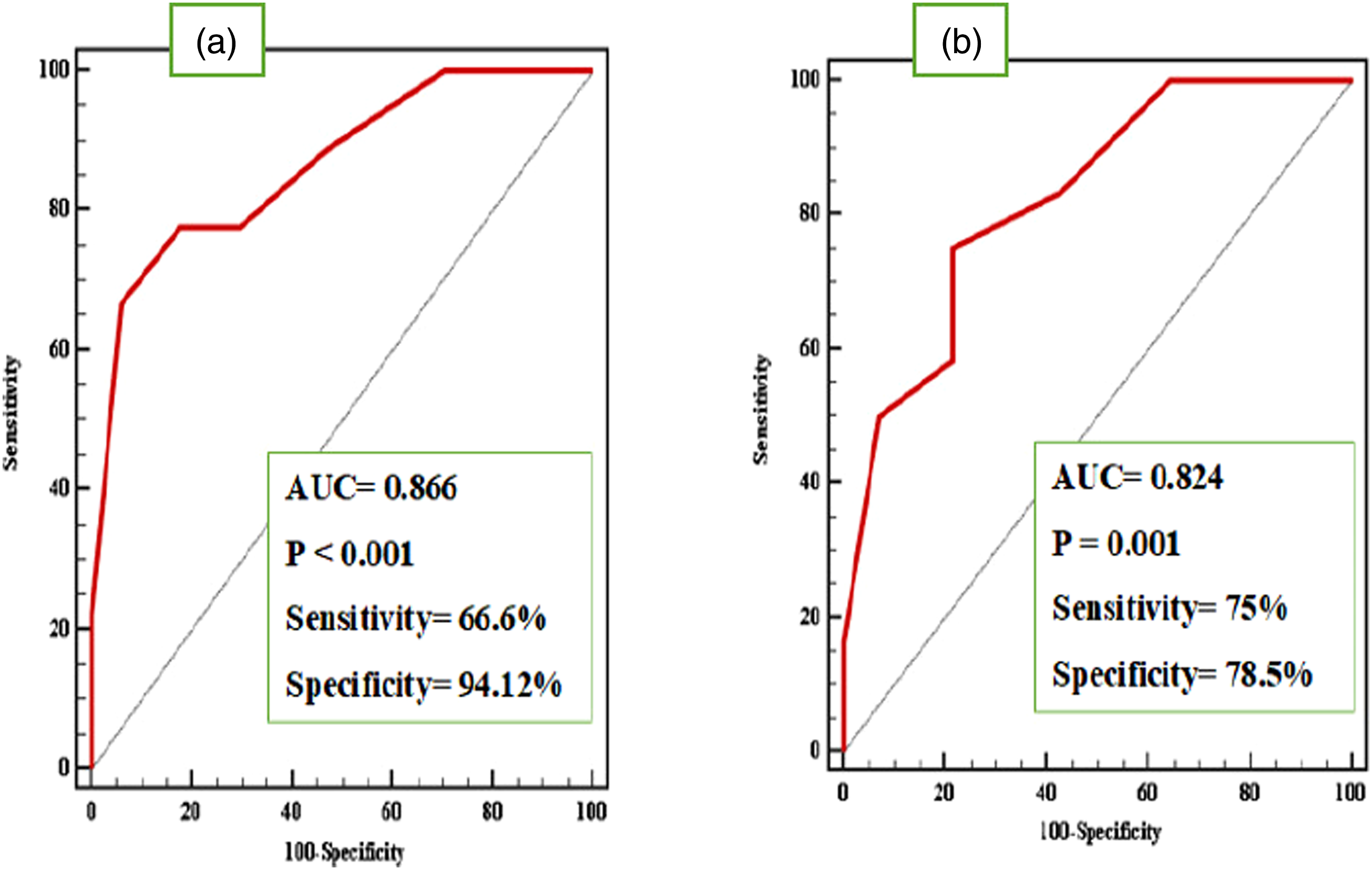
(a) Receiver-operating characteristic (ROC) curve showing the diagnostic value of SLEDAI cutoff value >6 in detection of LV Global longitudinal strain affection and (b) ROC curve showing the diagnostic value of SLEDAI in detection of LV Global area strain affection, SLEDAI cutoff value >4.
Discussion
LV remodeling refers mainly to series of myocardial changes at the microscopic level and ensues changes on the cardiac structure, volume, and function. It is the result of complex interplay between neurohormonal factors such as the RAS system and natriuretic peptides as a result of myocardial injury. Myocardial deformation can be considered one of the macroscopic sequelae of myocardial remodeling. The progressive change in myocardial shape in every plane of myocardial contraction is an early marker of myocardial remodeling. This renders 3D speckle tracking a useful tool for assessment of myocardial remodeling. 17 GLS mainly expresses the efficiency of contraction of the subendocardial fibers, while global circumferential strain allows the detection of middle myofibril dysfunction. Adding a third measure combining both fibers’ effect can lead to better characterization of myocardial deformation and remodeling, namely global area strain. There is limited data about the clinical application of GAS in pediatrics, a relevant study by Shin et al. about the use of GAS in the prediction of death in patients with myocardial infarction, showed that GAS is superior to GLS in the prediction of progressive heart failure and death in patients with myocardial infarction. 18 This study underscores that early onset left ventricular deformation was evident by three dimensional speckle tracking in juvenile SLE patients even with normal ejection fraction assessed by conventional echocardiography and the severity of disease activity was the best predictor of this left ventricular changes in the pediatric age.
Clinical characteristics of the studied population
The age at disease onset of our cohort was similar to most worldwide studies in the last 10 years.19,20 In our study, females were affected more often than males with a ratio of 2.7:1, this is consistent with previous publication. 19 This observation could be interpreted by hormonal effect on SLE occurrence. In our cohort, the most common initial presenting symptom was arthritis/arthralgia and malar rash and this is in harmony with published data.20,21
Left ventricular echocardiographic study by conventional method
To our series there was no statistically significant difference between patients and controls regarding conventional LV dimension and systolic function assessed by M-mode, this finding is similar to previous publications.22,23 This underscores that M-mode is a rapid screening modality but subclinical ventricular dysfunction could be undiagnosed. In contrary, other studies showed that the SLE patients had significantly higher LV dimensions by M-mode. 24 Interestingly, a classical characteristic for longitudinal function of LV, MAPSE was significantly reduced in patients with SLE compared to controls. Similarly, it was published that despite that SLE patients had normal FS and EF by M-mode, MAPSE was reduced compared to controls. 25
Tissue Doppler imaging of LV (TDI)
Some degree of LV diastolic dysfunction was relevant by TDI particularly affecting the septum more than the free wall as septal mitral annulus E’ was significantly lower compared to controls. This finding is in harmony with the previous published studies that concluded that the SLE patients have a subtle LV dysfunction.5,22,23,25,26 Multiple factors may be involved in the development of SLE diastolic and also systolic dysfunction. First, immune complex-mediated inflammatory process plays a pivotal role in SLE subclinical vasculitis, myocarditis, or vascular stiffening. 4 Second, both chloroquine and hydroxychloroquine used to treat rashes and joint pain may be trapped in cell lysosomes and lead to intracellular accumulation of glycogen and membrane phospholipids, inducing cardiomyopathy. 27
Left ventricular deformation by 3-D STE
Tissue Doppler methodology is known to be angle-dependent and 2-D STE can only track motion within the imaging plane, while through-plane motion adversely affects tracking when speckles move out of the imaging plane. 9 In contrast, 3-D STE is likely better suited for the assessment of myocardial deformation, because it is mostly angle-independent and moving speckles remain in the imaging volume and can thus be tracked from frame to frame. 6 The left ventricle of our SLE patients had statistically significant higher diastolic and systolic volumes with reduced ejection fraction as well as lower GLS compared to controls. Through large recent meta-analysis, including five studies that used 2-D STE for assessment of LV myocardial deformations in SLE patients, concluded that LV GLS and GCS were significantly lower in SLE patients than in non-SLE controls. 28 In our series, another 3-D STE parameter was used for assessment of LV function; area strain which is a deformation parameter that quantifies endocardial area change and integrates both longitudinal and circumferential deformation. LV myocardium is composed of three different anatomical layers. The subendocardial and epicardial myocardial fibers predominantly contribute to the longitudinal myocardial function, whereas mid-wall fibers, which have a circumferential arrangement, govern the short-axis function. 29 Due to microvascular lesions of the subendocardial layer, impairment of longitudinal myocardial function, but not circumferential or radial, is often more prominent in an early stage of multiple disease. 30 In other words, GAS was a sensitive and reproducible parameter to detect early and subtle LV systolic dysfunction, showing greater feasibility than other conventional strain parameters (GLS, GCS, and GRS) and could reflect subclinical microvascular abnormalities. 31
The impact of disease characteristics on myocardial performance in SLE patients
In order to detect the impact of different clinical and laboratory variables together with different therapy in SLE patients {SLEDAI, HGB, ESPAP, age of onset disease duration, duration of steroid therapy, and duration of hydroxychloroquine therapy} on the LV, linear and multiple regression correlations were done with all echocardiographic parameters. Estimation of systolic pulmonary artery pressure is considered essential during assessment of left ventricular function as elevated PAP leads to prolongation of RV systole, leftward septal shift, and reduced LV myocardial deformation. By multi-regression analysis, the age of disease onset was the only independent variable that affect LVEDV by 3-D STE meaning that younger patients had larger left ventricular volume. Contrary, Deng et al. reported that younger patients had moderate/severe disease activity. 22 The disease duration was not correlated to GLS and GAS. However, it was previously published that disease duration affects diastolic rather than systolic LV function in 92 children with jSLE. 32 Duration of therapy: In our cohort, Hydroxychloroquine therapy was not related to left ventricular deformation. Similarly, early cardiac injury measured by GLS, GCS and GAS was not associated with the use of drugs (steroids and hydroxychloroquine). 22 On the other hand, some studies reported that immune complex could lead to lupus myocarditis, hydroxychloroquine/chloroquine cardiotoxicity were other causes of cardiac dysfunction. 33 SLEDAI; higher disease activity correlated with more left ventricular systolic dysfunction as global left ventricular systolic strain and global area strain were impaired. Similar linear correlations were present in other studies.5,22,23 SLEDAI had a good predictive value for LV deformation as SLEDAI >6 is associated with LV GLS < −14% and SLEDAI >4 is associated with LV GAS < −35%. In our study, disease severity affecting systolic rather than diastolic function, there was no significant correlation between SLEDAI and any of diastolic function parameters by PW or by TDI. This interesting finding was also reported by Buss et al. as the measurements of TDI and PW-TDI could not differentiate between subjects with higher versus lower disease activity. 25 This is in contrary to previous publications that mentioned that disease severity significantly affected the LV +/− RV diastolic function. 24 Although disease activity generally declines under long-term drug treatment of SLE disease, early organ damages are more likely to be associated with inflammatory processes due to disease activity, while later damages are often attributable to drug side effects. 34
Conclusions
Subclinical left ventricular dysfunction was evident in asymptomatic juvenile SLE patients using 3D speckle tracking imaging. SLE activity index was an independent factor and predictor for longitudinal deformation of LV and systolic dysfunction in jSLE at pediatric age. A SLEDA between 4 and 6 warrants screening of affected patients with global longitudinal and area strain to determine any subtle myocardial dysfunction, clinical trials on the use of cardio-protective drugs such as Captopril, Carvedilol, and Neprylisin inhibitors will be needed in this context to enhance the outcome of affected patients.
Study limitations
We confronted many limitations; this was a single center cross-sectional study with a relatively small number of patients, transthoracic echocardiography was used for assessment of systolic pulmonary hypertension, which is less accurate than that measured by cardiac catheterization, the diastolic function of left ventricle by 3-D speckle tracking was not studied. Technical limitations of 3-D STE are highly dependent on image quality, especially endocardial boundary delineation, and its low frame rate may lead to miscorrelation among frames and affect strain data accuracy.
Footnotes
Acknowledgments
The authors thank the great efforts of Mr. Amgad Aly Hamza for his contribution in the statistical analysis of our data.
Author Contributions
Hala M Agha Conception and design of the target clinical management criteria, critical review and manuscript drafting; final approval of the version to be published.Mahmoud A Othman Data collection, clinical evaluation of patients; data interpretation.Sonia El-Saeidi Data acquisition, clinical evaluation of patients; final approval of the version to be published.Fatma El Zahrae Hassan Data interpretation; final approval of the version to be published.Heba Taher Pediatric patient’s selection, data interpretation; final approval of the version to be published. Final approval of the version to be published.Amal El-Sisi Data interpretation; final approval of the version to be published.Rodina Sobhy Data interpretation; final approval of the version to be published.Antoine Abdelmassih Data collection, echocardiographic assessment of patients; data interpretation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.