
Abstract
Background
In patients with systemic lupus erythematosus (SLE), infections, especially bacteremia, can occur throughout the course of the disease and are often fatal. We evaluated the characteristics of patients with bacteremia and SLE.
Methods
In this retrospective single-center observational study, we analyzed bacteremia in 65 patients with SLE. We compared the group that survived to the group that died. To compare demographic and clinical characteristics between groups, the Mann–Whitney U test was used for non-normally distributed variables. Categorical variables were compared using Fisher’s exact test.
Results
The median observation period was 39 (interquartile range: 6–74) months. The median age was 54 (43–64) years. Patients consisted of six males and 59 females. In 49 cases, the patient survived. In 16 cases, the patient died. The dead group was older, with lower Glasgow Coma Scale scores, higher sequential organ failure assessment (SOFA) scores, and lower fibrinogen levels.
Conclusion
When physicians encounter patients with suspected bacteremia, they should pay attention to the consciousness assessment and SOFA score, and be aware of infections caused by common microorganisms and opportunistic infections.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease in which multiple organs are damaged. The etiology of SLE is unknown, but various autoantibodies and immune complexes are associated with the pathogenesis of SLE. Although patients with SLE are usually treated with glucocorticoids (GCs), immunosuppressants (ISs), or both, patients might exhibit cycles of remission, exacerbation, or comorbidities that follow a refractory course. The mortality rate for patients with SLE is two- to five-fold higher than for the general population.1,2 Infections can occur throughout the course of the disease and are often fatal. Previous studies have reported that bacteremia further exacerbates mortality in patients with SLE.3–5
Patients with SLE were well known to be immunocompromised hosts. Physicians should always be aware of the risk of opportunistic infections. The optimal use of antibiotics to treat infections in patients with SLE remains unclear. The aim of this study is to evaluate the clinical risk factors for mortality and microbiological characteristics of patients with bacteremia and SLE.
Methods
Patients
This study was a retrospective single-center observational study. We included patients who received blood culture tests in the Department of Internal Medicine and Rheumatology at Juntendo University Hospital from April 2009 to April 2020. There were 5188 samples and 2799 sets of blood culture tests, with 388 positive tests. We excluded 101 cases clinically diagnosed as contamination. Of these, 75 episodes of bacteremia were diagnosed in 65 patients with SLE. In all 75 episodes, patients had a sign or symptom of sepsis or a systemic inflammatory response. Although, four patients developed bacteremia twice, one patient had three episodes of bacteremia, and one patient had five episodes of bacteremia. We analyzed the last episode in patients with multiple episodes of bacteremia. All 65 patients were diagnosed with SLE according to the 1997 American College of Rheumatology SLE classification criteria. 6 Empirical antimicrobial therapy was performed as the initial therapy prior to the availability of blood culture results. Appropriate antimicrobial therapy was performed as the administration of any antimicrobial agent to which the causative organism was considered susceptible according to the antibiogram. The ethics committee of Juntendo University Hospital approved this study (approval number 20-144). Patients could opt out of the study through the hospital’s website.
Clinical evaluation and outcomes
Clinical data, including patient demographics, clinical manifestations, laboratory data, sequential organ failure assessment (SOFA) score, 7 quick SOFA score (qSOFA), 8 and outcomes were obtained from medical records. We analyzed clinical manifestations from any point in time. The site of infection was based on the clinician’s diagnosis. Laboratory data were from the time of diagnosis with sepsis. Treatments included all therapies received by patients at the time when sepsis was diagnosed. SPACE refers to Serratia, Pseudomonas, Acinetobacter, Citrobacter, and Enterobacter, which are important for nosocomial infections.
The primary outcome was survival rate. SLE disease activity at the time of bacteremia was estimated using the Safety of Estrogens in Lupus Erythematosus National Assessment–Systemic Lupus Erythematosus Disease Activity Index (SELENA-SLEDAI) 9 and the lupus low disease activity state (LLDAS). 10 Multi-target therapy was defined as the combination of mycophenolate mofetil (MMF) and calcineurin inhibitors.
Statistical analysis
The Mann–Whitney U test was used to compare demographic and clinical characteristics between groups for non-normally distributed variables. Categorical variables were compared using Fisher’s exact test. Data are presented as medians (interquartile range (IQR)). Analyses were performed using SPSS version 23.0 software (SPSS, Armonk, NY) with p < .05 considered to be statistically significant.
Results
Comparison of clinical, microbiological, and background characteristics between the survived and dead groups.
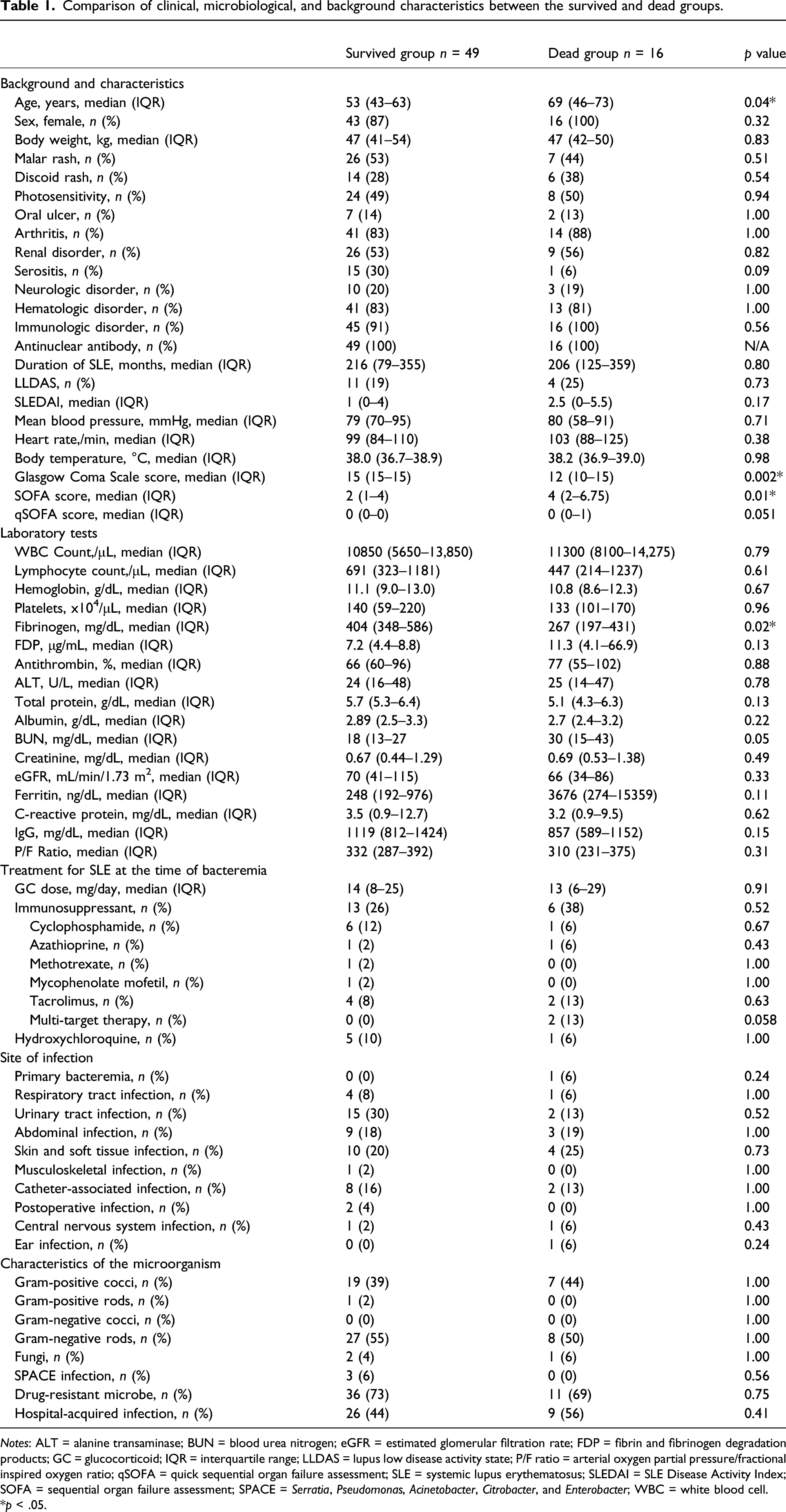
Notes: ALT = alanine transaminase; BUN = blood urea nitrogen; eGFR = estimated glomerular filtration rate; FDP = fibrin and fibrinogen degradation products; GC = glucocorticoid; IQR = interquartile range; LLDAS = lupus low disease activity state; P/F ratio = arterial oxygen partial pressure/fractional inspired oxygen ratio; qSOFA = quick sequential organ failure assessment; SLE = systemic lupus erythematosus; SLEDAI = SLE Disease Activity Index; SOFA = sequential organ failure assessment; SPACE = Serratia, Pseudomonas, Acinetobacter, Citrobacter, and Enterobacter; WBC = white blood cell.
*p < .05.
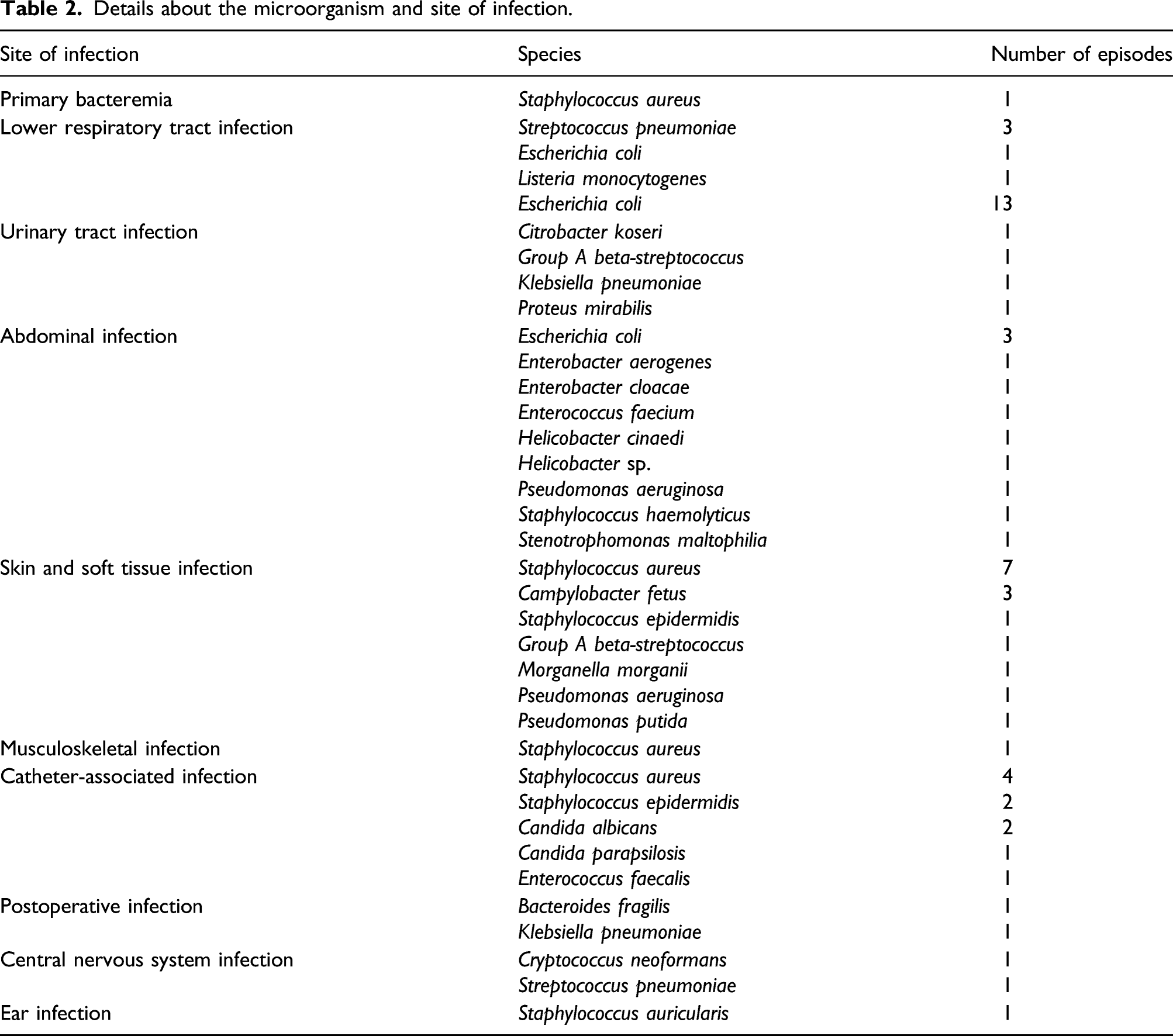
Details about the microorganism and site of infection.
We analyzed age, GCS score, SOFA score, qSOFA score, and fibrinogen levels with Spearman’s correlation test. Lower GCS and higher SOFA score were strongly correlated (p < .001). Older and higher SOFA score were correlated (p = .039). Fibrinogen levels were not correlated with these factors.
There were no significant differences between the survived group and the dead group by the site of infection (Figure 1 and Table 1). There were no differences in classification based on Gram staining or the proportion of patients with fungal infection, SPACE infection, drug-resistant organisms, or hospital-acquired infection. Table 2 shows the details about the site of infection and microorganism. Site of infection and Gram stain results in bacteremia patients with SLE. (A) Site of infection. (B) Gram stain and fungi results. Notes: GNC = Gram-negative cocci; GNR = Gram-negative rods; GPC = Gram-positive cocci; GPR = Gram-positive rods; SLE = systemic lupus erythematosus.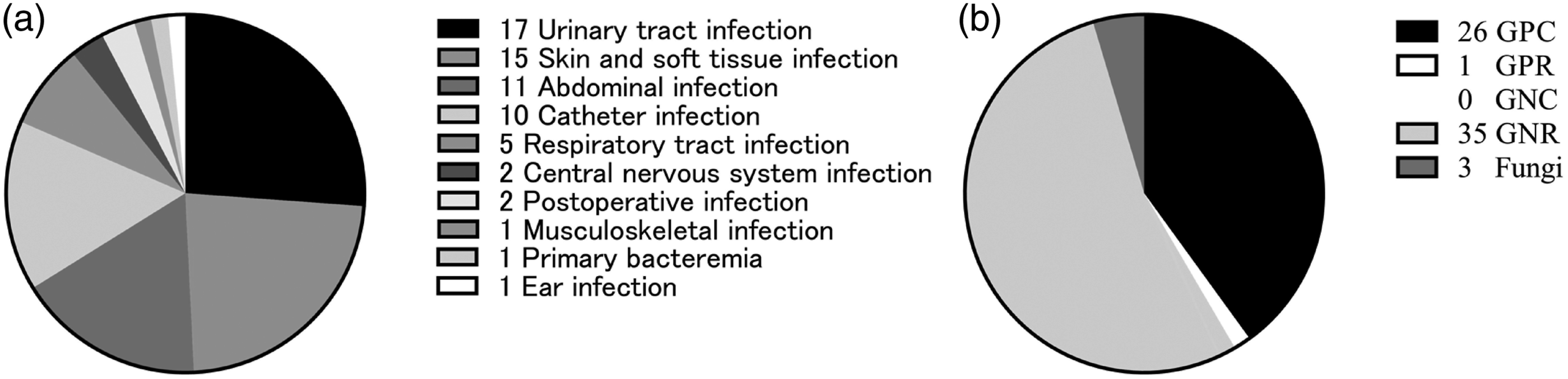
Discussion
We analyzed bacteremia in 65 patients with SLE, which was the largest cohort in Japan. The dead group was older and had lower GCS scores, higher SOFA scores, and lower fibrinogen levels. Although microorganisms were diverse, most microorganisms also caused infectious diseases in the general population.
Poor prognostic factors such as older, lower GCS score, higher SOFA score, and lower fibrinogen level were similar to those for the general population.7,8 Lower fibrinogen level might reflect the state of disseminated intravascular coagulation. In addition, older age and diagnosis of sepsis were also shown to be risk factors for mortality in patients with SLE hospitalized for infectious diseases, as previously reported. 11 Although there was no difference between the survived group and the dead group by the qSOFA score, the dead group tended to have higher qSOFA scores. The European League Against Rheumatism recommendations for the management of SLE also suggested that qSOFA score is a prognostic factor for poor outcomes due to infections in patients with SLE. 12
When focused on the details of the microorganism, we encountered two bacteremia episodes involving Helicobacter species and abdominal infection. Bacteremia with these microbes is rare. In opportunistic infections, although blood cultures were negative, we encountered two cases of disseminated nocardiosis during the observation period, and also reported two cases of Pneumocystis pneumonia from 2006 to 2017. 13 Escherichia coli was the most common causative organism, which was the same as in a Spanish SLE registry. 5 Physicians need to manage opportunistic infections and rare microbes.
Careful consideration should be given to the two patients with bacteremia and SLE receiving multi-target therapy. They were women aged 33 and 37 years, respectively, and treated with 40 mg and 13 mg of prednisolone, respectively. Both patients developed bacteremia due to disseminated VZV, which has a poor prognosis. Compared with non-Asians, Asians might have higher serum mycophenolate acid (MPA) concentrations with the same dose of MMF. We reported the possibility of an association between higher serum MPA concentration and infection. In this study, there were only four patients taking MMF, considering that MMF was approved for SLE on 31 July 2015 in Japan. High mortality with bacteremia may be indirectly associated with multi-target therapy, high serum MPA levels, or both. 14
We evaluated the association between the prognosis of bacteremia and SLE disease activity. LLDAS and SLEDAI were not associated with mortality. A previous study showed that low IgG levels are associated with poor prognosis in patients with sepsis, but no association between IgG levels and mortality was observed in this study. 15 When each organ disorder due to SLE was considered separately, they were not associated with mortality. Although we analyzed the data at the level of patients with bacteremia in this study, we will evaluate the risk of bacteremia by organ disorder in the future. These results suggested that physicians should always pay attention to bacteremia in patients with SLE.
Our study included several limitations. There might have been selection bias because this study was a retrospective single-center observational study. Since we evaluated only bacteremia rather than sepsis, there might have been biases such as fewer lower respiratory tract infections included. Since the observation period ranged from 2009 to 2020, improvements in the treatment of infection might have affected mortality over time.
In conclusion, when physicians encounter patients with SLE who have suspected bacteremia, they should pay attention to the consciousness assessment and be aware of infections caused by common microorganisms and opportunistic infections.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: YS is an employee of the Intelligent Systems Laboratory, SECOM, Co., Ltd. Other authors declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.