
Abstract
Background
The influence of anti-nuclear antibody (ANA) on induced ovulation was controversial, and the effect of prednisone plus hydroxychloroquine (HCQ) treatment on frozen embryo transfer outcomes of in-vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) for ANA-positive women was unclear.
Methods
Fifty ANA-positive women and one-hundred ANA-negative women matched for age and anti-Mullerian hormone (AMH) were included from a Reproductive Medical Central of a University Hospital. Sixty-one oocytes pick-up (OPU) cycles in ANA+ group and one-hundred OPU cycles in ANA
Results
There was no statistical difference in number of retrieved oocytes (13.66 ± 7.71 vs 13.72 ± 7.23, p = .445), available embryos (5.23 ± 3.37 vs 5.47 ± 3.26, p = .347), high-quality embryos (3.64 ± 3.25 vs 3.70 ± 3.52, p = .832), and proportion of high-quality embryos (26.5% vs. 26.7%, p = .940). Biochemical pregnancy rate (33.3% vs. 68.2%, p < .05), clinical pregnancy rate (20.0% vs. 50.1%, p < .05), and implantation rate (5.6% vs. 31.8%, p < .05) were lower, and pregnancy loss rate (83.3% vs. 23.1%, p < .05) was higher in patients with treatment than no treatment.
Conclusion
The influence of ANA on number of retrieved oocytes, available embryos, high-quality embryos, and proration of high-quality embryos was not found. The treatment of prednisone plus HCQ may improve implantation rate, biochemical pregnancy rate, and clinical pregnancy rate, and reduce pregnancy loss rate in frozen embryo transfer outcomes for ANA-positive women.
Keywords
Introduction
Anti-nuclear antibody (ANA) is a group of heterogenous autoantibodies that can bind to the nuclear and cytoplasmatic antigens of cells, 1 and it is a hallmark of various autoimmune diseases such as undifferentiated connective tissue diseases (UCTD), systemic lupus erythematosus (SLE), Sjogren syndrome (SS), and rheumatoid arthritis (RA). 2 In recent years, the association between ANA and pregnancy gets a lot of attention. A meta-analysis including 5038 participants demonstrated that the presence of ANA in serum was positively related to increased risk of recurrent pregnancy loss, 3 and other systematic review and meta-analysis also showed the association between ANA and recurrent miscarriage. 4
Assisted reproductive treatment (ART), especially in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI), is important technology to solve infertility problems. There were 8 million children born by IVF/ICSI treatment between 1987 and 2018 worldwide. 5 A meta-analysis published in 2019 indicated that ANA significantly reduced the clinical pregnancy rate and implantation rate, and increased the miscarriage rate among patients undergoing IVF/ICSI treatment. 6 However, the influence of ANA on oocyte and embryo development is unclear. A retrospective study showed that patients with positive ANA had lower proportion of MII oocytes and two-pronuclear zygotes (2PN), lower proportion of available embryos, and lower proportion of high-quality embryos than those with negative ANA. 7 But, these results were of some differences in different studies.8–10
Moreover, the therapeutic regimen for ANA-positive women undergoing IVF/ICSI treatment was still controversial. Prednisone alone, prednisone plus low-dose aspirin (LDA), and low molecular weight heparin (LMWH) plus LDA even intravenous immunoglobulin (IVIG) were potential effective treatment protocols explored by previous studies.11–16 Hydroxychloroquine (HCQ) is a kind of immunosuppressant that was regarded to be safe for pregnant women. For pregnancy with SLE and refractory antiphospholipid syndrome (RAPS), HCQ was recommended throughout pregnancy because of the function of immune regulation and anti-inflammatory.17,18 However, the effect of HCQ on the IVF/ICSI outcomes for ANA-positive women was little explored, especially in frozen embryo transfer cycles. This study was performed to explore the influence of ANA on oocyte and embryo development, and investigate the therapeutic effect of prednisone plus HCQ on frozen embryo transfer outcomes of IVF and ICSI for ANA-positive women.
Materials and methods
Subjects
We searched patients who received IVF/ICSI treatment from Jan 2020 to May 2021 in the medical record system of Reproductive Medical Central of West China Second University Hospital, Sichuan University. All basic information of them was scanned, including age, anti-Mullerian hormone (AMH) levels, the basic levels of follicle-stimulating hormone (bFSH), the basic levels of luteinizing hormone (bLH), the basic levels of estradiol (bE2), type of infertility (primary infertility or secondary infertility, secondary infertility is usually defined as a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse, after having conceived at least once before), ovarian stimulation methods, embryo transfer methods, history of previous diseases, and medical procedures. Moreover, ANA, antibodies against extractable nuclear antigens (ENA-Ab), anti-cardiolipin antibody (ACA), anti-beta2-glycoprotein I antibody (A-β2-GPI), and anti-thyroid antibody (ATA) were detected in most of the patients before the beginning of every IVF/ICSI cycle to recognize patients with autoimmune diseases, as well as hysteroscopy was performed to recognize intrauterine adhesion, myoma of the uterus, and adenomyosis.
Fifty patients with positive ANA and one-hundred autoantibody-negative patients matched for age and AMH were included in this study, all of them met the following criteria: (1) age not over 42 years, (2) undergoing induced ovulation with the GnRH agonist protocol, (3) infertility caused by tubal disorder and/or male factor or unexplained infertility, (4) all embryos are frozen because of personal reasons, poor endometrium, or ovarian hyper-stimulation syndrome (OHSS). The titers of ANA ≥1:100 were regarded as positive. For ANA-positive group, patients received no treatment or combined treatment of prednisone (10 mg/d) and HCQ (200 mg/d) beginning at the third day of menstrual period in every frozen embryo transfer cycle. The treatment of prednisone plus HCQ continues until the 12th week of gestation or the occurrence of terminal event (implantation failure, biochemical pregnancy loss, or pregnancy loss before 12th week of gestation). According to the treatment protocols, patients in ANA-positive group were divided into group A (no treatment) and group B (combined treatment of prednisone and HCQ).
The exclusion criteria for both groups were as follows: uterine malformation, endometritis, intrauterine adhesion, myoma of the uterus, adenomyosis, endometriosis, abnormal uterine bleeding, polycystic ovarian syndrome, hypothyroidism, hyperthyroidism, family history of genetic disease, chromosome abnormality of the couples, mycoplasma, gonococcus, trichomonas vaginalis, chlamydia, HIV, fungi, fever, infection, hepatitis, renal insufficiency, Treponema pallidum, history of adverse pregnancy outcomes (such as pregnancy loss, premature delivery, and intrauterine growth restriction), positive for other auto-antibodies except ANA (ENA-Ab or ATA presence, titers of ACA, or A-β2-GPI > 20 IgG phospholipid units or IgM phospholipid units 18 ), symptoms of autoimmune diseases (joint pain, arthrocele, photophoby, alopecia, xerophthalmia, xerostomia and, Raynaud’s sign), or any autoimmune disease such as SLE, APS, autoimmune thyroiditis (AS), and Sjogren syndrome (SS). For patients receiving HCQ treatment, fundus examination was performed prior to the beginning of treatment, and patients were excluded if there were lesions in the fundus. For the same patient, the time interval between two embryo transfer cycles must be ≥3 months to elute the effects of the drug. This study was performed according to the World Medical Association Declaration of Helsinki and was approved by the Ethics Committee of West China Second University Hospital.
ANA assay
The ANA in serum was detected before the beginning of IVF/ICSI treatment using the indirect immunofluorescence (IFT) method on the human epithelial (HEp-2) cell substrate by the department of laboratory medicine of West China Second University Hospital. Olympus BX51 fluorescence microscope and all the antibodies’ kits were purchased from Euro immune Company (Germany).
IVF/ICSI program
Patients were treated by gonadotropin-releasing hormone (GnRH) antagonist protocol. Recombinant daily follicle-stimulating hormone (rFSH, Gonal F, Serono) was started on day two or three of the cycle. Subsequent gonadotropin medication doses were adjusted based on the ovarian response as assessed by follicular growth and estradiol levels. The GnRH antagonist (Orgalutran 0.25®, Organon, Netherland) was initiated on day five or six of the stimulation. When ≥2 follicles had reached 18 mm in mean diameter or ≥3 follicles had reached 17 mm in mean diameter were observed, human chorionic gonadotropin (hCG) at a dose of 10,000 IU was intramuscularly injected and the oocytes pick-up (OPU) was performed after about 36–37 hours. The embryos were graded on day 3 according to the following three characteristics: the number and size of their blastomeres, percentage of fragmentation, and cleavage rate. A high-quality embryo is defined as 6–8 cell stage, equally sized blastomeres, and less than 20% fragmentation of the blastomeres.
Frozen embryo transfer cycle
During frozen embryo transfer cycles, pentanoic acid estradiol was used orally at the third day of menstrual period. The dose was based on endometrial thickness measured by ultrasound and serum levels of sex hormones, and it was not changeless. Progesterone (60 mg/d) was intramuscularly injected to translate endometrium into secretory phase if the thickness of endometrial ≥8 mm or serum level of estradiol was higher than 100 pg/mL. One or two blastocysts were transplanted on the fifth day of progesterone injection. Progesterone supplementation by daily transvaginal progesterone or injective progesterone was performed for all patients. For patients with positive ANA, no treatment or combined treatment of prednisone (10 mg/d) and HCQ (200 mg/d) was used at the same time of pentanoic acid estradiol used. The serum β-hCG levels were measured at 14 days after frozen embryo transfer, and ultrasonography was performed if patients were positive for β-hCG. Clinical pregnancy was diagnosed by the presentence of a gestational sac with a fetal heartbeat.
Data collection
The fertilization program (IVF or ICSI), the serum levels of LH, E2, P on the day of hCG injection, the thickness of endometrium on hCG day, days of ovarian stimulation, total Gn dose, number of retrieved oocytes, number of available embryos, number of high-quality embryos, and proportion of high-quality embryos (number of high-quality embryos/total retrieved oocytes) were collected. For frozen embryo transfer cycles, biochemical pregnancy rate (biochemical pregnancy/total cycles), clinical pregnancy rate (patients detected with fetal heartbeat/total cycles), implantation rate (embryos with fetal heartbeat/total transferred embryos), and pregnancy loss rate (pregnancy loss/clinical pregnancy) were calculated.
Statistical analysis
Statistical analyses were performed by SPSS, version 25.0 (SPSS Inc., Chicago, IL, USA). Continuous variables with a normal distribution were expressed as a mean plus or minus a standard deviation (SD) and were compared by the student’s t-test or an analysis of variance (ANOVA). Continuous variables with an abnormal distribution were expressed as medians (interquartile range) and were compared by the Mann–Whitney U test or the Kruskal–Wallis H-test. The rates were compared by the chi-squared test and Fisher’s Exact Test when appropriate. p values less than .05 were considered statistically significant.
Results
Basic characteristics of included patients
Basic characteristics between ANA+ group and ANA
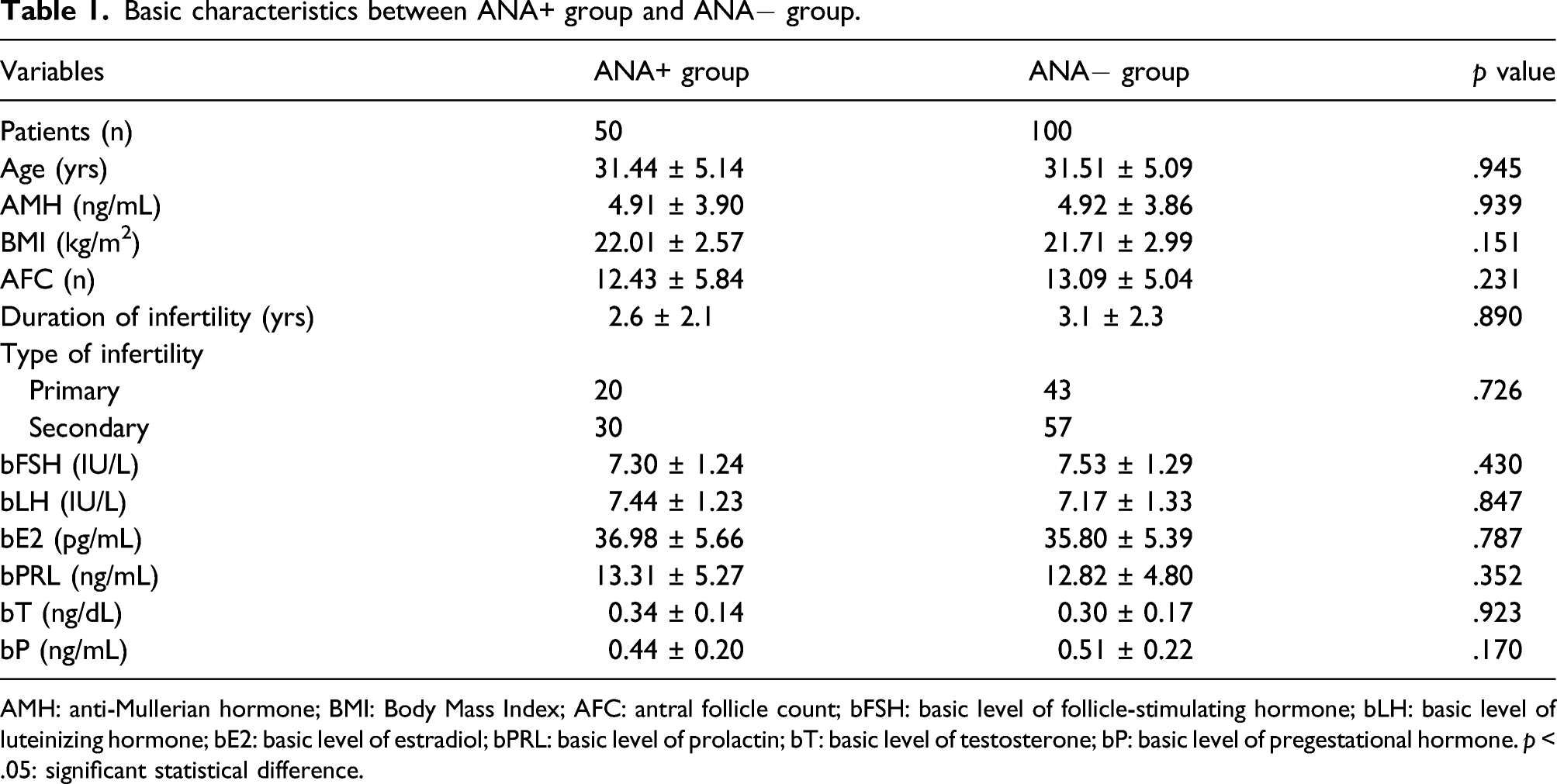
AMH: anti-Mullerian hormone; BMI: Body Mass Index; AFC: antral follicle count; bFSH: basic level of follicle-stimulating hormone; bLH: basic level of luteinizing hormone; bE2: basic level of estradiol; bPRL: basic level of prolactin; bT: basic level of testosterone; bP: basic level of pregestational hormone. p < .05: significant statistical difference.
Ovarian stimulation outcomes in ANA+ and ANA− groups
Ovarian stimulation and oocytes pick-up outcomes between ANA+ group and ANA
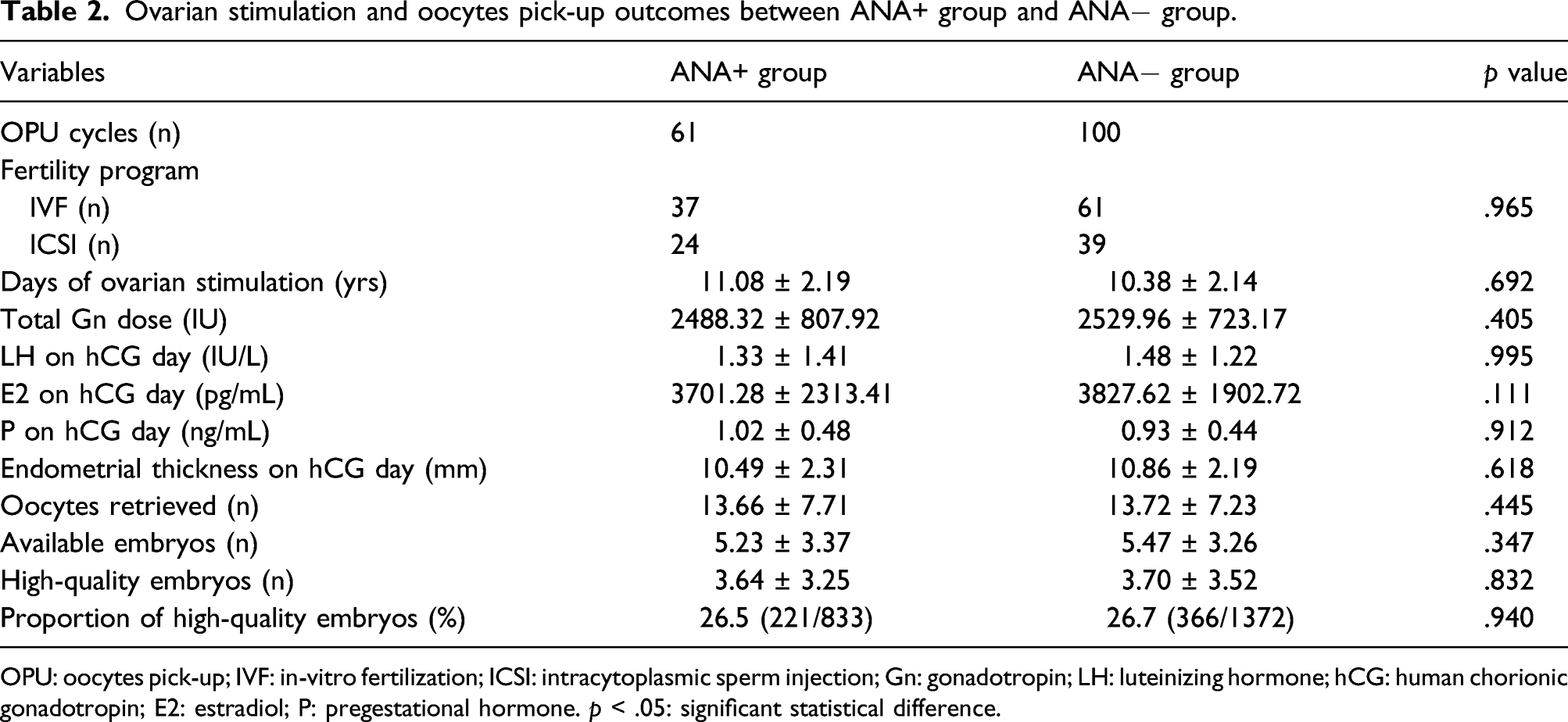
OPU: oocytes pick-up; IVF: in-vitro fertilization; ICSI: intracytoplasmic sperm injection; Gn: gonadotropin; LH: luteinizing hormone; hCG: human chorionic gonadotropin; E2: estradiol; P: pregestational hormone. p < .05: significant statistical difference.
Frozen embryo transfer outcomes between group A and group B
Frozen embryo transfer outcomes between group A and group B.
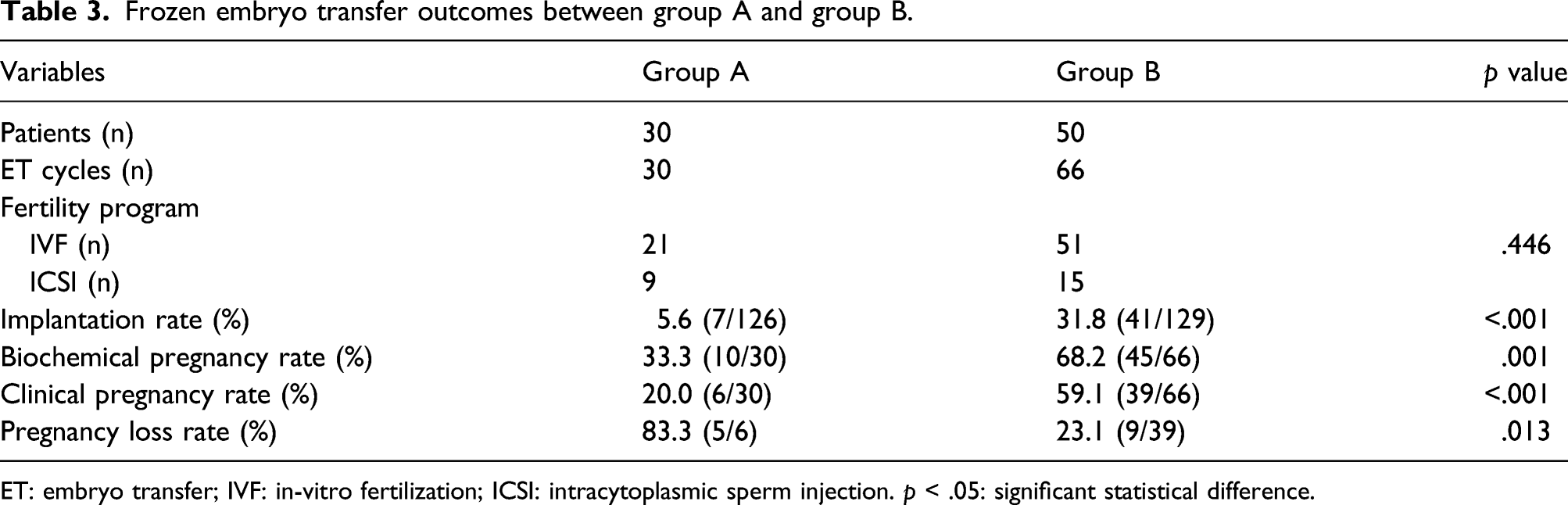
ET: embryo transfer; IVF: in-vitro fertilization; ICSI: intracytoplasmic sperm injection. p < .05: significant statistical difference.
Discussion
As a group of heterogeneous autoantibodies, ANA was found in a lot of autoimmune diseases even in some healthy people. However, the present understanding for the generation, function, and pathological mechanism of ANA was still confused. Women of reproductive age are susceptible for many autoimmune diseases such as SLE and SS, and they are also easier to be found as carriers of ANA.19,20 The effects of ANA on reproductive health are widely concerned in recent years. Previous studies proved that ANA was associated with pregnancy loss,3,4,21,22 and there were also some studies indicating that ANA in serum or oocyte fluid may be related to unexplained infertility.23–25 Li et al. 26 found that the existence of ANA in granular cells and endometrial tissues may cause imbalanced apoptosis of these cells and induce infertility and pregnancy loss. Veglia et al. 27 performed an in vivo study and indicated that ANA+ IgG injection in mice is able to induce fetal resorption and complement activation, and the formation and deposition of antigen–antibody complex in tissues may relate to complicated clinical manifestations. Bruno et al. performed a retrospective study exploring the significance of uterine and placental blood flow indexes and ANA as predictive factors for pregnancy loss. The results showed that ANA may be associated with abnormal uterine and placental blood flow indexes, which may be a potential mechanism for ANA affecting pregnancy. 28 However, the above mechanisms are not enough to explain problems we faced at present. It is worthy to be concerned that women with IVF/ICSI treatment are a specific group because the use of fertility drugs and the manual processing of oocytes and embryos may distinguish them from women with natural pregnancy. Many studies indicated that the presence of ANA reduced the implantation rate, biochemical pregnancy rate, and clinical pregnancy rate, and improved the pregnancy loss rate during IVF/ICSI treatment.6–9 However, the effect of ANA on egg and embryo development and the treatment protocols for ANA-positive women undergoing IVF/ICSI were controversial in previous studies.
A study including 66 patients found the proportion of MII oocytes and 2PN embryos, cleavage rate, number of available embryos, and number of high-quality embryos were significantly lower in ANA+ group than those in the ANA−group, 7 but another studies demonstrated that the proportion of 2PN, cleavage rate, and number of retrieved oocytes were similar in two groups.8,9 In this study, we investigated the eggs and embryo development in 69 OPU cycles of 50 ANA-positive patients and 100 OPU cycles of 100 controls, and the results showed no statistical difference in number of retrieved oocytes, available embryos, and high-quality embryos. It seems that difference between our study and previous studies came from the matching of age and AMH for two groups strictly. It is necessary to be mentioned that previous studies found the ANA in follicular fluid reduced efficacy of IVF/ICSI and embryo transfer by invading endometrium and granular cells, 26 but our study did not explore these influences. The presence of ANA in serum and follicular fluid was not consistent in all patients, 8 for example, a study investigated 50 patients with positive ANA in serum, but only 36 patients were detected positive ANA in follicular fluid. 8 Uncertainty about the distribution of ANA in follicular fluid also accounts for the differences between our study and previous studies.
Effective intervention for ANA-positive patients undergoing IVF/ICSI treatment was recommended by many clinicians because of the adverse influence of ANA on IVF/ICSI outcomes. However, the treatment regimens for these patients were controversial. A randomized controlled trial demonstrated that combined treatment of prednisone (10 mg/day) and aspirin (100 mg/day) starting 3 months before induction of ovulation can improve the fertilization rate, pregnancy rate, implantation rate, and reduce abortion rate compared to non-treatment group. 11 Another study administered prednisolone (15–60 mg/d for 5 days) treatment starting 1 day after oocyte retrieval to ANA-positive patients, and compared to prednisolone-nontreated ANA-positive cycles, and the implantation and clinical pregnancy rates were improved significantly, but the live birth rate was not. 13 In addition, all of the above studies were performed in fresh embryo transfer cycles; the therapeutic regimen for frozen embryo transfer cycles was not explored. Frozen embryo transfer is a common transfer plan with uncertain starting time in IVF/ICSI treatment, and the use of prednisolone and/or aspirin starting before oocytes retrieval was not recommended because of the risk of long-time use of glucocorticoid. A case report published in 2018 indicated the potential of HCQ in treating IVF/ICSI patients with positive ANA, but the grade of evidence is limited. 29 This study was designed focusing on the therapeutic regimen for ANA-positive patients undergoing frozen embryo transfer cycles; prednisone (10 mg/d) and HCQ (200 mg/d) were used starting at the third day of menstrual period. The results indicated that combined treatment of prednisone (10 mg/d) and HCQ (200 mg/d) starting at the third day of menstrual period improved implantation rate, biochemical pregnancy rate, clinical pregnancy rate, and reduce pregnancy loss rate for ANA-positive patients during frozen embryo transfer cycles.
The study has many implications on clinical practice. At first, the presence of ANA in serum was not associated with outcomes of OPU cycles, including number of retrieval oocytes, available embryos, high-quality embryos, and the proportion of high-quality embryos. The treatment before induction of ovulation may not be necessary for the most of ANA-positive patients. Second, combined treatment of prednisone (10 mg/d) and HCQ (200 mg/d) starting at the third day of menstrual period was selectable therapeutic regimen for ANA-positive patients during frozen embryo transfer cycles. Compared to other therapeutic regimen, this regimen reduced total dose of glucocorticoid and the risk of side effect mediated by glucocorticoid. HCQ is a pregnancy-safe immunosuppressant, which is widely used for pregnancy with autoimmune diseases throughout pregnancy. If necessary, the usage of HCQ can be lengthened to the whole period of pregnancy for some indication related to autoimmune diseases including undifferentiated connective tissue disease or SLE. Therefore, this regimen is preferred for ANA-positive patients who are predisposed to develop autoimmune diseases.
There are still some limitations in this study. First, we did not detect ANA in follicular fluid, and the association between ANA in follicular fluid and outcomes of OPU cycles may be underestimated. Future studies should pay more attention to the effects of ANA in follicular fluid on IVF/ICSI outcomes. Second, the therapeutic regimen for fresh embryo transfer cycles in ANA-positive patients was not explored in this study; it needs to be explored in the future. Third, the severity of diseases between group A and group B was not compared, which may reduce the accuracy of the results. The titers of serum ANA cannot reflect the severity of ANA affecting IVF/ICSI exactly, and serum complement 3 (C3), C4 levels may be effective predictive indicators according to previous studies on SLE/APS. 17 This hypothesis needs to be explored in the future. Last but not least, the sample size in this retrospective study was small, which restricted the clinical application of the conclusions. More prospective studies on this topic with large sample size are necessary to explore the value of this therapeutic regimen composed by prednisone and HCQ for both fresh embryo transfer and frozen embryo transfer cycles.
In conclusion, the influence of ANA on serum on number of retrieved oocytes, available embryos, high-quality embryos, and proportion of high-quality embryos was not found. The treatment of prednisone (10 mg/d) plus HCQ (200 mg/d) starting at the third day of menstrual period in frozen embryo transfer cycles may improve biochemical pregnancy rate, clinical pregnancy rate, and implantation rate, and reduce pregnancy loss rate in frozen embryo transfer cycles of ANA-positive patients undergoing IVF/ICSI treatment. More prospective studies on this topic with large sample size are of importance to explore the mechanisms of ANA on IVF/ICSI treatment, and to explore more valuable therapeutic regimen.
Footnotes
Authors contributions
R.G. and L.Q. were involved in study design; K.C. and C.M. performed data collection; W.D. and X.Z. performed statistical analysis. All authors participated in the interpretation of data, and have since revised drafts. They have also read and given final approval for the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundamental Research Funds for the Central Universities under Grant SCU2020D4132 and Department of Science and Technology of Sichuan under Grant 2020YFS0127.