
Abstract
Background
Age at disease onset may modulate systemic lupus erythematosus (SLE), but its relation to cutaneous/extracutaneous manifestation remains understudied.
Objective
To compare the cutaneous, systemic features, laboratory characteristics, and disease severity between late- and adult-onset SLE patients
Methods
Analyses of the cutaneous, systemic involvement, laboratory investigations, SLE disease activity index 2000 (SLEDAI-2K), and disease damage were performed to compare between groups.
Results
Of 1006 SLE patients, 740 and 226 had adult- (15–50 years) and late-onset (>50 years), respectively. Among 782 with cutaneous lupus erythematosus (CLE), acute CLE (ACLE) and chronic CLE (CCLE) were more common in the adult- and late-onset SLE, respectively (p = 0.001). Multivariable logistic regression analysis demonstrated that male patients and skin signs, including papulosquamous subacute CLE, discoid lupus erythematosus, and lupus profundus, were associated with late-onset SLE (all p < 0.05). Late-onset SLE had lower lupus-associated autoantibodies, and systemic involvement (all p < 0.05). ACLE, CCLE, mucosal lupus, alopecia, and non-specific lupus were related to higher disease activity in adult-onset SLE (all p < 0.001). There was no difference in the damage index between the two groups.
Conclusions
Late-onset SLE had a distinct disease expression with male predominance, milder disease activity, and lower systemic involvement. Cutaneous manifestations may hold prognostic values for SLE.
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease. The annual incidence of SLE is approximately 1–10 per 100,000. The prevalence of SLE is around 5.8–130 per 100,0001,2 and is high among Hispanics, African Americans, and Asians. 3 SLE affects all races, gender, and age with variable incidence rates around the world. 4 Although the onset of SLE can occur at any age, the most commonly affected population is women in childbearing age. The onset of SLE over the age of 50 or late-onset SLE is uncommon, occurring 2%–20% of all patients with SLE. 5 However, due to a longer life expectancy, physicians will encounter more cases of late-onset SLE and need to have high clinical awareness of this condition. Studies have suggested that late-onset SLE display a more insidious clinical course and better prognosis compared to the juvenile-onset (<15 years-old) and adult-onset (15–50 years-old) SLE. 6 However, conflicting results indicating higher disease activity and damage have been demonstrated among older onset SLE in several studies as well. 7 , 8 A meta-analysis regarding late-onset SLE as a distinct subgroup has also demonstrated no substantial differences compared to other age groups. 9
Cutaneous manifestation can occur between 59%–85% of SLE patients and it is presented as the first sign in approximately 25%. 10 Cutaneous features are included in the classification criteria for SLE in the American College of Rheumatology (ACR) 1997, 11 the Systemic Lupus International Collaborating Clinics (SLICC) 2012 12 and the European League Against Rheumatism (EULAR)/ACR 2019. 13 Certain skin signs have been reported as markers of systemic involvement and may hold prognostic values for SLE.14–17 The age onset of SLE may be considered as an influential factor for both the clinical manifestation and disease course, but differences in cutaneous findings between the adult- and late-onset of SLE have not been fully elucidated. Moreover, there is limited data regarding cutaneous presentations as prognostic indicators among different age groups of SLE. The objective of this study was to examine the cutaneous and extracutaneous features and laboratory characteristics of late-onset compared to the adult-onset SLE in the Southeast Asia population. We also aimed to explore the presence of cutaneous findings in relation to the disease activity among different age groups of SLE.
Methods
Patients
International Classification of Disease 10th revision (ICD-10) codes M32 (SLE) was used to perform a computer search for all patients treated at a tertiary referral center (Ramathibodi hospital, Bangkok, Thailand). Data was obtained from January 2008 to May 2018. Records of patients who fulfilled the ACR 1997 11 and/or SLICC 2012 12 classification criteria for SLE were retrospectively reviewed. The diagnosis of SLE and cutaneous lupus erythematosus (CLE) was made by certified rheumatologists and dermatologists, respectively. SLE patients with other coexisting connective tissue diseases, cases with the first clinical symptom appearing before 50 but had subsequent symptoms after 50 years of age, loss to follow-up and/or referred cases, and patients with incomplete medical records were excluded. SLE patients who developed their clinical symptoms between 15–50 years of age were classified as adult-onset SLE, whereas those with symptoms occurring after 50 years of age were categorized in the late-onset SLE group.
Study design
This retrospective cross-sectional study was approved by the Institutional Review Board of the Faculty of Medicine, Ramathibodi Hospital, Mahidol University (MURA 2018/313). Patients’ demographic data, mucocutaneous manifestation (i.e. lupus erythematosus-specific cutaneous signs (acute cutaneous lupus erythematosus; ACLE, subacute cutaneous lupus erythematosus; SCLE, chronic cutaneous lupus erythematosus; CCLE) and non-specific lupus erythematosus lesions), systemic involvement (e.g. hematologic, renal, arthritis, neurologic, serositis) and laboratory characteristics (antinuclear antibody (ANA) titer, anti-deoxyribonucleic acid (DNA) antibody, anti-Smith (anti-Sm) antibody, anti-Sjögren's-syndrome-related antigen A (anti-SSA/Ro) autoantibody, anti-Sjögren's-syndrome-related antigen B (anti-SSB/La) autoantibody, lupus anticoagulant, anticardiolipin, β2-glycoprotein 1 antibody, erythrocyte sedimentation rate (ESR), 18 , 19 complement, 20 complete blood count (CBC) and urinary analysis)) were retrieved and analyzed. ANA titer was classified into low (<1:640) and high titer (≥1:640). 21 , 22 Assessment of disease activity was based on the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) at diagnosis. The SLEDAI-2K was used to classified patients into; mild (scores <3), moderate (scores 3–6) and severe (scores >6) disease activity. 23 Additionally, a longitudinal review of systemic involvement until the data collection date was further undertaken. SLICC/ACR damage index (SLICC/ACR-DI) was used analyze the disease damage score. 24 Finally, a multivariable logistic regression analysis was performed to find independent factors associated with the late-onset SLE group in particular.
Statistical analysis
Categorical data were shown as percentages. Continuous data with normal distribution were presented as means and standard deviations. Statistics including t-test, chi-square test, or Fisher’s exact test were used to compare the clinical and laboratory characteristics as well as SLEDAI-2K at diagnosis between adult- and late-onset SLE patients. A p-value <0.2 was considered in the multivariable logistic regression analysis. Odds ratios (ORs) and 95% confidence intervals (95%CI) were calculated on variable independent factors. All statistical analyses are accessed by stata 14.0 (Stata Corp LLC, College Station, TX) version. A p-value < 0.05 was considered statistically significant.
Results
Medical records of 1920 patients who met the inclusion criteria from January 2008 to May 2018 were reviewed. Nine hundred and fourteen patients were excluded from the analysis due to overlapping diagnosis with other connective tissue diseases (n = 264), SLE symptoms occurring both before and after 50 years of age (n = 208), loss to follow-up/referred cases (n = 259) and incomplete medical records (n = 183). A total of 1006 patients were analyzed consisting of 740 (73.6%) adult- and 266 (26.4%) late-onset SLE patients. Details regarding the study protocol are provided in Figure 1.
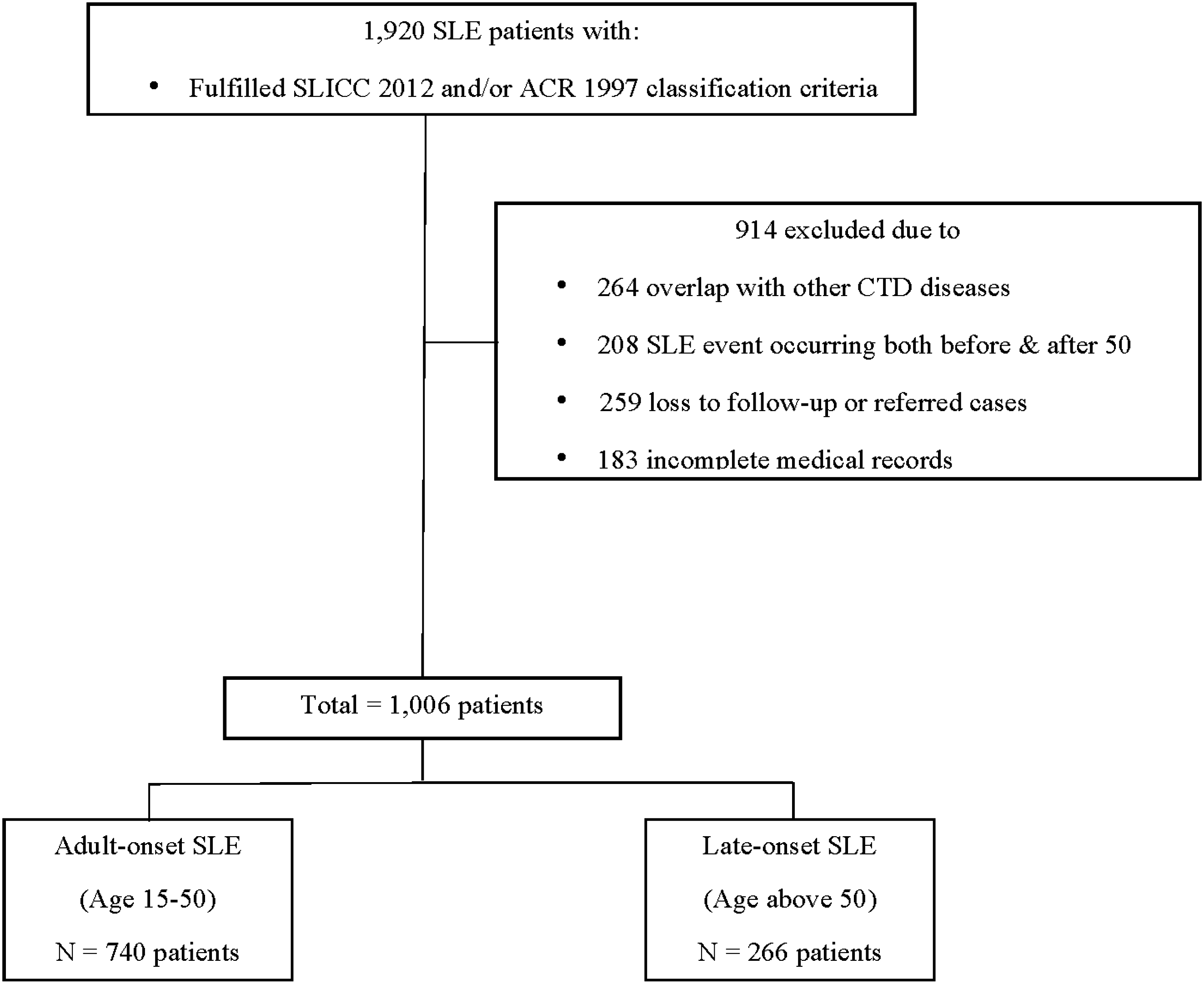
Recruitment process and inclusion and exclusion criteria.
The mean age of disease onset was 29.9 ± 10.3 and 60.7 ± 8.5 years old in the adult- and late-onset SLE groups, respectively. Female predominance was observed in both groups (female: male; 14:1 for adult- and 5:1 for late-onset group). All of our patients were of Southeast Asian descent. The mean SLEDAI-2K was higher in the adult-onset SLE group (11.5 ± 5.8 vs. 7.1 ± 5.6). Adult-onset SLE cases had longer follow-up period than late-onset SLE patients (13.3 ± 8.1 vs. 9.5 ± 7.4 years). Skin biopsy to confirm the diagnosis of CLE was performed in 171 (23.1%) and 97 (36.5%) of adult- and late-onset SLE cases, respectively. The baseline characteristics are shown in Table 1.
Baseline characteristics of 1006 patients with adult- and late-onset SLE.
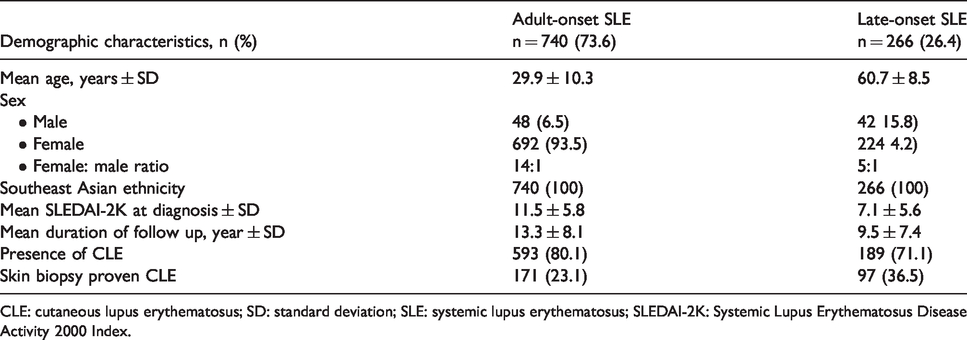
CLE: cutaneous lupus erythematosus; SD: standard deviation; SLE: systemic lupus erythematosus; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity 2000 Index.
Seven hundred and eighty two patients (77.7%) presented with CLE. The differences among cutaneous features between the adult- and late-onset SLE are demonstrated in Table 2. ACLE was significantly more predominant in adult- compared to late-onset SLE patients (n = 391, 52.8% vs. n = 74, 27.8%, p < 0.001). The most common cutaneous finding in ACLE was malar rash, followed by photosensitive rash, and both were more frequently found in the adult-onset SLE patients (malar rash; n = 320, 43.2% vs. n = 34, 12.8%, p < 0.001 and photosensitive rash; n = 188, 25.4% vs. n = 46, 17.3%, p = 0.007). There was no between-group difference on the occurrence of SCLE in general; however, papulosquamous SCLE was remarkably more common in late-onset SLE patients (n = 11, 4.1% vs. n = 12, 1.6%, p = 0.019). Late-onset SLE had significantly more CCLE than adult-onset SLE (n = 105, 39.5% vs. n = 23,732%, p = 0.028).
Cutaneous manifestations in adult- and late-onset SLE patients.
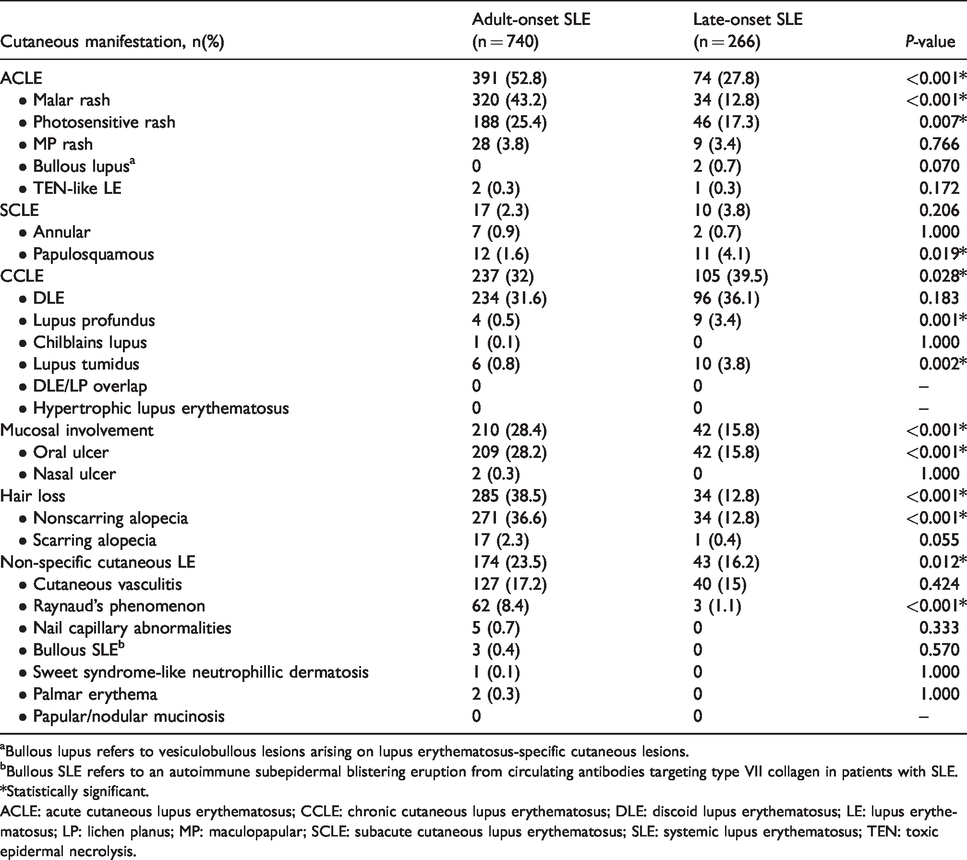
aBullous lupus refers to vesiculobullous lesions arising on lupus erythematosus-specific cutaneous lesions.
bBullous SLE refers to an autoimmune subepidermal blistering eruption from circulating antibodies targeting type VII collagen in patients with SLE.
*Statistically significant.
ACLE: acute cutaneous lupus erythematosus; CCLE: chronic cutaneous lupus erythematosus; DLE: discoid lupus erythematosus; LE: lupus erythematosus; LP: lichen planus; MP: maculopapular; SCLE: subacute cutaneous lupus erythematosus; SLE: systemic lupus erythematosus; TEN: toxic epidermal necrolysis.
Oral ulcer was the most common mucosal involvement and was significantly more prevalent in adult-onset SLE (n = 209, 28.2% vs. n = 42, 15.8%, p < 0.001). Non-scarring alopecia appeared significantly more common in the adult-onset SLE patients (n = 271, 36.6% vs. n = 34, 12.8%, p < 0.001). Additional lupus non-specific lesions were also found more often in the adult-onset SLE (n = 174, 23.5% vs. n = 43, 16.2%, p = 0.012) with cutaneous vasculitis (n = 127, 17.2% vs. n = 40, 15%, p = 0.424) and Raynaud’s phenomenon (RP) (n = 62, 8.4% vs. n = 3, 1.1%, p < 0.001) being the most common.
A multivariable logistic regression analysis for variables predictive of late- compared to adult-onset SLE was performed (Table 3). Male patients were independently associated with late-onset SLE (OR = 1.9, 95%CI = 1.16–3.11, p = 0.01). Cutaneous lesions significantly linked to older-onset patients were SCLE (papulosquamous type; OR = 6.05, 95%CI = 2.2–16.64, p < 0.001) and CCLE (i.e. DLE; OR = 1.71, 95%CI = 1.21-2.42, p = 0.002, lupus profundus; OR = 6.56, 95%CI = 1.56–27.51, p = 0.01). Conversely, malar rash (OR = 0.2, 95%CI = 0.13–0.3, p < 0.001), nonscarring alopecia (OR = 0.3, 95%CI = 0.2–0.46, p < 0.001), scarring alopecia (OR = 0.06, 95%CI = 0.01–0.63, p = 0.019) and Raynaud’s phenomenon (OR = 0.17, 95%CI = 0.05–0.55, p = 0.003) were negatively associated with late-onset cases.
Variables independently associated with adult- and late-onset SLE patients by multivariable logistic regression analysis.
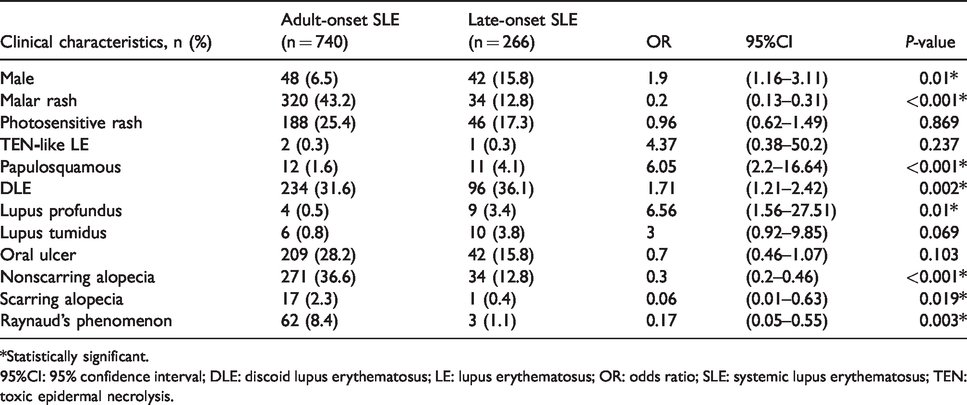
*Statistically significant.
95%CI: 95% confidence interval; DLE: discoid lupus erythematosus; LE: lupus erythematosus; OR: odds ratio; SLE: systemic lupus erythematosus; TEN: toxic epidermal necrolysis.
Table 4 compares disease activity, damage index, systemic involvement and laboratory characteristics between the adult- and late-onset SLE patients. SLEDAI-2K > 6 indicating severe disease was significantly higher in the adult-onset SLE group (n = 599, 80.9% vs. n = 138, 51.9%, p < 0.001), while mild SLE disease activity (SLEDAI-2K < 3) was predominantly found in late-onset SLE cases (n = 98, 36.8% vs. n = 61, 8.2%, p < 0.001). Although there was a trend towards a higher percentage of patients with any organ damage (SLICC/ACR-DI score of ≥1) in the adult-onset group, it did not reach statistical significance (p = 0.127). Besides, the median SLICC/ACR-DI was not different between groups. Systemic involvement was remarkably more common in adult-onset SLE. Anemia (n = 534, 72.2% vs. n = 116, 43.6%, p < 0.001), hemolytic anemia (n = 109, 14.7% vs. n = 20, 7.5%, p = 0.003), leukopenia (n = 490, 66.2% vs. n = 131, 49.2%, p < 0.001) and lymphopenia (n = 463, 62.6% vs. n = 13,350%, p < 0.001) occurred significantly higher in adult-onset SLE. For the renal involvement, the presence of proteinuria was greater in adult-onset SLE (n = 564, 76.2% vs. n = 153, 57.5%, p < 0.001). Moreover, severe proteinuria (>1500 mg) was significantly more prevalent in adult-onset SLE patients (n = 249, 33.6% vs. n = 30, 11.3%, p = 0.002). Arthritis was also observed more frequently in adult-onset SLE (n = 475, 64.2% vs. n = 126, 47.4%, p < 0.001). Likewise, neurological involvement was more common in adult-onset SLE (n = 182, 24.6% vs. n = 38, 14.3%, p < 0.001). However, the presence of serositis was not different between the two groups.
Systemic involvement and laboratory characteristics in adult- and late-onset SLE.
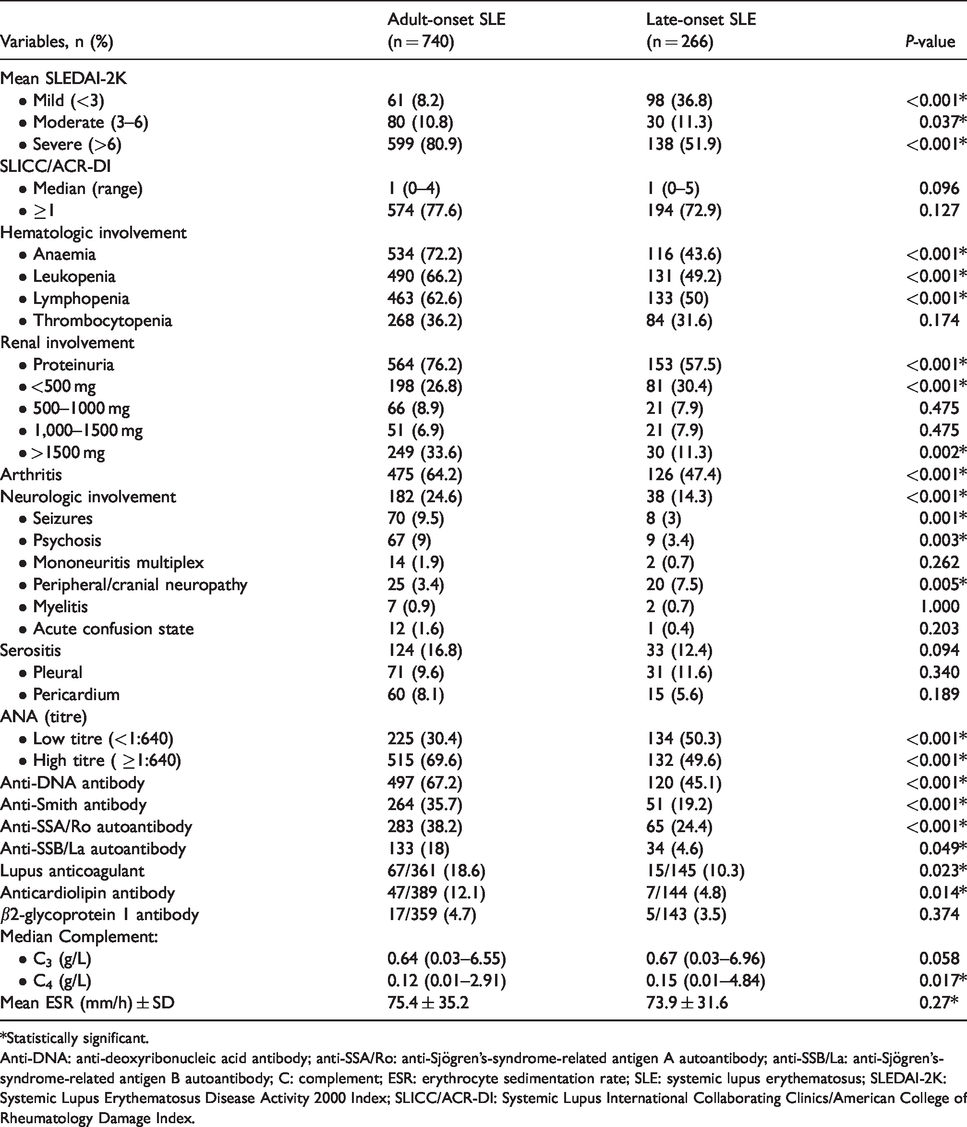
*Statistically significant.
Anti-DNA: anti-deoxyribonucleic acid antibody; anti-SSA/Ro: anti-Sjögren's-syndrome-related antigen A autoantibody; anti-SSB/La: anti-Sjögren's-syndrome-related antigen B autoantibody; C: complement; ESR: erythrocyte sedimentation rate; SLE: systemic lupus erythematosus; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity 2000 Index; SLICC/ACR-DI: Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index.
With regards to laboratory characteristics, late-onset SLE presented with low ANA titer (<1:640) were more commonly demonstrated than adult-onset SLE (n = 134, 50.3% vs. n = 225, 30.4%, p < 0.001), whereas high ANA titer (≥1:640) was significantly found in the adult-onset SLE patients (n = 515, 69.6% vs. n = 132, 49.6%, p < 0.001). Anti-DNA antibody, anti-Sm antibody, anti-SSA/Ro autoantibody and anti-SSB/La autoantibody were more commonly observed in adult-onset SLE, p < 0.05. Antiphospholipid antibodies consisting of lupus anticoagulant and anticardiolipin antibody were also found more often in the adult-onset group, p < 0.05. There was no between-group difference in the median C3 level; however, the median C4 level was significantly lower in adult-onset SLE (0.12 (0.01–2.91) vs. 0.15 (0.01–4.84), p = 0.017). The mean ESR level was not different between the two groups.
Table 5 compares mean SLEDAI-2K in relation to the presence of cutaneous manifestations. ACLE, CCLE, mucosal involvement, and non-specific cutaneous lesions were associated with higher SLEDAI-2K in adult-onset SLE with statistical significance (p < 0.001). However, late-onset SLE patients presenting any with CCLE had lower disease activity score (p = 0.016). Hair loss was significantly associated with higher SLEDAI-2K (p < 0.001) in both groups.
Association between cutaneous manifestations and SLE disease activity in adult- and late-onset SLE.
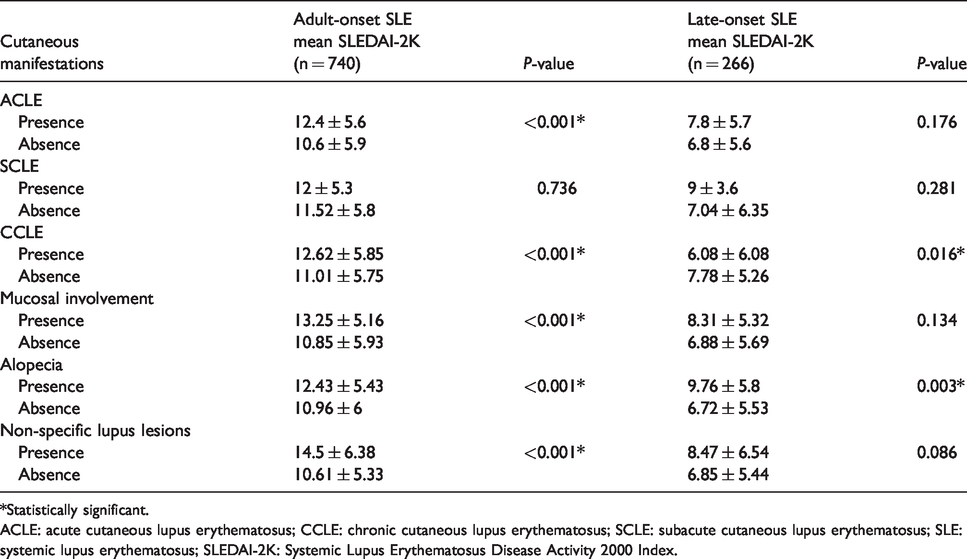
*Statistically significant.
ACLE: acute cutaneous lupus erythematosus; CCLE: chronic cutaneous lupus erythematosus; SCLE: subacute cutaneous lupus erythematosus; SLE: systemic lupus erythematosus; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity 2000 Index.
Discussion
A large number of patients in the present study provides solid evidence that late-onset Thai SLE patients had a distinct disease expression with milder disease activity and fewer systemic involvement. We were also able to identify that ACLE was more common in the adult-onset SLE, while CCLE was more common in late-onset patients. Moreover, certain cutaneous signs were associated with higher disease activity and may hold prognostic values for SLE patients. From this study, late-onset SLE occurred in 26.4% of our SLE cohort, which was relatively higher than previously reported.5–7 However, a prevalence as high as 39% has been documented in the Spanish population. 7 This may be due to dissimilarities in ethnicity, geographical areas, environmental factors, and the number of geriatric populations among different studies. Thailand and Spain have similarly high sunshine hours per day (approximately 11 h). Therefore, we may possibly have a comparable accumulative rate of damage generated by UV radiation through the lifetime, predisposing to a similar prevalence of photosensitive disorders such as lupus in the older population. 25 , 26 Moreover, according to the statement from the Department of Economic and Social Affairs Population Division, United Nations in 2019, Thailand has higher older residents than most countries and similar to the Spanish population. Thailand also has the second most rapidly expanding aging population in South-Eastern Asia after only Singapore, a growth far faster than other countries in this region. 27 Moreover, better access to health care, increase awareness of late-onset SLE, and increase serological monitoring may also reflect a high incidence from our study.
Our data showed that SLE exhibited a female predilection for both the adult- and late-onset cases. However, we found a reduction in the female to male ratio in the late-onset group (5:1) compared to the adult-onset group (14:1). Our multivariable logistic regression analysis also confirmed that male gender was associated with late-onset SLE. This data is in line with the literature. 6 ,28–31 Hormonal factors may play an important role in the pathogenesis of SLE.32–36 Androgen has been postulated to be anti-inflammatory. Hypoandrogenicity has been described in many chronic diseases, including SLE. 37 Reduction of estrogen in postmenopausal woman and a possible protective role of androgen may be associated with decreased incidence in women and an increase in men with advancing age.
Cutaneous manifestations were common in both groups (80.1% in adult- and 71.1% in the late-onset SLE). We confirm the observation by Catoggio et al and Padovan et al. that late-onset SLE patients had slightly less mucocutaneous manifestations. 38 , 39 However, Jarukitsopa et al. demonstrated that CLE was three times more common in the elderly population. 28 Our multivariable logistic regression analysis revealed that cutaneous features significantly associated with older SLE were papulosquamous SCLE and CCLE (i.e. DLE, lupus profundus). On the contrary, ACLE (malar rash) and several lupus nonspecific lesions (e.g. nonscarring alopecia, RP) were more commonly observed in adult-onset SLE. Data from the literature is rather inconsistent regarding the major cutaneous manifestation between adult- versus late-onset SLE. Our results are in line with Sassi et al., Catoggio et al. and Sohn et al. regarding ACLE, oral ulcers, and/or RP, being more common in the adult-onset group. 6 , 38 , 40 However, in their data CCLE (discoid rash) was noted indifference among different age groups. 6 , 38 , 40 Previous studies used the ACR 1997 classification criteria to define SLE patients; therefore, the differences among additional lupus-specific cutaneous subtypes presented in the SLICC 2012 and EULAR/ACR 2019 were not analyzed. 6 , 38 ,40–44 Moreover, most literature reports on cutaneous findings among distinctive age groups were performed by non-dermatologists mostly lacking histopathologic confirmation and may have missed uncommon forms of CCLE e.g. lupus profundus, lupus tumidus ect.
With regards to internal organ damage, our study demonstrated that late-onset patients had fewer hematologic, renal, joint, and neurological involvement, which paralleled the lower SLEDAI-2K. We also found lower ANA titer, fewer autoantibodies (i.e. anti-DNA, anti-Sm, anti-SSA, anti-SSB), including antiphospholipid antibodies (i.e. lupus anticoagulant, anticardiolipin), and higher complement levels in the late-onset group. The milder clinical manifestations and systemic involvement may in part explain the longer time to diagnosis in late-onset SLE patients compared to early-onset, as also previously reported. 38 , 39 As we found significantly less lupus-related serologies in the older SLE patients, perhaps the true difference in autoantibody formation among the age groups may reflect phenotype differences. Senescence of the immune system with aging may contribute to the differences in disease manifestations and the generally milder course in late-onset SLE patients. 45
Certain skin signs such as malar rash correlate with systemic involvement and may signal prognostic implication for SLE. 18 To the best of our knowledge, we are the first to determine whether particular cutaneous manifestations were linked to the disease severity in the adult- versus late-onset SLE patients. We demonstrated that the presence of ACLE, CCLE, oral ulcers, and lupus non-specific lesions were associated with higher disease activity in adult-onset SLE. Hair loss was a marker for greater severity in both groups. Intriguingly, we have demonstrated for the first time that older onset SLE patients presenting with CCLE had significantly lower SLEDAI-2K. Therefore, CCLE may possibly serve a protective marker in this age group.
The present study may have had several limitations. First, the study was analyzed retrospectively; selection and recall bias as well as incompleteness of data may have occurred. Some of the clinical and laboratory findings may have been related to the different length of follow-up. Second, we conducted a relatively large study in a homogenous population, the Southeast Asian descent, hence, a uniform population analysis was performed. However, the results may not be universally applicable to all ethnicities. Third, our rigid patient selection criteria resulted in a decent number of patients eliminated from this study. Finally, the administration of certain medications (corticosteroids/immunosuppressants) may have had an impact on variables related to the disease activity; however, the present study did not consider therapeutic management in our study cohort. Further detailed analyses in prospective studies are required to confirm our results.
In conclusion, late-onset SLE patients have a unique clinical expression compared to the adult-onset group showing male preponderance and milder disease characterized by fewer systemic involvement and lower disease activity index. The importance of thoroughly examining for cutaneous manifestations should be greatly emphasized, as it is fundamental for establishing the diagnosis and holds prognostic values for both late- and adult onset SLE patients. Finally, age of disease onset of SLE may be considered in developing an individualized clinical approach and disease monitoring to optimize the treatment strategies for SLE patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study was approved by the Institutional Review Board of the Faculty of Medicine, Ramathibodi Hospital, Mahidol University (MURA 2018/313).
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.