
Abstract
Objectives
The antiphospholipid syndrome (APS) is an autoimmune disease associated with thrombotic and non-thrombotic neurologic manifestations. APS is classified as primary (PAPS) or secondary (SAPS) when it co-exists with another autoimmune disease. We aim to describe the spectrum of acute cerebrovascular disease among patients with APS, their differences between stroke subtypes, and long-term functional outcomes.
Methods
Retrospective cohort study including adult (≥18 years) patients with APS followed in the stroke clinic of a tertiary-care reference center for autoimmune diseases in Mexico from 2009 to 2019.
Results
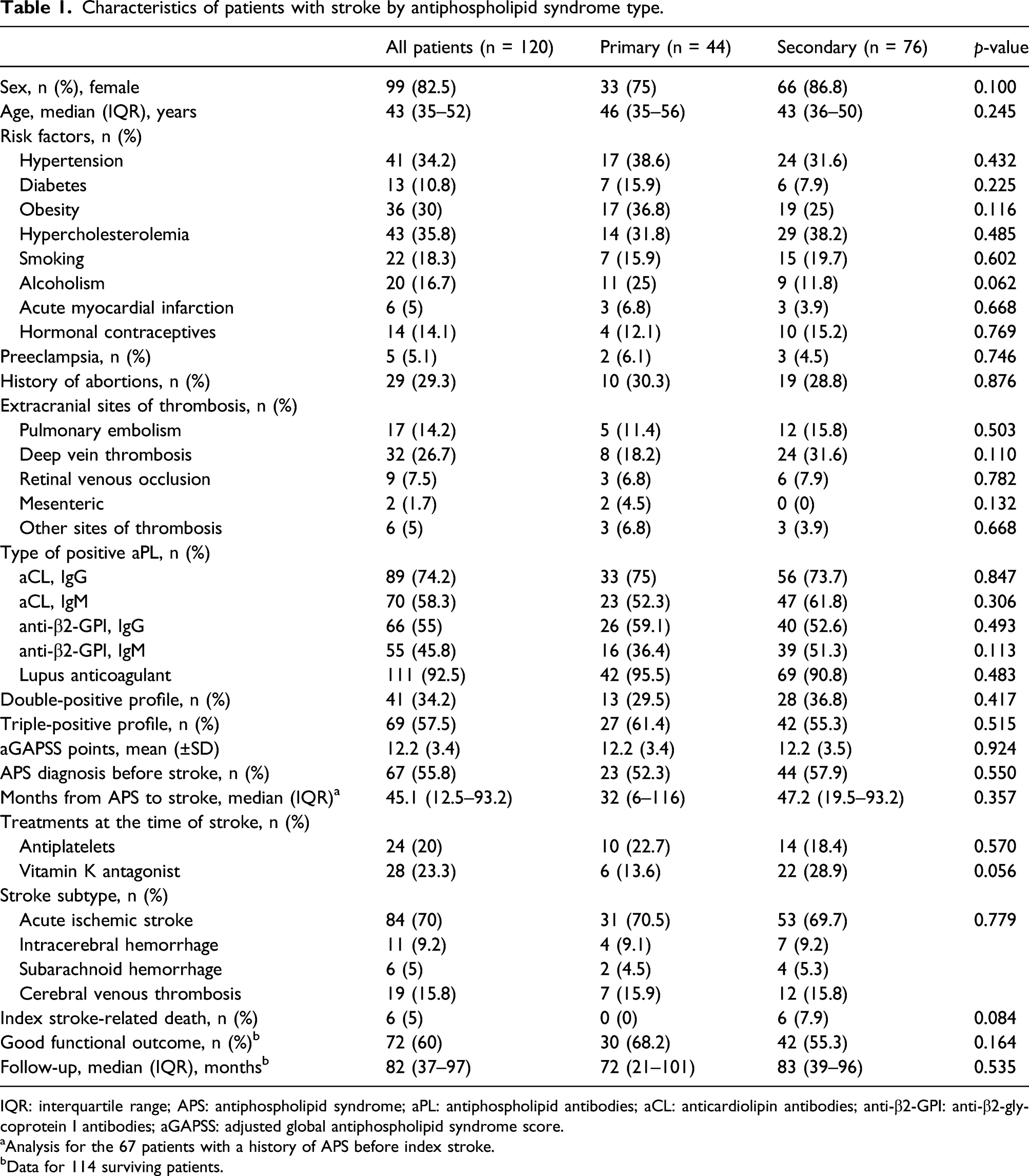
We studied 120 cases; 99 (82.5%) women; median age 43 years (interquartile range 35–52); 63.3% with SAPS. Demographics, comorbidities, and antiphospholipid antibodies (aPL) positivity were similar between APS type and stroke subtypes. Amongst index events, we observed 84 (70%) acute ischemic strokes (AIS), 19 (15.8%) cerebral venous thromboses (CVT), 11 (9.2%) intracerebral hemorrhages (ICH), and six (5%) subarachnoid hemorrhages (SAH). Sixty-seven (55.8%) were known patients with APS; the median time from APS diagnosis to index stroke was 46 months (interquartile range 12–96); 64.7% of intracranial hemorrhages (ICH or SAH) occurred ≥4 years after APS was diagnosed (23.5% anticoagulation-related); 63.2% of CVT cases developed before APS was diagnosed or simultaneously. Recurrences occurred in 26 (22.8%) patients, AIS, in 18 (69.2%); intracranial hemorrhage, in eight (30.8%). Long-term functional outcomes were good (modified Rankin Scale ≤2) in 63.2% of cases, during follow-up, the all-cause mortality rate was 19.2%.
Conclusion
We found no differences between stroke subtypes and APS types. aPL profiles were not associated with any of the acute cerebrovascular diseases described in this cohort. CVT may be an initial thrombotic manifestation of APS with low mortality and good long-term functional outcome.
Keywords
Introduction
The antiphospholipid syndrome (APS) (also known as Hughes syndrome) is a systemic autoimmune disease characterized by arterial or venous thrombosis and/or pregnancy morbidity in the presence of persistently positive circulating antiphospholipid antibodies (aPL).1,2 APS may be classified as primary (PAPS) or secondary (SAPS) when it co-exists with another systemic autoimmune disease.1,3 Both syndromes are associated with a broad spectrum of neurologic and non-neurologic thrombotic manifestations and pose a high risk for recurrence.4,5 Among APS patients, the most common acute cerebrovascular disease (stroke) subtype is acute ischemic stroke (AIS), followed by transient ischemic attacks (TIA) and cerebral venous thrombosis (CVT). In addition, intracranial hemorrhage (intracerebral hemorrhage [ICH] or subarachnoid hemorrhage [SAH]) has been mostly reported as a consequence of antithrombotic treatments.4,6 Although APS has been studied for almost four decades, information about APS-patients characteristics, stroke subtypes, lesion topography, concurrent causes, and long-term outcomes is limited to a few case series. Therefore, the objective of this study is to describe the spectrum of acute stroke among patients with APS, the differences between APS type and stroke subtypes, and their long-term functional outcomes in a cohort of patients followed in a stroke clinic over a 10-year period.
Methods
Study design, setting, and patient selection
This observational retrospective cohort study was conducted at the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, a tertiary-care reference center for autoimmune diseases in Mexico. The study was revised and approved by our institutional Ethics and Research Committees (Reference NER-2046-16-17-1). Due to the nature of the study, both Committees waived the need for signed informed consent. We reviewed electronic medical records of all patients aged ≥18 years with a history of an acute stroke, and APS followed in our outpatient stroke clinic from January 2009 to December 2019. We excluded patients not fulfilling the APS classification criteria, cases where the time of APS diagnosis or index stroke could not be accurately determined, and those with missing data regarding neuroimaging studies on the medical records.
Antiphospholipid syndrome diagnosis and treatment
APS diagnosis was made according to the revised Sydney classification criteria. 6 The aPL profile included lupus anticoagulant (LA), anticardiolipin antibodies (aCL), and anti-β2-glycoprotein I (anti-β2-GPI) antibodies. According to recommendations from the International Society on Thrombosis and Hemostasis, IgG and IgM isotypes of anti-β2-GPI and aCL in serum or plasma were measured by enzyme-linked immunosorbent assay and considered positive in titers >99th percentile of normal controls; LA positivity was determined by dilute Russell viper venom time; positive aPL were confirmed in two or more occasions, 12 weeks after the initial testing.7,8 Cases were categorized according to aPL positivity profile as double-positive (any combination of LA, aCL, or anti-β2-GPI) or triple-positive (all three aPL subtypes).2,9 Patients with co-existing autoimmune diseases were classified as SAPS cases.1,3 To evaluate risk of recurrent AIS we calculated the adjusted global antiphospholipid syndrome score (aGAPSS), which considers aPL positivity (aCL IgG/IgM, 5 points; anti-B2GPI IgG/IgM, 4 points; LA, 4 points) and CVD risk factors (hyperlipidemia, 3 points; hypertension, 1 point).10,11 After the initial diagnosis, patients without contraindications for anticoagulation were treated with vitamin K antagonists (VKA) with a target international normalized ratio (INR) of 2–3.5; 12 or with antiplatelet drugs, according to the attending physician’s criteria. As for cases of intracranial hemorrhage, initial treatment included antiplatelet drugs followed by VKA initiated 4–12 weeks after the event depending on patient characteristics.13,14
Stroke subtypes and clinical outcomes
Stroke subtypes were classified according to the 2013 American Heart Association/American Stroke Association Updated Definition of Stroke as AIS, TIA, CVT, ICH, or SAH, and confirmed by either computed tomography (CT), magnetic resonance imaging (MRI) with angiography/venography, or digital subtraction angiography (DSA), as deemed appropriate. 15 Besides presence of circulating aPL, the approach to determine other causes of AIS included a transthoracic or transesophageal echocardiogram, an electrocardiogram, 24-h Holter monitoring, assessment of the carotid/vertebral arteries by duplex ultrasound, and intracranial vessels by transcranial Doppler ultrasound. Testing for other prothrombotic states was performed according to attending neurologist criteria. The approach for all CVT cases included testing for antithrombin III, protein C and S deficiency, hyperhomocysteinemia, factor V Leiden and prothrombin gene (G20210A) mutations, aside from considering other related conditions (e.g., pregnancy and puerperium, oral contraceptives, drugs, or cancer), as proposed by expert international consensus. 16 As for intracranial hemorrhage (ICH and SAH), we included other possible causes after excluding CVT, such as severe thrombocytopenia (platelet count ≤20 × 109/L), over-anticoagulation (INR ≥4.5), hypertension, trauma, and ruptured aneurysm.17,18 All cases were evaluated in consensus by two experienced vascular neurologists (C.C-B and F.D.F-S). Stroke-related death was defined as that occurring within the first 30 days after the event. 19 Follow-up functional outcome was assessed using the modified Rankin scale (mRS) and defined as good (mRS ≤1) or poor (mRS ≥2). 20
Data collection
De-identified data were extracted from electronic medical records using a standardized case report format and entered into a secure online database. Data collection included age, sex, cardiovascular disease (CVD) risk factors including hypertension, diabetes, obesity (BMI ≥30 kg/m2), hypercholesterolemia, smoking, alcoholism, history of myocardial infarction, and use of corticosteroids and hormonal contraceptives drugs at the time of index stroke. We also registered the history of APS-related obstetric complications (abortions and preeclampsia) and extracranial sites of thrombosis (arterial or venous) at the time of the first (index) stroke; aPL positivity (LA, IgG/IgM aCL, and IgG/IgM anti-β2-GPI) and titers at the time when APS was confirmed, co-existence of another rheumatic autoimmune disease such as systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), Sjögren’s syndrome (SS), mixed connective tissue disease (MCTD), or systemic sclerosis (SSc), diagnosed before or during the study period; the interval in months from APS diagnosis to index stroke and first recurrence, stroke subtype, neuroimaging studies, for AIS cases we recorded the presence of carotid and intracranial atherosclerosis, determined by any imaging study as either present or absent and categorized it by the percentage of stenosis (≤50% or >50%); also, the involved arterial territories; diagnostic approach for all stroke subtypes, use of VKA or antiplatelet drugs before the events, platelet count and INR level at the time of presentation; in-hospital mortality, long-term clinical outcome, and interval in months from index stroke to last follow-up visit. Two researchers reviewed all data, and a third researcher adjudicated any difference in interpretation between the two primary reviewers.
Statistical analysis
We compared the characteristics of patients with PAPS or SAPS and index events; recurrences were analyzed independently. To analyze the differences between stroke subtypes, we categorized them as AIS, intracranial hemorrhage (ICH or SAH), and CVT. Categorical variables are reported as frequencies and proportions; continuous variables as median with interquartile range (IQR) or mean with standard deviation (SD). Analyses of categorical variables were performed with the χ2 or Fisher’s exact tests; non-parametric continuous variables with the Mann–Whitney U test or Kruskal–Wallis test; normally distributed continuous variables using the t-test for unpaired data, or analysis of variance, as appropriate. Kaplan–Meier survival curves were created to assess the overall mortality by stroke subtypes during the 5 years after the event and analyzed using the log-rank test. All p-values were two-tailed and considered significant when <0.05. Statistical analyses were performed with IBM SPSS Statistics, version 26 (IBM Corp., Armonk, NY, USA), and statistical figures were created using GraphPad Prism, version 9 (GraphPad Software, La Jolla, CA, USA).
Results
Characteristics of patients with stroke by antiphospholipid syndrome type.
IQR: interquartile range; APS: antiphospholipid syndrome; aPL: antiphospholipid antibodies; aCL: anticardiolipin antibodies; anti-β2-GPI: anti-β2-glycoprotein I antibodies; aGAPSS: adjusted global antiphospholipid syndrome score.
aAnalysis for the 67 patients with a history of APS before index stroke.
bData for 114 surviving patients.
Antiphospholipid syndrome type
Regarding the APS type, SAPS was frequent (63.3%), with SLE accounting for 96% (73 patients) of cases; co-existence of SLE with another autoimmune disease was detected in two patients (RA and secondary SS, respectively). Other causes included primary SS, SSc, and MCTD, one case each. Demographics and CVD risk factors were similar, as well as the proportion of patients with a known history of APS, extracranial thrombosis (PAPS 38.6% vs. SAPS 42.1%, p = 0.709), or preventive treatments (Table 1). There were no statistical differences between aPL subtypes, positivity profiles, or titers between groups (Table S1). Supplemental Table S2 shows aPL titers by stroke subtype. Among patients with a known history of APS, the median time from APS diagnosis to index stroke was 46 months (IQR 12–96), and in 15.8%, the diagnosis was simultaneous (Figure 1). Index stroke subtypes and stroke-related death rates were similar between APS types (Table 2). Temporality of stroke subtype with the diagnosis of antiphospholipid syndrome. APS: antiphospholipid syndrome. Characteristics of patients with antiphospholipid syndrome by stroke subtype. IQR: interquartile range; APS: antiphospholipid syndrome; aPL: antiphospholipid antibodies; aCL: anticardiolipin antibodies; anti-β2-GPI: anti-β2-glycoprotein I antibodies; aGAPSS: adjusted global antiphospholipid syndrome score. aAnalysis for the 67 patients with a history of APS before index stroke. bData for 114 surviving patients.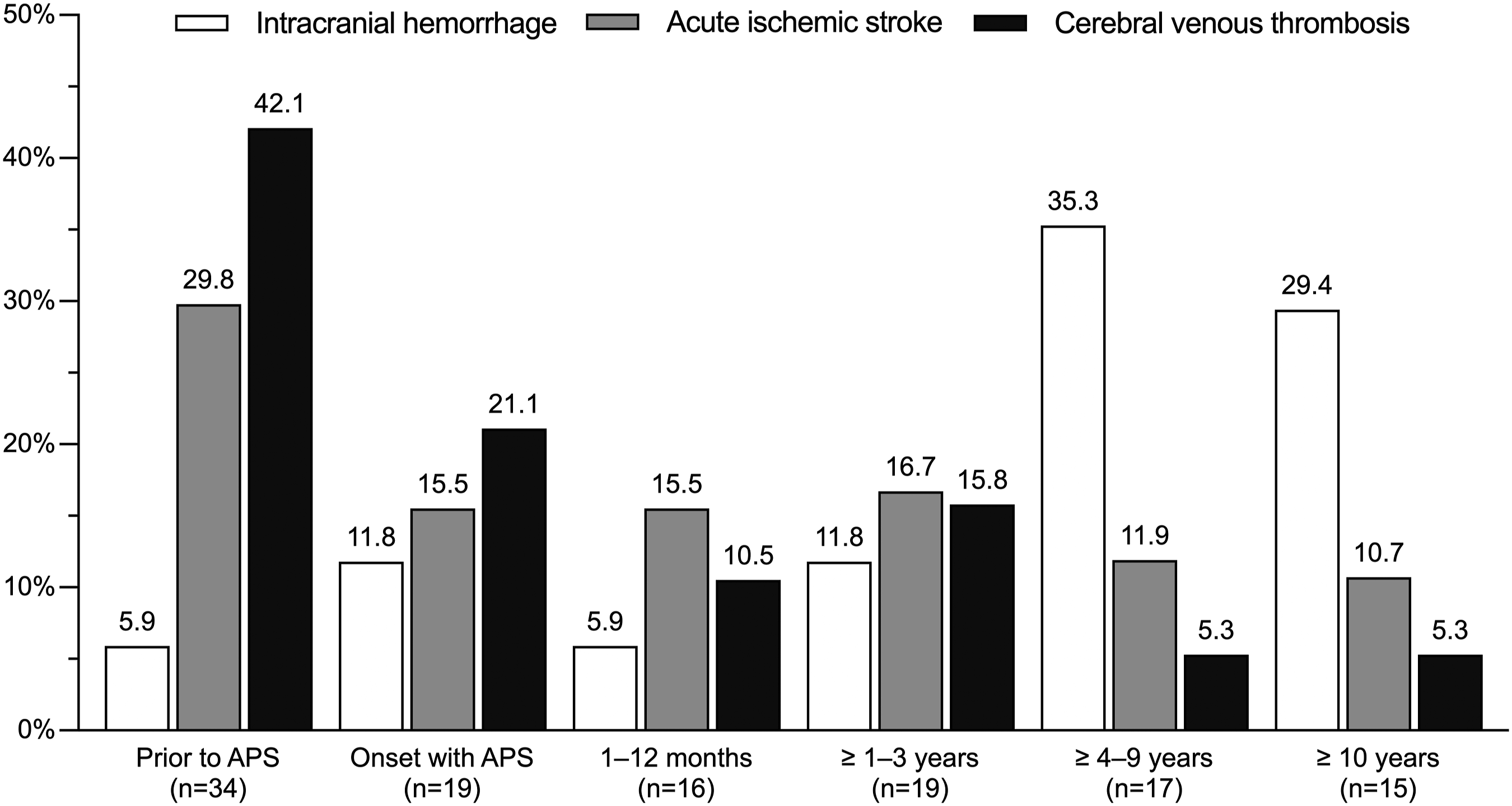
Index stroke subtypes
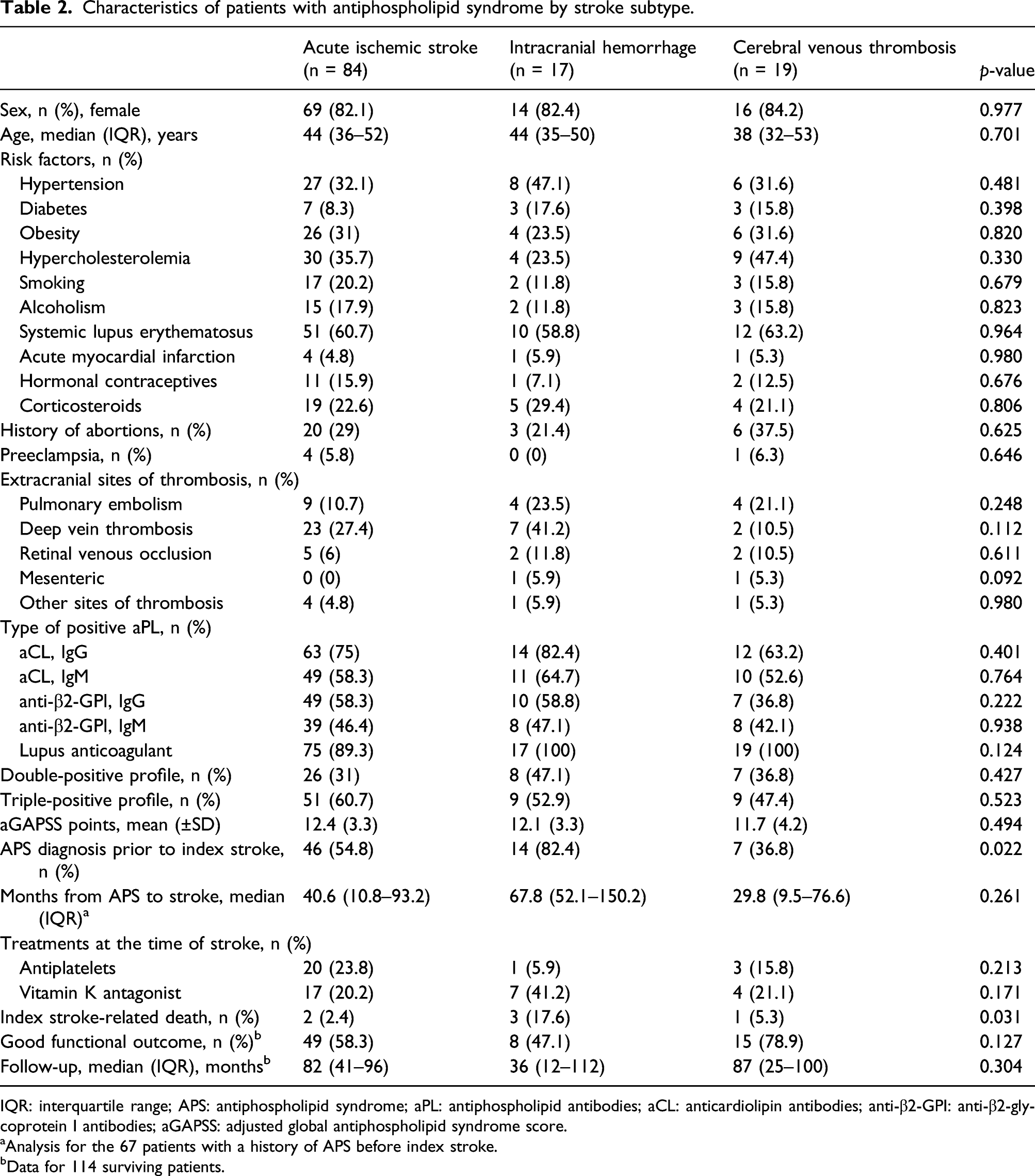
Of the 84 patients with AIS, four (4.8%) had a history of TIA, and 46 (54.8%) were known patients with APS; the median time from APS diagnosis to AIS was 40.6 months (IQR 10.8–93.2). Twelve (14.3%) patients had atherosclerosis without statistical differences between the type of APS (PAPS 16.1% vs. SAPS 13.2%, p = 0.753); in three of them, the stenosis was >50%; the internal carotid artery in two and the middle cerebral artery (MCA) in one more. A cardioembolic source was detected in 11 (13.1%) patients; six cases were secondary to Libman–Sacks endocarditis, four to valve disease (mitral stenosis in three; prosthetic aortic valve in one more), and one was classified as a paradoxical embolism due to an atrial septal defect, cardioembolism was more frequent in SAPS patients, but without statistical differences (17% vs. 6.5%, p = 0.201). None had known atrial fibrillation (KAF) or atrial fibrillation detected after stroke (AFDAS). Other prothrombotic states were tested in 27/84 (32.1%) patients; the performed approach was negative for all. Of the 17 patients taking VKA, five (29.4%) were within therapeutic goals of anticoagulation. On neuroimaging, bilateral lesions were detected in 24 (28.6%) patients; 19 (22.6%) had multivessel disease, and 33 (39.3%) had multiple lesions. Fifty-one (60.7%) had anterior circulation lesions, 18 (21.4%) had posterior circulation lesions, and 15 (17.9%) had lesions in both. The MCA territory was the most commonly involved in 62 (73.6%) patients, followed by the posterior cerebral artery in 15 (17.9%). Figure 2 shows the overall distribution of the lesions, and Supplemental Table S3 their differences between APS types. Distribution and frequency of acute ischemic stroke lesions by arterial territories. (A) Frequency of the lesions by their main arterial vascular territory and infratentorial structures. (B) Frequency of the lesions located within the territory of the main cerebral arteries perforating branches. (C) Frequency of subcortical lesions (includes watershed infarcts and non-specific white matter lesions) located within the territory of the main cerebral arteries perforating branches. (D) Frequency of lesions (cortical/subcortical) involving a well-defined vascular territory. ACA: anterior cerebral artery; MCA: middle cerebral artery; PCA: posterior cerebral artery.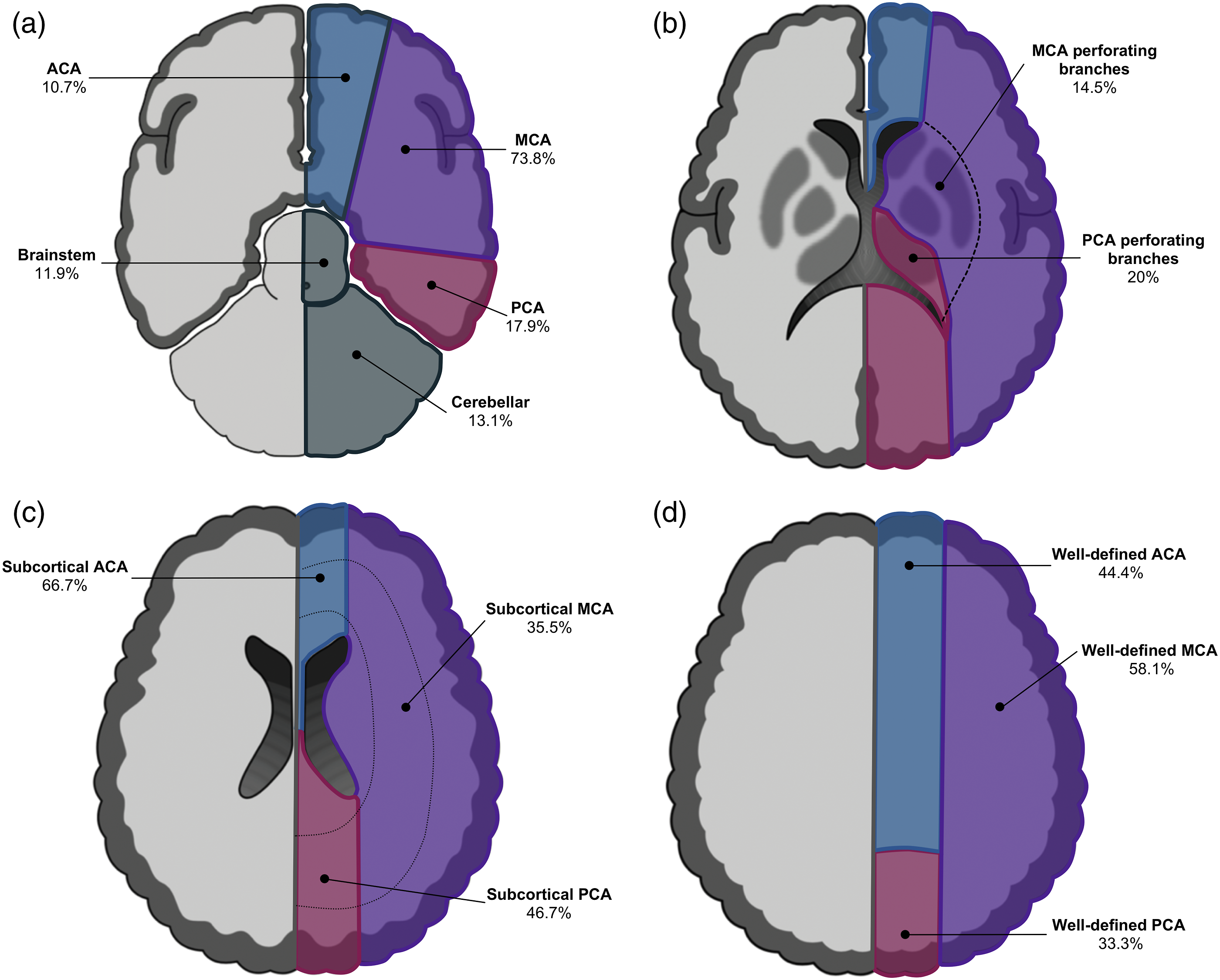
Among the 19 patients with CVT, the index event occurred before or at the time of APS diagnosis in 66.2% of cases (Figure 2); the median time from APS diagnosis to CTV was 29.8 months (IQR 9.5–76.6). None tested positive for other prothrombotic states; at the time of the event, two out of four patients taking VKA were within therapeutic goals. The superior sagittal sinus (8/19, 42.1%) was the most common site involved, followed by the transverse (lateral) sinus (6/19, 31.6%), deep cerebral venous system (3/19, 15.8%), and cortical veins (2/19, 10.5%); four had a concomitant hemorrhagic component (superior sagittal sinus in three; transverse sinus in one), none of them were anticoagulated at the time of CVT onset.
There were 17 cases of intracranial hemorrhage, 14 (82.4%) in patients with a known history of APS, within a median time of 67.8 months (IQR 52.1–150.2) after the diagnosis. Of all hemorrhages, 11 were ICH, seven were lobar, three were within the basal ganglia, and one was intraventricular; five patients were taking VKA. Putative causes included severe thrombocytopenia (lobar in two cases; basal ganglia and intraventricular in one case each), uncontrolled hypertension (basal ganglia and lobar; two cases each), and three were over-anticoagulation-related (lobar in all cases). In addition, there were six SAH cases; two were related to an intracranial aneurysm located within the right proximal MCA and right anterior communicating artery in one case each, two more were associated to severe thrombocytopenia, located within the frontoparietal region (bilateral) and the right parieto-occipital sulcus (one case each), one case was due to over-anticoagulation (anterior interhemispheric fissure), and in one, the mechanism remained undetermined (perimesencephalic); none had a history of recent trauma. Among patients receiving VKA, over-anticoagulation accounted for 23.5% (4/17) of intracranial hemorrhages.
Clinical outcome
There were six (5%) index stroke-related deaths; the median follow-up time for the 114 surviving patients was 82 months (IQR 37–97). During follow-up, the all-cause mortality rate for the entire cohort was 19.2% (stroke-related in 10 [8.3%] cases and non-stroke–related in 13 [10.8%]), which was significantly higher in those who suffered an intracranial hemorrhage either during index stroke or during follow-up, and the 5-year survival probability was higher for patients with CVT (Figure 3(a)). Among the 13 patients who died of a non-stroke-related cause during follow-up, eight deaths were associated with an infectious cause, two were related to status epilepticus, one due to acute gastrointestinal bleeding, decompensated chronic heart failure, and chronic kidney disease in one case each. Long-term functional outcome was good for 72 (63.2%) and poor for 42 (36.8%) of the index stroke survivors. Patients diagnosed with CVT had a better functional prognosis than those with other stroke subtypes (Figure 3(b)). Mortality over time and functional outcome during follow-up. (a) Kaplan–Meier analysis of 5-year mortality according to stroke subtype. (b) Overall long-term functional outcome during the median follow-up time of 82 months (interquartile range 37–97 months) by stroke subtype.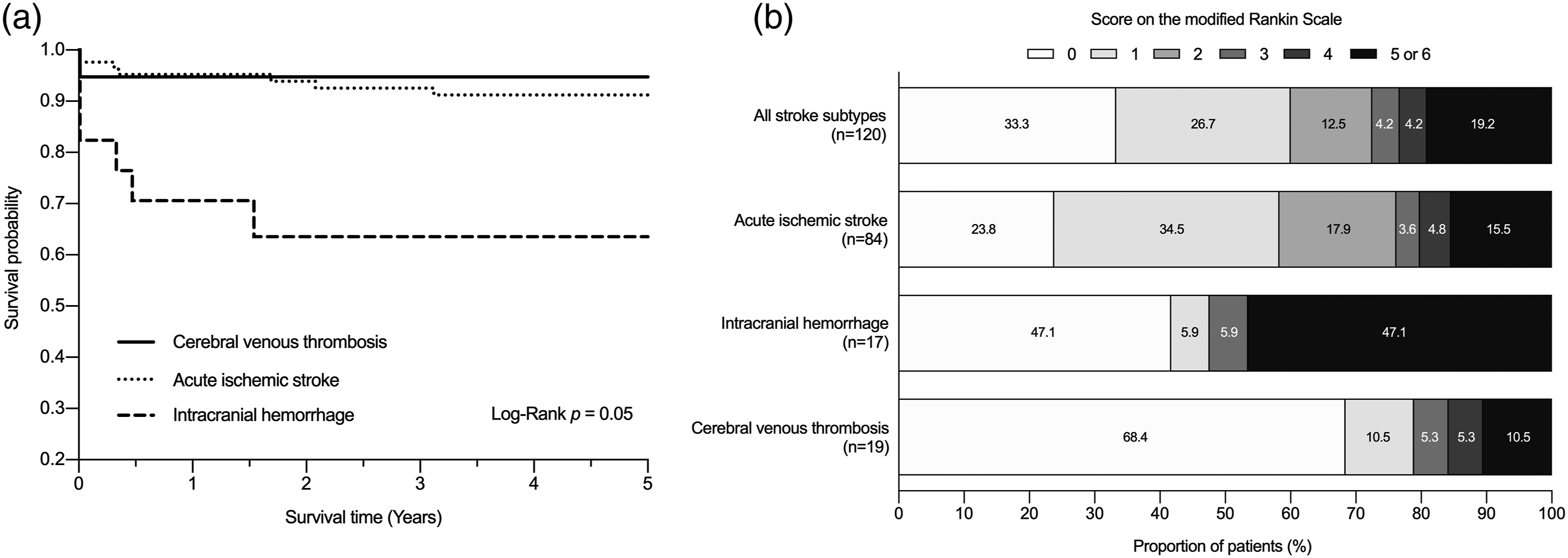
Recurrences
Twenty-six patients (22.8%) had recurrent events (PAPS 25% vs. SAPS 19.7%, p = 0.5) within a median time of 37.8 months (IQR 25–57). There were 18 (69.2%) cases of AIS (median time to recurrence 35.5 months, IQR 25–55), 16 were taking VKA, but only six (37.5%) were within therapeutic goals. Intracranial hemorrhage occurred in eight (30.8%) patients (ICH, in seven; SAH, in one) within a median time of 49.5 months (IQR 27–63.5); six were taking VKA, four within therapeutic ranges, and two were over-anticoagulated, none had thrombocytopenia. There were no recurrent cases of CVT. Recurrent stroke subtypes and APS type were similar (p = 0.741).
Of the initial 84 cases of AIS, 14 (16.7%) had a recurrent arterial event; five (41.7%) out of 12 patients taking VKA were within anticoagulation goals; two were diagnosed with Sneddon syndrome with skin biopsy after the initial event. The proportion of patients according to APS type was similar (PAPS 7/31, 22.6% vs. SAPS 7/31; p = 0.266). On univariable analysis, there were no statistical differences of mean aGAPSS points between recurrent and non-recurrent AIS patients (13.9 ± 2 vs 12.1 ± 3, p = 0.065). There were four deaths related to stroke recurrence; three occurred in patients with ICH.
Discussion
This study describes the spectrum of APS-related acute stroke in a national tertiary-care reference center for autoimmune diseases. Interestingly, most SAPS cases in our cohort were SLE-related (96%), a well-known risk factor for intracranial thrombotic events and atherosclerosis;21–23 however, there were no differences between APS types and stroke subtypes, aPL positivity profiles, recurrences, or long-term functional prognosis. Similar to the reported in the Euro-Phospholipid Project, which included patients with PAPS and SAPS, AIS was the most frequent stroke subtype in our cohort. 6 In the present study, CVT was the second most common type of stroke, while TIA’s took this place in their cohort. This finding may be due to differences in methodological approaches or because in our center, the diagnosis and reference of TIA’s to the stroke clinic relied upon attending physician criteria, and as we only detected four patients who later developed an AIS, we took the latter as the qualifying event.
The timing from APS diagnosis to stroke onset was highly variable; most intracranial hemorrhages occurred ≥4 years after the diagnosis, despite a low frequency of anticoagulation-related hemorrhages. On the other hand, AIS occurred early in 45% of cases (before or at the time of APS diagnosis) or late after several years of the course of the APS, and most CVT cases (63%) developed before or at the time of APS diagnosis, suggesting that CVT may be the first clinical manifestations of APS. Also, it has been reported that LA positivity increases the risk for AIS; 24 however, we detected LA in 92.5% of our studied population, including those with intracranial hemorrhage and CVT. Interestingly, we found no differences between CVD risk factors or aPL profiles and stroke subtypes. The aforementioned suggests that multiple potentially preventable systemic factors, not solely APS, may cause the spectrum of cerebrovascular diseases hereby described.
Among our 84 index AIS cases, 22.6% had multivessel disease, and lesions of the MCA territory accounted for 73.6% of cases, comparable with the 68% reported in a series analyzing the lesion topography of 25 patients. 25 Additionally, 34.5% of our cases had lesions of the large vessels perforating branches. In a study of 53 patients with PAPS using the Oxfordshire Community Stroke Project classification system, clinically, the lesion was located within the posterior circulation in 22.6% of their patients, 26 whereas when taking into account multivessel disease restricted to the posterior circulation (including vertebral and basilar arteries perforating branches), we found a frequency of 42.9%. This high proportion of simultaneous involvement of several arterial territories and vessel size shows that the cerebral arterial system can be globally affected in APS.
APS patients develop endothelial cell dysfunction during the early stages of the disease, followed by accelerated systemic atherosclerosis and microvascular endothelial dysfunction that may also present as small vessel disease,5,27 which in some series of APS and non-APS patients has shown to predict cognitive impairment.28,29 Atherosclerosis was detected in 14.3% of AIS cases without differences between APS types, falling within the reported frequency by other authors among APS patients, regardless of the type.30–32 Furthermore, 60% of our patients had an associated CVD risk factor despite a relatively young age or an APS-related cardiac manifestation (e.g., Libman–Sack endocarditis and valvular disease), implying that in APS, multiple AIS etiologies may co-exist, not solely in-situ thrombosis.4,33 Therefore, a broad range of mechanisms should be considered when approaching these patients.
SLE patients have a threefold higher risk for ICH or SAH. 34 However, little is known about intracranial hemorrhage in APS. During the 10-year follow-up of the Euro-Phospholipid Project, 61 (24.6% intracranial) major bleeding episodes were reported, all in patients with antithrombotic treatments. 6 Of our 17 index intracranial hemorrhage cases, over-anticoagulation accounted for 23.5% of these cases, suggesting that intracranial bleeding disorders among these patients are not merely related to anticoagulant complications; other identifiable risk factors included hypertension and platelet disorders; as the exact mechanisms for intracranial hemorrhage in these patients are still unclear, we hypothesize that chronic thrombotic microangiopathy may predispose APS patients for both ICH and SAH in combination with other CVD risk factors, 27 especially in patients with SAPS where the chronic inflammatory state by the underlying autoimmune disease may promote vascular fragility.23,27
Stroke-related mortality in this group of young patients was 8.3%, higher than the 4–5% of stroke-related deaths foreseen for this age group;35,36 however, during long-term follow-up, the overall mortality rate of 19.2% is similar to that of 20% reported among non-APS adults aged 18–50 years during an 11-year follow-up period, regardless of the stroke subtype. 35 As for the functional prognosis, more than 60% of patients with AIS and CVT had a good functional outcome, contrary to those who presented with an intracranial hemorrhage, as expected for the general population within the studied age group.23,36–40
Our AIS recurrence rate (16.7%) falls within the 15–37% reported among APS patients;26,41 despite this high frequency, to date there is no reliable biomarker or prediction tool to help distinguish patients most likely to have a recurrent event. The aGAPSS is a tool that has proven to predict extracranial thrombotic events;10,11 therefore, as there is no defined cut-off value for intracranial events, we explored by univariable analysis if there was a difference in the total score of this prediction tool between patients who had an AIS recurrence and those who did not, finding that there was no statistical difference. Furthermore, despite adequate anticoagulation, our AIS recurrence rate also falls within the 5-year recurrence rate of 14–26% reported in non-APS patients,42,43 reinforcing the need for strict goal-oriented care of comorbidities as in patients without APS.1,34
This study has several limitations. First, due to our retrospective and observational design, where we retrospectively collected data from electronic medical records, we could not accurately determine the acute clinical presentation to assess the significance of the neuroimaging findings herby described, the short-term functional outcome to evaluate its evolution during follow-up, cumulative doses of corticosteroids, as well as treatment strategies, adherence, or INR fluctuations for patients receiving VKA. Second, although the study was conducted in a national reference hospital for autoimmune diseases, as it is a single-center, hospital-based study, our findings may not represent our entire population due to referral bias. In line with the previous limitation, we were unable to record and analyze other well-known risk factors such as pregnancy or puerperium because in our center as standard practice, those cases are referred to a third-level hospital specialized in maternal and child health care; however, none of the cases presented within this timeframe. Third, as anti-phosphatidylserine/prothrombin antibodies (aPS/PT) included in the original global antiphospholipid syndrome score (GAPSS) are not routinely tested in our center, we were unable to evaluate the predictive accuracy of the already validated cut-off values for this version. 44 Last, as APS is a relatively rare disease, in addition to the low number of recurrences we observed, statistical power was limited to accurately evaluate the risk of AIS or CVT recurrences by multivariable analysis or derive cut-off values for the aGAPSS; therefore, our results should be taken with caution.
In conclusion, we found no differences between the analyzed stroke subtypes and the APS type. APL profiles were not associated with any of the acute cerebrovascular diseases hereby described. CVT may be an initial thrombotic manifestation of APS with low mortality and good long-term functional outcome. In this relatively young cohort, well-known CVD risk factors for acute cerebrovascular events were detected in more than half of cases; therefore, close follow-up and strict goal-oriented care of comorbidities are imperative for patients with APS. More extensive prospective studies to detect patients who will develop a recurrent stroke and accurately determine the pathophysiological mechanisms of the different cerebrovascular events that patients with APS can develop are still required.
Data availability
The manuscript provides all the collected data. De-identified data to replicate our results will be available to qualified researchers upon written request to the corresponding author.
Supplemental Material
sj-pdf-1-lup-10.1177_09612033221074178 – Supplemental Material for Antiphospholipid syndrome–mediated acute cerebrovascular diseases and long-term outcomes
Supplemental Material, sj-pdf-1-lup-10.1177_09612033221074178 for Antiphospholipid syndrome–mediated acute cerebrovascular diseases and long-term outcomes by Miguel García-Grimshaw, Diego Ruben Posadas-Pinto, Sergio Iván Valdés-Ferrer, Arturo Cadena-Fernández, Jose Domingo Barrientos-Guerra, Margarita Amancha-Gabela, Erwin Chiquete, Fernando Daniel Flores-Silva and Carlos Cantú-Brito in Lupus
Footnotes
Acknowledgments
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.