
Abstract
Background:
Jaccoud’s arthropathy (JA) is a condition characterized by joint deformities that have a “reducible” pattern, that is, they return to the normal appearance with a passive manoeuvre. JA was described in patients with rheumatic fever (RF) more than a century ago, and presently, the majority of the patients have systemic lupus erythematosus (SLE).
Purpose:
The aim of this review is to draw one attention to the epidemiology, pathogenesis, histopathology, clinical features, imaging, and management of JA in patients with SLE (Jaccoud-type lupus arthropathy).
Data collection:
The search strategy included articles retrieved from PubMed utilizing the terms “lupus arthropathy”, “lupus deforming arthropathy”, “lupus hand”, “lupus foot”, “chronic postrheumatic arthropathy”, “Jaccoud’s” and “Jaccoud” from 1950 until March 2021, with no language restriction.
Results:
The prevalence of Jaccoud-type arthropathy in SLE is approximately 5%. The aetiopathogenic mechanisms of JA are not yet known. The most common joint deformities of JA, are ulnar deviation, swan neck, and the “z” of the thumb. Unfortunately, none of the proposed classification criteria for JA have been validated so far. Characteristically, there is no bone erosion on plain radiographs of the joints, but more sensitive imaging methods, magnetic resonance imaging or high-performance ultrasound may reveal small bone erosions. There is no preventive measure against JA development, specific clinical treatment or convincing surgical approach for correcting the deformities.
Conclusion:
As daily activities and quality of life are compromised in patients with JA, other studies are urgently needed in this area.
Introduction
In 1869, a Swiss physician, Sigismond Jaccoud, made the first clinical description of chronic deforming arthritis appearing after attacks of rheumatic fever (RF) in a 19-year-old man. 1 To pay homage to this author, this arthropathy has been called Jaccoud’s arthropathy (JA).
JA is characterized by joint deformities that resemble those seen in patients with rheumatoid arthritis (RA), such as ‘swan neck’, thumb subluxation, ulnar deviation, ‘boutonniere’ and hallux valgus, but with a ‘reducible’ pattern, that is, the deformities are correctable by passive manoeuvres (Figure 1). Characteristically, there is no bone erosion on plain radiographs of the joints. Classical joint deformities in Jaccoud-type lupus arthropathy. A: ‘Boutonniere’, ulnar deviation and ‘z’ of the thumb. B: Reducible pattern of the deformities.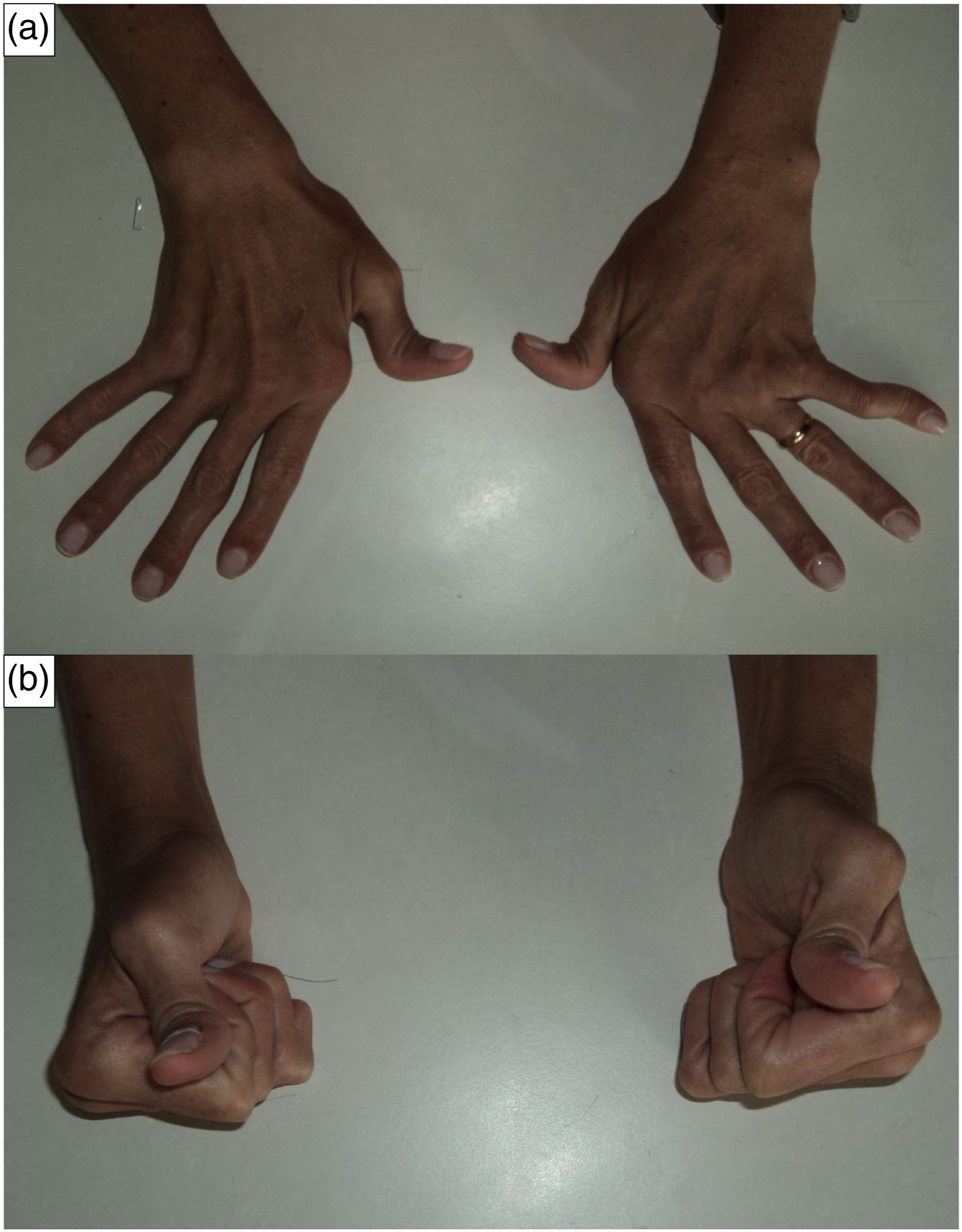
As RF has become increasingly rare, at least in developed countries, the number of cases of JA in this clinical scenario has been scarce. On the other hand, in the last few years, joint features similar to those seen in classical JA secondary to RF have been observed in patients with diffuse connective tissue diseases (DCTDs), particularly systemic lupus erythematosus (SLE).2–4 Other conditions for which JA has also been described in case reports are Sjögren’s syndrome, scleroderma, dermatomyositis, psoriatic arthritis, vasculitis, pyrophosphate deposition disease, gout and neoplasia 5 .
In this review, we report the epidemiology, pathogenesis, histopathology, clinical features, imaging and management of JA in patients with SLE (Jaccoud-type lupus arthropathy).
The search strategy included articles retrieved from PubMed utilizing the terms ‘lupus arthropathy’, ‘lupus deforming arthropathy’, ‘lupus hand’, ‘lupus foot’, ‘chronic postrheumatic arthropathy’, ‘Jaccoud’s’ and ‘Jaccoud’ from 1950 until March 2021. There was no language restriction. Secondary references were also searched.
Epidemiology
Cases series of jaccoud’s arthropathy in systemic lupus eryrhematosusa.
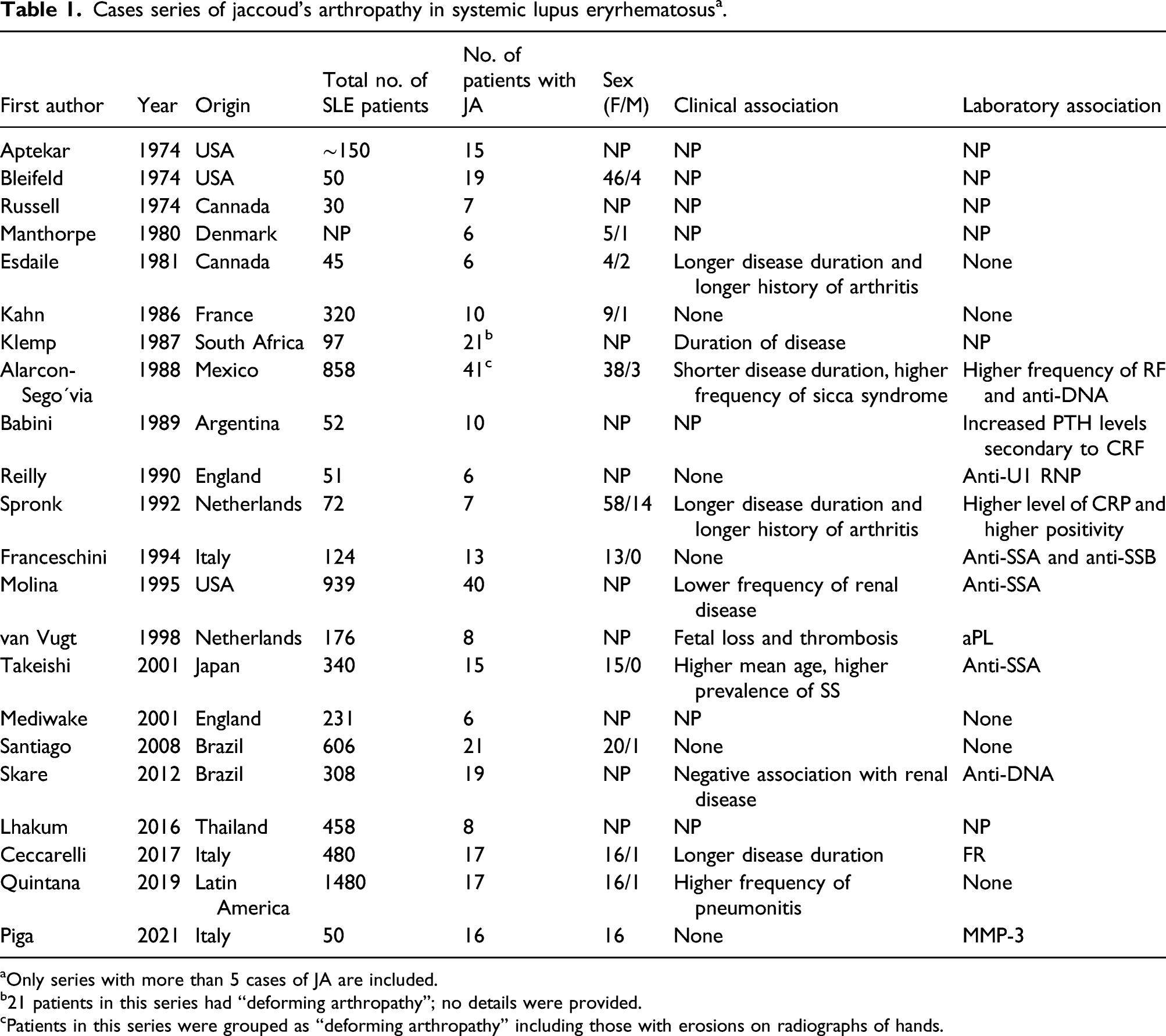
aOnly series with more than 5 cases of JA are included.
b21 patients in this series had ‘‘deforming arthropathy’’; no details were provided.
cPatients in this series were grouped as ‘‘deforming arthropathy’’ including those with erosions on radiographs of hands.
Proposed aetiopathogenic mechanisms for the development of JA
The deformities of JA are due to soft tissue abnormalities such as laxity of ligaments and joint capsule, distension and deviation of the tendon from its axis and muscular imbalance. While synovitis is mild, tenosynovitis leading to a loosened and weak tendon may have a stronger role. 5
The reason why only a minority of SLE cases develop such complications is not well understood. Some authors have suggested that JA is associated with disease duration; 9 however, it does not seem to be the case, as the majority of SLE populations of long duration do not have JA. Others have tried to associate JA with the presence of autoantibodies such as anti-SSA/Ro, anti-dsDNA, anti-RNP, antiphospholipid and rheumatoid factor2,10 and higher levels of C reactive protein in serum, 9 but such associations have not been confirmed in other studies. Similarly, conflicting results were observed when biomarkers for RA were tested in JA patients. Thus, we searched anti-CCP antibodies in a group of patients with SLE and found 12.5% positivity of these antibodies, and no difference was observed between cases with JA and controls. 11 Moreover, Damian-Abrego found a frequency of 7% anti-CCP in their series of SLE patients, and again, no association was found with JA. 12 Recently, Massaro et al. studied anti-carbamylated protein antibodies in SLE and found a higher frequency of such antibodies in lupus patients without deforming arthritis than in JA patients (48.8 versus 27.8%, p = 0.003). 13
Choi et al. studied 109 SLE patients, five of whom had ‘current evidence of deforming arthritis’, and found a statistically significant association between the presence of such arthritis and anti-collagen type II antibodies. 14 No other study addressing this issue has been published.
Generally, the idea of participation of any antibody in the development of JA seems to be weak since in RF with (or without) JA, no specific antibody has been claimed to have any role in its etiopathogenesis.
Another point of controversy is the association of JA with hypermobility, with divergent findings in the literature.
15
Indeed, although a few patients with heritable disorders of connective tissue can have hypermobile joints simulating JA, it is not true for the majority of such patients. Likewise, in well-defined JA, the presence of some degree of joint hypermobility secondary to a laxity of soft tissue elements is not rare (Figure 2). Genu recurvatum in a patient with long standing Jaccoud-type lupus arthropathy.
Babini et al. described 52 patients with SLE, and in 14 of them, JA and/or tendinous laxity were observed. They proposed that an increase in parathyroid hormone secondary to renal failure would be a cause for these joint abnormalities. 3 Although the effect of parathyroid hormone on the collagen of ligaments and tendons through an increase in bone collagenase activity has been well known, 16 there is no association between renal failure and JA in SLE patients.
In a study published by our group, patients diagnosed with SLE were divided into two groups, one with JA (n = 18) and a control group without JA (n = 62). Several interleukins (IL) and tumour necrosis factor α (TNF-α) were measured in serum, and it was observed that serum levels of TNF-α IL-2, IL-10, IL-21 and IL–22 were not significantly different between the two groups (p > 0.05), but the IL-6 level was higher in the JA group (p < 0.001). Although these preliminary results do not allow establishing a direct connection between IL-6 and the development of JA, they raise the idea that further studies are needed to explore the potential benefit of blocking IL-6 in this clinical complication. 17
Studies on the genetic aspects of JA are scarce. In a Japanese case series of 340 SLE patients, Takeishi et al. identified 15 individuals with JA. They genotyped HLA-A11 or B61 in nine patients, with positivity found in five individuals (55%), and this prevalence was higher than that in the Japanese population (A11, 17.4%, p < 0.05; B61, 17.5%, p < 0.057). 18
In a pilot study developed in our service, 144 individuals with SLE (38 with JA and 106 with SLE without JA) were included and genotyped for rs9271100, rs7574865, rs10488631 and rs13277113 polymorphisms in the HLA, STAT4, IRF5 and BLK genes, respectively, using real-time polymerase chain reaction. We found that the A allele of rs13277113 in the BLK gene was associated with the presence of JA in this sample of Brazilian SLE patients. BLK codes for a nonreceptor tyrosine–kinase which is involved in the signalling, development, and differentiation of B lymphocytes. Altered levels of BLK protein may influence the tolerance mechanisms of B lymphocytes. These findings can raise questions on the role of B cells and their performance in the pathogenesis of JA. 19
Histopathology of JA
There are only a few reports on the histopathologic findings seen in JA. Synovitis is present but in general not as intense as that in RA. There is fibrin deposition, haematoxylin corpuscles and inflammatory cellular infiltrate without pannus. In one of the autopsy cases of JA secondary to RF cited by Bywaters, the pathology of the joints was described as follow: ‘Sections of synovial membrane therefrom showed a few lymphocyte collections, a few plasma cells and pigment-containing macrophages consistent with a relatively inactive and healed inflammatory lesion’. ‘There was no pannus formation. Active inflammatory synovitis was absent, although a few round cells and plasma cells were visible’. 20 Periarticular fibrosis and normal synovium were the only findings in a surgical specimen of the metacarpophalangeal joint from one patient with RF and deforming arthropathy described by Twigg and Smith. 21
Russell et al. reported seven SLE patients with ‘progressively deforming arthritis’ in the hands. Joint surgery was performed in four patients. The articular cartilage was macroscopically normal, and the observed histopathological findings were ‘little inflammation in [the] synovial membrane’ and ‘synovial hyperplasia with mild mononuclear cell infiltration’. 22
Girgis et al. reported a necropsy analysis of three joints of a female patient with JA secondary to RF. They found only fibrous thickening of the joint capsule and no evidence of significant synovial pathology. 23
Schumacher et al. reported the histopathological findings of a tissue sample obtained in corrective surgery of the hand in a 33 year-old woman with SLE and JA. They observed ‘mild lining cell proliferation, many fibrotic villi, areas of haematoxyphilic degeneration in (the) villi and capsule and infiltration with clumps of lymphocytes and plasma cells in (the) synovium and capsule’. 24
Cruickshank performed an autopsy study on 14 joints and seven tendon sheaths from 10 SLE patients, one of whom had apparent JA. The researchers found the presence of a thick layer of fibrin-like material on or under the surface in synovial tissue, haematoxylin bodies among the synovial cell nuclei, a slight-to-moderate infiltrate with lymphocytes and plasma cells, and damage of articular cartilage in five of six finger joints (in three of these, there were marginal erosions). In six of seven investigated patients, inflammation was more marked in the tendon sheath than in the joints. Unfortunately, there were no specific details on the only patient with JA. 25
Diagnostic criteria
There are no definite classification criteria for JA. Initially, Bywaters 20 described features that might differentiate the chronic arthropathy seen in RF from RA: a) history of acute rheumatic fever attacks; b) delayed recovery and gradual development of join deformity; c) deformity due to periarticular and fascial fibrosis rather than synovitis; d) the deformity consists of flexion and ulnar deviation at the metacarpophalangeal and hyperextension at the proximal interphalangeal joints. This deviation is correctable by voluntary effort in the early stage; e) tendon crepitus may be elicited; f) the disease is relatively inactive, with a normal sedimentation rate and often little or no complaints regarding the joints; and g) radiologically, hook-like erosion is present.
In 1973, Murphy and Staple suggested criteria for JA secondary to RF quite similar to those items proposed by Bywaters adding features in ‘historical’, ‘clinical’, ‘roentgenologic’ and ‘laboratory’ subitems. 26
Alarcon-Segovia et al. classified deforming arthropathy in SLE as any deviation of the metacarpal finger axes. In this case, patients with ‘rhupus’ might be misclassified as having JA, and patients with JA without ulnar deviation but with other joint deformities might be excluded. 27
In 1992, Spronk et al. developed a diagnostic ‘index’ to define the presence of JA in SLE patients, taking into consideration the presence of different deformities. A score higher than five points suggests JA. 9
In 1998, Van Vugt et al. merged the features of the Alarcon-Segovia et al. and Spronk et al. criteria and proposed three different forms of deforming arthropathy in SLE patients named ‘erosive (rhupus hand)’, ‘JA’ and ‘mild non-erosive arthropathy’. 28 The weakness of these criteria resides in the difficulty in separating the last two subgroups.
We have previously proposed a set of criteria for JA, specifically for SLE, 29 which includes the presence or history of articular inflammation and the absence of similar deformities in other healthy members of the same family. These are to avoid overdiagnosis of JA. One of our inclusion criteria was the absence of erosion on plain radiographs, but it did not mean that this finding does not exist when magnetic resonance imaging (MRI) or high-performance ultrasound (US) examination is utilized, as we have previously demonstrated. 30 In those original criteria, we had stated that the deformities should be correctable in a passive position. However, the spectrum of deformity in JA is very wide, varying from a simple ‘reducible’ ulnar deviation to a more complicated ‘severe’ or ‘mutilans-type’ deformity with fixed joints and subluxations. 6 Thus, a modified set of criteria for JA in SLE contemplating ‘severe’ forms of the disease has been recently published. 31
The importance of having classification criteria for JA lies in two points: a) standardize patients for future clinical trials; b) distinguish SLE cases with JA from those with RA, as the therapeutic approach is different. Unfortunately, none of the proposed criteria has been validated so far to reach these aims.
Clinical features
As mentioned above, the most common joint deformities of JA are seen in the hands, such as the ulnar deviation, the swan neck and the ‘z’ of the thumb, although other joints may be involved, such as the knees, shoulders and joints of the feet. 32 The clinical characteristic that classically differentiates JA from RA deformities is its ‘reversibility’, that is, the joints return to their normal position for passive movement. However, the term ‘reversible’ to designate JA, although widely used in the literature, seems inappropriate because once this complication is installed, the joint no longer returns to normal. Hence, it seems more appropriate to use the expression ‘reducible’ by passive movement. However, JA patients may have a ‘severe’ form of the disease when the deformities are not reducible. This is probably secondary to soft tissue fibrosis, disuse of the involved joints and muscle hypotrophy. 6 Curiously, based on Bywaters’ report in 1950, the original patient described by Jaccoud was probably an example of the severe form of this arthropathy in whom ‘deformity of the hands developed for the first time in the third month of the fifth attack and was initially correctable, only later becoming permanent’. 20 Other authors have confirmed the changing character of the deformities from reducible to fixed. 33
There is no direct relationship between the presence of clinically apparent joint inflammation and the degree of deformity of JA. Some patients may have arthropathy without much pain or may even be pain-free. These findings reinforce the idea that the main reason for the deformities is alterations of soft tissues such as the tendon sheath and capsule rather than synovitis. This has also been well described in RF. Notably, diffuse periarticular swelling of the hands is another finding rarely described in JA. 5
There is controversy in the literature regarding whether hand dominance has an influence on the frequency of musculoskeletal disorders, such as rotator cuff disorders, bicipital tendinitis, epicondylitis, and carpal tunnel syndrome, as well as on the degree of deformity in patients with RA. In a pilot study of 22 patients with SLE and JA, it was demonstrated that hand dominance does not seem to influence the degree of JA deformities. 34
The relationship between heart and joint diseases has been explored since the 18th century. Bywaters, in his publication in 1950, commented on the historical background of this relationship as follows: ‘In 1788, David Pitcairn, in his lectures to the students of St Bartholomew’s drew attention to the frequent occurrence of heart disease in patients who had been affected with rheumatism’. Bywaters comprehensively reported the association between JA and valvular heart disease in patients with RF. 20 Other examples of this relationship are the rare cases of JA in patients with primary hypocomplementaemic urticarial vasculitis and nonrheumatic valvular disease, probably mediated by immune complexes. 35 This syndrome resembles lupus arthropathy. To further explore this association, 113 SLE patients (25 with JA and 88 without JA) were assessed by transthoracic echocardiography, and valvulopathy was found in nine cases of JA (36%) against eight cases (9%) in the control group (p = 0.001). This study demonstrated for the first time the connection between JA and valvulopathy in SLE patients. 36
Other studies have demonstrated a positive association between JA in SLE and antiphospholipid syndrome 28 and Sjogren’s syndrome 18 and, conversely, a negative association with nephritis. 37 Further studies are necessary to confirm these findings.
Although clinical tenosynovitis is not frequently described in patients with JA, utilizing new imaging modalities, this condition has been more recognized recently in patients with or without symptomatic SLE, with or without JA (see below). In theory, tenosynovitis in JA may loosen the tendon or even weaken it, predisposing it to ruptures. A review of spontaneous tendon rupture in SLE patients identified 55 published cases. One-third of these patients had JA, suggesting a direct relationship between these two entities. 38
Differential diagnosis
The main issue in hand deformities such as the ulnar deviation and ‘swan neck’ types is to differentiate RA from JA. However, other conditions may also present abnormalities in the hand that may resemble these conditions. Thus, there are a few individuals who have hand deformities without any history of joint inflammation or systemic comorbidity. These cases are called ‘primary’ or ‘idiopathic’ JA. 39 Rarely more than one member of the same family has similar deformities but does not fulfil the criteria for heritable disorders of connective tissue, being labelled ‘familial JA’. 40 Moreover, hand deformities, particularly ulnar deviation without structural disease, have been described in elderly people, and these cases are designated ‘senescence JA’. 41
Parkinson’s disease, due to muscle contractures and tendinous retraction, does not rarely lead to hand deformities typical of JA. 42 Swan neck type deformity may be seen in Ehlers-Danlos syndrome or Marfan’s syndrome due to ligamentous laxity. Bilateral reducible boutonniere deformities have been described in an unprecedented case of Wilson’s disease in a 14 year-old male. After 6 months of d-penicillamine therapy, there was a significant improvement in his hand deformities. 43
Imaging
By definition, plain radiograph of joints in JA has no bone erosions (Figure 3). ‘Hook-like erosions’ is a classical radiographic feature of JA secondary to RF referring to a bone alteration observed on the palmar-radial surface of the metacarpal heads.
20
The term ‘erosion’ seems to be inappropriate, as the bone abnormality resembles an osteophyte in the form of a hook. Moreover, such erosions are not pathognomonic for JA, as they have also been described in RA, gout, pseudogout and osteoarthritis. In our experience, no SLE patient has shown this radiographic finding in metacarpal bone but a patient had a ‘hook osteophyte’ in the distal phalanx (Figure 4). Plain radiograph of the left hand showing joint deformities but no bone erosion. Plain radiograph of right hand. Note subluxation of the thumb with a ‘hook osteophyte’ in the distal phalanx.

Another interesting but uncommon finding on plain radiograph of JA is a carpal ‘collapse’ without erosions, simulating even more RA, probably secondary to weakness of soft tissue carpal structures
28
(Figure 5). Plain radiograph of left hand showing periarticular osteoporosis, joint subluxations and “collapsed” wrist without bone erosion in Jaccoud-type Lupus Arthropathy.
More sensitive imaging methods, such as MRI and US, may reveal small bone erosions. In a study carried out in our service, 20 patients with SLE and JA (19 women and one man) were studied by MRI of the hand, and a total of 300 joints were evaluated. In that study, some degree of synovitis was observed in 67.3%, tenosynovitis in 38.5% and in 16 of the joints analysed (5.3%), small areas of erosion were seen. 44 Likewise, in another study utilizing US, 40 patients with SLE and JA were included, and US examination was performed on 560 joints of the hands and wrists. Nineteen patients (47.5%) had synovial hypertrophy, nine (22.5%) had tenosynovitis, and seven (17.5%) had both. Small isolated bone erosions were identified in two patients (5.0%). 30
Treatment
At present, there is no specific treatment for SLE patients with already existing joint deformities. The therapeutic approach is similar to that for nondeforming active arthritis, including nonhormonal anti-inflammatory medications and low doses of corticosteroids, methotrexate, leflunomide and antimalarial drugs, aiming to control articular inflammation.
The use of orthoses and physical therapy has not shown satisfactory results, at least in our experience. Unlike what happens in RA, there has been very little experience in performing surgeries, either through the realignment of tendons or the placement of prostheses aiming to correct JA deformities. In the few cases we followed, the surgical results were frustrating. In a recently published systematic review of surgery in JA, only seven articles met the inclusion criteria previously established by the authors, and a total of 58 patients underwent surgical procedures for JA. Such studies were limited to a small series of cases, there was no uniform definition of the outcome, and the follow-up time varied widely. It was concluded that there is no consensus on the best surgical approach in patients with JA, who are the best candidates and when to recommend the procedure. 45
Of note, we have treated two patients with a severe form of JA refractory to conventional therapy with anti-TNF therapy (etanercept), despite its potential for inducing an immunological phenomenon. The rationale for this approach was a demonstrated long-term efficacy and safety of etanercept in 43 patients with refractory lupus arthritis. 46 These two patients had an improvement in their intensity of joint pain as well as in quality of life in general.
In theory, other biological molecules candidates for the management of JA would be rituximab, for its proven efficacy in RA and its safety during its off-label utilization in some other complications of SLE, and tocilizumab, because of the above-demonstrated evidence of higher levels of IL-6 in this subset of SLE patients.
In the future, the more optimistic scenario for the management of JA will be the identification of patients with potential for the development of this complication, through genetic markers or cytokine profiles, as well as early intervention in a more aggressive manner before the development of deformities.
Footnotes
Acknowledgments
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.