
Abstract
Background
Salivary gland ultrasound (SGUS) is a reliable technique for assessing the salivary glands in patients with primary Sjögren’s syndrome (SS); however, the role of SGUS for diagnosis of secondary SS (sSS) in patients with systemic lupus erythematosus (SLE) was not examined.
Objective
To assess the diagnostic value of SGUS for sSS in patients with SLE, and to investigate the relationship between SGUS findings with clinical and laboratory characteristics of patients with SLE.
Patients and methods
This cross-sectional study included 49 patients with SLE. The diagnosis of sSS was confirmed according to the 2016 ACR/EULAR criteria. Salivary gland US was performed for all patients and graded using a validated Hočevar scoring system. A complete clinical and laboratory workup for SLE was assessed. Schirmer’s test and the ocular staining were performed.
Results
Of the 49 patients with a mean age of 30.2 ± 9.6 years, 98% were female. 19 (38.8%) had sSS. SGUS changes consistent with sSS (≥17) were found in 29 (59.2%) of the patients. Patients with higher SGUS score had more sicca findings as well as positive anti-Ro, anti-La antibodies, and poorer psychological stress (p < 0.05). The SGUS (≥17) showed a sensitivity of 84.2% and a specificity of 56.7% for sSS diagnosis, with an area under the curve of 0.77 (95% CI: 0.63, 0.91).
Conclusion
We propose salivary gland ultrasound as a non-invasive method in the diagnostic workup for sSS in patients with SLE. Further studies to confirm the diagnostic value of SGUS in a larger sample of patients with sSS will be necessary.
Introduction
Systemic Lupus Erythematosus (SLE) is a complex autoimmune disease characterized by the presence of various autoantibodies and clinical manifestations affecting multiple organ systems. 1 Patients with SLE have an increased risk for the development of other autoimmune diseases such as Sjögren’s syndrome (SS). Sjӧgren’s syndrome can be present in either primary (pSS) or secondary forms. Secondary (sSS) occurs in association with other autoimmune diseases such as rheumatoid arthritis (RA), SLE, and scleroderma (SSc).2–4 The reported prevalence of sSS in adults with SLE has varied from 9% to 33%3, 5–7; with variation probably related to patient populations, diagnostic criteria, and testing used.
Sjögren’s syndrome is a chronic autoimmune disease ofthe lacrimal and salivary glands leading to keratoconjunctivitis sicca and xerostomia, along with other non-specific symptoms such as fatigue and musculoskeletal pain, and can lead to lymphoma. 8 The pathogenesis of SS is mostly autoimmune focal glandular lymphocytic infiltration that suggest a local immune response with an aberrant B-cell activity that correlate with the systemic manifestations of SS. 9
Many classification systems have been developed to define SS and assist in research and clinical practice.10,11 The 2016 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria for SS is the most recent one. 11 In fact, these criteria depend on several diagnostic tests as minor salivary gland biopsy, sialography, salivary flow, and scintigraphy in the classification. These techniques are somewhat considered to be painful, invasive, and expensive which make these procedures cumbersome for patients and physicians.
Nowadays, there is increasing interest for a safe and quick tool to identify salivary gland abnormalities. Ultrasound provides a non-invasive, non-ionizing imaging technique that can be performed readily at the bedside and is particularly well-suited to clinical practice. 12 Salivary gland US (SGUS) has been suggested to increase the performance of the ACR criteria.12,13 Several studies demonstrated good correlation of SGUS with other imaging modalities for diagnosing SS, 14 autoantibodies and dry mouth and eye symptoms, and minor pathological changes in the salivary gland.15–17 While many studies have focused on primary SS, limited studies examined the role of SGUS in patients with secondary SS. 18 The aims of this study were to 1) evaluate the performance of SGUS for the diagnosis of sSS in patients with SLE, and 2) identify the relationship between SGUS findings with clinical and laboratory findings in patients with SLE.
Patients and methods
Study design and study population
This cross-sectional study was carried out at the Rheumatology Department, Rheumatology and Clinical Immunology unit, Internal Medicine department, Assiut University Hospitals, Assiut, Egypt. Forty-nine patients aged ≥18 years who fulfilled the 2012 Systemic Lupus International Collaborative Clinics (SLICC) classification criteria were enrolled. 19 Exclusion criteria included head and neck malignancies and previous irradiation. The study was in accordance to the 1995 Helsinki declaration and approved by the ethical committee of Faculty of Medicine Ethics Research Office. Informed consent was obtained from all patients prior to their participation in the study.
Sociodemographic, clinical and laboratory assessments
The sociodemographic data, disease characteristics, and current medications use of all SLE patients at the time of the visit were collected. Disease activity and damage level of the patients were assessed using Systemic Lupus Erythematosus Disease Activity Index (SLEDAI), 20 and Systemic Lupus International Collaborative Clinics/American College of Rheumatology Damage Index (SLICC/ACR-DI) 21 , respectively. Symptoms of dry eye and mouth were assessed based on classification criteria questionnaire for more than 3 months. 10 SLE patients with secondary SS were determined according to the 2016 ACR/EULAR. 11 Functional status was assessed with a self-report multidimensional Health Assessment Questionnaire (MDHAQ).22,23 MDHAQ includes 10 activities of daily living, four items to assess psychological distress, duration of morning stiffness as well as visual analogue scales for pain, global status, and fatigue, review of the systems, falls and cardiovascular risk assessment, the rheumatology attitudes index and self-report of joint counts.
Specific laboratory investigations were examined. Laboratory characteristics of interest included the erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), complete blood cell count (CBC), serum creatinine, and urine analysis Complement (C3) and C4 and relevant autoantibodies including anti-double stranded DNA (anti-dsDNA), rheumatoid factor (RF), anti-Ro, and anti-La were measured by enzyme-linked immunosorbent assay (ELISA).
Ophthalmologic examinations
Tear function tests were performed by an expert ophthalmologist who was blind to the clinical diagnosis of patients. Tear function tests consisted of tear film break-uptime (TBUT), Rose-Bengal score, and the Schirmer test were performed for all patients. For TBUT, a strip of moistened fluorescein paper was used to touch the inferior fornix for a short time with minimal stimulation. The tear film was observed under cobalt blue–filtered light. The interval (seconds) between the last complete blink and the first emergence of randomly distributed dry spots was averaged. This was followed by staining with 1% Rose-Bengal solution. Both fluorescein and Rose-Bengal staining scores were recorded and ranged between 0 and 9 points. Schirmer test was performed using standardized strips of filter paper which were placed in the lateral canthus away from the cornea and left in place for 5 min with the eyes closed. Schirmer test was recorded in millimeters of wetting for 5 min (mm/5 min). The Schirmer test result ≤5 mm/5 min and/or a positive score Rose-Bengal ≥4 was considered positive objective ocular dryness.
Salivary gland ultrasonography features
Each patient underwent a one-time major SGUS assessment using a real-time, high-resolution ultrasound machine (General Electric Logiq S8) with an 8–15 MHz linear transducer. Ultrasound examination included static B-mode images. Parotid and submandibular glands on both sides were scanned in longitudinal and transverse planes. The parotid and submandibular glands were assigned based on the validated Hočevar score (maximum score of 48).24,25 Briefly, 5 variables were quantitatively assessed for each gland: parenchymal echogenicity relative to the thyroid gland, homogeneity, presence of hypoechoic areas, presence of hyperechoic foci, and glandular borders. The parenchymal echogenicity of bilateral parotid and submandibular glands was graded either 0 (isoechogenic) to the thyroid gland or 1 if decreased. The parenchymal homogeneity was graded from 0 (homogeneity) to 3 (gross inhomogeneity). Hypoechoic areas were graded from 0 (absent), 1 (few), 2 (several), and 3 (numerous). Presence of hyperechoic foci in parotid glands were graded from 0 (absent) up to 3 (numerous), and either 0 (absent) or 1 (present) for submandibular glands. Visibility of glandular borders of both parotid and submandibular glands were graded from 0 (well defined borders), 1 (slightly less defined borders), 2 (ill-defined borders), and grade 3 (not visible borders (Figure 1). On the whole, total SGUS scores of ≥17 were reported as having US changes consistent with SS, and patients were classified into two groups according to this cutoff score.24,25 Images of the salivary glands were obtained by a radiologist who had 10 years’ experience in the field of ultrasound and who was blind to the clinical information of the patients.
Statistical analysis
Standard descriptive statistics were used for demographic and SLE characteristics. The data were presented as mean (standard deviation, SD) or median (interquartile range, IQR) for continuous variables and number (percentage) for categorical variables. We categorized the participants into two groups according to the SGUS score and compared the clinical and serologic features using Student’s t-test for continuous variables and chi-square test for categorical variables, as appropriate. Receiver operating characteristic (ROC) curves were drawn to compare the ability of different US score to distinguish patients with sSS from those without. The Sjogren syndrome criteria were compared with SGUS using the area under the ROC curve (AUC), sensitivity, and specificity. P values less than 0.05 were considered statistically significant. All statistical analyses were performed using STATA 16 software.
Results
Characteristics of the study population
A total of 49 SLE patients were enrolled, 98% were female, with a mean age of 30.2±9.6 years. 19 (38.8%) patients were first-time diagnosed with sSS according to ACR/EULAR classification criteria. The characteristics of patients with SLE-sSS and SLE-only are shown in Supplementary Tables 1 and 2.
Comparison of demographic and clinical characteristics between those with and without salivary gland ultrasound (SGUS) changes among patients with SLE.
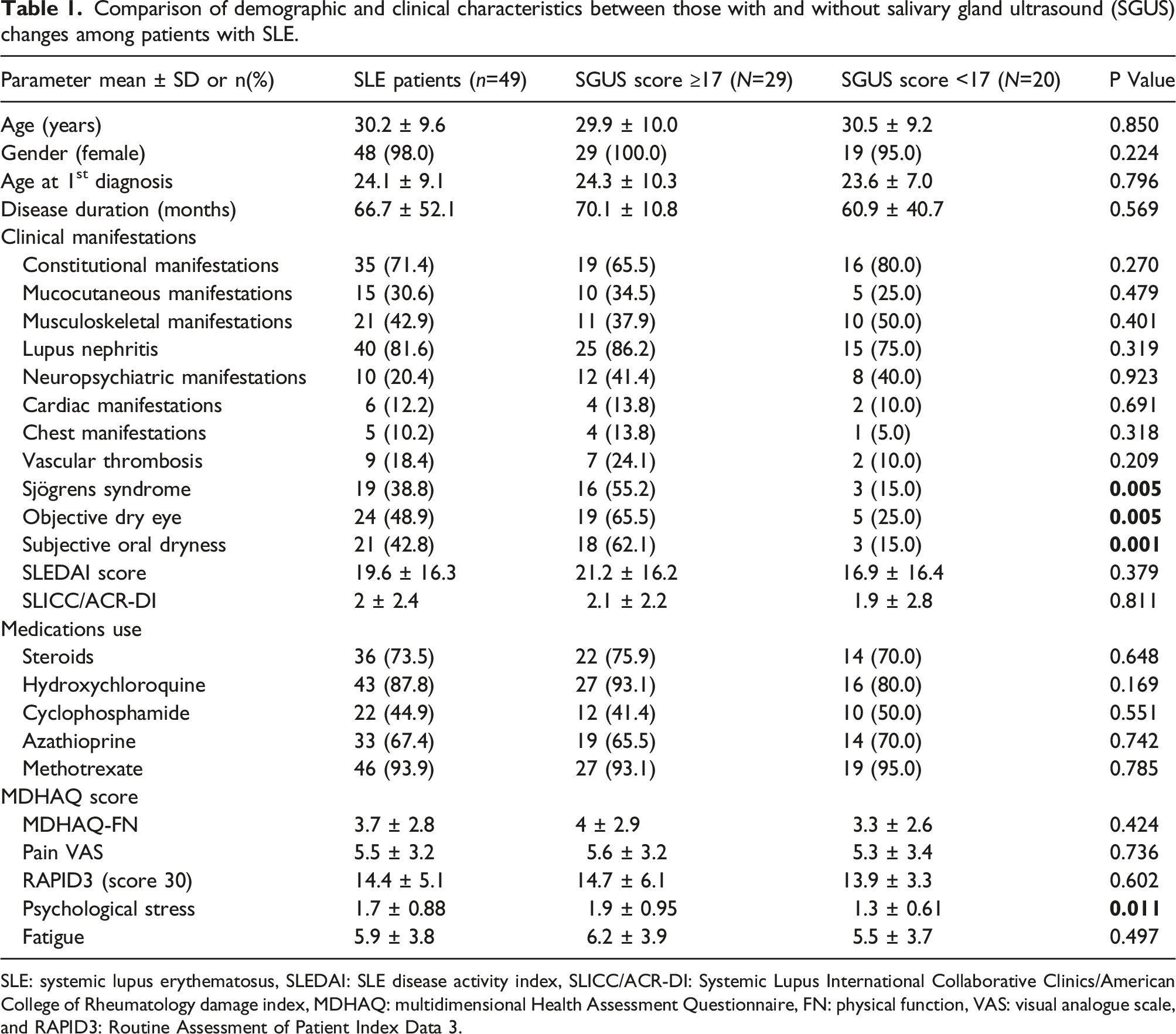
SLE: systemic lupus erythematosus, SLEDAI: SLE disease activity index, SLICC/ACR-DI: Systemic Lupus International Collaborative Clinics/American College of Rheumatology damage index, MDHAQ: multidimensional Health Assessment Questionnaire, FN: physical function, VAS: visual analogue scale, and RAPID3: Routine Assessment of Patient Index Data 3.
Comparison of laboratory characteristics between those with and without salivary gland ultrasound (SGUS) changes among patients with SLE.
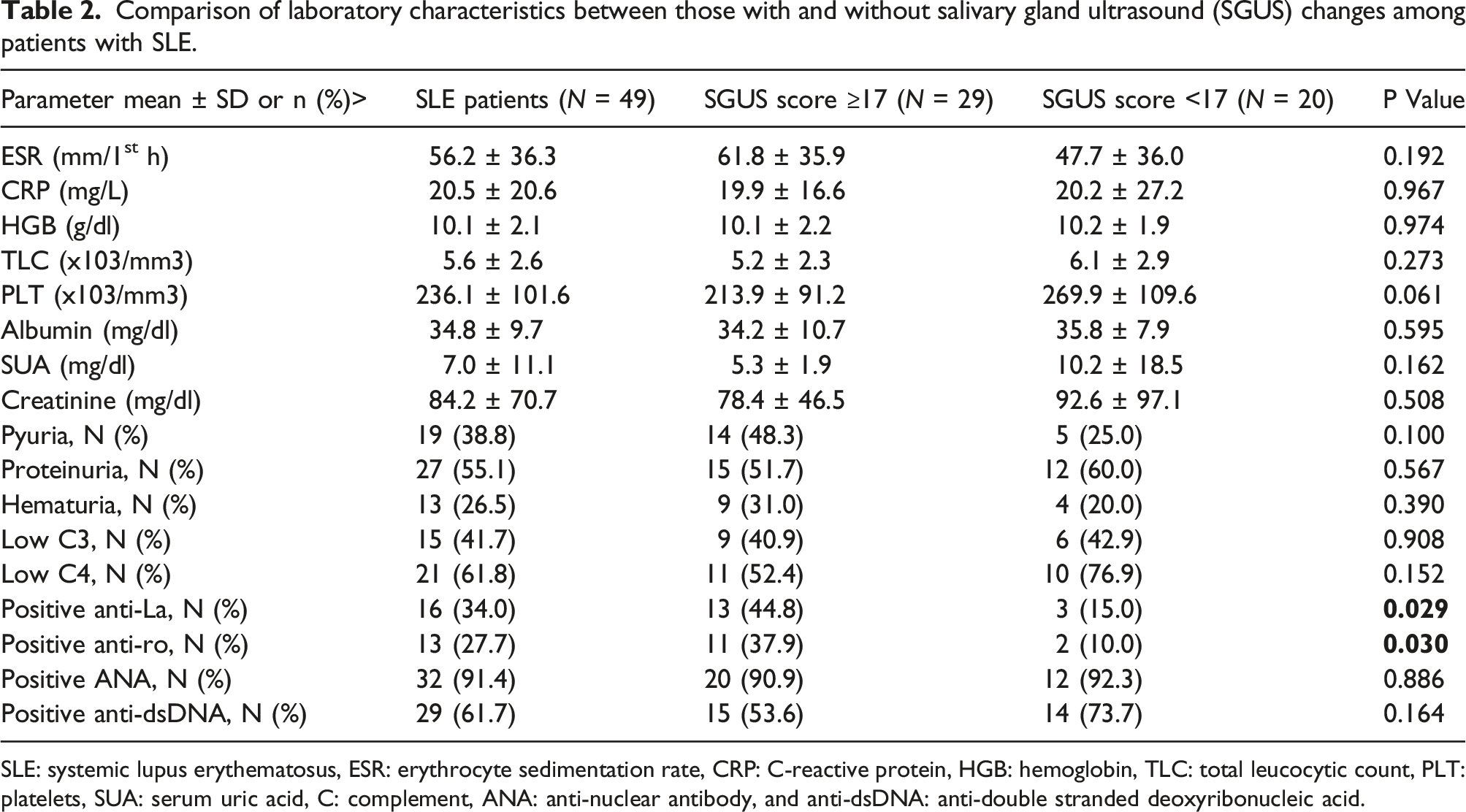
SLE: systemic lupus erythematosus, ESR: erythrocyte sedimentation rate, CRP: C-reactive protein, HGB: hemoglobin, TLC: total leucocytic count, PLT: platelets, SUA: serum uric acid, C: complement, ANA: anti-nuclear antibody, and anti-dsDNA: anti-double stranded deoxyribonucleic acid.
SGUS+ patients reported higher mean psychological stress scores than SGUS− patients (1.9 ± 0.95 vs 1.3 ± 0.61; p = 0.011). There were no differences in mean fatigue or pain scores reported on the questionnaire between SGUS+ and SGUS− patients (Table 1).
Most patients in both groups were on some form of systemic treatment with a majority being on methotrexate and/or hydroxychloroquine and/or azathioprine. There were no differences in medication regimen between SGUS+ and SGUS− patients, including the steroids use, Table 1. Overall, none of the study participants were using anticholinergics or antidepressants.
Among those with SGUS scores ≥17, there was a slightly higher SLEDAI (21.2 ± 16.2 vs 16.9 ± 16.4, p = 0.379) and SLICC/DI (2.1 ± 2.2 vs 1.9 ± 2.8, p = 0.811) compared to patients with scores <17; however, this was not statistically significant. Erythrocyte sedimentation rate and C-reactive protein, positive anti-dsDNA, low C3 and C4 were not significantly different between those with and without substantial ultrasonographic changes, Table 2.
Frequency of salivary gland ultrasonography findings according the SS diagnosis in patients with SLE.
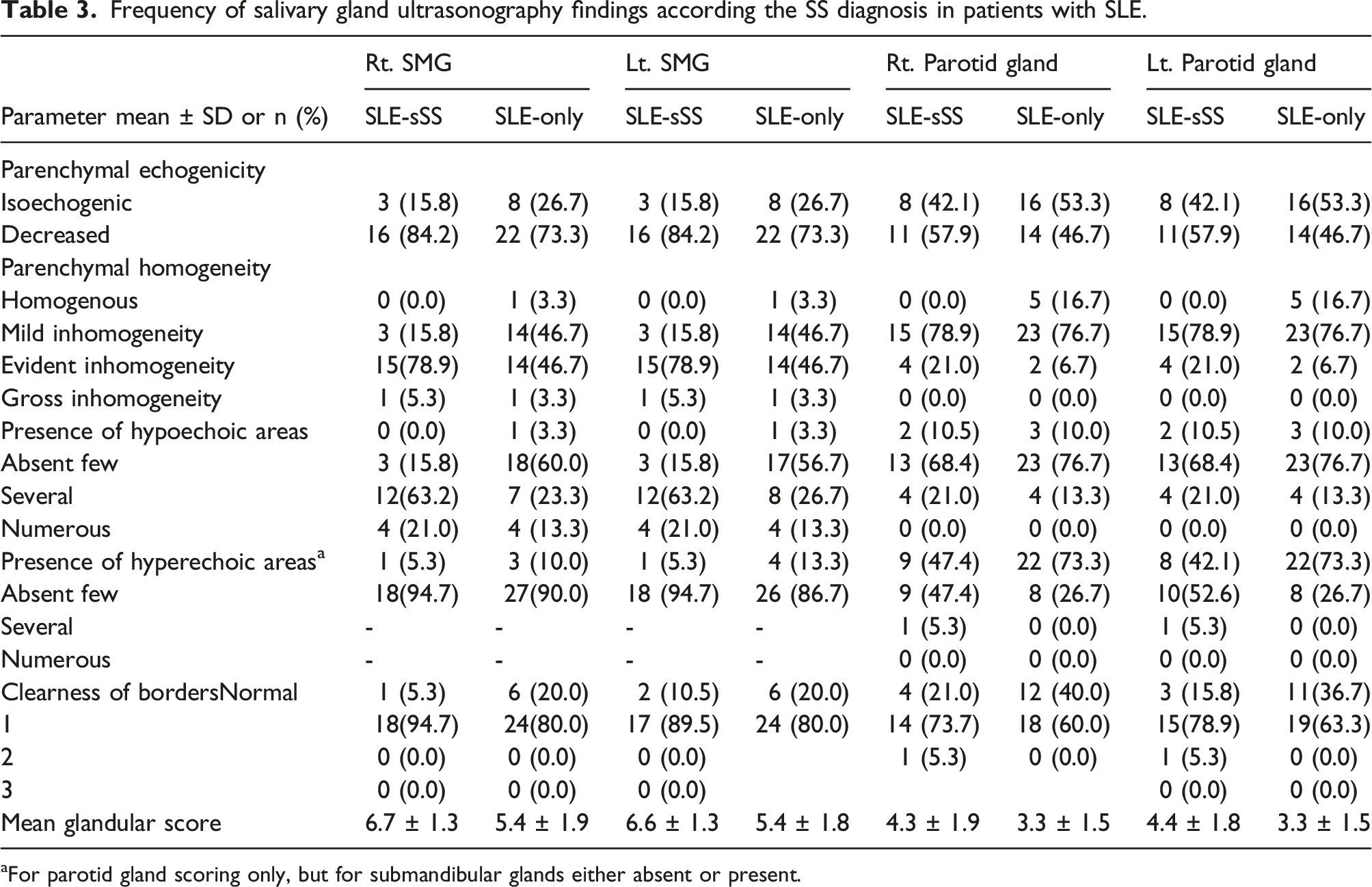
aFor parotid gland scoring only, but for submandibular glands either absent or present.
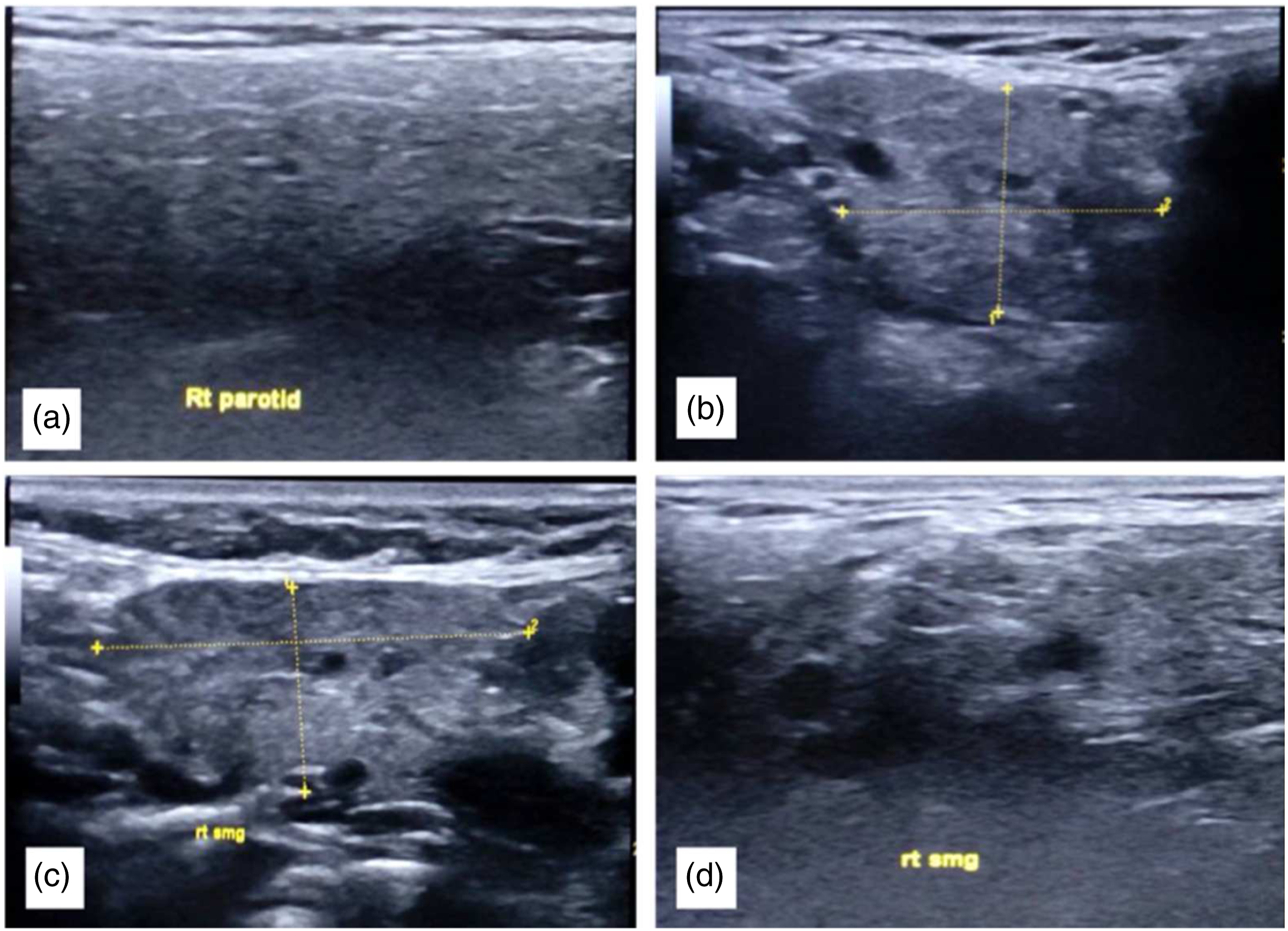
Ultrasound images of parotid and submandibular glands in systemic lupus patients. Major salivary gland ultrasonography images of parotid and submandibular glands according to Hočevar scoring systems illustrating: (A) Example of decreased echogenicity in parotid gland in comparison with thyroid gland (Score 1), (B) Inhomogeneity and hypoechoic areas in a submandibular gland in sSS (score 2), (C) Presence of hyperechogenic reflections submandibular gland (Score 1), (D) Example for ill-defined borders in sSS (Score 2).
SGUS as a tool to diagnosis sSS in SLE patients
The SGUS (cutoff score of 17) showed a sensitivity of 84.21% and a specificity of 56.67% for SS diagnosis with area under the curve (AUC) of 0.77 (95% CI: 0.634, 0.915) (Figure 2). ROC curve analysis for the performance of the SGUS‐Hočevar score system in discriminating between SLE patients with secondary SS and non-secondary SS.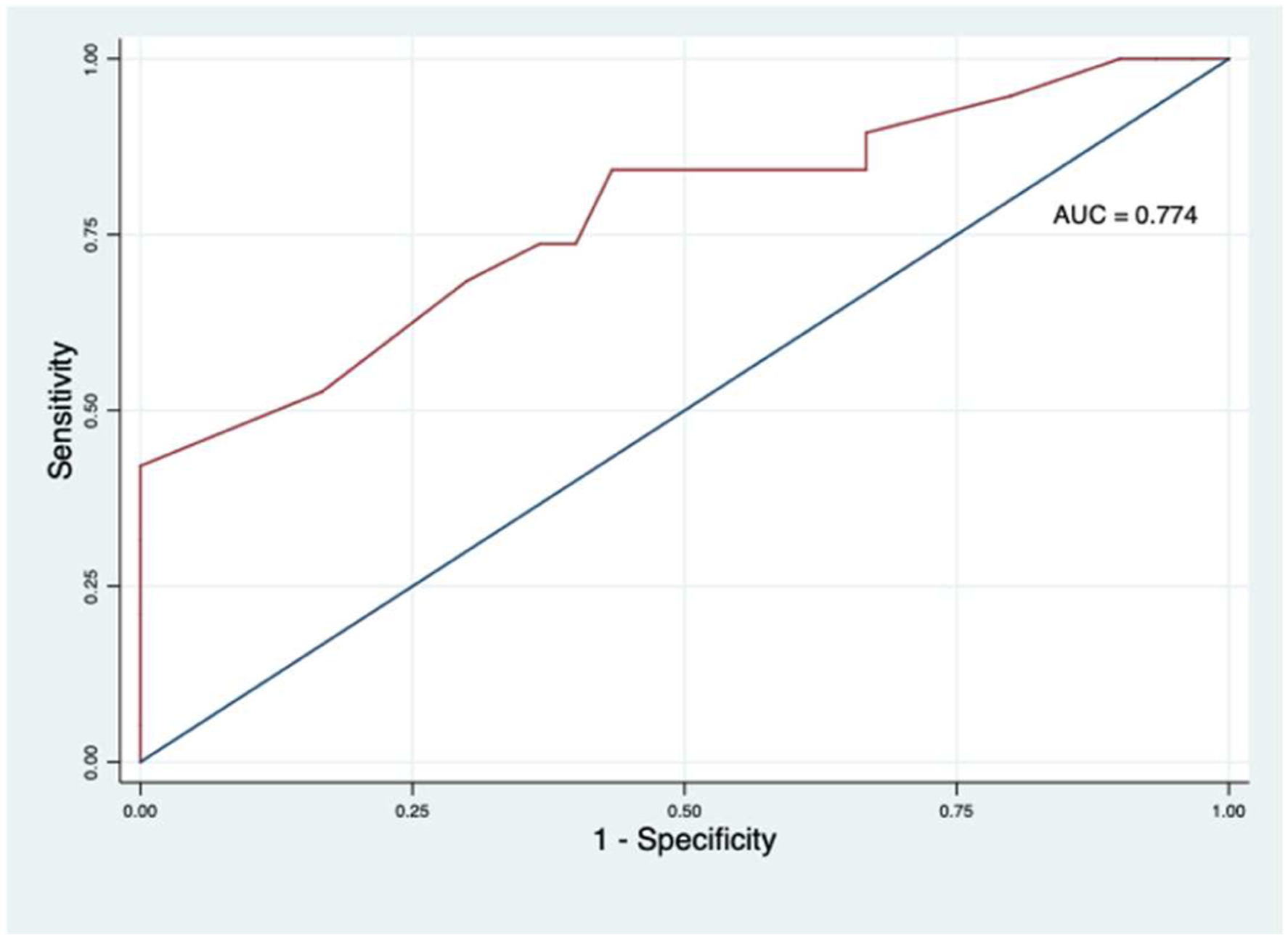
Discussion
Sjögren’s syndrome either primary or secondary leads to structural changes in the salivary glands, which can be detected with salivary glands ultrasound. While several studies have assessed SGUS for the diagnosis of pSS,12,24,25 limited data are available for the role of SGUS in secondary SS. Our goal was to assess the utility of SGUS in diagnosing sSS among patients with SLE. We found that 59.2% of patients with SLE, who do not have a formal diagnosis of SS, had sonographic salivary gland changes consistent with SS (SGUS scores ≥17). Our findings support the high sensitivity (84.2%) of the SGUS with low specificity (56.7%) for the identification of sSS. This study provides a window into the use of SGUS as an additional tool in the identification of particular clinical and immunological profile consistent with Sjogren syndrome.
Previous studies have reported prevalence of sSS in SLE ranging from 9% to 33% using the diagnostic criteria.3,5–7 In our study, using a sonographic scoring system, we found a prevalence of 59%. The rate of pathologic SGUS findings was higher than initially suspected. McDonald et al. found that 35% of childhood onset SLE patients (mean age 18.5 ± 2.6) had pathologic SGUS scores. 26 A recent study in adults evaluating SGUS in patients with SLE, mixed connective tissue disease, and undifferentiated connective tissue disease (with the majority of patients having SLE) found pathologic SGUS findings in 27% of patients. 27 The imaging findings may represent subclinical disease that could manifest itself with more overt clinical symptoms as time goes on. Destruction of lacrimal and salivary gland may precede the development of inflammation and the clinical symptoms of SS. 28
We evaluated the diagnostic accuracy of SGUS as a tool for detection of SS in patients with SLE. At a cut-off of 17, the AUC was 0.77 (95% CI: 0.634, 0.915), high sensitivity of 84.21%, but with low specificity of 56.67%. De Vita, et al. found that SGUS less sensitive in sSS (53.8% against asymptomatic controls; 46.2% against symptomatic controls) compared to pSS (sensitivity 81.5%). 27 Their scoring system assessed only one variable (gland homogeneity) and validated the diagnosis using older SS criteria. We performed SGUS using a scoring system described by Hočevar using five description components for gland echo structure24,25 had high accuracy 29 and diagnostic value even compared to scintigraphy. 30 Consistent with these observations, Lesturgie-Talarek et al. 31 showed that SGUS features of SS were observed in one quarter of CTD patients without SS. These data suggest that pathological SGUS features had low specificity for SS or could be observed in a preclinical stage of SS. Thus, SGUS changes might be associated with a particular clinical and immunologic profiles.
The diagnosis of SS is complex and there is no single diagnostic test with satisfactory validity. Many different classification criteria have been used for the diagnosis. The ACR/EULAR classification includes 3 objective measures; however, the salivary gland biopsy included in the ACR/EULAR classification is invasive and physicians may hesitate to use this method when screening for SS. Ultrasonography of the major salivary glands represents an informative imaging procedure for detection of parenchymal abnormalities in SS. It is non-invasive, inexpensive, and does not involve radiation. 12 The ultrasound assessment in our study was performed at the bedside during a regularly scheduled clinic visit. Cornec, et al. suggested that salivary gland US might be used initially to avoid salivary gland biopsy, and may further improve sensitivity.12,13
In this study, we found that SGUS positive patients have a distinct clinical phenotype in comparison with SGUS negative patients. Sonographic changes consistent with sSS were significantly higher in patients with sicca symptoms (oral and ocular dryness). Similar to our findings, McDonald et al. 26 observed that abnormal SGUS seemed to correlate with abnormal tear production and oral dryness. 27 This is an important practical observation because those with SS are known to be more prone to dental caries, oral candidiasis, and periodontal disease. 32 Thus, sonographic diagnosis of sSS in patients with SLE may potentially help to identify the patients who need routine consultation and management of their oral health.
Subjects with SLE and SGUS changes consistent with sSS tended to have higher mean fatigue and pain scores compared to patients without SGUS changes. This is in agreement with Giloe et al., 33 who reported that fatigue was positively associated with sicca symptoms in patients with SLE. Recently, Mossel E et al. reported that RA-sicca patients had significantly more limitations in daily activities, worse health-related quality of life, and more fatigue compared to RA-non-sicca patients. 34 However, patients with primary SS who were SGUS positive scored significantly lower for fatigue and pain. 35 The association of depression, pain, and fatigue with SGUS-SS changes in patients with primary versus patients with secondary SS is an area that warrants further study.
The proportion of patients with positive anti-Ro and anti-La antibodies was significantly different between patients with abnormal SGUS findings and those with negative SGUS. These results are consistent with previous SGUS studies in both adults and children.16,17,36
In our study, patients with changes on SGUS had similar SLEDAI and SLICC/ACR-DI scores with those without SGUS changes. This is consistent with the findings of Haga et al. and Antero et al. that RA patients with sSS did not have more active disease (using RA Disease Activity score).37,38 Prior studies have shown conflict correlations between SGUS findings and disease activity in patients with pSS.30,31,35 Thus, abnormal SGUS findings might reflect a more severe glandular involvement better than the systemic disease manifestations. However, longitudinal large SGUS studies are required to resolve the question. Additionally, we demonstrated that patients with abnormal SGUS scores did not differ significantly from those with normal findings with regard to age at examination, age at diagnosis, or disease duration in accordance with previous studies.15,35,39 Mossel et al. 35 found that there is no difference in disease duration between patients with medium positive or high-positive SGUS scores. It could be postulated that after certain disease duration there is stabilization in the SGUS lesions, as happened with the production of saliva. 39
There are several limitations in our study. One of these limitations is the relatively small number of patients. We did not include the objective measures of lacrimal and salivary gland structure and function, such as salivary gland biopsy, sialography, and salivary flow. This study was performed at a tertiary academic medical center that may explain the high prevalence of secondary SS detected by SGUS. Abnormal SGUS findings in these patients may be suggestive of subclinical SS, and they might not necessarily specific to SS. The abnormal findings should be taken in the context of the patient’s clinical presentation and should be further evaluated as necessary. Finally, the SGUS evaluation by one operator could be another limitation.
Conclusion
This study supports the use of salivary gland US as a potential simple, non-invasive, inexpensive imaging tool for diagnosis of Sjögren’s syndrome associated with SLE. It also provides real-time, easily accessible information on patients’ salivary gland conditions. Further analysis involving larger samples comparing ultrasound findings to salivary gland biopsy is required to support this finding.
Supplemental Material
Supplemental Material - Diagnostic value of salivary gland ultrasonography for secondary Sjögren syndrome in patients with systemic lupus erythematosus
Supplemental Material for Diagnostic value of salivary gland ultrasonography for secondary Sjögren syndrome in patients with systemic lupus erythematosus by Nevin Hammam, Mona H Elzohri, Amira M Elsonbaty, Zeiad H Eldaly, Osman Hammam, Dalia Tarik, Hamdy Ibrahim and Tamer A Gheita in Lupus.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Medical Research Council at the Assiut Faculty of Medicine, Assiut University.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.