
Abstract
The autoimmune/inflammatory syndrome induced by adjuvants (ASIA), also known as Shoenfeld’s syndrome, encompasses several autoimmune conditions/phenomena that are triggered following the exposure to materials with an adjuvant activity known to augment an antigen-driven immune response. In some inherently vulnerable patients, they act as second hits to trigger or unmask an autoimmune disorder which ranges from generalized non-specific constitutional symptoms, and autoantibody production, to a new onset, of a fully-fledged autoimmune syndrome. In this manuscript, we present a case of a 37-year-old lady who developed systemic lupus erythematosus characterized by mucocutaneous, musculoskeletal, hematological neurological, and renal involvement a few years after silicone breast implants.
Keywords
Introduction
The term autoimmune/inflammatory syndrome induced by adjuvants (ASIA) was first coined in 2011 to codify a growing number of diseases marked by innate and adaptive immune system dysregulation following an exposure to certain adjuvants. We report a case of ASIA syndrome with SLE evolving into cutaneous, musculoskeletal, hematological, neuro-lupus, and lupus nephritis following silicone breast implantation.
The case
A 37-year-old lady of Kashmiri origin presented with 3 weeks’ history of polyarthritis, mouth ulcers puffiness of face, edema feet, and passage of frothy urine. She denied any history of oliguria, hematuria skin rash, chest, cardiac, or gastrointestinal symptoms. Her past history was significant, 20 years back she had undergone silicone breast implants for breast augmentation in a private hospital in New Delhi. Two years post-surgery she started getting Raynaud’s symptoms in winter associated with arthralgia, myalgia, progressive fatigue with sleep disturbances which had somewhat intensified with time requiring analgesics, and gabapentin on a frequent basis. Five years back she had been diagnosed with systemic lupus erythematosus SLE by a physician when she had presented with arthritis, alopecia, oral ulcers, and bullous lesions on the face and trunk with positive ANA, anti-dsDNA. She was then treated with a 6-week course of prednisone which was rapidly tapered and stopped after improvement. Only 6 months back she had developed progressive weakness and heaviness of lower limbs with urinary urgency and was diagnosed with non-compressive dorsal myelopathy based on clinical, electrophysiological testing and imaging.
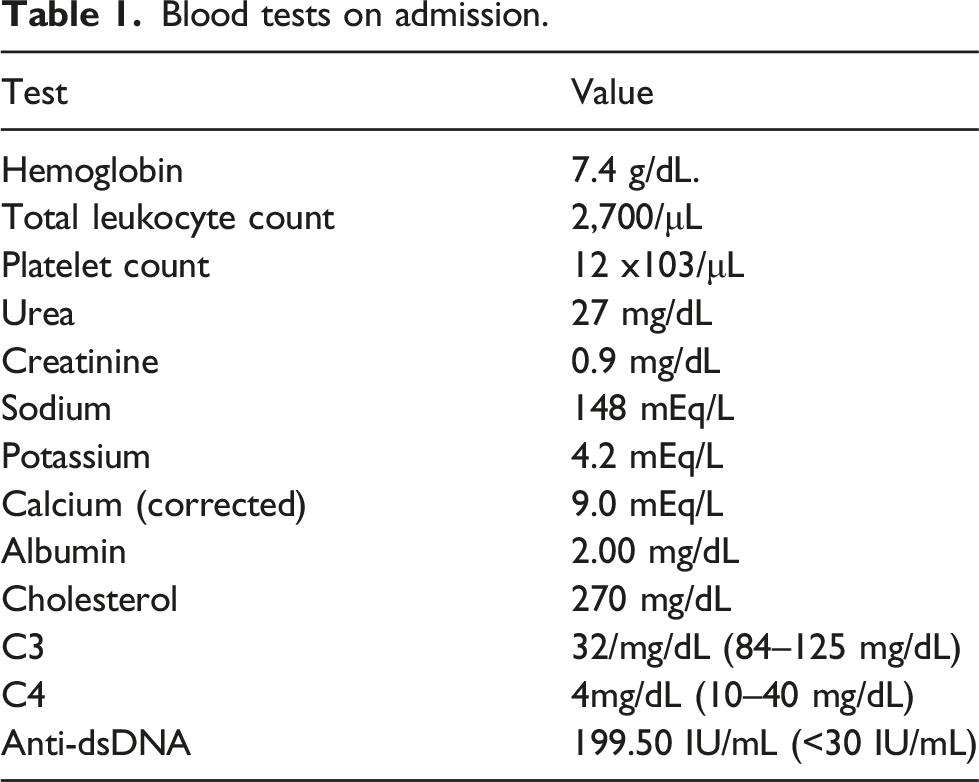
Blood tests on admission.
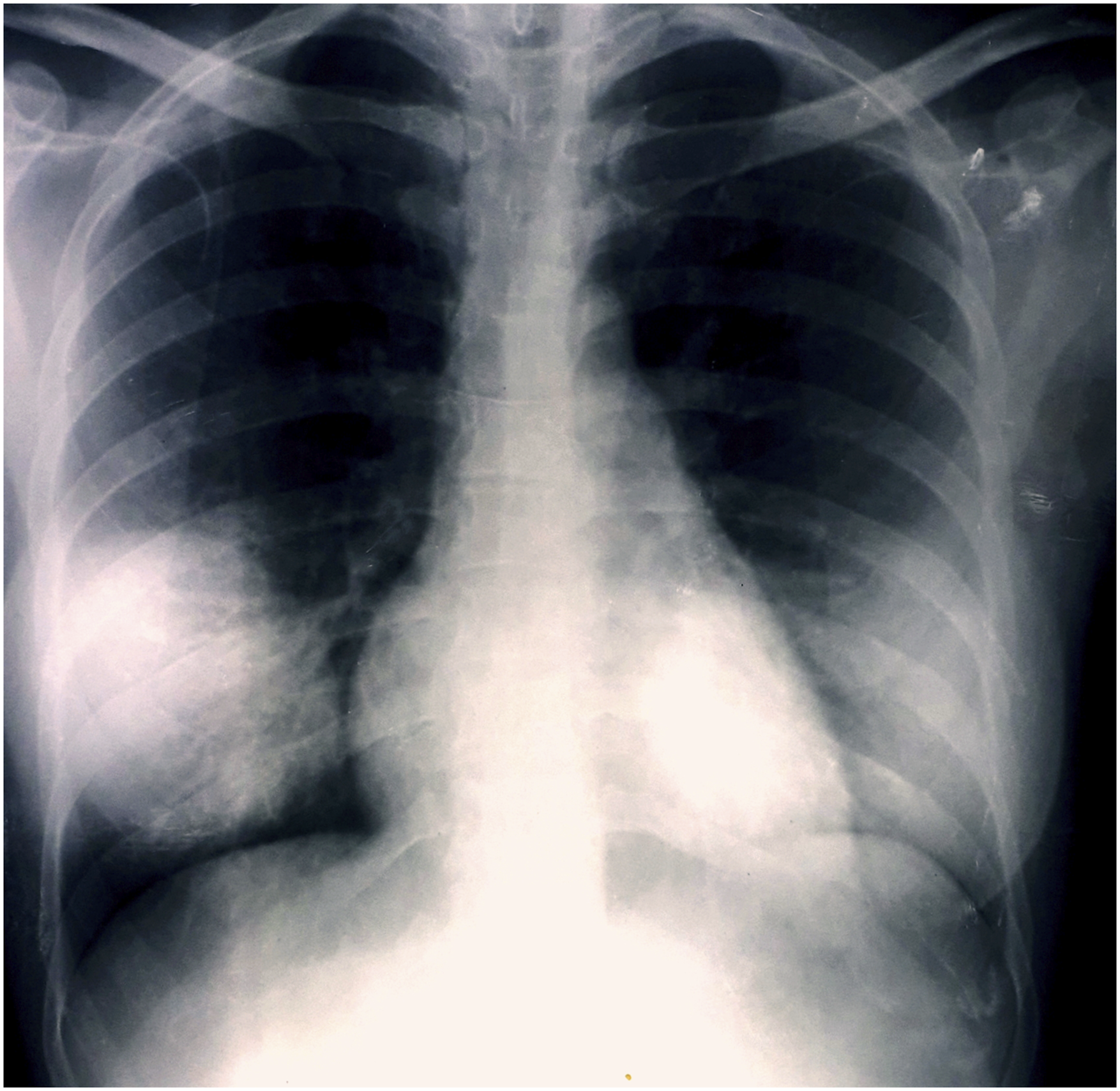
X-Ray Chest P. A. View: Prominent breast shadows due to silicone breast implants.
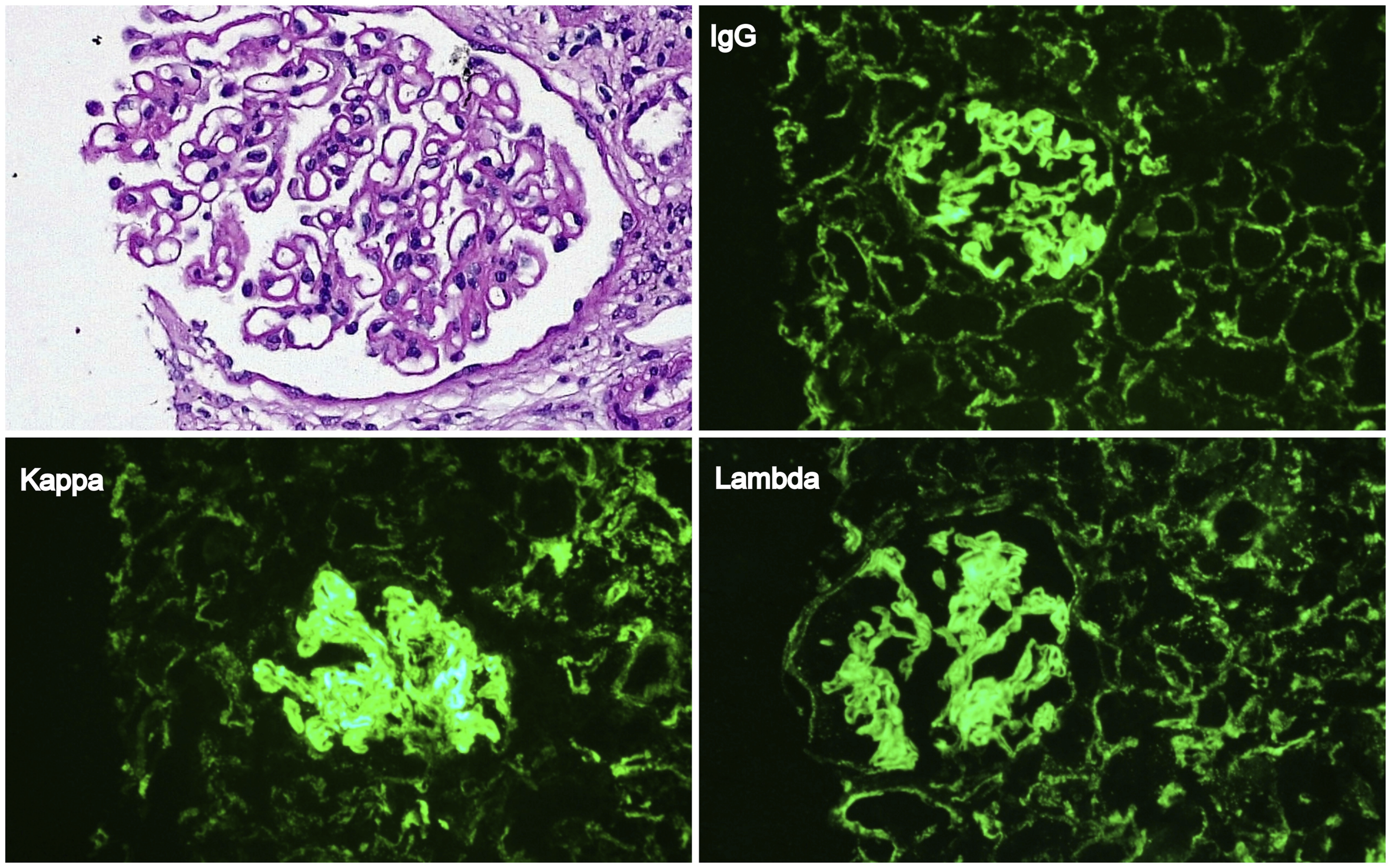
Kidney Biopsy showing: (a) Diffuse thickening of glomerular capillaries with patchy membrane texture alterations and mottling with segmental intracapillary neutrophil/mononuclear cell margination. (H&E X400). (b, c, d) Immunofluorescence showing strong 3+ granular staining for IgG, Kappa, and lambda along glomerular capillary wall and also along a few tubular basement membranes. Moderate 2+ staining for IgA, C3, and C1q was present (not shown in the image).
ASIA syndrome a.k.a. Shoenfeld syndrome defined as autoimmune/inflammatory syndrome induced by adjuvants was first described by Shoenfeld et al in 2011. 1 ASIA syndrome encompasses a set of immunological disorders with heterogenous clinical manifestations that are deemed to occur in certain genetically vulnerable subjects with a strong history of exposure to an adjuvant in which case the latter acts as a second hit in triggering the autoimmune phenomenon. 2 Adjuvants are immunological molecules that are known to enhance an antigen-driven immune response especially in vaccines. 3 These adjuvants are generally safe with a decent tolerability but in some inherently predisposed subjects an autoimmune disease/phenomenon can evolve. ASIA syndrome is sub grouped under the post vaccine autoimmune phenomenon, macrophagic myofasciitis syndrome, the gulf war syndrome, and siliconosis. Siliconosis is one of the autoimmune syndromic phenotype linked to the use of adjuvants. Silicone has been in use for many decades as an essential component in various medical implants including breast and gluteal implants, intraocular lenses, testicular prosthesis, and cardiac valves. Previously regarded as biologically inert, however, growing evidence has implicated silicone as a potential trigger for various autoimmune disorders in genetically vulnerable subjects.4,5 Silicone enhances an immune response by inducing cytokine release and T-cell proliferation. 6 Women with silicone breast implants represent the classical model of silicone induced ASIA syndrome. The presence of HLA-DRB1 and HLA-DQ alleles have been implicated in SBI induced ASIA syndrome. 7 Despite the initial controversy about the cause and effect relationship of silicone in triggering various autoimmune syndromes, recently substantial evidence has accumulated supporting this association. In large population based studies involving women with SBIs, multiple panels of antibodies have tested positive both in symptomatic and asymptomatic women. 8 Many studies have shown that silicone can spark various connective tissue disorders like fibromyalgia, sarcoidosis, Sjogren’s syndrome, undifferentiated connective tissue disorder, scleroderma, and lupus. 9 Recently antibodies against G protein coupled adrenergic and muscarinic acetyl choline receptors of the autonomic nervous system have been found in the sera of women with symptomatic SBIs and the removal of the implants led to attenuation of the symptoms.10,11 In our patient there was no family history of a connective tissue disorder and her rheumatic symptoms started appearing within 2 years of breast implantation which gradually worsened with time and a few years later she developed criteria positive systemic lupus erythematosus with features of the antiphospholipid syndrome (APS) with musculoskeletal and mucocutaneous involvement that improved with steroids. Later on she went on to develop neurological hematological and renal involvement, although her response to immunosuppressants was very good. To the best of our knowledge, this is possibly the first case of silicone induced ASIA syndrome reported having systemic lupus erythematosus with musculoskeletal, mucocutaneous, hematological, neurological, and renal involvement with APS. Her DVT and fatal pulmonary thromboembolism could have been due to an APS or even due to the relapse of her Class V lupus nephritis (membranous nephropathy) with hypoalbuminemia or even a combination of both.12–16
This case presentation is intended to increase the awareness among nephrologists, rheumatologists, immunologists, and physicians about the basic concepts and relative importance of ASIA syndrome. We suggest that patients with various ASIA syndrome phenotypes need to be kept under surveillance for a possible development of autoimmune glomerular nephritis and tubular disorders like autoimmune renal tubular acidosis and besides treating them adequately the removal of the possible triggering agent like silicone implant should be strongly considered. In conclusion growing evidence has revealed that silicone breast implants despite having a relatively wide margin of safety are not as benign as once deemed to be and in some genetically vulnerable patients SBI could actually be an incognito culprit in sparking and fueling a severe autoimmune process.
Footnotes
Author contributions
THM conceptualized the manuscript and wrote the draft and the entire discussion. Was primarily involved in the management of the patient and finalized the manuscript.
AKK was involved in patient management and contributed in writing the case.
MOP performed most of the literature search, arranged it and approved the final manuscript.
PDR revised and modified and approved the manuscript.
AS performed the histopathology and contributed in writing the case.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.