
Abstract
Background
Cyclophosphamide (CYC) has known cytotoxic effects on ovarian reserve and has been linked to premature ovarian failure (POF) in systemic lupus erythematosus (SLE). The concurrent use of gonadotropin-releasing hormone agonists (GnRHas) is postulated to preserve ovarian function by reducing the number of follicles exposed to CYC, but there is paucity of data to establish its efficacy. We conducted a meta-analysis to summarize the effect of concurrent GnRHa use in persevering ovarian function and pregnancy.
Methods
English language databases of PubMed, Embase, and Cochrane were searched to include studies published between 2000 and 2021. Studies in females with rheumatic diseases receiving concurrent GnRHa and CYC therapy to evaluate ovarian preservation as defined by amenorrhea, follicle stimulating hormone (FSH), anti-mullerian hormone (AMH), or estradiol levels or successful pregnancy were included. We used a fixed effect, exact, Mantel-Haenszel approach to estimate the overall odds ratio (OR) and associated 95% confidence intervals (95% CIs).
Results
Seven studies with 218 female patients were included. The ovarian function was preserved in 125/132 (94.6%) of women who received GnRHa concurrently with CYC compared to 50/86 (58%) of women who did not receive GnRHa (OR = 10.3, CI = 4.83–36.29). The OR for pregnancy with GnRHa use = 2.94 (CI = 1.04–9.89).
Conclusion
Our results based on limited published studies suggest that concurrent GnRHa use preserves ovarian function and increase odds of pregnancy. It can be considered for premenopausal SLE females receiving CYC
Introduction
Approximately 90% of the patients diagnosed with systemic lupus erythematosus (SLE) are women, with the majority being diagnosed before the age of 40 during childbearing years. 1 Systemic lupus erythematosus females often delay pregnancy to prevent fetal complications or disease flares during pregnancy. 2 Cyclophosphamide (CYC) is a chemotherapeutic agent that is used to treat organ-threatening cases of SLE, mostly commonly lupus nephritis, and other malignant diseases. 3 However, CYC exposure has been well established to cause gonadotoxicity and premature ovarian failure (POF), as manifested by sustained amenorrhea and abnormal reproductive hormone levels in premenopausal females. 4 Cyclophosphamide causes chromosomal damage to primordial follicles which inhibits estrogen production; in turn, increasing amounts of luteinizing hormone (LH) and follicle stimulating hormone (FSH) are released from the anterior pituitary which recruits more follicles from the ovary and prematurely depletes the follicular pool.5,6 The impact of this cytotoxic medication on the limited germ cells of the ovary is progressive and irrevocable leading to POF in as many as 50% of treated women. 4 Higher cumulative doses of CYC and older patient age seems to play a critical role in increasing the risk of POF, where females over the age of 30 and a cumulative dose greater than 5 g have been associated with a high risk of developing POF.7–12 In addition, other factors such as low neutrophil counts, temporary amenorrhea during treatment, greater SLE-related damage accrual, as measured by Systemic Lupus International Collaborating Clinics (SLICCs) scores > 1, and presence of anti-Sm, anti-RNP, and anti-cardiolipin antibodies have also been associated with higher incidence of CYC related gonadotoxicity.13–15 Cyclophosphamide is a cytotoxic medication used in the treatment of organ-threatening or life-threatening SLE. Furthermore, the use of CYC can result in fewer successful pregnancies with a higher risk of fetal miscarriage and preterm delivery. 16
Several approaches have been utilized for ovarian preservation and fertility in SLE females. The use of embryo or oocyte cryopreservation has been utilized but remains a costly and time-consuming option considering that patients typically initiate CYC treatment while experiencing a life-threatening or organ-threatening flare of SLE.17,18 This approach resulted in high rates of fetal and maternal complications and there are concerns for further increase in the risk of thrombosis in SLE due to ovarian stimulation.17,19 An accessible and cost-effective option to preserve ovarian function is to use gonadotropin-releasing hormone agonists (GnRHas) in conjunction with CYC; however, data about its effectiveness is limited and conflicting. The GnRHas have a dual function whereby they can bind to GnRH receptors in the anterior pituitary to cause desensitization and decrease the release of LH and FSH to prevent ovarian follicle maturation; as a result, fewer follicles are exposed to the toxic effects of CYC. Further, GnRHa reduces the ovarian blood flow where by decreasing the amount of CYC reaching the ovaries.5,6,20 Long-term follow-up studies in both SLE and cancer patients receiving CYC with GnRHa have shown both a positive effect and no difference in POF incidence when compared to patients receiving CYC alone or healthy controls.4,21,22 Both the American College of Rheumatology (ACR) and American Society of Clinical Oncology (ASCO) conditionally recommend the use of GnRHa for premenopausal females receiving IV CYC to induce menstrual suppression and for its possible protective effects on ovarian reserve.23,24 The aim of this meta-analysis is to provide evidence by analyzing existing literature, of the protective effects of GnRHa on ovarian function in lupus patients receiving CYC.
Methods
Data source
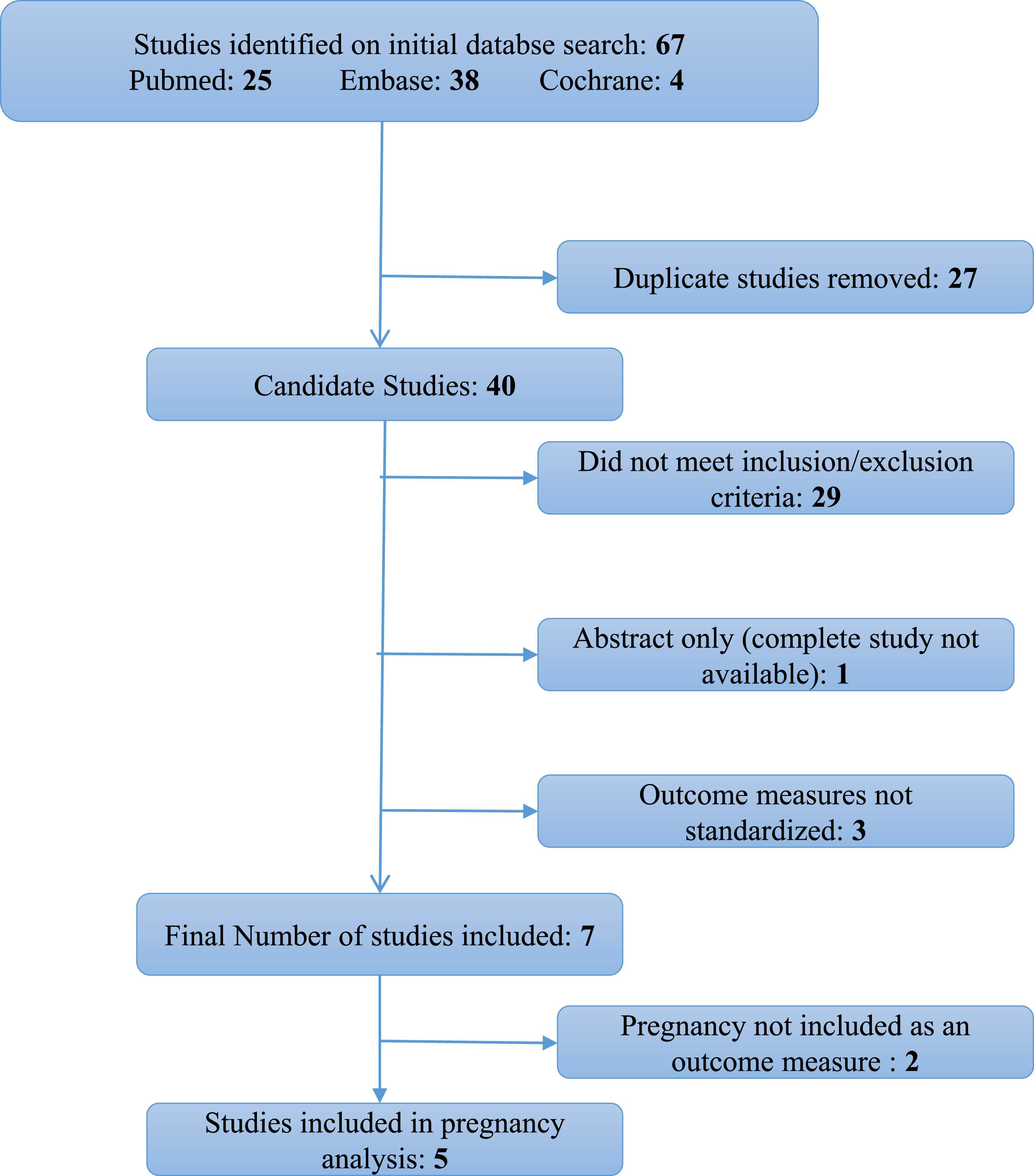
English language databases of PubMed, Embase, and Cochrane were searched for studies that reported an association between use of GnRHa for ovarian preservation in women receiving CYC for autoimmune diseases using key words GnRHa, cyclophosphamide side effects, systemic lupus erythematosus, autoimmune rheumatic diseases, and premature ovarian failure. The meta-analysis was conducted and reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines and checklist. 25 The study was registered with the International prospective register of systematic reviews (PROSPERO).
Study selection
Two investigators reviewed each study. Studies meeting the following inclusion criteria were included: (1) published after 2000 and in English language, (2) female patients with autoimmune rheumatic diseases who received CYC with concurrent GnRHa for ovarian preservation, (3) included a control group who received CYC without GnRHa, (4) defined an objective method of ovarian preservation, such as measuring levels of FSH, anti-mullerian hormones (AMH), estradiol levels, or duration of amenorrhea, (5) full length manuscripts (abstracts submitted to meetings were excluded), and (6) compared successful pregnancy after CYC in patients with and without concurrent GnRHa.
Data extraction and quality assessment
Data were extracted into contingency tables to facilitate the calculation of the odds of ovarian preservation and pregnancy with the concurrent use of GnRHa with CYC by two investigators and reviewed by the entire research group for accuracy. The data in each study were assessed for consistency among abstract, tables, and text.
Data analysis
A fixed-effect, exact, Mantel-Haenszel approach was used to estimate the overall odds ratio (OR) and its 95% confidence interval due to the small number of studies. The Mantel-Haenszel test was derived for the analysis of several 2 x 2 tables to examine the association between an antecedent variable and the presence/absence of an event over the entire set of tables, stratified by another condition (in this investigation, the set of studies). The I2 statistic was also calculated to examine the degree of heterogeneity to see if the use of a random effects model was even warranted, and the I2 value for this study was 22%.
Results
Summary of patient characteristics and POF incidence of eight studies regarding the efficacy of GnRH agonists.
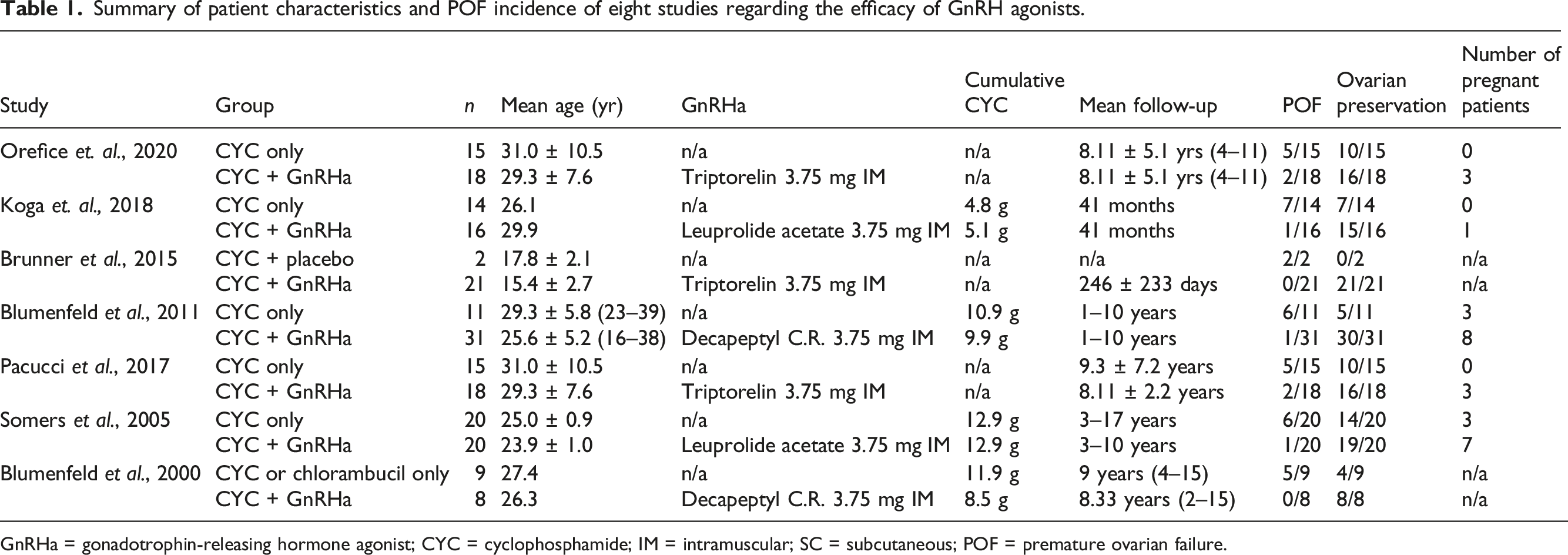
GnRHa = gonadotrophin-releasing hormone agonist; CYC = cyclophosphamide; IM = intramuscular; SC = subcutaneous; POF = premature ovarian failure.
There were a total of 218 female patients with autoimmune diseases, six of these studies included only patients with SLE while study by Blumefield et al. also included 11 patients with other autoimmune diseases. 4 Across all studies, patients in the treatment groups received a monthly injection of 3.75 mg GnRHa concurrently with IV CYC. Two different GnRHa formulations were used in the studies: leuprolide (Lupron, Tap Pharmaceuticals, Deerfield, IL) and triptorelin (Decapeptyl) either intramuscularly (six studies) or subcutaneously (1 study). Only one study described timing of GnRHa at 10 days before CYC (to avoid CYC exposure during initial ovarian hyperstimulation after GnRHa). 6 All studies used an upper limit age of 40 years to define POF. In addition POF was further defined in three studies as amenorrhea for at least 12 months and FSH levels ≥ 40 mIU/mL6,15,26; in one study each by (i) sustained amenorrhea, estradiol concentrations < 100pmol/L, and FSH > 25 IU/L 4 ; (ii) FSH ≥ 23 mIU/mL, LH ≥ 15.9 mIU/mL, and estradiol < 37 pg/mL 26 ; (iii) low estradiol levels, high FSH levels, and menstrual irregularity 27 ; and (iv) measuring FSH and estradiol levels but cutoff values were not provided. 28
Summary of seven study results relating treatment to ovarian preservation status.
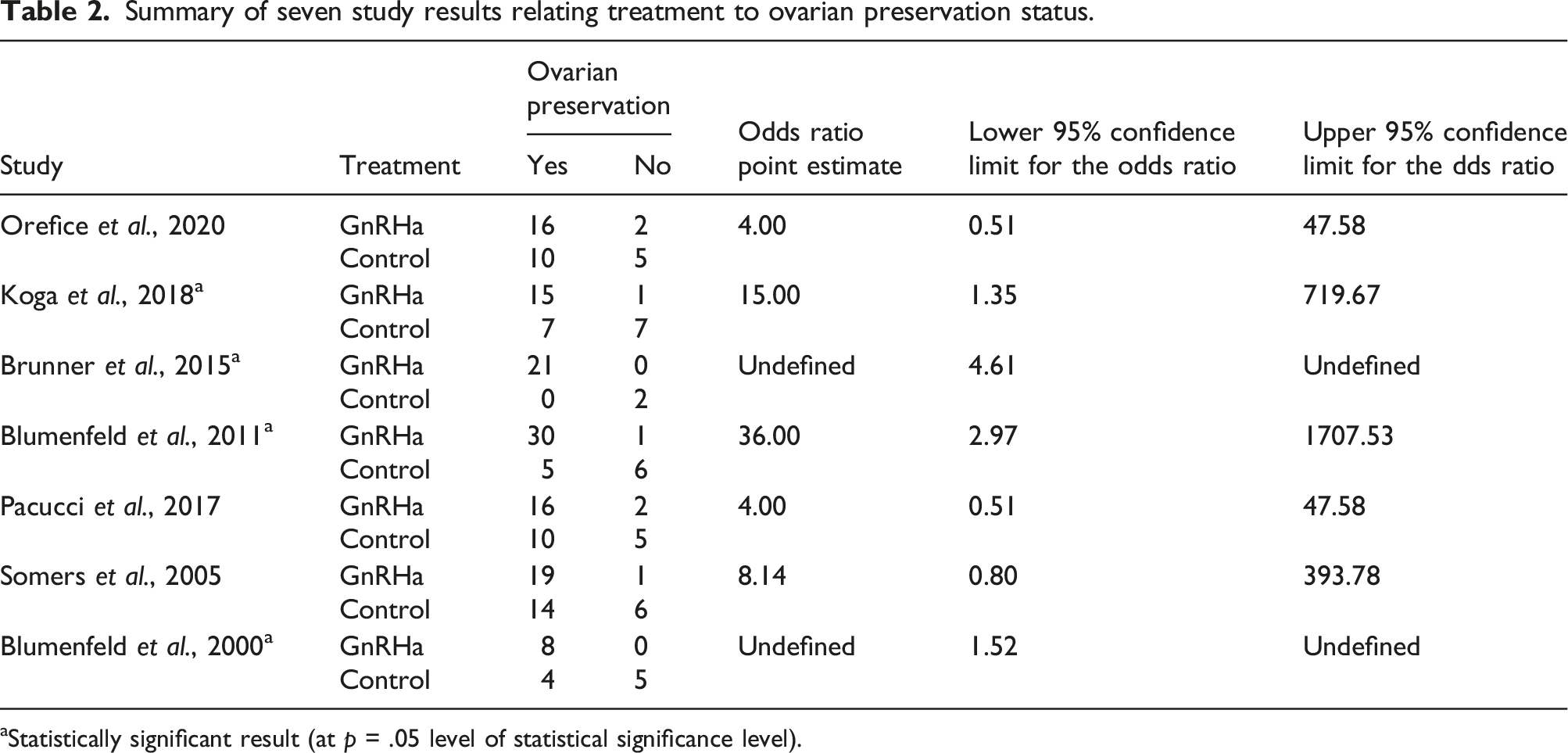
aStatistically significant result (at p = .05 level of statistical significance level).
Exact Mantel-Haenszel estimation results.

Summary of five study results relating treatment to pregnancy.
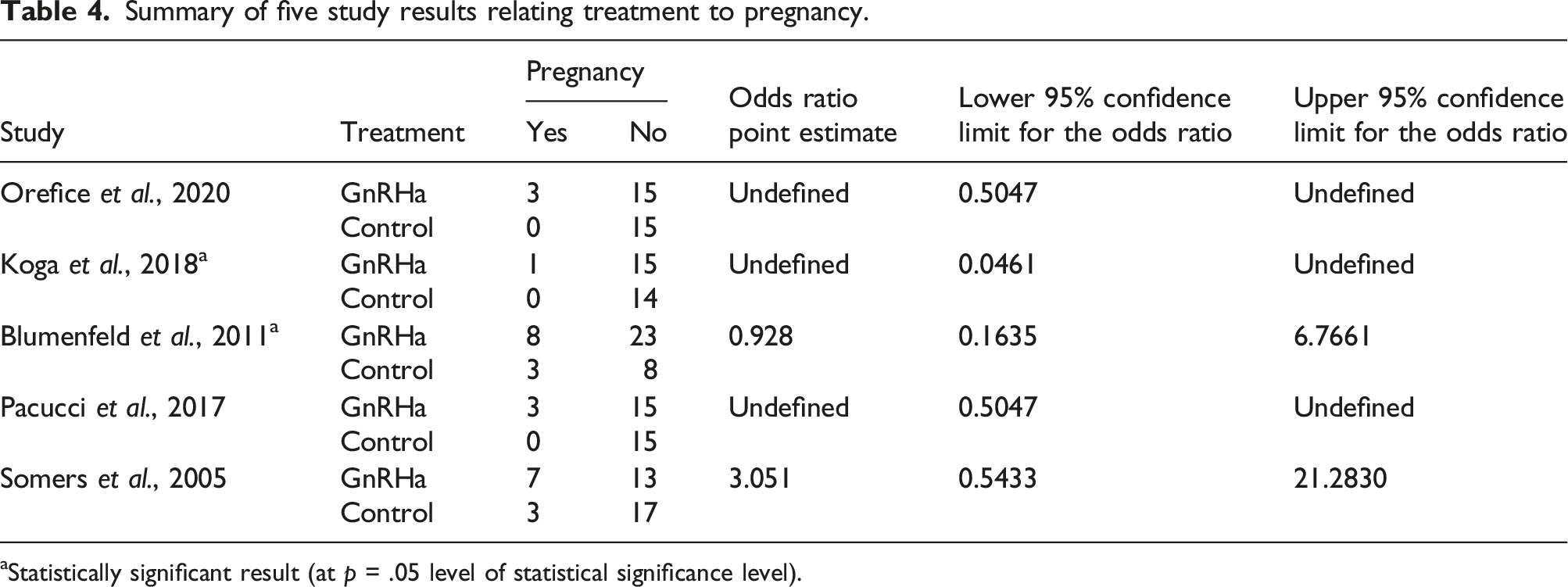
aStatistically significant result (at p = .05 level of statistical significance level).
Exact Mantel-Haenszel estimation results.

Discussion
This meta-analysis demonstrates that concurrent use of GnRHa with CYC is associated with significantly increased odds of a woman with SLE maintaining ovarian function and having a pregnancy following CYC treatment. These results are based on data from limited number of available studies which underscores the need for large, randomized trials to further define the role of GnRHa in ovarian preservation. In the meantime, premenopausal women with SLE and other autoimmune conditions requiring treatment with CYC should be offered concurrent GnRHa if they desire to preserve ovarian function and fertility.
The American College of Rheumatology (ACR) and the American Society of Clinical Oncology (ASCO) recently published guidelines in 2020 conditionally recommending GnRHa for ovarian protection in premenopausal women receiving CYC therapy.23,24 The mechanism by which GnRHa protects ovarian function is postulated to be via noncyclic stimulation of the gonadotrophs of the anterior pituitary gland resulting in release of FSH and LH, followed by desensitization and inhibition of the pituitary-gonadal axis. 29 The use of GnRHa is less invasive and significantly more cost-effective than some of the alternative options available such as cryopreservation of unfertilized ova or embryos. GnRHa also has a better safety profile since ovarian stimulation needed prior to ovarian preservation may lead to SLE disease flare which is not seen with use of GnRHa. 30
Conversely, there are side effects of GnRHa which need to be considered and discussed. Some of the short term side effects that have been associated with GnRHa include hot flashes and vaginal dryness 31 which can be addressed with concomitant estrogen replacement. A more concerning adverse effect reported with GnRHa is decrease in bone mineral density (BMD) due to loss of estrogen-dependent trabecular bone. 32 Studies by Paoletti et al. and Dawood et al. in women with normal baseline BMD demonstrated complete reversibility of BMD loss with 4 months of GnRHa use versus incomplete reversibility with 1 year of its usage, respectively.33,34 However, this observation may not be applicable to women with autoimmune conditions who have additional risk factors for developing osteoporosis such as chronic use of glucocorticoids.
An interesting observation made by a retrospective study of 188 women receiving IV CYC for SLE reported amenorrhea rate of 28.2%, which was significantly higher than 3.7% in non-CYC group (n = 347), and none of the subjects were reported to receive GnRHa. There were 90 pregnancies in the IV CYC group (48.5%) compared to 293 pregnancies in the non-CYC group (58.2%). Furthermore, CYC exposure was associated with significantly higher rates of preterm births. 35 This study and others underscore the deleterious effects of CYC on ovarian function and fertility. Our meta-analysis demonstrates use of concomitant GnRHa with CYC is associated with both increased odds of ovarian preservation and pregnancy. Hence, these limited data support the use of a relatively safe, convenient, and efficacious risk mitigation strategy to preserve ovarian function and fertility.
Our meta-analysis like many others aimed at addressing the question of effectiveness of GnRHa in ovarian preservation was limited by the lack of available data. We had to exclude few studies from our analysis due to the lack of uniform criteria defining POF or absence of a comparator control arm. The relevant studies are additionally limited by relatively small number of subjects and language barrier. From a statistical point of view, the small sample sizes of each study could also cause the commonly used Wald, or large-sample, type confidence intervals to perform improperly. Lastly, in one of the selected studies, all the women receiving the treatment regimen experienced ovarian preservation, the variance of the OR for this study would be undefined and it could not be used in the calculation of the overall OR and corresponding confidence interval for the meta-analysis using most standard approaches. The heterogeneity of small numbers of studies in a meta-analysis is usually greater than that of a larger number of similar studies in a meta-analysis and thus, it might be preferable to use a random effects model to accommodate smaller numbers of studies in a meta-analysis.36,37 However, this approach cannot employ studies in the calculations where all patients in a cohort experience an event or all fail to experience it. 38 Hence we followed a recommendation suggested by Efthimiou 39 to address these issues. A fixed effect, exact Mantel-Haenszel approach would use all available studies with small samples and circumstances where events or their compliment are absent in the treatment or control arms but not both, was chosen for the analysis.
In summary, despite the lack of conclusive evidence for efficacy of GnRHa in patients being treated with CYC, the summarized evidence suggests it provides ovarian protection and increased odds of pregnancy through a noninvasive, readily accessible, and a relatively safe approach. When offering methods of ovarian preservation to patients receiving CYC, it is pertinent to present all available options and the current literature supporting their use with known side effects to involve patients in shared decision making. This meta-analysis also calls out the need for clinical trials in larger patient populations with SLE and other autoimmune conditions to explore the effectiveness and the side effects of GnRHa.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.