
Abstract
Background
Primary antiphospholipid syndrome (PAPS) is characterized by the presence of antiphospholipid antibodies (aPL), repetitive fetal loss, and arterial/venous thrombosis and no association with other autoimmune rheumatic disease. Ocular involvement can also occur including retinal vascular thrombosis and neuro-ophthalmological manifestations, such as optic neuropathy and amaurosis fugax. Early detection of ocular changes is crucial to minimize functional loss.
Purpose
To perform a multimodal evaluation, including the use of Optical Coherence Angiotomography (OCTA), in patients with PAPS without ocular complaints and compare with healthy individuals.
Methods
We performed a complete structural and functional ophthalmological evaluation using OCTA and microperimetry exam in patients with PAPS, followed at a tertiary Rheumatology outpatient clinic.
Results
We included 104 eyes of 52 subjects [PAPS without ocular complaints (N = 26) and healthy individuals (N = 26)]. Among PAPS patients, 21 were female (80.8%) and 21 (80.8%) were Caucasians. PAPS manifestations were venous (65.4%), arterial thrombosis (34.6%), and obstetrical (34.6%) and all of them had lupus anticoagulant. Ophthalmologic findings were more frequent in PAPS compared to healthy individuals (19.2% vs. 0%, p = 0.05). The most common retinal change was paracentral acute middle maculopathy (PAMM) (3 patients, 5 eyes), followed by drusen (1 patient, 2 eyes) and pachychoroid pigment epitheliopathy (PPE) (1 patient, 1 eye). Hypertension and hyperlipidemia were present in 100% of the PAPS patients with PAMM, while only six patients (26.1%) with PAPS without PAMM presented these two risk factors together (p = 0.03).
Conclusions
We provide novel evidence that approximately 20% of our asymptomatic PAPS patients without ocular symptoms have ophthalmologic findings that require early identification and careful surveillance focusing on minimizing systemic and vascular risk factors.
Keywords
Introduction
Antiphospholipid syndrome (APS) is a systemic autoimmune disease characterized by thrombosis and/or pregnancy morbidity, accompanied by medium/high titers of antiphospholipid antibodies (aPL) such as lupus anticoagulant (LA), anticardiolipin (aCL), and/or anti-beta-2 glycoprotein (aβ2GPI). It is currently recognized as the most frequent acquired thrombophilia. APS is classified when at least one clinical and one laboratory criterion is present according to the Updated Sapporo criteria. 1
APS has been classically described as primary (PAPS), occurring in the absence other autoimmune rheumatic disease, or secondary, occurring in the context of a known systemic rheumatological autoimmune disorder, most frequently systemic lupus erythematosus (SLE). 2 APS is associated with arterial and venous thrombotic complications, in addition to non-thrombotic complications. Virtually any organ can be involved, and the presentation varies from acute to chronic and indolent ischemia. 3
The eye can also be a target in APS and the mainly ocular complications in APS include retinal and choroidal vascular occlusions, peripheral proliferative retinopathy and ischemic optic neuropathy. 4 In a retrospective study, antiphospholipid antibodies were associated with retinal vascular occlusions in young patients with no other risk factors, suggesting that aPL should be actively searched in patients with thrombosis in atypical sites. 5 To our knowledge, there are no studies focusing on early changes in retinal microvasculature of PAPS patients without ocular complaints. Prompt identification of early manifestations in patients' retinal microvasculature could avoid ophthalmological complications with risk of profound visual loss or even other more severe thrombotic events. Moreover, asymptomatic retinal vascular changes could potentially be linked to disease severity, thus having systemic therapeutic implications. Therefore, the purpose of this study is to evaluate the association between ophthalmologic manifestations in PAPS patients without ocular complaints using multimodal assessment, including the use of OCTA and microperimetry.
Methods
Study participants
This cross-sectional, observational and descriptive study followed the precepts of the Declaration of Helsinki (1996) and the Nuremberg Code (1947), as well as the Research Norms Involving Humans chosen in Resolution 196/96 of the National Health Council and our Institutional Review Board Ethics Committee. All subjects gave their informed written consent before enrolling in the study. This study was conducted from December 2019 to August of 2021.
Patients with PAPS regularly followed every 3 months at the Rheumatology clinics of Hospital das Clínicas of the University of São Paulo Medical School were consecutively invited to participate and included by convenience sampling. The diagnosis of PAPS was based on the Updated Sapporo classification criteria. 1 All thrombotic patients with PAPS are anticoagulated according to their site of thrombosis: venous (International Normalized Ratio (INR),2,3 arterial (INR 2.5–3.5), or (INR 2–3 plus aspirin). The adjusted Global AntiphosPholipid Syndrome Score (aGAPSS) was adopted to aid in the prediction of thrombotic events. 6
To be included, the subject had to be a consenting adult aged 18 and over, diagnosed with thrombotic PAPS. Patients with eye symptoms were excluded. Other exclusion criteria were: presence of any other systemic autoimmune disease, diabetes mellitus, serious chronic systemic disease, previous brain surgery, ocular surgery, ocular diseases that could affect the retina, choroid or optic nerve (retinopathies, uveitis, optic neuropathies or abnormalities), high myopia (axial length > 26.5 mm or spherical refraction < - 6 diopters), high hypermetropia (spherical refraction > + 6 diopters) or cylinder refraction > ± 3 diopters, intraocular pressure > 21 mm Hg, media opacification preventing proper examination and good quality OCT and OCTA imaging (corneal opacities, nuclear opalescence >2 according to Lens Opacities Classification System III, and vitreous opacities), 7 and best-corrected visual acuity (VA) worse than 20/25.
The healthy control group was paired by sex and age with the PAPS group, following the same exclusion criteria.
Ophthalmologic examination, OCTA image and MP-3 perimeter - acquisition
All patients underwent a complete ophthalmologic examination, including VA evaluation, slit-lamp biomicroscopy, Goldman applanation tonometry, fundoscopy, ocular biometry for axial length measurement (IOL Master 500; Carl Zeiss Meditec, Germany), optical coherence tomography (OCT) and OCTA. In all patients, the pupils were dilated with tropicamide 1% eye drops after visual acuity measurements, to perform a complete fundus examination and to acquire OCT scans with good image quality. Spectral-domain OCT scans were acquired using the SPECTRALIS® OCT module (Heidelberg Engineering, GmbH, Heidelberg, Germany). Macular and peripapillary scanning protocols were used with determined repetition of each image, called predetermined Automatic Real-time Tracking (ART) for each type of acquisition, with an acquisition quality index of at least 25. Images with many artifacts due to movement, projection, duplicated vessels, or distortions were reacquired and all scans were manually reviewed to ensure adequate segmentation.
The macular protocol consisted of a 10°x10°, 15°x15°, or 20°x20° Angio Tomography Scan (512 A-scan/B-scan and 512 B-scan/volume) centered at the fovea. The location of the foveal center was confirmed by cross-referencing the OCT exams associated with the image obtained from the OCTA. The optic nerve head protocol consisted of a 15°x15° Angio Tomography Scan (512 A-scan/B-scan and 512 B-scan/volume) centered at the optic disc. Enface OCTA images of the superficial vascular complex (SVC) and deep vascular complex (DVC) were generated using the automatic segmentation of retinal layers by the Spectralis software. To define the upper and lower limits of the SVC, the internal limiting membrane and 17 μm above the lower edge of the inner plexiform layer were used as references, respectively. The DVC limits were defined as 17 μm above the lower edge of the inner plexiform layer to the rear of the outer plexiform layer.
The microperimetry exam with the MP-3 perimeter (Nidek Technologies) was performed in both eyes of all patients. Patients were dilated with 1 drop of tropicamide 1% 30 min before the exam. For fixation, the target was a red cross, 1° in diameter. To determine the retinal light sensitivity threshold, a red ring fixation target, 1° in diameter, was used on a white, monochromatic background at 31.4 asb (apostilb); a Goldman III stimulus size was chosen, with a 200 ms projection time. The maximum luminance of the MP-3 is 10 000 asb, and the stimulus dynamic range is between 0 and 34 dB. The lower the decibel value at a point, the lower the sensitivity in that region. A personalized grid of 68 test points was positioned identically to the observed in the Humphrey Field Analyser 10–2 test grid. The 4–2 (fast) scheduling method was used with an automatic eye tracker, in order to determine the threshold visual sensitivity of each point. Briefly, in this strategy, a stimulus of greater than expected intensity is presented; if seen, the intensity is reduced in steps of 4 dB until it is no longer observed, increasing the stimulus again at 2 dB intervals, until it is seen again. Self-tracking and auto-alignment functions ensured accurate measurements. A flash color fundus photograph with a resolution of 1388x1038 pixels and 45° was taken at the end of the examination, thus allowing visual function to be superposed and therefore compared to retinal structures.
Statistical analysis
Statistical analysis was performed using SPSS Version 22 (Chicago, Illinois). Categorical variables were presented as numbers and percentages and were analyzed by Fisher’s exact test. Normality was analyzed by the Shapiro–Wilk test. Continuous variables were expressed as mean and standard deviation (SD) or median and interquartile range. A p-value of <0.05 was considered as statistically significant.
Results
Demographic and clinical characteristics of 26 PAPS patients (N = 26).
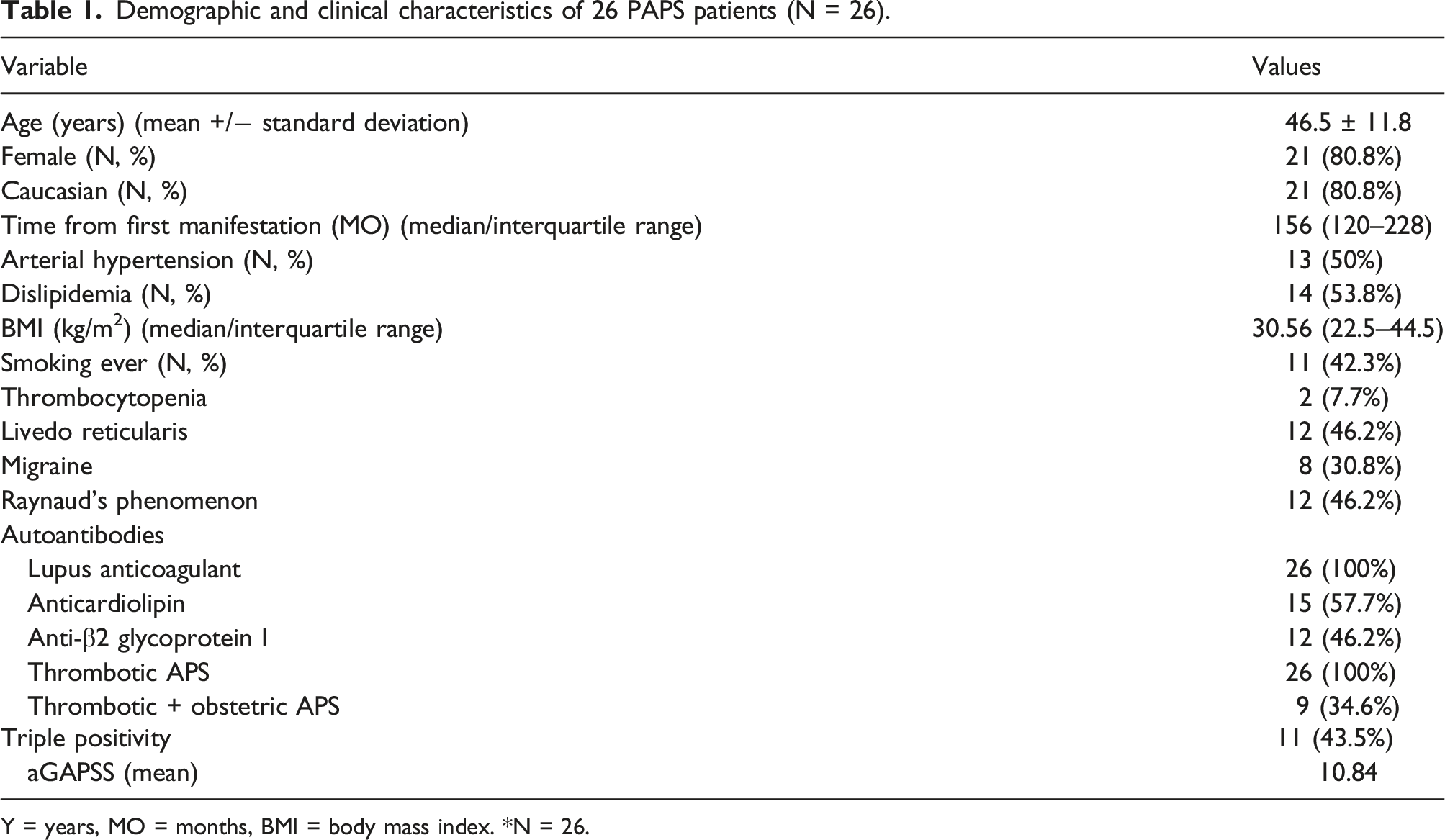
Y = years, MO = months, BMI = body mass index. *N = 26.
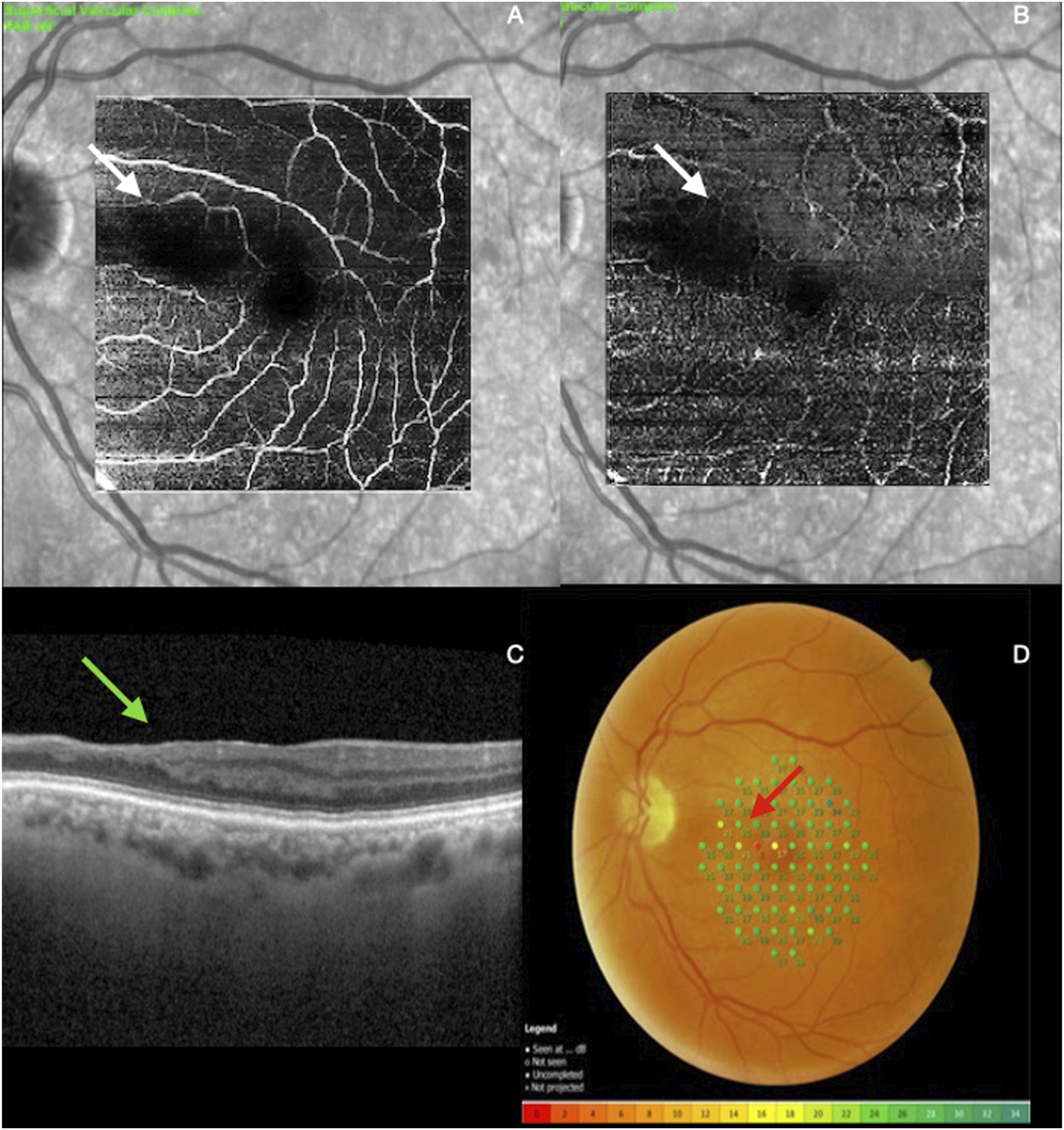
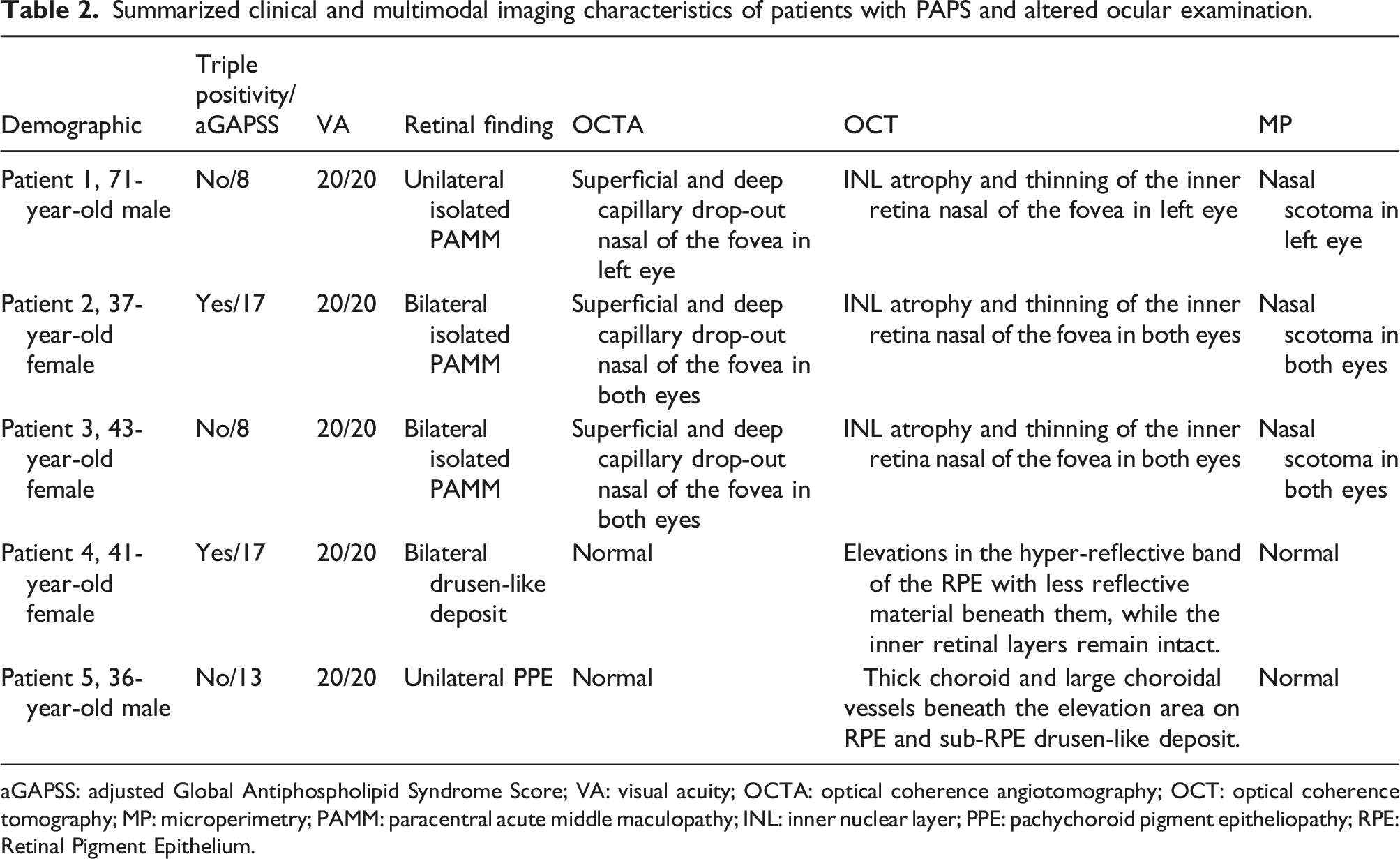
Five (19.2%) PAPS patients presented with ophthalmologic findings versus none of healthy individuals (p = 0.05) (Figure 1). The most common change was PAMM (3 patients, 5 eyes) (Figure 2), followed by drusen-like deposit (1 patient, 2 eyes) and pachychoroid pigment epitheliopathy (PPE) (1 patient, 1 eye). Hyperlipidemia and hypertension were present in 100% of the patients who presented PAMM, while only six patients (26.1%) with PAPS without PAMM presented these two risk factors together (p = 0.03). 66% (2 of 3) of PAPS patients who presented PAMM had previous arterial thrombosis, while it was present only in seven patients (30.4%) with PAPS without PAMM (p = 0.26). A trend of higher mean values of aGAPSS in both groups of patients with and without PAMM (11 ± 5.2 vs. 10.8 ± 4.4, p = 0.09) was observed. Similar frequency of triple positivity to aPL was observed in PAPS with PAMM compared to those without this condition (33.3% vs. 43.5%, p = 0.73). Clinical and multimodal exam findings are summarized in Table 2. Normal exams in a healthy individual. Enface OCTA demonstrating normal vascular superficial (a) and deep (b) capillary plexus. (c) SD-OCT normal b-scan. (d) Microperimetry sensitivities. Patient with a late (chronic) stage of PAMM in the left eye. Enface OCTA demonstrate focal vascular remodeling with localized occlusion (white arrows) of the intermediate (a) and posterior capillary (b). (c) The perfusion void coincides with the SD-OCT thinning of the retinal inner layers (green arrow). (d) Microperimetry sensitivities were significantly lower at the corresponding points in the atrophic areas shown on OCT and OCTA (red arrow). Summarized clinical and multimodal imaging characteristics of patients with PAPS and altered ocular examination. aGAPSS: adjusted Global Antiphospholipid Syndrome Score; VA: visual acuity; OCTA: optical coherence angiotomography; OCT: optical coherence tomography; MP: microperimetry; PAMM: paracentral acute middle maculopathy; INL: inner nuclear layer; PPE: pachychoroid pigment epitheliopathy; RPE: Retinal Pigment Epithelium.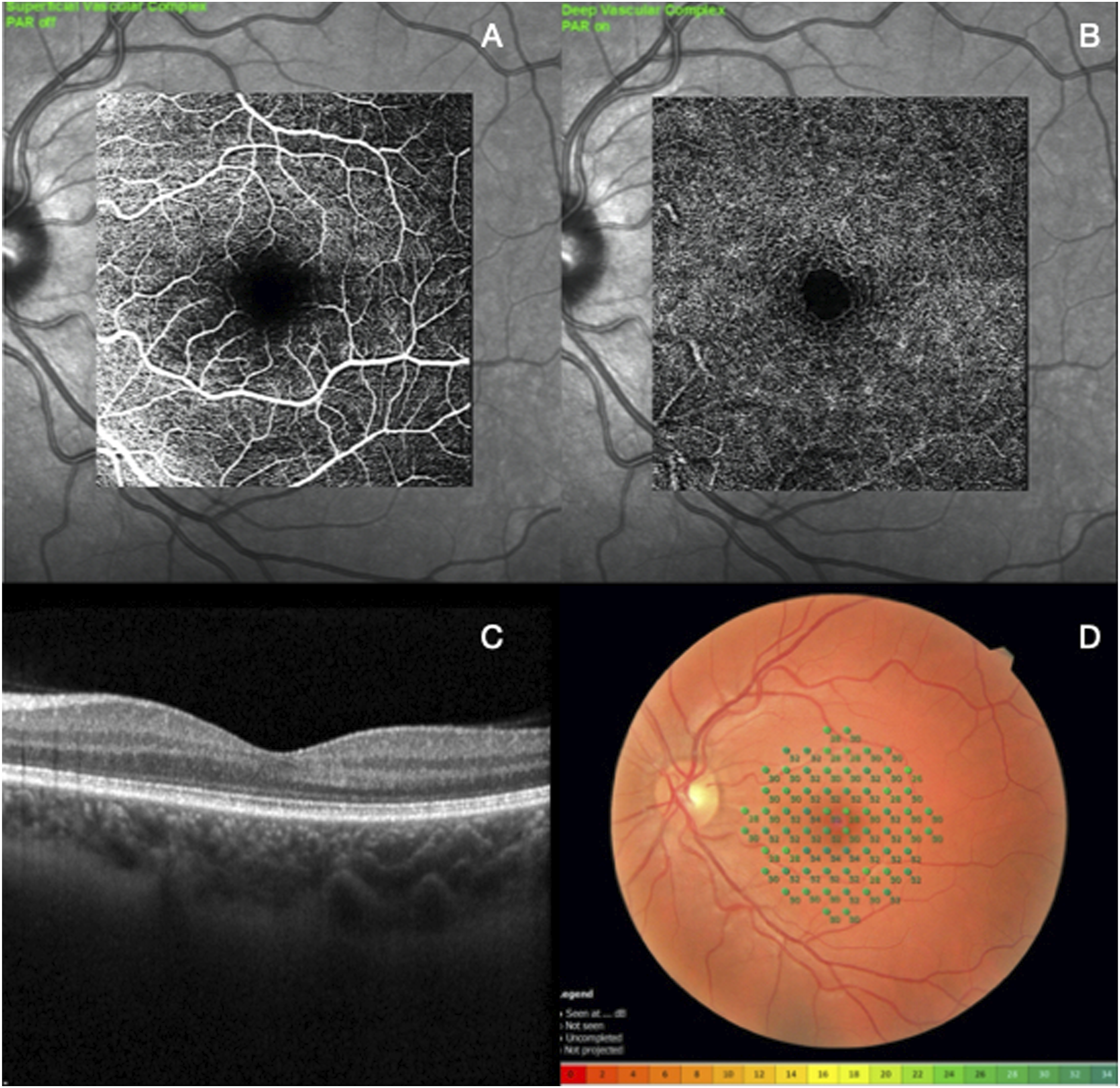
Discussion
Our study supports that PAPS patients without ocular manifestations have retinal alterations and some of them may be related to underlying prothrombogenic condition of this disease.
The major advantage of this study is the well characterized population of PAPS patients fulfilling rigorously the criteria for this rare syndrome. The inclusion of secondary APS in previous studies precludes a definitive conclusion about their findings since cotton-wool spots, choroidal infarcts, serous macular detachment, and vitritis were also reported in other immunological diseases, particularly SLE.8,9 In addition, all patients were asymptomatic allowing a more precise definition of subclinical eye involvement in this syndrome. The cross-sectional design and the small number of patients are relevant limitations of the present study.
The lack of anterior ocular findings in the present study is consistent with the knowledge that this eye segment is not commonly involved in PAPS. 4 Additionally, the exclusion of patients with ocular manifestation may account for this observation. In fact, previous reports described scleritis, filamentary keratitis, and iritis, accounting for 75% of the anterior segment changes and these conditions are usually symptomatic.10–12
On the other hand, the posterior segment of the eye (retina, choroid and optic nerve) is described as the most frequently affected in PAPS patients with ocular manifestations. 8 Retinal vascular occlusions, whether arterial and/or venous, are the most often described alterations in these patients.13–15 Unexpectedly, approximately one-fifth of asymptomatic APS patients had retinal changes.
We demonstrated herein that the parafoveal region is the most frequent site for ischemic lesion in asymptomatic APS. Late-stage PAMM was observed in three patients (five eyes) and suggests that APS thrombogenic disorder may underlies this alteration. This condition was described for the first time in 2013 by Sarraf et al., 16 and it is characterized by the infarction of the inner nuclear layer (INL) due to ischemic events located in the intermediate capillary plexus and deep capillary plexus (DCP) of the retina.17,18
PAMM is typically associated with a permanent paracentral scotoma, identified in the microperimetry exam and/or visual field, although central visual acuity prognosis is often excellent and the patient may be asymptomatic, 19 as were the three patients described here. OCT is the most sensitive and specific technique to identify PAMM and, therefore, serves as the basis for diagnosis. 20 In the acute phase, PAMM appears as a hyper-reflective band spanning the INL. In the late phase, the lesion evolves to INL thinning. 21 The advent of OCTA exam helped to understand that the hyperreflectivity band represents infarction of the INL and is due to DCP hypoperfusion. OCTA segmentation at the DCP has shown hypoperfusion of the DCP in both acute and chronic lesions. 22 The retinal sensitivity defect demonstrated with microperimetry also colocalizes with deep capillary flow deficit in OCTA. 23
The presence of PAMM raises a wide differential diagnosis that requires a systematic workup to exclude potential vascular, inflammatory, infectious, toxic and iatrogenic causes. The main associated systemic conditions are diabetes mellitus (DM) and hypertension, however, it can also be present in a variety of other clinical illnesses.18,21 The DM was excluded in the present study. Recently, case reports have associated PAMM with hypercoagulable disorders such as APS with eye manifestations24–26 and we extend this observation to ocular asymptomatic PAPS patients.
Hypertension and hyperlipidemia are also well-documented risk factors for PAMM and for thrombosis recurrence in APS patients. 27 In line with this observation, all PAPS patients with PAMM evaluated herein had concomitant hypertension and dyslipidemia whereas in those without PAMM, these two risk factors occurred simultaneously in only approximately one-fourth of them. This significant association identifies the triple comorbidity group as high-risk factor for PAMM and raises the hypothesis that these patients may require a more appropriate treatment target. Reinforcing this possibility high levels of aGAPSS, an independent prognostic factor for thrombosis, was observed in patients with PAMM, all of them above the mean of 7.6 aGAPSS reported for patients that experienced arterial thrombosis recurrence. 28 In contrast, triple positivity was not associated with PAMM in spite of previous observation that this profile imposes the greatest risk for thrombotic and obstetric events. 29
Macular drusen-like deposit was diagnosed in one patient, a condition usually related to aging 30 but the patient was 41 years old. Another patient presented with PPE, a commonly asymptomatic disease characterized by focal RPE abnormalities overlying abnormal and permanent increase in choroidal thickness (pachychoroid disease), without the presence of subretinal fluid. The precise etiology and pathogenesis of this eye condition remains unknown, but systemic use of glucocorticoid and sympathomimetics are reported as risk factors.31,32
In conclusion, we identified that more than 10% of our ocular asymptomatic PAPS patients have PAMM, an uncommon retinal disorder related to ischemia of retinal capillary plexus. The shared underlying mechanism of these two conditions related to the thrombotic milieu as well as their common association with other risk factors for vascular occlusion such as hyperlipidemia and hypertension supports the notion that PAPS patients should be investigated for subtle ocular involvement.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (88887507684202000) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (307787/2021-4).