
Abstract
Objectives
This study aimed to investigate the incidence rate and risk factors of bloodstream infection (BSI) in patients with systemic lupus erythematosus (SLE) exposed to medium to high doses of glucocorticoids.
Methods
This study included 1109 treatment episodes with prolonged (≥4 weeks) medium-to-high-dose glucocorticoids (≥15 mg/day prednisolone) in 612 patients with SLE for over 14 years. Clinical features regarding systemic lupus erythematosus disease activity index 2000 (SLEDAI-2K), immunosuppressant use, and laboratory results were obtained from the electronic medical database. The primary outcome of this study was the 1-year incidence of BSI. The effect of clinical factors on the outcome was investigated using a generalized estimating equation.
Results
During a total of 1078.64 person-years, 30 cases of BSI occurred, with an incidence rate of 2.78 (95% confidence interval (CI) 1.88–3.97) per 100 person-years. Mortality rate of the treatment episodes with BSI was 16.7%, which was significantly higher than that in the other episodes (incidence rate ratio (IRR) 19.59, 95% CI 7.33–52.44). When the incidence rate of BSI was stratified by baseline glucocorticoid dose and SLEDAI-2K score, a higher incidence rate of BSI occurred as disease activity or baseline glucocorticoid dose increased. In the multivariable analysis, SLEDAI-2K ≥20 (adjusted IRR (aIRR) 4.66, 95% CI 2.17–10.00), initial baseline prednisolone ≥ 60 mg/day (aIRR 2.42, 95% CI 1.11–5.32), and cumulative prednisolone dose ≥15 mg/day during the previous 6 months (aIRR 2.13, 95% CI 1.03–4.40) significantly increased the risk of BSI.
Conclusion
In patients with SLE exposed to prolonged medium-to-high-dose glucocorticoids, the 1-year incidence rate of BSI was significantly higher than previously reported in the general patients with SLE. Severe disease activity, and high-dose glucocorticoid treatment previously or at baseline increased the risk of BSI.
Keywords
Introduction
Over the past few decades, the survival of patients with systemic lupus erythematosus (SLE) has significantly improved owing to early diagnosis and appropriate management of organ involvement with effective immunosuppressive agents, including high-dose glucocorticoids. The 5-year survival rate of patients with SLE improved from approximately 50% in the 1950s to over 90% since the 1990s. 1 However, infection remains a significant cause of morbidity and mortality in SLE. 2 Severe infection in patients with SLE has been shown to have the highest incidence rate in the first year after diagnosis and is the leading cause of death during the first 5 years.3,4 Abnormal cell-mediated immunity and complement deficiency in patients with SLE increase their susceptibility to infection.5,6 In addition, immunosuppressive agents for treating SLE have been shown to increase the risk of various infections. Among them, glucocorticoids which are an important treatment for SLE, is a well-known risk factor for infections, especially at high doses during induction therapy. 7
Among the various infections, bloodstream infection (BSI) is a major burden with a considerable mortality in patients with SLE. Previous studies suggested that BSI in patients with SLE was associated with an increased mortality rate, mainly in the early phase of the disease. 8 In addition, other studies have shown that BSI can be a risk factor for developing a severe flare. 9 However, few studies have investigated the relationship between disease activity, immunosuppressant use, and BSI risk in patients with SLE. Therefore, despite its clinical significance, there are few evidence-based guidelines regarding the monitoring and prophylaxis of BSI in patients with SLE. To address this clinical question, we investigated the incidence and risk factors of BSI in patients with SLE who received prolonged, medium-to-high doses of glucocorticoids.
Methods
Study design and treatment episode
This research was a single-center retrospective cohort study. We examined the database of electronic medical records at Seoul National University Hospital to identify the clinical event in which patients with SLE were consecutively treated with medium-to-high doses of glucocorticoids (≥15 mg/day of prednisolone or equivalent) for more than 4 weeks (defined as a treatment episode) between January 2004 and December 2017. The date of starting medium-to-high dose glucocorticoid in each treatment episode was defined as its index date. Included treatment episodes were followed up until death, loss of follow-up, or one year from the index date, whichever came first. If two treatment episodes in one patient were spaced more than 1 year apart, each one was considered an individual treatment episode. Observational scheme of the treatment episode was illustrated in Supplementary figure S1.
All patients fulfilled four or more of the 1997 ACR revised classification criteria for SLE at the time of diagnosis. 10 Patients with a history of a solid organ or bone marrow transplantation, active cancer, or those younger than 18 years of age were excluded. This study was approved by the Institutional Review Board (IRB No. 2009-065-1156), and patient consent was waived due to the retrospective nature of the study.
Data collection
For each treatment episode, we collected data on demographics, clinical manifestations of SLE, SLEDAI-2K score, and laboratory findings at the index date. Prescription data of immunosuppressive agents before and after one year from the index date were also collected to capture concomitant immunosuppressive use and cumulative dose of glucocorticoid previous 6 months from the index date. To detect a BSI, all blood culture data preformed in the study population during the observation period were captured.
Outcomes
The main outcome in this study was the incidence of BSI during the observation period. In addition, we investigated the incidence rate of each group stratified by disease activity, evaluated using the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) and the initial dose of glucocorticoid at the index date. Finally, clinical factors significantly associated with BSI were investigated.
Detection of BSI during observation periods
BSI was defined as a pathogen confirmed in the blood in the presence of clinically apparent signs or symptoms of systemic inflammatory response syndrome. 11 Medical records of the treatment episodes with any positive results for blood culture test were reviewed by one author (MHK) to confirm the BSI and to investigate the causative microorganism, anatomical infection source, and clinical features. If a common skin microorganism such as coagulase-negative Staphylococcus species, Bacillus species, and Corynebacterium species was isolated, at least two different positive blood cultures were required for diagnosis of BSI. If the patient had positive blood cultures for different pathogens during the same hospitalization period, it was counted as one event. BSI-related death was defined as death occurring during hospitalization without evidence of previous disease-related severity and was strongly suspected to be an infection-related event.
Statistical analysis
Numerical variables were expressed as mean and standard deviation (SD), and categorical variables were described as absolute frequencies and percentages. Continuous or dichotomous baseline data were compared using Student’s t-test or the χ2 test, as appropriate. To investigate the clinical factors related to the incidence of BSI in the treatment episodes, we used generalized estimation equation (GEE) Poisson regression to consider intracluster correlation caused by multiple treatment episodes from one patient. The relative risk ratio (RR) was adjusted for baseline clinical factors with a relevant association with the outcome (p < 0.1) in the univariate analysis. When two covariates had a clinically relevant correlation (i.e., baseline SLEDAI-2K and initial glucocorticoid dose), Pearson correlation coefficient was calculated and one of them was removed from the multivariable model if the coefficient > 0.7. We used multiple imputations to handle the missing values, which mainly occurred in the presence of urinary casts, proteinuria, or hematuria in the treatment episodes in patients without clinical manifestation of nephritis. The main analysis was performed after applying multiple imputations, and the same analysis was repeated without applying imputations as a sensitivity analysis. In addition, we analyzed the effect of clinical factors on the outcome using the Cox proportional hazard model. Finally, we repeated the same analysis after excluding catheter-related BSI (CRBSI).
All statistical analyses were performed using SPSS (version 26.0; SPSS Inc., Chicago, IL, USA), and a p-value <0.05 was considered statistically significant.
Results
Baseline characteristics
Baseline characteristics of the study population (N = 1109)
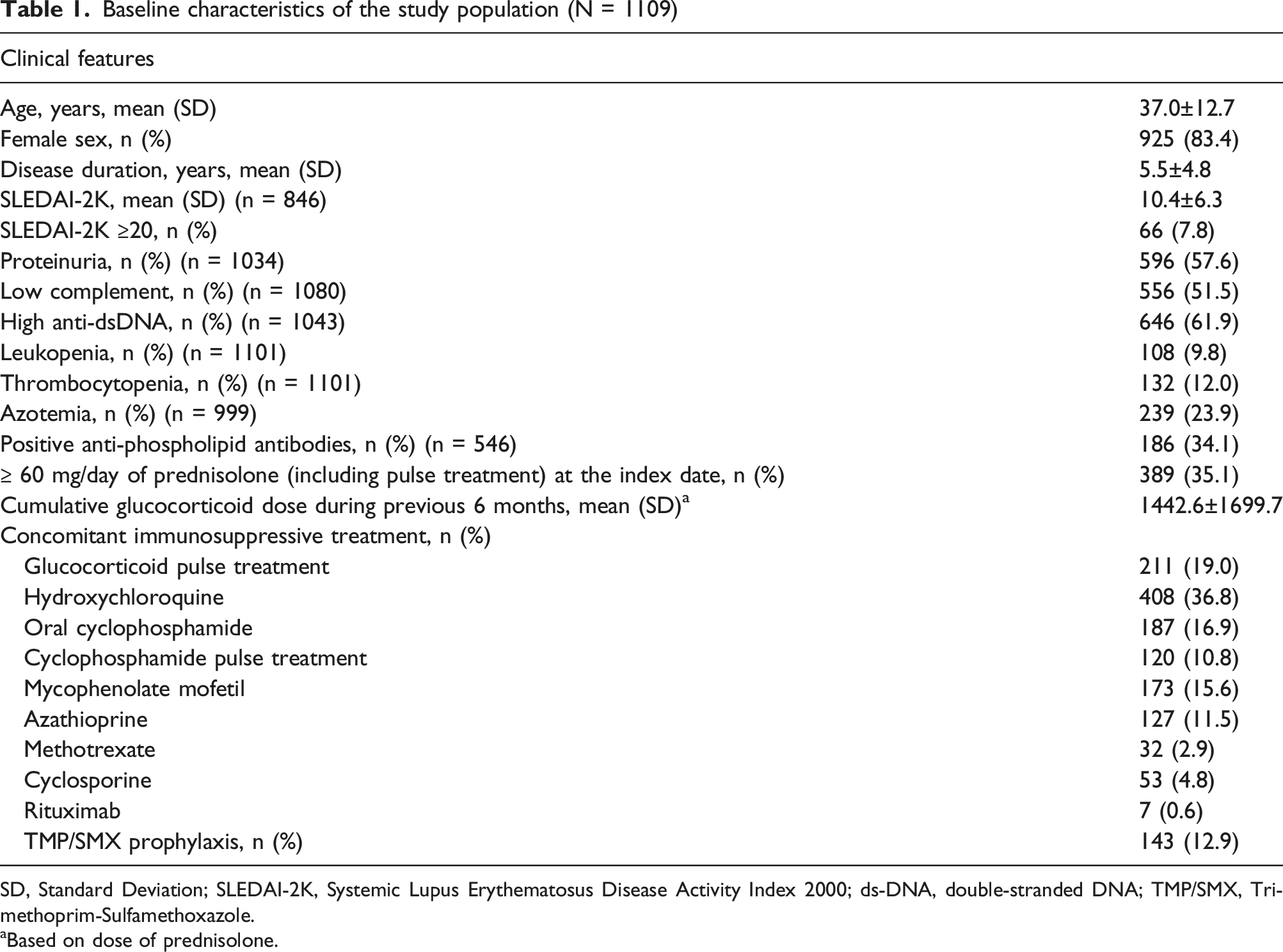
SD, Standard Deviation; SLEDAI-2K, Systemic Lupus Erythematosus Disease Activity Index 2000; ds-DNA, double-stranded DNA; TMP/SMX, Trimethoprim-Sulfamethoxazole.
aBased on dose of prednisolone.
The number of treatment episodes with a SLEDAI-2K score ≥ 20 at baseline was 66 (7.8%). The most common clinical manifestation in this subgroup was nephritis (n = 50; 75.8%) (Supplementary table S1). Regarding treatment for SLE at the index date, the subgroup received cyclophosphamide pulse therapy more frequently and were treated with higher dose of glucocorticoid than the treatment episodes with SLEDAI-2K <20.
Incidence and clinical characteristics of BSI
Clinical characteristics at the time of BSI and its outcomes (N = 30)
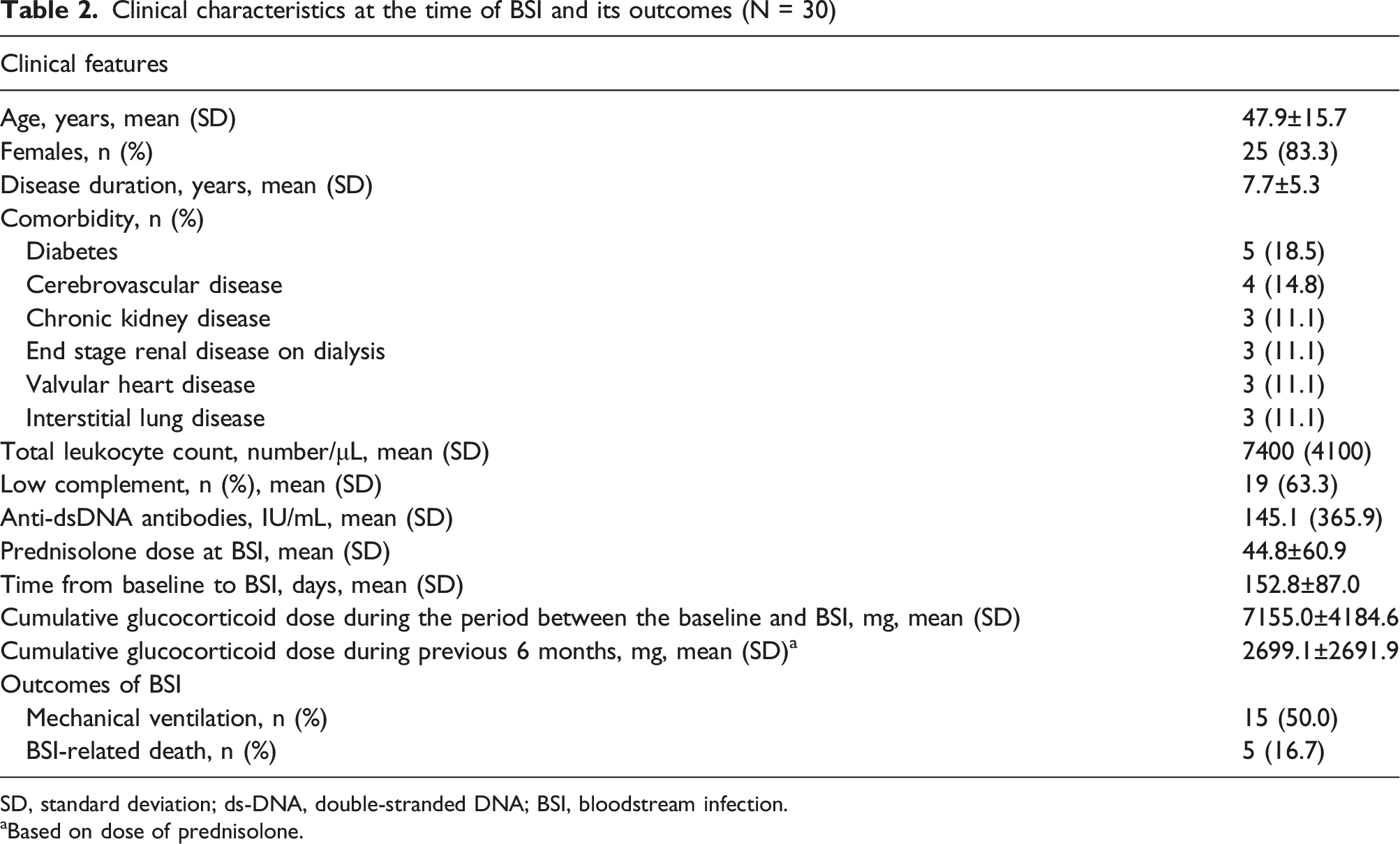
SD, standard deviation; ds-DNA, double-stranded DNA; BSI, bloodstream infection.
aBased on dose of prednisolone.
Among the BSI events, Escherichia coli (E. coli) was the most common microorganism (30.0%), followed by Staphylococcus aureus (26.7%) and coagulase-negative Staphylococcus (10.0%) (Supplementary table S2). Regarding the area of acquisition, the respiratory tract (20.0%) was the most common infection focus, followed by the urinary tract, soft tissue, and catheter-related BSI, all of which was 16.7%. Finally, the origin remained undetermined in three (10.0%) cases.
Clinical factors associated with the incidence of BSI
The BSI incidence rate increased with the use of a higher dose of glucocorticoid at baseline, with 5.01 (3.01–7.82) per 100 person-years in patients treated with ≥ 60 mg/day of prednisolone or its equivalent at baseline (Figure 1(a)). Additionally, SLE disease activity results showed a similar effect on the risk of BSI. The incidence rate rose with increasing SLEDAI-2K index and was 12.93 (5.57–25.48) in those with SLEDAI-2K ≥20. This subgroup of treatment episodes showed higher BSI incidence than other subgroups with lower SLEDAI-2K. By contrast, there were no significant differences among subgroups with SLEDAI of less than 6, between 6 and 10, and between 11 and 19 (Figure 1(b)). Incidence rate of bloodstream infection in the study population stratified by (a) initial dose of glucocorticoid (based on prednisolone, PD) and (b) initial disease activity measured by SLEDAI-2K.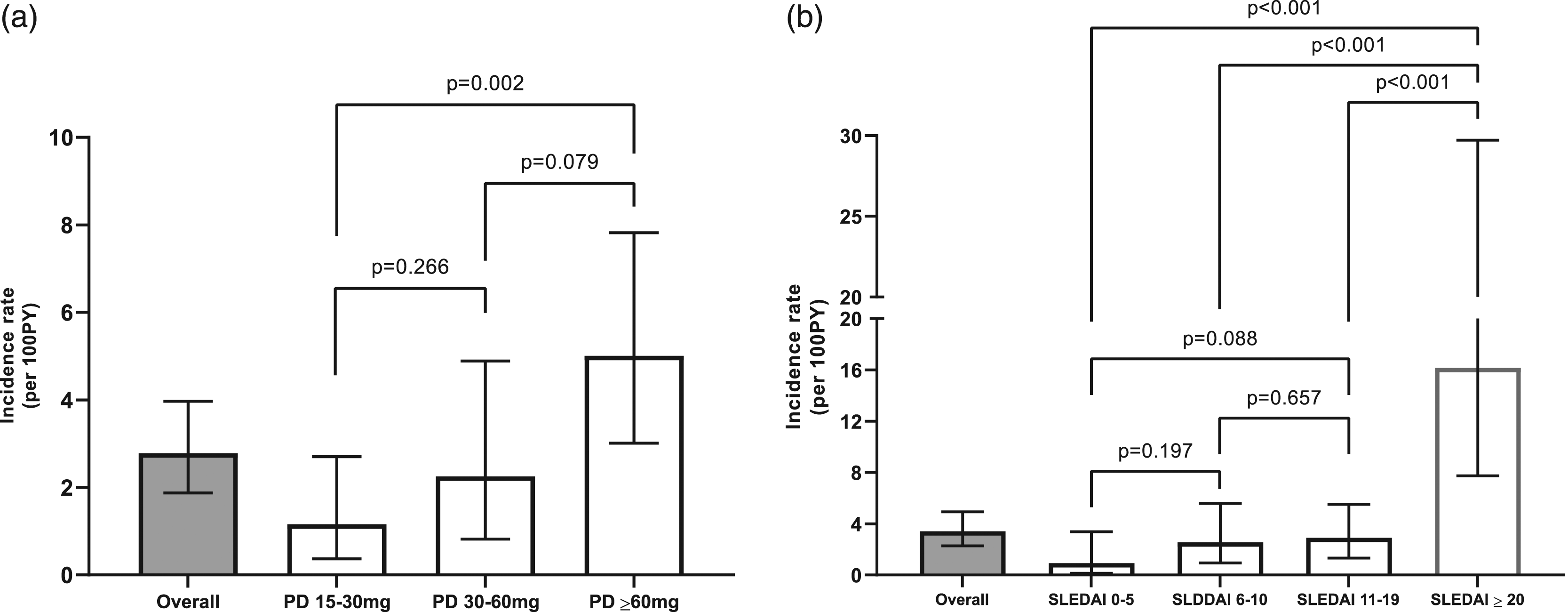
Clinical factors affecting incidence of bloodstream infection in study population after multiple imputation analysis
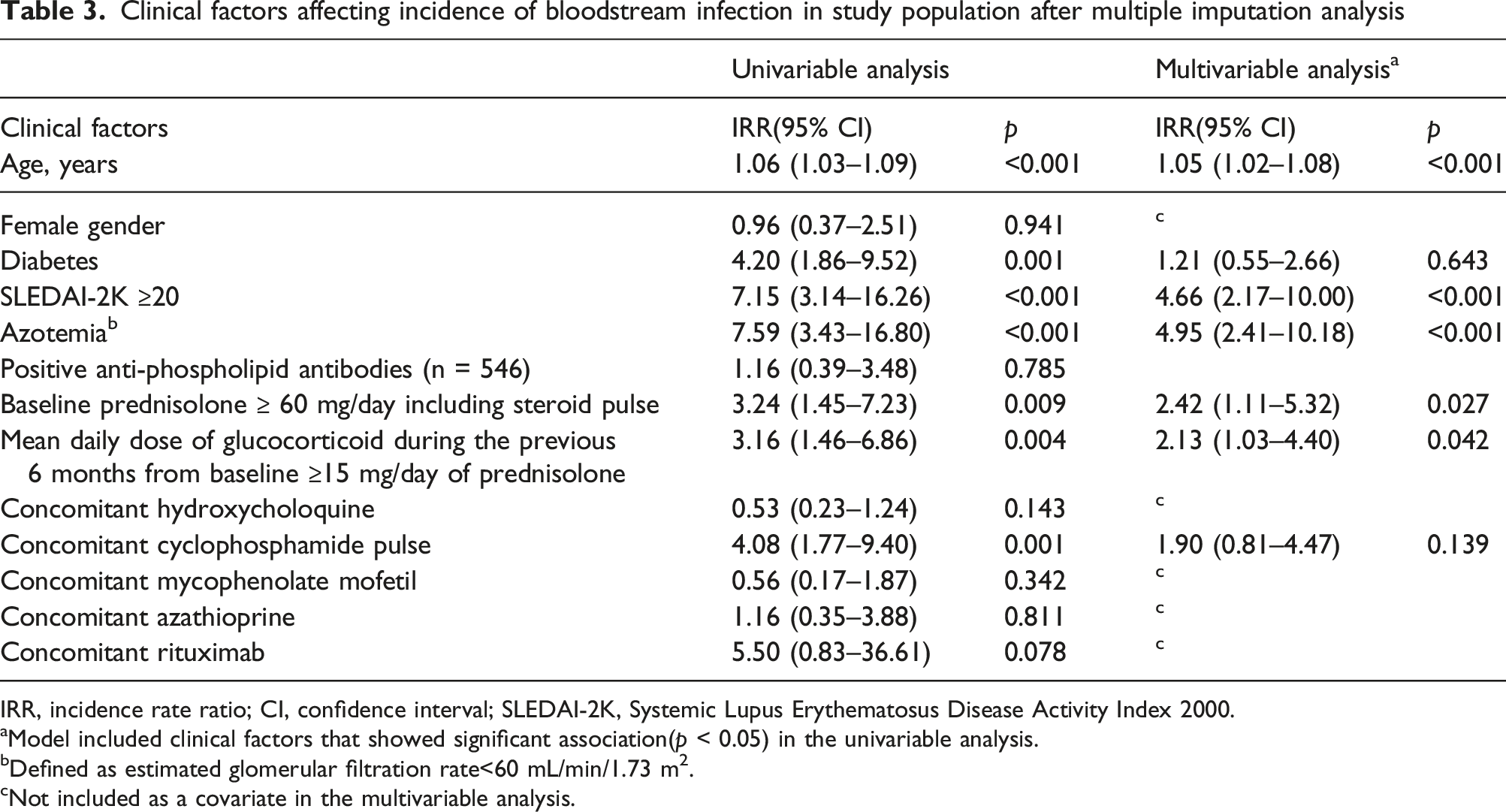
IRR, incidence rate ratio; CI, confidence interval; SLEDAI-2K, Systemic Lupus Erythematosus Disease Activity Index 2000.
aModel included clinical factors that showed significant association(p < 0.05) in the univariable analysis.
bDefined as estimated glomerular filtration rate<60 mL/min/1.73 m2.
cNot included as a covariate in the multivariable analysis.
The use of prophylactic trimethoprim-sulfamethoxazole (TMP-SMX) did not influence the BSI incidence rate in the univariable analysis. However, after adjusting the effect of the baseline glucocorticoid dose and SLEDAI-2K index, it was associated with a significantly decreased BSI risk (aIRR 0.42 (0.18–0.99)). Treatment episodes with TMP-SMX prophylaxis showed higher baseline SLEDAI-2K scores and higher baseline glucocorticoid doses than those without TMP-SMX prophylaxis (Supplementary table S3).
Sensitivity analysis
The main analysis results were compared with those of the sensitivity analyses in which (1) multiple imputations were not applied and (2) clinical factors associated with BSI were performed using the Cox proportional hazard model (Supplementary table S4 and S5). Additionally, sensitivity analysis, excluding CRBSI from the outcome, showed a consistent result (Supplementary table S6).
Discussion
BSI is an important cause of morbidity and mortality in patients with SLE receiving immunosuppressive treatment. Despite clinical importance of BSI, its actual risk during the treatment of SLE is uncertain because most previous studies included patients with various disease activities, which made it difficult to estimate the incidence of BSI during remission induction. This study showed the incidence rate of BSI in the treatment episodes of medium-to-high-dose glucocorticoids to address the clinical question.
The incidence rate of BSI in the study population was 2.78 per 100 person-years, which was significantly higher than that reported in the general population.12,13 It was also significantly higher than those previously reported for patients with SLE. For example, a large multicenter cohort study of patients with SLE from Spain showed that the incidence rate of BSI was 2.7 per 1000 person-years. Considering the observation period of this study that followed up patients who started medium-to-high dose glucocorticoid treatment for 1 year, the difference suggests that BSI frequently occurs within 1 year after intensive immunosuppressive treatment. This result is also supported by other studies showing that the infection incidence rate was highest during the early diagnosis phase.14,15
We also showed that treatment episodes with BSI were significantly associated with more frequent ICU admission and with high mortality rate. These results reinforce previous findings that lupus patients with episodes of bacteremia have poor outcome. 16 According to previous studies, the most common cause of ICU admission for patients with SLE was infection,17–19 and those who were admitted to ICU due to infection had showed substantially longer ICU stay, higher Acute Physiology and Chronic Health Evaluation (APACHE) II score and higher mortality compared with SLE with non-infectious causes. 20 Considering its deteriorating effect on treatment outcomes and prognosis of SLE, identifying risk factors for BSI during immunosuppressive treatment is essential to establish an appropriate surveillance and prophylaxis strategy against BSI in patients with SLE receiving medium-to-high dose glucocorticoid treatment. Of note, we also showed that old age and azotemia, which are conventional risk factor for infection, further increased the incidence of BSI. This result suggests that high degree of clinical suspicion and low threshold for evaluation should be required for better prognosis of the high-risk patients.
In this study, the incidence of BSI significantly increased with a higher dose of glucocorticoid use at baseline, which is comparable to previous studies.21,22 Glucocorticoids inhibit Toll-like receptor (TLR) signaling and nuclear factor-kB in the innate immune system, which play vital roles in recognizing microorganisms and initiating antimicrobial responses. 23 In addition, glucocorticoids inhibit the migration and phagocytic function of neutrophils, thus increasing their susceptibility to extracellular bacteria. Moreover, impaired skin barriers caused by glucocorticoids allow pathogen access to adjacent tissues and increase the risk of BSI.24,25 These immunosuppressive effects of glucocorticoids are known to be dose-dependent, which is consistent with our result that the incidence rate of BSI was significantly increased in the subgroup of patients who received ≥ 60 mg/day of prednisolone. Furthermore, we observed that high SLE disease activity was an independent risk factor for BSI, especially in cases of SLEDAI-2K ≥20. This result could be partially attributed to severe lupus flares requiring intensive immunosuppressive treatments. However, we found no significant correlation between SLEDAI-2K and the initial glucocorticoid dose. In addition, many studies have suggested that SLE impairs several immune responses against infection. The diminished number of T lymphocytes and T-helper cell activity correlated with higher disease activity in patients with SLE. 26 Moreover, it has been shown that there is an inverse relationship between the SLE disease activity score and complement receptor 2 expression on B cells, suggesting that disease activity worsens complement dysfunction. 27
Previous studies have shown that anti-malarial agents could lower the risk of infectious complications in patients with SLE. In a nested case–control study by Ruiz-Irastorza, et al., SLE patients receiving hydroxychloroquine showed a significantly lower rate of major infection than those without hydroxychloroquine. 28 Although the mechanism underlying anti-infection effect of hydroxychloroquine has not been fully understood, recent studies showed that alkalinization of phagolysosome by anti-malarial drugs enhances killing intracellular bacteria or fungi, which supports the clinical result. 29 Our study also showed that concomitant hydroxychloroquine treatment tended to decrease the risk of BSI. Although the effect was not statistically significant, it probably due to low rate of concomitant hydroxychloroquine treatment (36.8%) in the study population.
Interestingly, our results showed that prophylactic TMP-SMX use was associated with a lower incidence rate of BSI. Although primary prophylaxis for pneumocystis pneumonia using TMP-SMX is highly effective, its efficacy in preventing other types of infection has not been thoroughly investigated. Recently, Kronbichler et al. showed that in patients with ANCA-associated vasculitis, prophylactic TMP-SMX was associated with a lower frequency of severe infection, which aligns with our result. 30 However, the exact mechanism underlying this result is still uncertain, and sulfa drugs are known to induce flares in patients with SLE. In addition, previous studies suggested that prophylactic TMP-SMX is frequently associated with adverse drug reactions in patients with SLE.31,32 Therefore, the risk-benefit assessment of TMP-SMX to prevent infectious complications in patients with SLE should be further evaluated in future studies.
This study has several limitations. First, as this study was retrospective design, some patients had missing data for calculating the SLEDAI-2K index and the possibility of missing cases on BSI diagnosed at other hospitals exists. Although we performed multiple imputations for SLEDAI-2K score, the outcome could be significantly biased. 33 Second, the number of BSI cases in this study was relatively small; therefore, it is possible that the effects of some potential risk factors were imprecisely estimated. Finally, the effect of covariates on the outcome could be biased by unmeasured confounders such as patient’s compliance with glucocorticoid treatment. In addition, it is possible that change in glucocorticoid dose during the observation could influence on the risk for BSI.
In summary, this study showed the incidence and risk factors of BSI in patients with SLE receiving medium-to-high-dose glucocorticoids. High-dose glucocorticoids, especially prednisolone ≥ 60 mg/day and SLEDAI ≥ 20 at baseline, were the most critical risk factors. Considering the high mortality and morbidity rates of BSI, further studies to establish effective surveillance and preventive strategy for BSI in high-risk patient groups are required for better treatment outcomes.
Supplemental Material
Supplemental Material - Risk of Bloodstream Infection in Patients with Systemic Lupus Erythematosus Exposed to Prolonged Medium-to-High-Dose Glucocorticoids
Supplemental Material for Risk of Bloodstream Infection in Patients with Systemic Lupus Erythematosus Exposed to Prolonged Medium-to-High-Dose Glucocorticoids by Mi Hyeon Kim, Se Rim Choi, Jin Kyun Park, Eun Young Lee, Eun Bong Lee and Jun Won Park in Lupus.
Supplemental Material
Supplemental Material - Risk of Bloodstream Infection in Patients with Systemic Lupus Erythematosus Exposed to Prolonged Medium-to-High-Dose Glucocorticoids
Supplemental Material for Risk of Bloodstream Infection in Patients with Systemic Lupus Erythematosus Exposed to Prolonged Medium-to-High-Dose Glucocorticoids by Mi Hyeon Kim, Se Rim Choi, Jin Kyun Park, Eun Young Lee, Eun Bong Lee and Jun Won Park in Lupus.
Footnotes
Declaration of Conflicting Interests
The Authors declare that there is no conflict of interest
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: This research work was supported by the research fund of Rheumatology Research Foundation’ (RRF-2020-05)
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.