
Abstract
Since the improvement in management and the reduction of mortality caused by the disease activity, infections have represented the main cause of morbidity and mortality in systemic lupus erythematosus patients. We aimed to determine the prevalence and identify risk factors of severe infections in systemic lupus erythematosus patients. We conducted a retrospective study on 93 Tunisian lupus patients followed between 2010 and 2019. The mean age of the disease was 33.63 ± 13.76 years. Fifty-two patients had 118 infections and 16% of the infections were serious. The bivariate analysis revealed a positive correlation between the total cumulative doses of corticosteroids and the number of serious infections (p = 0.009). The multivariate study has shown that the number of flares (p = 0.03), pulmonary manifestations (p = 0.01), pleuritis (p = 0.001), and the total cumulative dose of corticosteroids (p = 0.04) were independent risk factors of severe infections (p < 0.001). The use of antimalarials exerted a protective effect from severe infection [OR = 0.19 (95% CI 0.03-0.9)] p < 0.03.
Introduction
Over the last decades, we have observed an improvement of the systemic lupus erythematosus (SLE) patients’ survival rates due to early diagnosis and better control of organ damage. It has increased from 50% in 4 years 1 to 90% in 10 years. 2 Alternative causes of morbidity and mortality has risen, including infection as a leading cause. Thirty to fifty percent of SLE patients have infections during the course of their disease.3–8 Infection represents the main cause of morbidity9–11 and mortality 12 in patients with SLE. A combination of external factors and underlying immune dysregulation increase the susceptibility to infections. In this study of a sample of Tunisian lupus patients followed in the military hospital of Tunis, we aimed to determine the prevalence of serious infections and investigate the risk factors of these infections.
Methods
Patients’ selection
We conducted a retrospective study on Tunisian lupus patients followed between 2010 and 2019. All fulfilled at least four of the 1997 revised criteria for the classification of systemic lupus erythematosus published by the American College of Rheumatology. We included 93 and divided them to three groups: the Group 1 includes patients who had severe infections, the Group 2 includes patients who had non-severe infections and the Group 3 includes patients who haven’t developed infection during the follow-up period. We excluded patients with incomplete records.
Definition of infection
The diagnosis of a bacterial infection was certain if an organism had been identified on microscopy or culture. If no germ was identified, it was probable based on clinical, biological, radiological arguments or a response to antibiotic treatment. Invasive fungal infection (IFI) was diagnosed based on “Revised definitions of Invasive Fungal Disease from European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group.” 13 Acute viral infections were diagnosed based on multiple arguments (clinical features, identification of specific anti-viral IgM antibodies and subsequent seroconversion with detection of specific IgG antibodies, quantification of virus molecular components and nucleic acid amplification by polymerase chain reaction, imaging and non-response to immunosuppressive treatment). An infectious episode is considered severe when it is complicated by organ failure, required a stay in intensive care, involved several germs or several sites simultaneously. Severe manifestations of lupus are cardiac, neuropsychiatric, renal, and hematological manifestations.
Data collection
For each patient, we collected demographic, clinical, para-clinical, therapeutic data and for each infection we specified the date, type, location, germ, if the patient was in flare or in remission, prior treatments (immunosuppressant, biotherapy, etoposide, intravenous immunoglobulins, and plasma exchanges) and the cumulative dose of these treatments, diagnostic examinations, management, and evolution.
Statistical analysis
Data were analyzed using SPSS 21. Numerical variables were expressed as mean (mean) with standard deviation (SD) in case of normal distribution, and as median with interquartile range (IQR) in case of abnormal distribution. The comparison of the means over several independent series (>2) was carried out by means of Snedecor’s F test of parametric analysis of variance (one-way ANOVA) and in the case of small numbers by the Kruskall–Wallis H test. The comparison of percentages over several independent series (≥2) was carried out using Pearson’s chi-square test, and in case of non-validity by Fisher’s two-tailed exact test. The variables which had reached the threshold of significance during the bivariate study were introduced into a multivariate model (multinominal logistic regression) with serious infection as dependent variables. In all statistical tests, the significance level was set at 0.05.
Results
Clinical features and treatments of patients with severe infections.
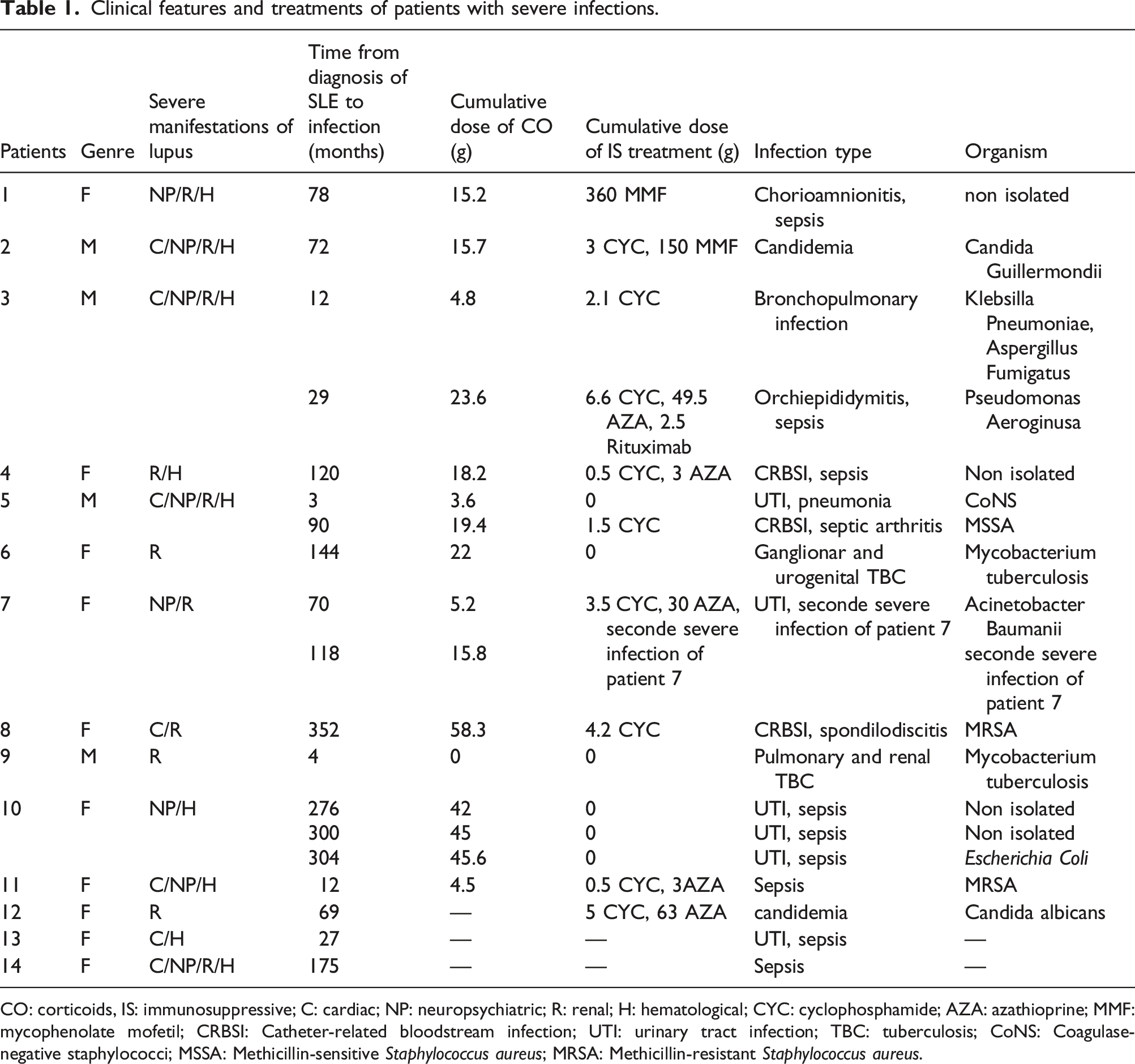
CO: corticoids, IS: immunosuppressive; C: cardiac; NP: neuropsychiatric; R: renal; H: hematological; CYC: cyclophosphamide; AZA: azathioprine; MMF: mycophenolate mofetil; CRBSI: Catheter-related bloodstream infection; UTI: urinary tract infection; TBC: tuberculosis; CoNS: Coagulase-negative staphylococci; MSSA: Methicillin-sensitive Staphylococcus aureus; MRSA: Methicillin-resistant Staphylococcus aureus.
Regarding etiologic agents, there was a clear predominance of bacterial agents (52.6%) with 37% corresponding to unknown causes. Two patients had tuberculosis. The first had pulmonary and renal localizations, whereas the second had ganglionar and urogenital tuberculosis. The predominant localization for serious infection was the circulatory stream (73.7%). No deaths were recorded among this series of SLE patients.
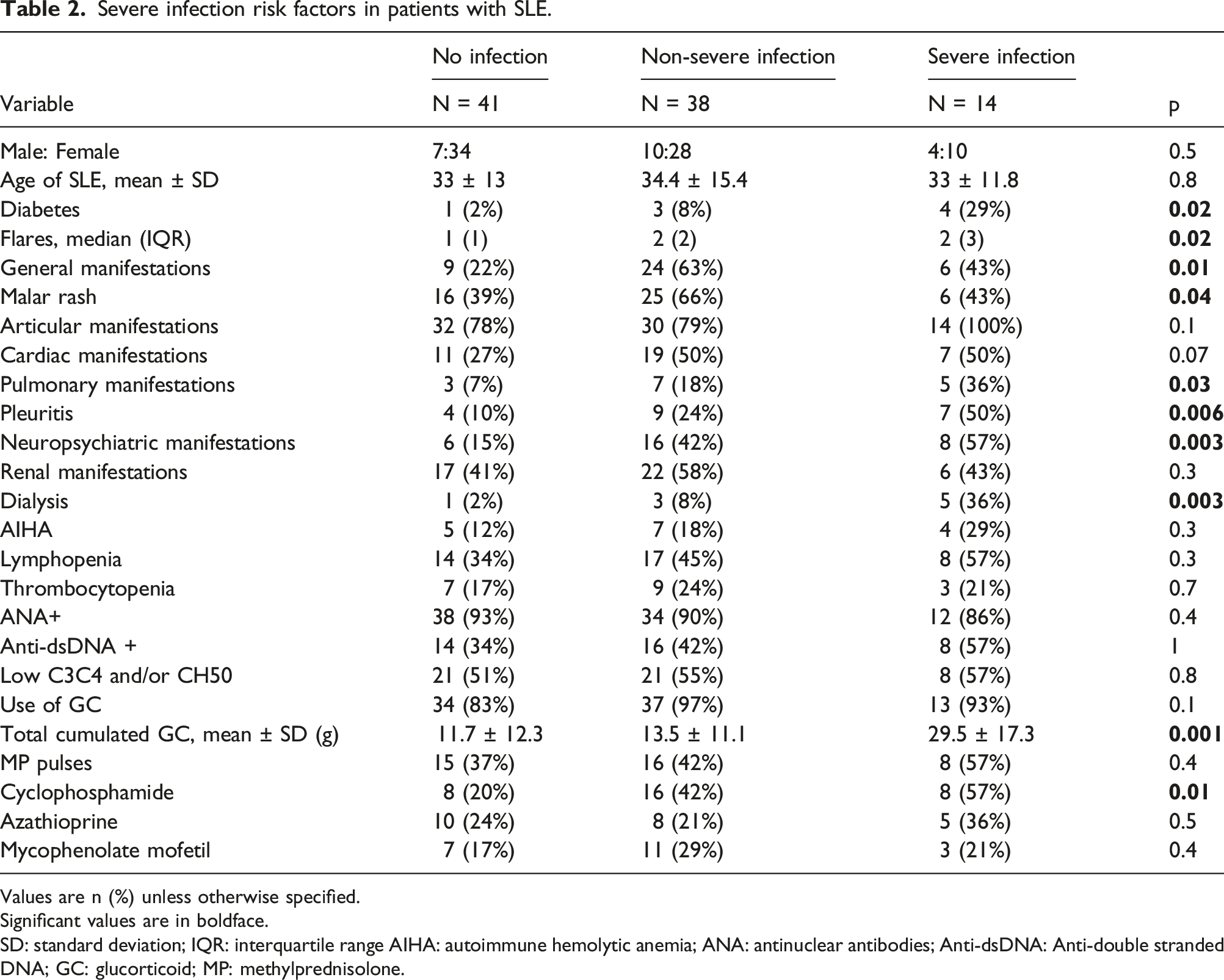
The univariate and bivariate analysis have shown the presence of multiple risk factors of severe infection. Patients with history of diabetes were prone to develop severe infections. Number of flares, general manifestations, malar rash, pulmonary manifestations, pleuritis, neuropsychiatric manifestations, dialysis, total cumulated dose of GC (Figure 1), and use of cyclophosphamide were risk factors of severe infection (Table 2). Furthermore, we observed a positive correlation between the total cumulated dose of GC and the number of serious infections (p = 0.009). The multinominal logistic regression analysis reduced the predictors of severe infection. Only the number of flares (p = 0.03), pulmonary manifestations (=0.01), pleuritis (p = 0.001), and the total cumulated dose of corticosteroids (p = 0.004) were independent risk factors of severe infections (p < 0.001). The use of antimalarials exerted a protective effect from severe infections [OR = 0.19 (95% CI 0.03-0.9)] p = 0.03. Means of total cumulated glucocorticoid doses in SLE patients with no infection, non-severe infection, and severe infection. Severe infection risk factors in patients with SLE. Values are n (%) unless otherwise specified. Significant values are in boldface. SD: standard deviation; IQR: interquartile range AIHA: autoimmune hemolytic anemia; ANA: antinuclear antibodies; Anti-dsDNA: Anti-double stranded DNA; GC: glucorticoid; MP: methylprednisolone.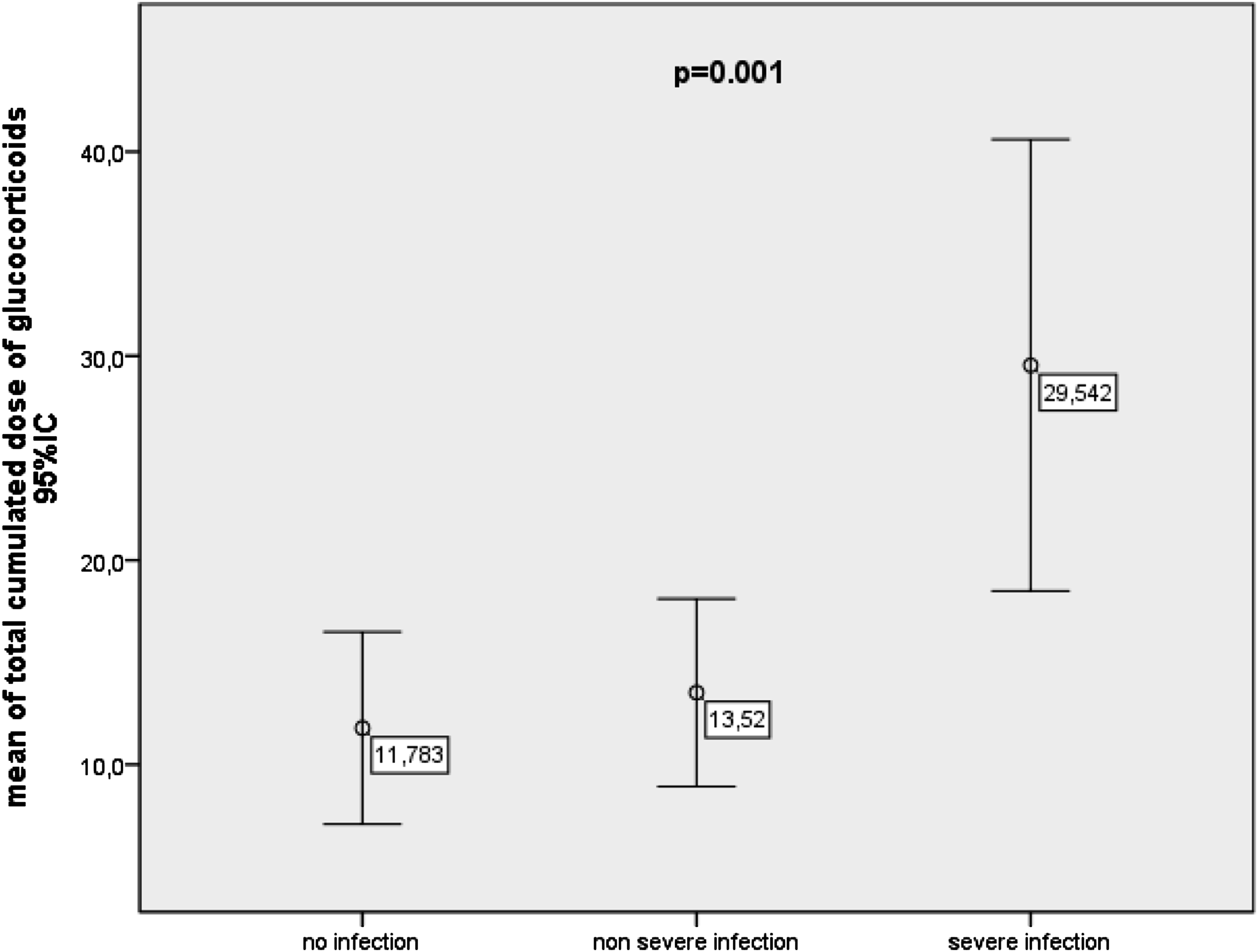
Discussion
The prevalence of serious infection in our study was similar to previous reports.14–16 Differences can be explained by the selection of patients, the health care system and the size of the cohort. Our rates might be underestimating considering more strict selection criteria for serious episodes. Most studies showed that respiratory infection was the most common in serious infections.14–16 Among our patients, the most frequent localization was bloodstream. Bacterial agents were the leading cause of severe infections,16,17 so was the case in our series.
Hospitalization rates for serious infections was 12 times higher than among patients without SLE. 18 A Canadian study showed that 13.8% of infections required a stay in an intensive care unit, resulting in a longer hospital stay. 19
Patients with severe infection suffer more severe disease. 15 This is an expected finding considering immunological disorders predisposing SLE patients to infections. 20 The number of flares was an independent risk factor of severe infections in our study. Other studies showed that lung involvement was an independent risk factor as it’s the case with our results. 17 The association of infection with immunoseppressive treatment is well known. 21 According to a Spanish study, any use of GC ≥10 mg increases the risk of severe infection. 15 And in a British series, in one-third of infective episodes, the immunosuppressant has been commenced or increased within 6 months prior to the admission. 14 The immunosuppressive treatment effect on infection has also been proven in our multivariate analysis and a positive correlation was found between the total cumulative dose of GC and the number of serious infections.
The protective effect of antimalarials has been proven. 17 Current or past use of antimalarials were protective factors and a decrease in the incidence ratio of serious infections was found when analyzing quintiles of time of exposure to antimalarials. 15
Different strategies can be applied in order to reduce the risk of infection in SLE patient like monitoring, screening, and vaccination. 22 Serological screening for hepatitis B before immunosuppressive treatments is recommended in lupus patients to avoid viral reactivation. 23 HPV vaccine may be prescribed in lupus patients to avoid the increased incidence of anogenital warts and cervical intraepithelial dysplasia or carcinoma associated with high-risk viral genotypes. 24 Annual cervical cytology is recommended in immunocompromised patients. 25 Influenza vaccination is well tolerated and provides moderate protection for lupus patients. It reduces morbidity and mortality according to a large Taiwanese study. 26 The pneumococcal vaccine is recommended at any stage of the disease. 25
The limitations of this study must be acknowledged. Various variables could not be collected considering the retrospective nature of the study, such as SLEDAI (systemic lupus erythematosus disease activity index), SKI (severity katz index), and SDI (slicc damage index). Further multicentric studies should be performed for better preventive strategy.
Conclusion
The rates of severe infections in our study are similar to literature. These rates might underestimate the prevalence of severe infection given the strict criteria of severe infection. They result in longer hospitalizations and stay in intensive care units increasing health related costs associated to SLE. Better disease management and wise use of immunosuppressive treatments is recommended. Regular surveillance for infections particularly in patients with severe disease, pulmonary manifestations or under high dose of corticosteroids may help to prevent or early diagnose infections. Most non-live vaccines are immunogenic and safe in patients with SLE. Some are even recommended like influenza and pneumococcus.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.