
Abstract
Objectives
To evaluate the prevalence of self-perceived depression and anxiety in patients with systemic lupus erythematosus (SLE) and to explore associated factors.
Methods
Cross-sectional study of unselected patients with SLE (ACR-97 criteria) and controls with chronic inflammatory rheumatic diseases. Both completed the Hospital Anxiety and Depression Scale (HADS). Demographic and clinical characteristics, comorbidity, and treatments were collected, and a multivariate analysis was performed to explore factors associated with depression and anxiety in SLE.
Results
The study population comprised 172 patients and 215 controls. Women accounted for 93% of the patients with SLE. Fibromyalgia was recorded in 12.8% and a history of depression in 17%. According to HADS, 37.2% fulfilled the diagnostic criteria for depression and 58.7% those for anxiety; prevalence was similar in the controls (32.6% and 55.1%, respectively). Up to a third of patients with self-perceived depression were not receiving antidepressants. There was no concordance between a previous history of depression and current depression. In the multivariate model, current depression was associated with single marital status (OR 2.69; 95% CI: 1.17–6.42; p = .022), fibromyalgia (7.69; 2.35–30.72; p = .001), smoking (3.12; 1.24–8.07; p = .016), severity of SLE (0.76; 0.6–0.94; p = .016), and organ damage (1.27; 1.01–1.61; p = .042). Current anxiety was only associated with fibromyalgia (3.97; 1.21–17.98; p = .036).
Conclusions
Depression and anxiety are most likely underdiagnosed in SLE. Prevalence appears to be similar to that of other chronic inflammatory rheumatic diseases. Anxiety is associated with fibromyalgia, while depression is also associated with single marital status, smoking, organ damage, and severity of SLE.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune rheumatic disease that is more common in women. It is characterized by multiorgan involvement, and the central nervous system is often affected.1–4 In 1999, the American College of Rheumatology (ACR) proposed a nomenclature for the 19 neuropsychiatric syndromes in SLE, which are known collectively as neuropsychiatric SLE. 5 According to this classification, the prevalence of neuropsychiatric SLE reported in the literature ranges between 14% and 89% of all SLE patients.3,6 Neuropsychiatric symptoms often precede other clinical manifestations.7–9 The most common neuropsychiatric manifestations of SLE are depression and anxiety. A recent review shows a prevalence that varies from 29.9% to 40.3% and from 19.2% to 32.9%, respectively.7,8 Depression is more prevalent in patients with chronic diseases, and in patients with SLE, it has been reported to be twice that of the general population.8,9 However, the clinical and psychobiological nature of the relationship between depression and SLE is poorly understood.
Recently, holistic management of patients with SLE by the rheumatologist has been advocated, with emphasis on the need to address aspects such as mental health. Anxiety and depression have been shown to have wide-ranging adverse clinical and socioeconomic impacts, including increased cardiovascular disease,10,11 suicide,12,13 poor adherence to treatment, 14 impaired work capacity, 15 and increased utilization of health services. 14 Furthermore, according to data from the Spanish multicenter register of SLE (RELESSER), depression has been independently associated with mortality in this disease. 16 Therefore, depression and anxiety should be relevant targets of interventions aimed at improving subjective health and quality of life among individuals with SLE.
Depression and anxiety are common in SLE although their prevalence in low-disease-activity, low-organ-damage cohorts, and associated factors have received less attention. Similarly, it is not known whether these affective disorders are more common in SLE than in other chronic inflammatory rheumatic diseases, which could shed light on whether or not lupus itself is a cause of depression. The objectives of this cross-sectional study were to evaluate the prevalence of self-perceived depression and anxiety in patients with SLE, using a validated questionary, to compare the findings with those of a control group with other chronic inflammatory rheumatic diseases and exploring associated factors.
Materials and methods
Patients
Ours was a case-control, cross-sectional study carried out by the Rheumatology Service in collaboration with the Psychiatry Department of Doctor Negrín University Hospital in Gran Canaria, Spain. Unselected and agreed patients were consecutively recruited from a specialist SLE clinic between June 2019 and June 2021. Diagnosis was based on the 1997 criteria of the American College of Rheumatology. All those who agreed to participate in the study were included. In parallel, patients with chronic inflammatory disease (rheumatoid arthritis, ankylosing spondylitis, or psoriatic arthritis) belonging to the same age group and sex (1:1 assignment) were consecutively enrolled as controls.
Evaluation and definitions
Both groups completed the Hospital Anxiety and Depression Scale (HADS), a validated self-administered questionnaire that was applied to explore the presence of anxiety and depression at the time of the study. 17 HADS is a valid screening instrument for the detection of comorbid mental disorders (such as depression) in patients with chronic somatic diseases and performs better than other questionnaires. 18 A cut-off point >8 was used to define the presence of anxiety (“current anxiety” from here onwards) or depression (“current depression” from here onwards); this has been considered highly predictive of a medical diagnosis of depression or anxiety. 19 Demographic data and disease duration were recorded for both groups. In the SLE patient group, we also collected the following data: socioeconomic status (years of education, GRAFFAR scale, 20 and marital status), and clinical SLE-related characteristics, namely, disease activity (SLEDAI-2k), organ damage (SLICC/ACR/Damage Index) (SDI), severity (Katz index) (KSI), 21 comorbidity (Charlson index, smoking, menopause, previous diagnosis of depression, and vitamin D deficiency) based on through review of medical records, and treatments for SLE.
Statistical analysis
The normality of the data was determined using the Kolmogorov-Smirnov test. The t test was used to compare numerical variables in both groups, and the Fisher exact test was used for categorical variables. Logistic regression was performed to assess the relationship between dichotomous variables; the forward-backward technique was applied to select the optimal model. To check the goodness of fit of the model, the area under the ROC curve was calculated. The variance inflation factor (VIF) statistic was used to test for possible multicollinearity of the variables. The propensity score matching technique was used to eventually select the same number of controls as cases adjusted for sex and duration of the disease. p-values <0.05 were considered significant. The statistical program used was R Core Team 2021, version 4.1.0.
Results
A total of 172 cases (SLE) and 215 controls were included; most participants in the control group had rheumatoid arthritis (60.8%), followed by psoriatic arthritis (23.8%) and ankylosing spondylitis (15.3%). Only 1 patient refused to participate in the study.
Demographics and baseline characteristics SLE patients.
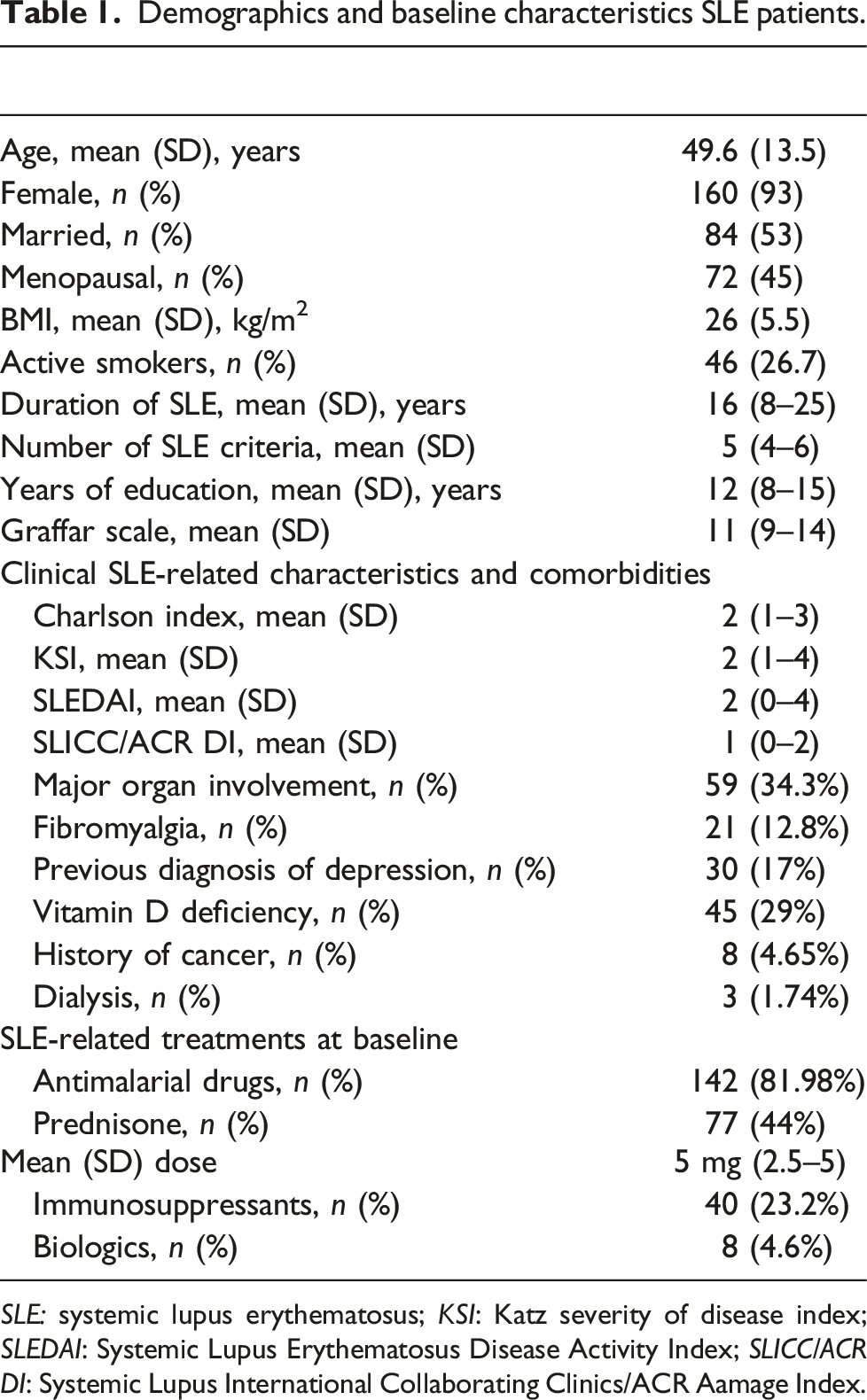
SLE: systemic lupus erythematosus; KSI: Katz severity of disease index; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; SLICC/ACR DI: Systemic Lupus International Collaborating Clinics/ACR Aamage Index.
After matching, the mean HADS score for depression and anxiety was lower than for cases (5.24 ± 4.6 and 8.13 ± 4.87, respectively). However, according to the predefined HADS cut-off point, 64 of the 172 SLE patients (37.2%) had depression (current depression) and 101 (58.7%) had anxiety (current anxiety). The figures for patients in the control group were 55.1% for current anxiety and 32.6% for current depression. Interestingly, no significant differences were observed between cases and controls regarding the frequency of current anxiety (p = .246) or current depression (p = .4).
Up to 29.7% of patients with SLE and current depression (according to the HADS score) were not receiving antidepressants. There was no concordance between the previous diagnosis of depression and current depression (kappa 0.10; 95% CI: 0.07–0.26; p = .26).
Bivariate logistic regression analysis of current depression in patients with SLE.
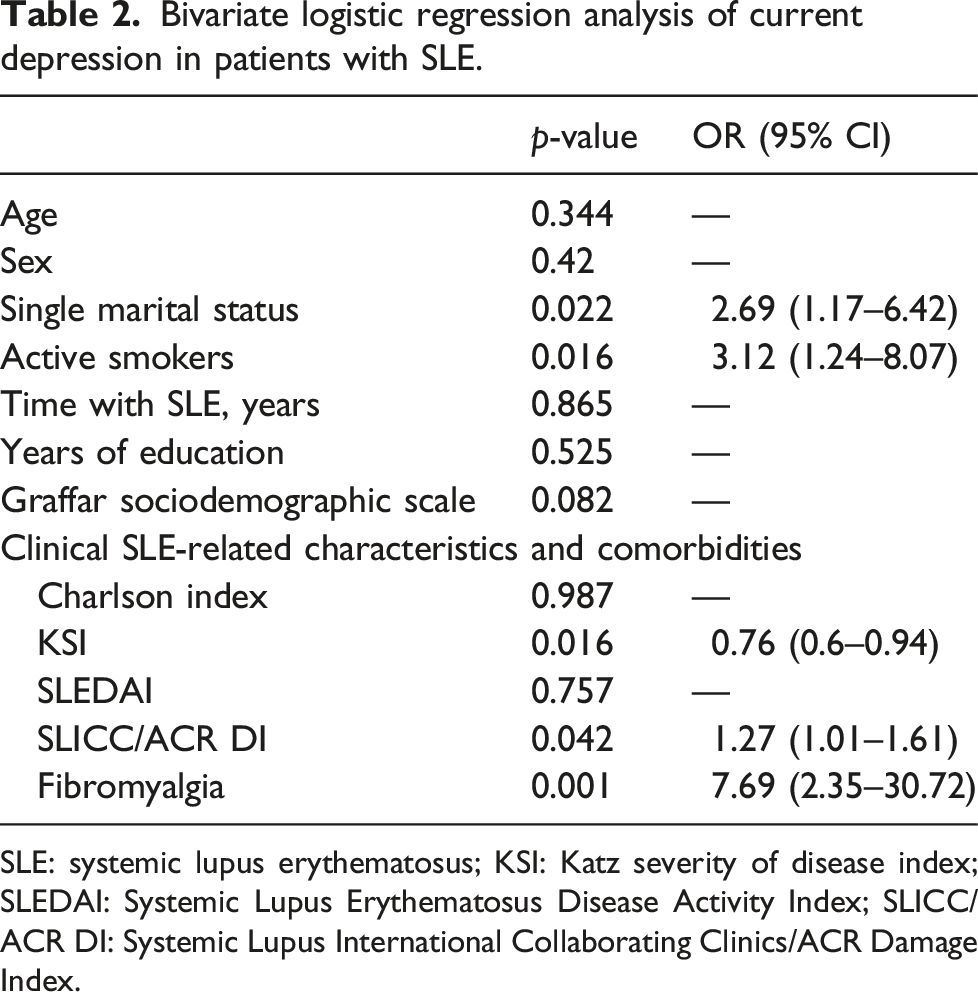
SLE: systemic lupus erythematosus; KSI: Katz severity of disease index; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; SLICC/ACR DI: Systemic Lupus International Collaborating Clinics/ACR Damage Index.
Bivariate logistic regression analysis of current anxiety in patients with SLE.
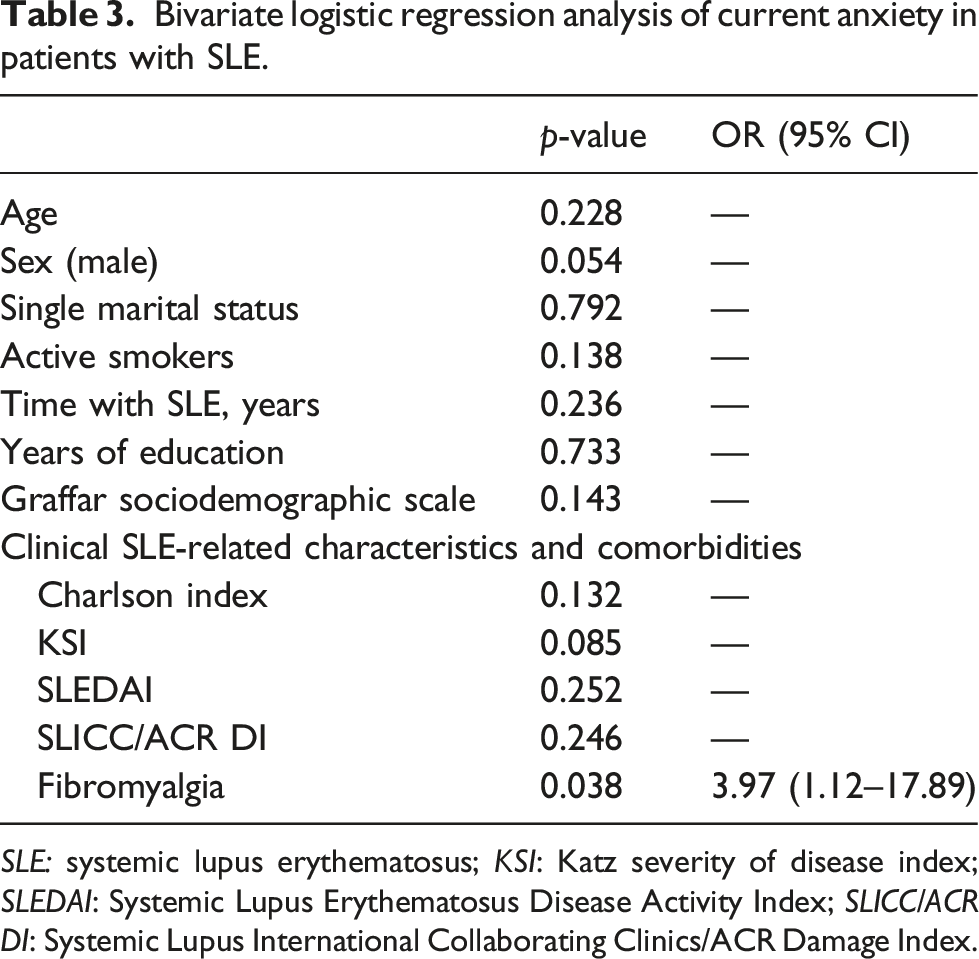
SLE: systemic lupus erythematosus; KSI: Katz severity of disease index; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; SLICC/ACR DI: Systemic Lupus International Collaborating Clinics/ACR Damage Index.
Discussion
Our study shows that self-perceived depression and anxiety are prevalent in patients with SLE (37.2% and 58.7%, respectively). However, these values did not differ from those recorded for controls with chronic inflammatory rheumatic diseases. Depression was associated with single marital status, smoking, disease severity, and disease-associated organic damage. The presence of fibromyalgia increased the risk of depression up to 7 times, while anxiety was related only to the presence of fibromyalgia, which increased the risk up to almost 4 times.
As pointed out previously, psychiatric manifestations are highly prevalent in patients with SLE.22,23 However, anxiety and depression can be underdiagnosed, mainly owing to the shortage of time available for each patient in medical consultations. 17 Depression is perhaps the best known and most widely studied psychiatric manifestation in SLE. A recent study suggests that the prevalence of depressive disorders in SLE is greater than 39%, 24 consistent with our findings. The prevalence of depression clearly depends on the method used to estimate its presence. Regarding self-applied questionnaires, HADS revealed depression rates 2-4 times higher than with the Mini International Neuropsychiatric Interview (MINI), 17 while for anxiety, similarities in diagnostic performance were observed between HADS and MINI. One study found that the 30-days and lifetime prevalence of anxiety in patients with SLE was 46.5% and 52.1%, respectively. 25 In a meta-analysis, 19 the prevalence of anxiety was 40% according to HADS using a threshold of 8. A systematic review and meta-analysis 19 of 59 studies involving 10,828 patients with SLE revealed that few studies use the gold standard in clinical interviews (Diagnostic and Statistical Manual and/or International Classification of Diseases) and reported major depression and anxiety, respectively, in 24% and 37% of patients with SLE, that is, a somewhat lower prevalence than found in our study. Most of the studies using screening tools found significant depression in 30% using the HADS with a threshold of eight or more, that is, the cut-off point used in our study. Differences in the level of damage or severity of SLE and/or disease duration could account for discrepancies in prevalence. Another plausible explanation for the diversity of results is treatment with prednisone, which can induce depression. 26 Although the mean dose of prednisone in our study was lower than reported elsewhere23,27 (5 mg vs 18.2 mg and 14.5 mg), we found no association between corticosteroids and anxiety or depression.
The estimated prevalence of anxiety in patients with SLE has been reported to be higher than in the general population 28 and in other rheumatic and connective tissue diseases. 29 However, after matching the groups for age, sex, and disease duration, we did not find differences with respect to patients with various other chronic inflammatory joint diseases. Therefore, we might hypothesize that specific factors associated with SLE itself probably do not cause depression or anxiety; instead, these affective disorders would be a consequence of a chronic immune-mediated inflammatory disease.
A relationship between depression and anxiety and age has been reported in patients with chronic diseases, for example, in cancer, 30 as well as in autoimmune systemic rheumatic diseases such as systemic sclerosis. 31 In contrast to results reported elsewhere showing that young patients with SLE had a higher risk of major depression,23,32 we found no association with age.
While a previous study showed that disease activity in patients with SLE was associated with the severity of depression (measured using the Montgomery-Asberg Depression Rating Scale), 27 we and other authors23,29 found no association with ongoing activity of SLE. We did observe, however, that depression was related more to the cumulative severity of the disease and organ damage. While the low degree of activity in our cohort at the time of the study may have led us to underestimate its impact on depression, the point is that the prevalence of depression and anxiety was high in our study population.
Smoking is a well-known major risk factor for cardiovascular diseases, cancer, and chronic lung disease, yet less is known about its impact on neuropsychiatric diseases. 33 In our study, being a smoker increased the risk of depression by up to 3 times, a finding not previously reported in SLE. There is strong evidence from epidemiology and experimental studies indicating that smoking may increase the risk of various neuropsychiatric diseases, such as depression and anxiety disorder. 34 The neuropsychiatric effects of smoking could be explained by the increase in inflammatory and oxidative stress, for example, in the reduced activity of the antioxidant enzyme paraoxonase, which is associated with smoking. 35
Our findings are subject to a series of limitations. First, the study of the associated factors was retrospective, thus placing objective restrictions on the amount of data that can be inferred and preventing us from establishing causal relationships. In addition, given that ours was a study of self-perceived affective disorders, with no confirmatory psychiatric diagnosis, the prevalence obtained can only be considered an estimate. On the other hand, taking into account the numeric differences between SLE and controls in the prevalence of anxiety (58.7% vs 55.1%, respectively) and depression (37.2% vs 32.6%, respectively), perhaps our study did not reach the necessary statistical power to show true differences between the groups. Finally, since there is a high prevalence of SLE in women, almost all the participants were women. Caution should be exercised when extrapolating these data to men with SLE.
It is also worth considering the discrepancy between a previous history of depression and self-perceived depression found in our study, suggesting under-diagnosis of this condition. Furthermore, many patients with self-perceived depression were not receiving antidepressants. Given the high prevalence of anxiety and depression, under-diagnosis, and impact on health outcomes and quality of life, every effort should be made to develop efficient tools to facilitate diagnosis and thus enable prompt psychiatric evaluation and appropriate treatment.
In summary, self-perceived depression and anxiety are very prevalent in patients with SLE, even in low-disease-activity, low-organ-damage cohorts. However, the prevalence seems to be no greater than for other immune-mediated inflammatory rheumatic diseases. A significant percentage of patients with SLE and depression are underdiagnosed and do not receive adequate psychiatric treatment. Both anxiety and depression are associated with fibromyalgia, while depression is also associated with single marital status, smoking, organ damage, and severity of SLE.
Footnotes
Acknowledgments
The authors thank the Spanish Foundation of Rheumatology (FERBT2022) for providing medical writing/editorial assistance during the preparation of the manuscript.
Author contributions
All authors contributed towards the study design, analysis and development of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study involves human participants and was approved by Las Palmas Clinic Research Ethics Committee (Hospital Universitario de Gran Canaria Dr Negrín). Participants gave informed consent to participate in the study.