
Abstract
Objectives
Medication access and adherence play key roles in determining patient outcomes. We investigated whether cost-related non-adherence (CRNA) to prescription medications was associated with worse patient-reported outcomes in a population-based systemic lupus erythematosus (SLE) cohort.
Methods
Sociodemographic and prescription data were collected by structured interviews in 2014–2015 from patients meeting SLE criteria in the established Michigan Lupus Epidemiology & Surveillance (MILES) Cohort. We examined the associations between CRNA and potential confounders such as sociodemographics and health insurance coverage, and outcome measures of SLE activity and damage using multivariable linear regression.
Results
462 SLE participants completed the study visit: 430 (93.1%) female, 208 (45%) Black, and mean age 53.3 years. 100 (21.6%) participants with SLE reported CRNA in the preceding 12 months. After adjusting for covariates, CRNA was associated with both higher levels of current SLE disease activity [SLAQ: β coeff 2.7 (95% CI 1.3, 4.1), p < 0.001] and damage [LDIQ β coeff 1.4 (95% CI 0.5, 2.4), p = 0.003]. Race, health insurance status, and fulfilling Fibromyalgia (FM) Survey Criteria were independently associated with both higher (worse) SLAQ and LDIQ scores; female sex was further associated with higher SLAQ scores.
Conclusion
Patients with SLE who reported CRNA in the previous 12 months had significantly worse self-reported current disease activity and damage scores compared to those not reporting CRNA. Raising awareness and addressing barriers or concerns related to financial implications and accessibility issues in care plans may help to improve these outcomes.
Keywords
Introduction
Systemic lupus erythematosus is a multi-organ systemic autoimmune disease disproportionately affecting women and minorities and can have debilitating outcomes if left untreated.1,2 Advances in SLE medical management have resulted in improved 4-year survival from 51% in the 1950s 3 to >90% in recent years.4–6 However, out-of-pocket costs for prescriptions may limit their accessibility and decrease the likelihood that patients initiate or maintain therapy. 7
Cost-related non-adherence (CRNA) includes “stretching” medication to save money, such as by skipping doses, taking lower doses than prescribed, or delayed filling of prescriptions. Based on a cross-national study of adults aged 55 and older in 11 high-income countries, the United States had the highest prevalence of self-reported CRNA (16.8%), which was over twice as high as the country with the second highest prevalence, and 3.5 times or higher than the remainder of countries included. 8 This occurs in the context of the United States having comparatively high per capita drug spending and out-of-pocket spending (e.g., cost sharing or direct payments due to un- or under-insurance) despite similar drug utilization as other countries.9,10 Such trends highlight the potential for structural factors in healthcare systems and policies to influence rates of CRNA across populations.
Studies on the consequences of non-adherence related to cost in rheumatologic diseases are limited, and in SLE are sparse. Research among Medicare beneficiaries aged 65 years and older has shown that patients reporting CRNA were more likely to perceive their overall health as poor and reported worsening hypertension, heart disease, arthritis, and higher rates of hospitalization. 11 We previously documented that one in five adults with SLE in southeastern Michigan reported CRNA within the preceding 12 months, which was twice the rate of general-population controls of similar sociodemographics in the same region; CRNA in SLE was significantly associated with lower income, not having private insurance, and non-White race. 12 Poor medication adherence in SLE is associated with worse outcomes in both patients with renal and non-renal lupus,13–16 including increased emergent hospitalizations. 17 A growing literature addressing adherence specifically to hydroxychloroquine in SLE, utilizing objective measures such as drug dispensing data or therapeutic drug monitoring (with blood levels) for this commonly prescribed SLE treatment, has documented a large scope of sub-optimal or non-adherence and association with outcomes such as higher acute care utilization and SLE activity.18–22 Recent studies have highlighted contextual factors 21 and “personal reasons” 22 as being associated with non-adherence, but have not concentrated on cost-related factors.
We performed this study to examine whether prescription non-adherence attributed to cost-related reasons is associated with SLE activity and damage in the population-based Michigan Lupus Epidemiology & Surveillance (MILES) Cohort.
Methods
The MILES Cohort is a population-based cohort of adults with SLE from southeastern Michigan. The precursor to the MILES Cohort was the MILES Surveillance Registry, one of the National US Lupus Registries supported by the Centers for Disease Control and Prevention (CDC), described elsewhere.1,23 In brief, the MILES Registry included residents of Wayne or Washtenaw Counties in Michigan during 2002–2005, with a new or existing diagnosis of SLE during this calendar period. The two counties comprising the source population for the Registry encompass the cities of Detroit and Ann Arbor, and a population of approximately 2.4 million persons (roughly 25% of the Michigan population).
The Institutional Review Boards of the University of Michigan and Michigan Department of Health and Human Services provided ethics approval; cohort participants signed written informed consent.
Data collection
This study utilized data from structured interviews and validated questionnaires collected at baseline cohort visits, from February 2014 to September 2015.
Cost-related non-adherence
Questions related to prescription medication access within the preceding 12 months were modeled on items in the 2014 US National Health Interview Survey (NHIS) for adults 24 (see Supplementary Material). “Cost-related non-adherence” was defined as participant report of at least one of the following practices in the preceding 12 months to save money: skipping medication doses, taking less medicine, or delay in filling a prescription.
Patient-reported outcomes
The Systemic Lupus Activity Questionnaire (SLAQ) 25 is a validated tool for epidemiologic studies to assess patient-reported SLE disease activity over the past 3 months, and not intended for clinical decision-making. It consists of 24 items related to symptoms (range: 0–47), with higher scores indicating greater lupus disease activity. The Lupus Damage Index Questionnaire (LDIQ) 26 is a validated tool to assess self-reported organ damage related to SLE or its treatment (range: 0–22); higher scores indicate higher cumulative damage.
The Fibromyalgia (FM) Survey Criteria were used to evaluate the likelihood that FM criteria would be present. A combination of the Widespread Pain Index (WPI) (range: 0–19) and the Symptom Severity (SS) scale (range: 0–12) are used to determine FM criteria status. FM criteria positive could be either (1) WPI ≥7 and SS ≥5 or (2) WPI 3–6 and SS ≥9; all others were considered negative. Symptoms had to be present for at least 3 months in the absence of another condition that would explain the pain. 27
Depression and anxiety were measured using the corresponding PROMIS Short Form v1.0 measures. The 8-item static forms were used in this study. For both measures, higher scores indicate worse depressive or anxiety symptoms.28,29
Other variables
Sociodemographic data, including race/ethnicity, were based on self-report. Income was considered household pre-tax income in the prior year. Health insurance was based on coverage in the preceding 12 months; for participants reporting both private and public (e.g., Medicaid) coverage, insurance was classified as private for this analysis.
Statistical analysis
Two-sample t tests or Pearson’s chi-squared tests were used for comparing continuous or categorical variables, respectively. Linear regression was used to model the association between the variables and outcomes of interest. Multivariable models adjusted for 10 covariates determined to be potential confounders a priori: sociodemographics (age, sex, self-identified race, health insurance, education, income) and clinical characteristics (PROMIS-Depression score, PROMIS-Anxiety score, fulfillment of FM survey criteria, SLE duration). Results from multivariable models are reported as β coefficients with 95% confidence intervals (CIs). Data management was performed using REDCap electronic data capture tools hosted at the University of Michigan. 30 Statistical analyses were performed using Stata 15 software (StataCorp, College Station, TX).
Results
Baseline characteristics of study participants with SLE, according to cost-related non-adherence–MILES Cohort, 2014–2015.
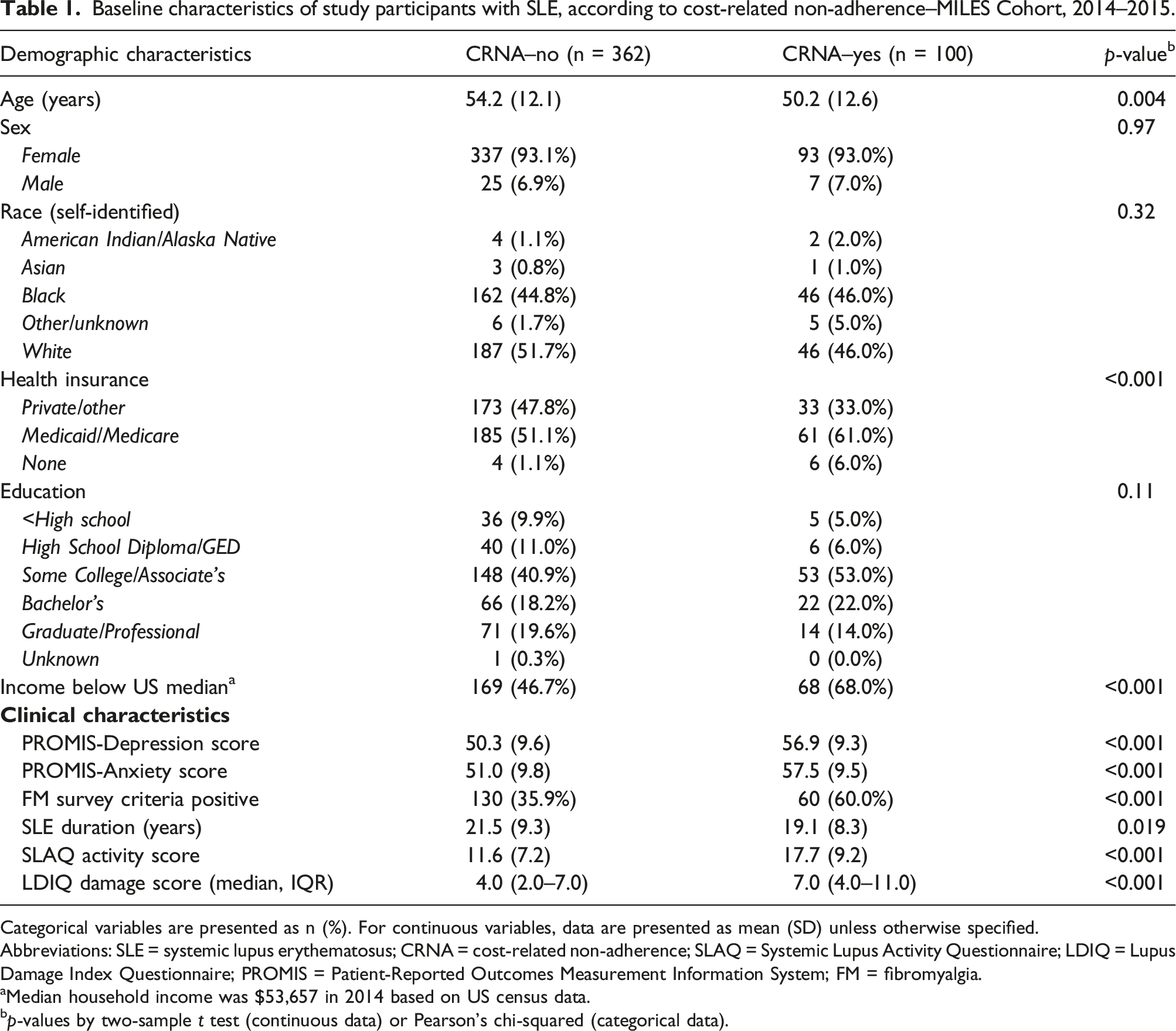
Categorical variables are presented as n (%). For continuous variables, data are presented as mean (SD) unless otherwise specified.
Abbreviations: SLE = systemic lupus erythematosus; CRNA = cost-related non-adherence; SLAQ = Systemic Lupus Activity Questionnaire; LDIQ = Lupus Damage Index Questionnaire; PROMIS = Patient-Reported Outcomes Measurement Information System; FM = fibromyalgia.
aMedian household income was $53,657 in 2014 based on US census data.
bp-values by two-sample t test (continuous data) or Pearson’s chi-squared (categorical data).
Cost-related non-adherence and patient-reported SLE outcomes
Prescription access, cost-related non-adherence, and participant strategies used to reduce prescription drug costs.
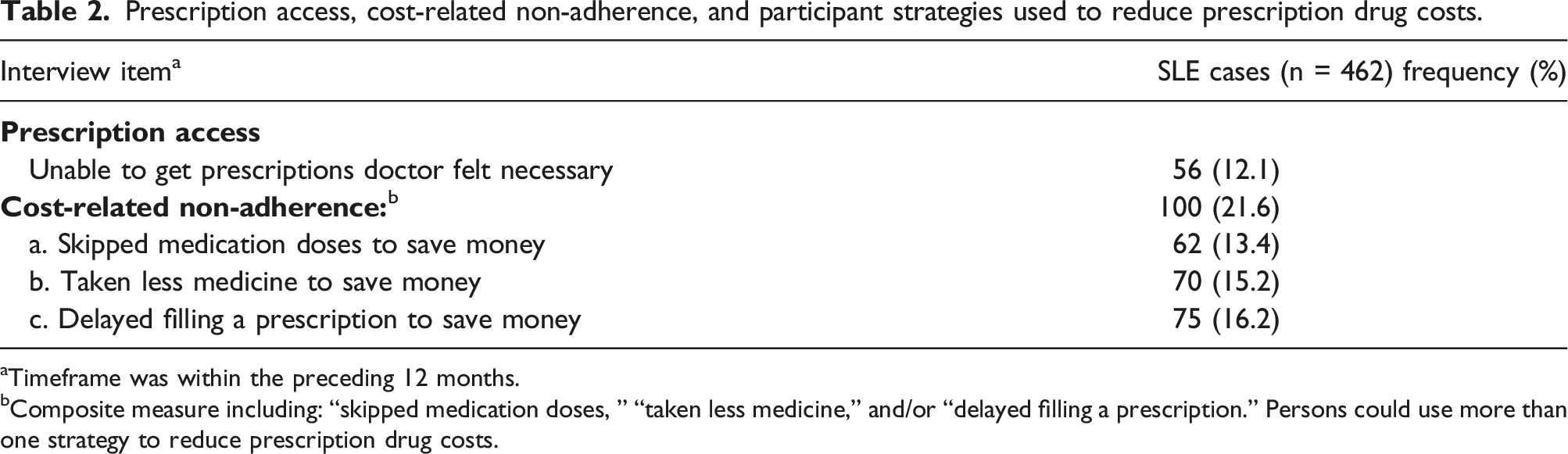
aTimeframe was within the preceding 12 months.
bComposite measure including: “skipped medication doses, ” “taken less medicine,” and/or “delayed filling a prescription.” Persons could use more than one strategy to reduce prescription drug costs.
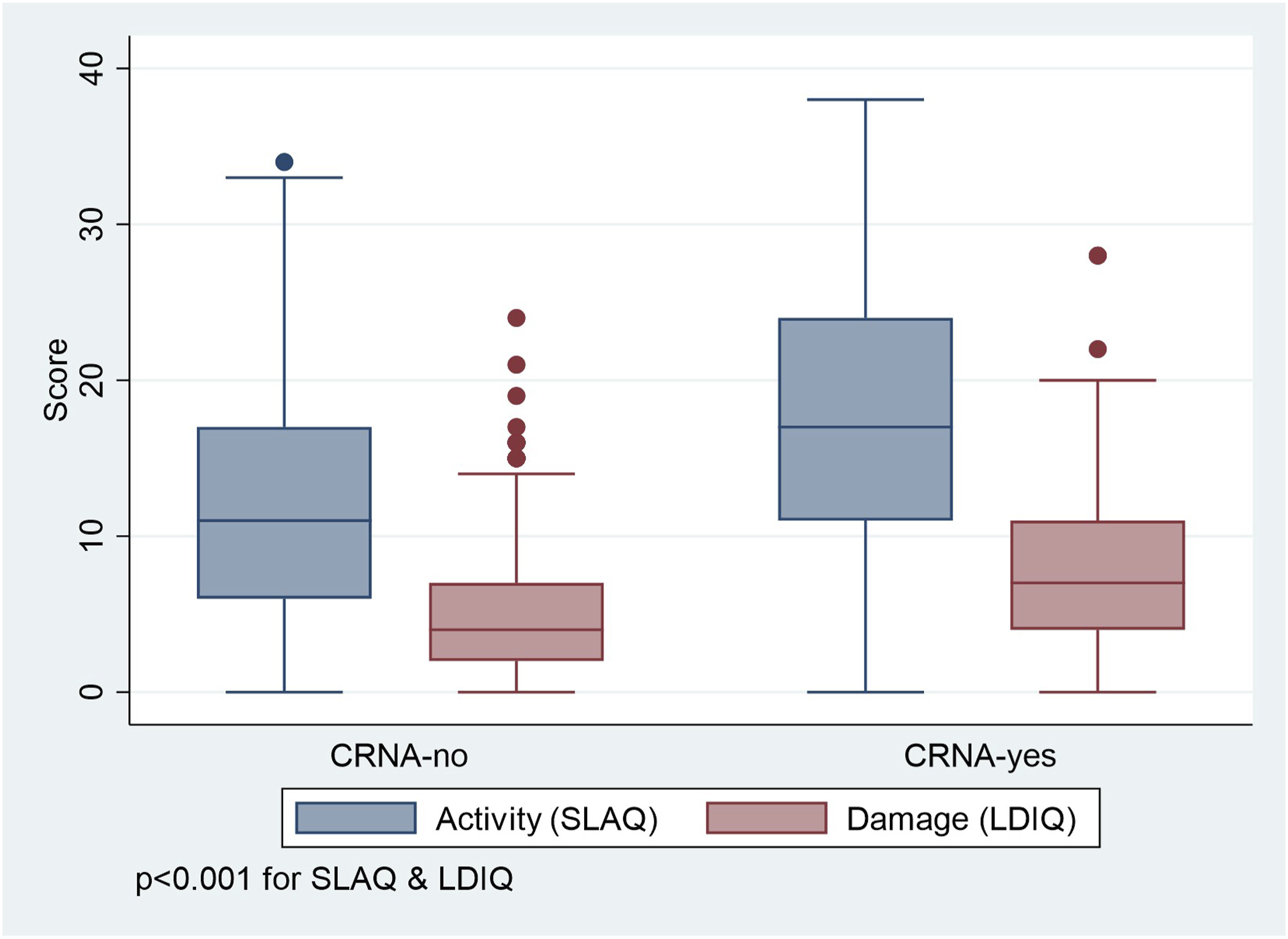
SLE activity and damage scores according to cost-related non-adherence, MILES cohort, 2014–2015. Legend: Both SLE activity and damage were significantly higher for SLE participants reporting CRNA. CRNA = cost-related non-adherence; SLAQ = Systemic Lupus Activity Questionnaire; LDIQ = Lupus Damage Index Questionnaire.
Multivariable regression results for cost-related non-adherence and lupus-related activity and damage, MILES Cohort, 2014–2015.
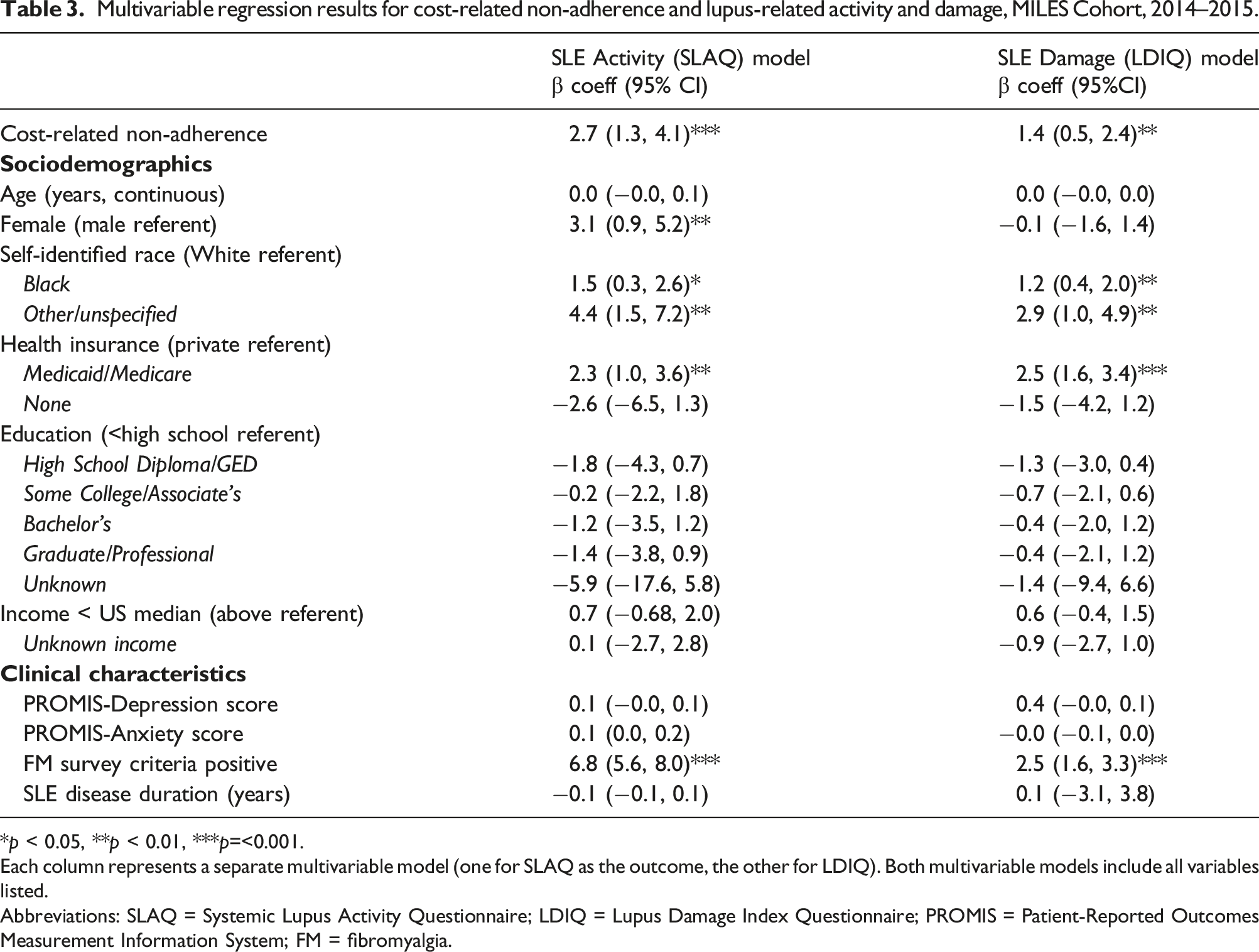
*p < 0.05, **p < 0.01, ***p=<0.001.
Each column represents a separate multivariable model (one for SLAQ as the outcome, the other for LDIQ). Both multivariable models include all variables listed.
Abbreviations: SLAQ = Systemic Lupus Activity Questionnaire; LDIQ = Lupus Damage Index Questionnaire; PROMIS = Patient-Reported Outcomes Measurement Information System; FM = fibromyalgia.
Discussion
We previously documented CRNA in one in five adults with SLE, a level significantly higher than adults from the general population. 12 In this study, we extend those findings by reporting that higher levels of both patient-reported SLE activity and damage at the baseline study visit were associated with CRNA within the last 12 months. Race other than White, public insurance, and fibromyalgia were also associated with both SLE activity and damage, and female sex with SLE activity.
The American College of Rheumatology (ACR) and its Simple Tasks™ public awareness campaign highlighted challenges in prescription affordability in a US nationwide survey in 2019 of over 1500 rheumatology patients. Although 90% of respondents had health insurance, 60% still had difficulty affording their prescribed medication treatment plan over the past year, and 25% of total respondents had more than $1000 in out-of-pocket costs for treatments yearly. 31 A study of older adults in the Medicare Current Beneficiary Survey found that those with RA had higher levels of CRNA than even those with three or more non-RA conditions. 32
Prescription medications are an essential part of SLE management. Policies such as Medicare Part D, 33 and later the Patient Protection and Affordable Care Act of 2010 (ACA) 34 have aimed to improve medication access by reducing out-of-pocket costs. Despite their implementation, the benefits may not reach all of the population equally and racial and ethnic disparities in CRNA persist.35–38 The 2015 National Healthcare Disparities Report assessed the quality of care among different populations based on using more than 260 healthcare process, outcome, and access measures, and covering a wide variety of conditions and patient settings. The results indicated that White patients receive better quality of care than that of Hispanic patients for 36.7% of quality measures, and better quality of care than that of Black patients for 41.1% of quality measures. 39
SLE is a disease with higher occurrence in Black persons, as well as earlier age of onset and increased morbidity, end-organ damage, and mortality compared to White persons with SLE. 40 In this study, participants with SLE who identified as Black had higher SLE activity and damage on average compared to White participants; this persisted after adjusting for CRNA and other variables. Racial disparities in outcomes have complex and multifaceted causes, and there is increasing awareness of structural racism impacting health outcomes.
Sex differences related to CRNA have been observed in some chronic conditions.41–45 One hypothesis is that women may prioritize limited resources for expenses such as food, rent or health care for other family members more so than men. As such, women may skip or delay filling prescriptions, saving money to be able to care for the entire family. Although we were unable to directly address these factors in our study, it represents an area for further investigation, to be equipped to reduce medication non-adherence.
While more studies are needed to understand these issues better, strengthening patient-physician relationships could potentially decrease the likelihood of CRNA. Studies have shown that patients reporting low quality physician relationships are at higher risk for CRNA, even when accounting for prescription costs and income. 46 Further studies are needed to explore the role of structural racism and gender disparities in patient outcomes and may provide guidance on potential mitigation strategies for CRNA.47–49
In the United States, with the confluence of comparatively higher levels of per capita drug spending, out-of-pocket spending, and CRNA than other countries, the extent that cost-related medication factors influence care and outcomes warrants particular scrutiny.8–10 These broad healthcare system issues, coupled with our findings in a SLE cohort, point to the need for healthcare professionals caring for persons with SLE to be well-versed in both financial implications and accessibility issues of care plans. It is also important to maintain vigilance for recognizing and addressing barriers and facilitators that enable medication adherence to be optimized. Ensuring equitable access to appropriate medications required to manage health needs, or pharmacoequity, is gaining recognition as a key facet of reducing health disparities. 50
This study has several strengths. MILES is one of the largest epidemiologic studies of SLE in the United States, and with its population-based design, is comprised of a study population reflecting the sociodemographic diversity of the underlying geographic region. The Cohort includes persons with lupus with a wide spectrum of disease manifestations. Cohort participants are not restricted to patients from the tertiary care setting, and as such, they face the healthcare access challenges encountered by the US population as a whole. The MILES Program documented CRNA and was able to relate it to a wide variety of variables, including potential confounders.
Our study also has several limitations. First, self-report questionnaires are subject to recall and social desirability bias. There are limitations of self-reported data compared to objective data such a prescription refills or disease activity assessment including laboratory data to measure adherence. To the extent possible, we utilized validated questionnaires considered appropriate for epidemiologic studies. Aside from self-reported data from questionnaires, there are limited options to assess patients’ reasons for non-adherence. Strengths of self-reported data include direct assessment of patient experience, and for variables such as race, self-identification is considered the gold-standard. Second, the majority of our study population self-reported race as White or Black, and only a small percentage reported other races or Hispanic ethnicity. While this reflects regional demographics in southeastern Michigan, 51 it limits the generalizability of our results beyond such groups. Further, study participation involves English language proficiency. Third, our Michigan-based study may not be generalizable beyond the state or nation. Fourth, our CRNA study questionnaires did not delineate between SLE-specific medications (e.g., antimalarials, immunosuppressives) and non-SLE medications (e.g., anti-hypertensives). Rather, questions about medication access encompassed prescriptions in general. While it is unclear how much of the cost-related medication non-adherence was related explicitly to the treatment of underlying lupus compared to medication for other health conditions, treatment of comorbidities such as hypertension is important in reduction of poor outcomes. 52 Fifth, it is possible that CRNA may serve as a surrogate for other unmeasured factors surrounding healthcare access and utilization that influence outcomes, such as adherence with timely healthcare appointments and laboratory monitoring, or health literacy. 53 Sixth, our cross-sectional assessment did not assess changes in CRNA or disease activity over time, or in response to factors such as changing economic circumstances.
Our findings reveal that adults with SLE reporting CRNA in the last 12 months had worse disease activity and damage scores. Self-reported race other than White, having Medicaid or Medicare, and fulfilling FM survey criteria were also independently associated with higher SLE activity and damage, though it should be noted that there is a potential for misclassifying FM features as lupus activity when assessed by self-report. Healthcare teams may help address CRNA by becoming familiar with cost containment measures, including prescribing generic medications when available, discussing medication options in the context of future health and cost implications, and involving institutional support services including social work, pharmacy, and patient advocacy. Asking patients about financial barriers, mindfulness about issues relating to disparities, and incorporating cost-related factors in shared decision-making represent potential opportunities to partner with patients to improve outcomes in SLE.
Supplemental Material
Supplemental Material - Cost-related prescription non-adherence and patient-reported outcomes in systemic lupus erythematosus: The Michigan Lupus Epidemiology & Surveillance program
Supplemental Material for Cost-related prescription non-adherence and patient-reported outcomes in systemic lupus erythematosus: The Michigan Lupus Epidemiology & Surveillance program by Deeba Minhas, Wendy Marder, Afton L Hassett, Suzanna M Zick, Caroline Gordon, Sioban D Harlow, Lu Wang, Kamil E Barbour, Charles G Helmick, W Joseph McCune and Emily C Somers in Lupus
Footnotes
Acknowledgements
We thank the study staff and the MILES Cohort participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centers for Disease Control and Prevention (CDC) of the US Department of Health and Human Services (HHS) under grant number U01DP006489 as part of a financial assistance award totaling $2,690,000 with 100% funded by CDC/HHS. This study was also supported by the National Institutes of Health (NIH) through the National Institute of Environmental Health Sciences (NIEHS) and the National Center for Research Resources (NCRR) (grants P30ES017885; UL1TR002240).
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the National Institutes of Health.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.