
Abstract
Objectives
To evaluate adverse pregnancy outcomes in patients with systemic lupus erythematosus (SLE), compare their maternal and fetal outcomes with those of age-matched pregnant women without SLE, and identify factors linked to increased risks of adverse outcomes.
Methods
Medical records from Tawam Hospital were reviewed retrospectively to identify patients with SLE and a history of pregnancy. Demographics, clinical variables, and maternal and fetal outcomes were obtained. A one-to-one age-matched healthy control group was randomly selected. The outcomes and odd ratios of women with and without SLE were compared, and factors associated with adverse pregnancy outcomes were examined.
Results
The outcomes of 78 SLE pregnancies in 39 women were analyzed. Adverse maternal outcomes, such as gestational diabetes mellitus (GDM), occurred in 32% of pregnancies, whereas adverse fetal outcomes, such as low-birth weight and preterm deliveries, occurred in 51% of pregnancies. Pregnant women with SLE had a 5-fold higher risk of GDM, had higher odds of maternal hypertension, and were more likely to deliver through cesarean section than those without SLE. Preterm deliveries and low-birth weight were also more common in SLE pregnancies. Steroid use during pregnancy was significantly associated with an increased risk of GDM development. Lupus nephritis, maternal hypertension, pre-eclampsia, and GDM were linked to preterm deliveries.
Conclusion
Pregnant women with SLE were at a higher risk for adverse maternal and fetal outcomes than age-matched pregnant women without SLE. These findings can guide clinical management and emphasize the need for close monitoring of SLE pregnancies.
Keywords
Introduction
Systemic lupus erythematosus (SLE) is a chronic inflammatory autoimmune disease that mainly affects women of childbearing age. Previously, SLE was considered a contraindication to pregnancy because of the high incidence of adverse outcomes; however, recent advancements in care have enabled women with SLE to safely conceive, carry pregnancies to term, and achieve favorable fetal outcomes. 1 Nevertheless, SLE exerts detrimental effects on maternal and fetal outcomes, with high incidence of adverse events.2–5 Maternal adverse outcomes include pre-eclampsia, maternal hypertension, and the need for a cesarean section, whereas fetal adverse outcomes mainly consist of preterm deliveries, small for gestational age/low-birth weight, and intrauterine growth restriction.4,6,7 Recent improvements in care and the establishment of high-risk clinics that involve interdisciplinary collaboration among rheumatology, obstetrics, fetomaternal, and nephrology services have significantly reduced the incidence of adverse pregnancy outcomes in patients with SLE.2,4,8
This study aimed to evaluate adverse pregnancy outcomes in patients with SLE, compare their maternal and fetal outcomes with those of age-matched pregnant women without SLE, and identify factors associated with increased risk of maternal and fetal adverse outcomes.
Methods
Study population
Medical records of patients with SLE who fulfilled the American College of Rheumatology (ACR) criteria 9 were obtained from Tawam Hospital, a tertiary hospital in Al Ain, Abu Dhabi emirate, the United Arab Emirates, between 2010 and 2020 and were retrospectively reviewed. Patients with SLE and a history of pregnancy were included in the analysis. Pregnant women who were not monitored at Tawam Hospital or who delivered outside this hospital were excluded.
Clinical and demographic variables
Demographic data, including date of birth, date of diagnosis, number of pregnancies, date of last menstrual period for each pregnancy, and delivery date, were extracted from medical records where available. SLE-related clinical data, including all SLE criteria and the SLE disease activity index 2000 (SLEDAI-2K) within 3 months before the last menstrual period and during pregnancy, were also extracted. Further, data on the presence of antiphospholipid antibodies, anti-SSA and anti-SSB antibodies, and comorbidities (Charlson’s index) as well as medications taken before and during pregnancy were collected.
Maternal and fetal outcomes
Maternal outcomes were assessed for the development of thromboembolic events; stroke; heart failure; pregnancy-induced hypertension (hypertension that occurs after 20 weeks of pregnancy); pre-eclampsia (hypertension and proteinuria after 20 weeks of pregnancy); hemolysis, elevated liver enzymes, and low platelets (HELLP) syndrome; gestational diabetes mellitus (GDM) using the World Health Organization (WHO) criteria; and postpartum hemorrhage. Fetal outcomes were evaluated for preterm delivery (defined as delivery before 37 weeks of gestation), low-birth weight (defined as <2500 g), stillbirth (fetal death at or after 20 weeks of gestation), miscarriage (fetal death before 20 weeks of gestation), fetal anomalies, and neonatal lupus.
Control group
Pregnant women without SLE who received antenatal care and delivery services at Tawam Hospital were randomly included in a one-to-one age-matched control group. Similar to the SLE group, data on demographics, comorbidities (Charlson’s index), medications, and maternal and fetal outcomes were collected for the control group.
Statistical analysis
Continuous variables were presented as means (standard deviations), whereas categorical variables were presented as frequencies and percentages. The incidence of maternal and fetal outcomes in women with and without SLE was obtained, and odds ratios (ORs) and confidence intervals (CI) between the groups were calculated. Differences between groups and pregnancy outcomes were compared using chi-square tests for categorical variables and independent t-tests for continuous variables. Statistical analyses were conducted using IBM SPSS Statistics for Windows, version 27.0 (IBM Corporation, Armonk, NY, USA). Ethical approval was obtained from the Ethics Research Board of Tawam Hospital.
Results
Demographic characteristics, diagnostic criteria, and disease activity in pregnant women with SLE.
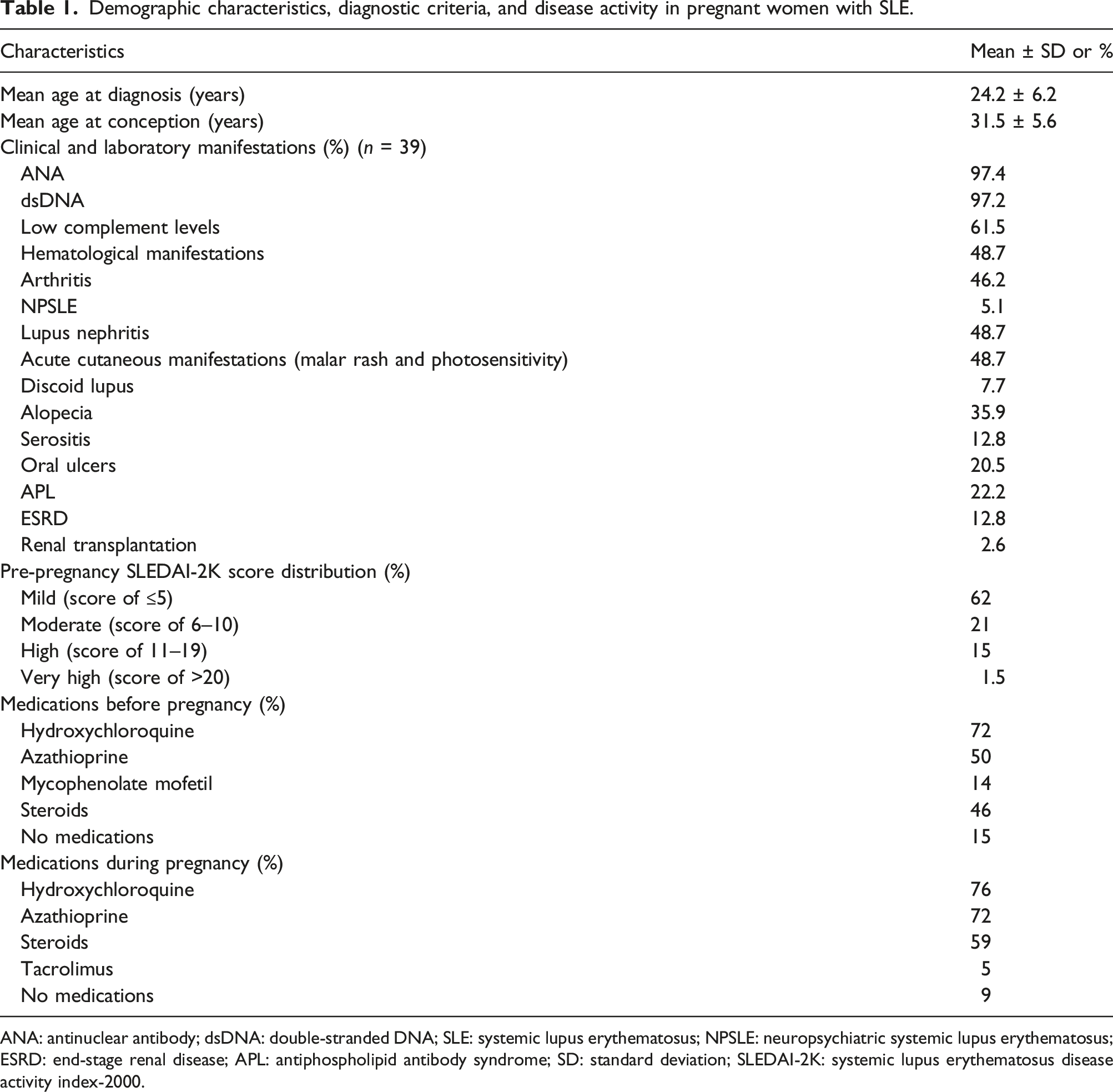
ANA: antinuclear antibody; dsDNA: double-stranded DNA; SLE: systemic lupus erythematosus; NPSLE: neuropsychiatric systemic lupus erythematosus; ESRD: end-stage renal disease; APL: antiphospholipid antibody syndrome; SD: standard deviation; SLEDAI-2K: systemic lupus erythematosus disease activity index-2000.
Maternal outcomes
Comparison of maternal outcomes in women with and without SLE.
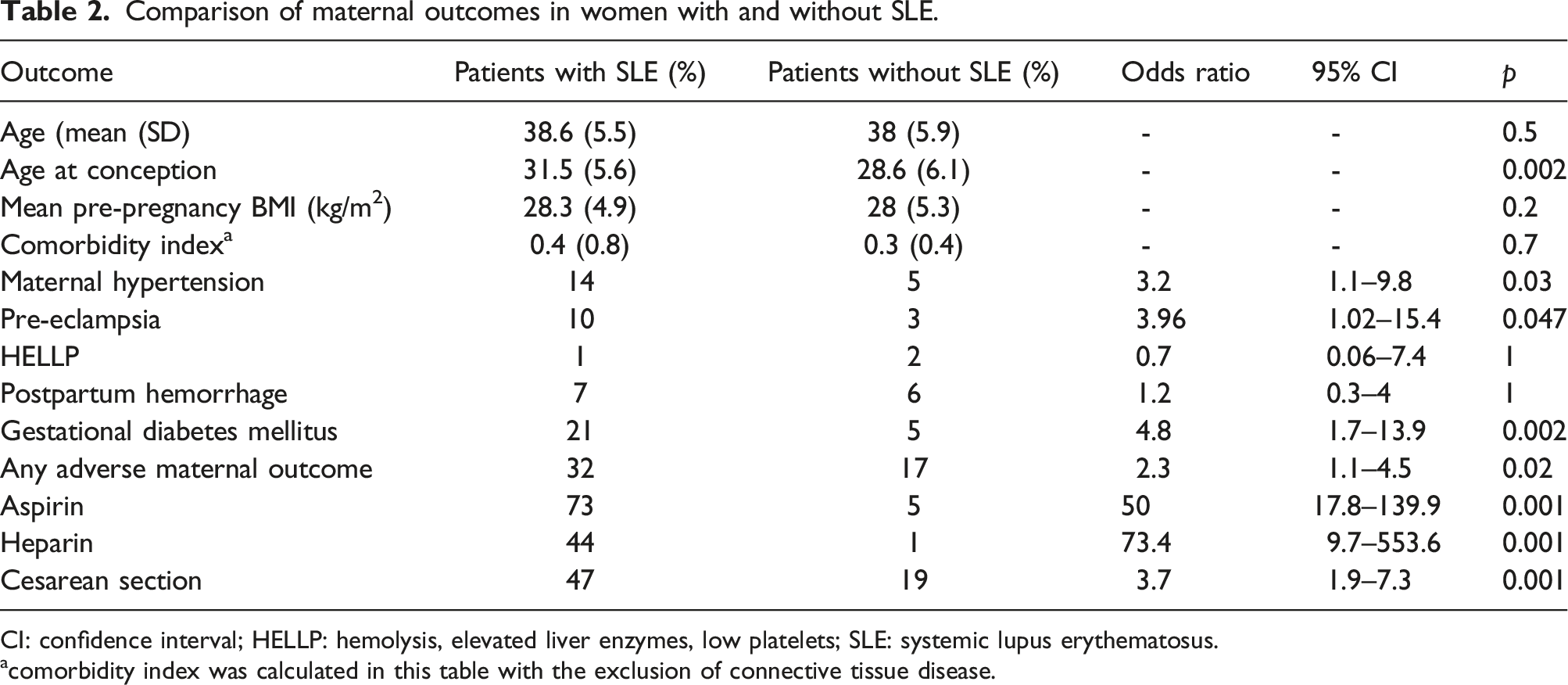
CI: confidence interval; HELLP: hemolysis, elevated liver enzymes, low platelets; SLE: systemic lupus erythematosus.
acomorbidity index was calculated in this table with the exclusion of connective tissue disease.
Factors associated with gestational diabetes mellitus among pregnant patients with SLE.
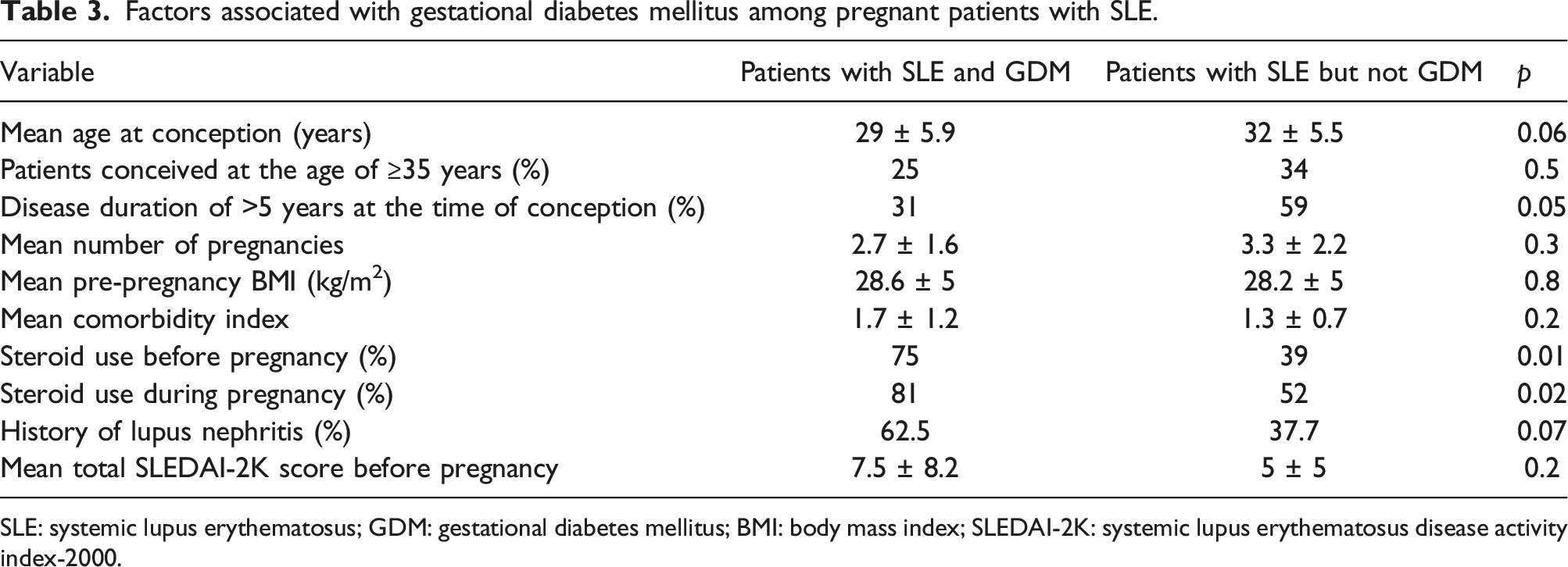
SLE: systemic lupus erythematosus; GDM: gestational diabetes mellitus; BMI: body mass index; SLEDAI-2K: systemic lupus erythematosus disease activity index-2000.
Fetal outcomes
Comparison of fetal outcomes in women with and without SLE.
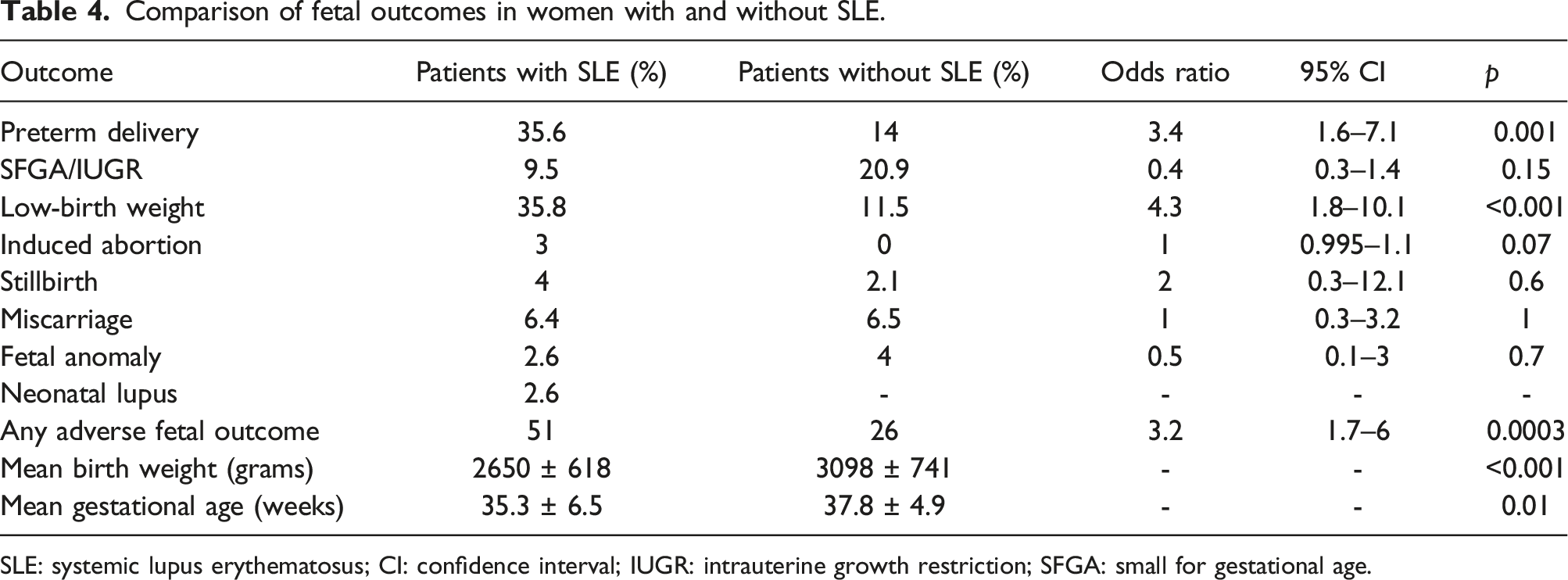
SLE: systemic lupus erythematosus; CI: confidence interval; IUGR: intrauterine growth restriction; SFGA: small for gestational age.
Factors associated with preterm delivery among pregnant patients with SLE.
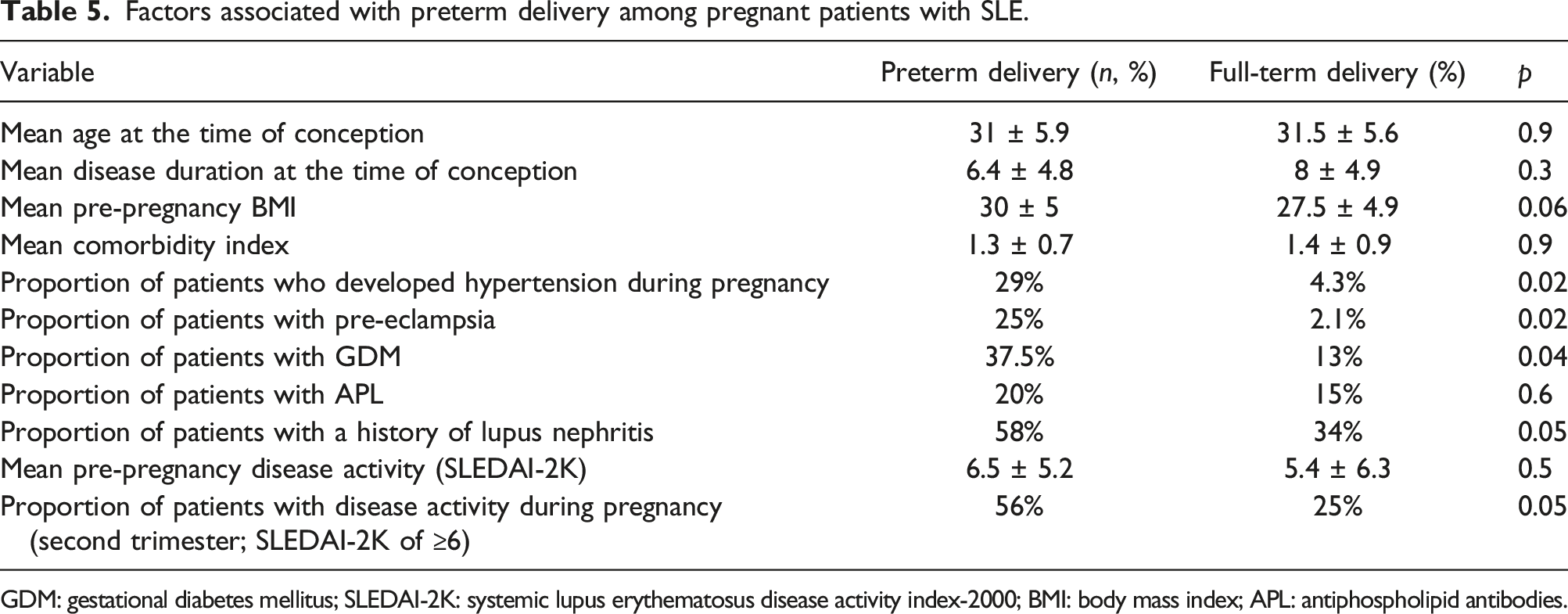
GDM: gestational diabetes mellitus; SLEDAI-2K: systemic lupus erythematosus disease activity index-2000; BMI: body mass index; APL: antiphospholipid antibodies.
Pregnancies in women with and without SLE
The outcomes of pregnancies were compared between the SLE and control group. The mean age of women in the control group at the time of the study was 38 ± 5.9 years, which was similar to that in the SLE group (38.6 ± 5.5 years; p = .5), although age at conceptions was statistically higher for SLE group (31.5 vs 28.6 years, p=.002). Both groups had comparable comorbidities and pre-pregnancies BMI as shown in Table 2. However, pregnant women with SLE had a 5-fold higher risk of developing GDM than those without SLE (p = .002; Table 2). Moreover, compared with women without SLE, those with SLE were more likely to develop maternal hypertension (OR, 3.2; p =.03). Further, pregnant women without SLE were less likely to deliver via cesarean section than those with SLE (p = .001).
In this study, women with SLE were more likely to deliver preterm than those without SLE (OR, 3.4; p = .001; Table 4). Moreover, low-birth weight was more likely to occur in SLE pregnancies (OR, 4.3; p = .001). The mean birth weight in non-SLE pregnancies (3098 ± 741 g) was higher than that in SLE pregnancies (2650 ± 618 g). The mean gestational age in non-SLE pregnancies was 37.8 (4.9) weeks, whereas that in SLE pregnancies was 35.3 (6.5) weeks (Table 4).
Discussion
This retrospective cohort study in patients with SLE revealed different types of adverse maternal and fetal outcomes, factors associated with these outcomes, and higher prevalence of these outcomes in pregnant women with SLE than in those without SLE. The demographic and clinical characteristics of this cohort were consistent with those reported in previously published research on SLE pregnancies.10–14 Approximately 32% of pregnancies in women with SLE are at a risk for adverse maternal outcomes, whereas 51% of them result in adverse fetal outcomes. This finding is consistent with that in the literature, indicating a high risk of adverse pregnancy outcomes in women with SLE.6,15
Adverse maternal outcomes
Several maternal adverse outcomes were identified in this study, among which GDM was the most common (21%). In the literature, the association between GDM and SLE during pregnancy is controversial. According to a recent study, 16 the incidence of GDM is 2-fold higher in SLE pregnancies than in non-SLE pregnancies; however, a meta-analysis suggested no risk of GDM associated with SLE. 17 In this cohort study, GDM occurred in a significantly higher proportion of patients with SLE than in their age-matched control patients without SLE. This finding is substantiated by a meta-analysis of pregnancies in the United Arab Emirates, 18 that reported a GDM prevalence of 8.6% to 16.3%, and aligns with a prior Middle Eastern study identifying GDM in 28% of pregnant women with SLE. 19 In further analysis of clinical and laboratory variables associated with GDM, patients taking oral steroids before (75%) and during pregnancy (81%) were significantly more likely to develop GDM, a finding consistent with a previous study. 17 The development of GDM in patients with SLE is probably influenced by factors beyond oral steroid use. For instance, individuals with SLE exhibit reduced insulin sensitivity and resistance, even in absence of steroid treatment. 20 Our study did not establish a significant association with maternal overweight, obesity, or a maternal age of ≥ 35 years, identified as major risk factors for GDM in the general population. 21 These variations in GDM risks in SLE may be a consequence of differences in study design, sample characteristics, diagnostic criteria for GDM, as well as variations in SLE disease activity and severity. In order to fully comprehend the underlying mechanisms and risk factors contributing to GDM in SLE pregnancies, additional research is required. This will enable the development of more precise interventions to enhance maternal outcomes.
The prevalence of maternal hypertension and pre-eclampsia in the present study were similar to those in some but not all previously reported studies;6,15 the rates of pre-eclampsia reported in different studies ranged from 2% to 20%.3,14,22 The increased risk of pre-eclampsia in SLE patients can be attributed to several factors. Immune dysregulation and inflammation, common features of SLE, contribute to endothelial dysfunction, which plays a crucial role in the development of pre-eclampsia. 23 Additionally, certain autoantibodies found in SLE, such as anti-phospholipid antibodies, are associated with an increased risk of adverse pregnancy outcomes, including pre-eclampsia. 24 Other risk factors include lupus nephritis, 25 active disease during pregnancy, and the use of certain medications such as corticosteroids. 26 Recognizing the heightened risk of pre-eclampsia in SLE patients is essential for clinicians, as it enables them to implement proactive monitoring, early detection, and appropriate management strategies during pregnancy to ensure optimal maternal and fetal outcomes.
Adverse fetal outcomes
This study revealed that pregnancies in women with systemic lupus erythematosus (SLE) are associated with a high prevalence of adverse fetal outcomes. Specifically, 51% of the pregnancies in women with SLE resulted in one or more adverse fetal outcomes, with low-birth weight and preterm delivery being the most commonly reported outcomes. These results are consistent with those of earlier reports of an increased risk of adverse fetal outcomes in women with SLE;4,10,12,27; for example, the prevalence of preterm deliveries among women with SLE reportedly ranged from 25% to 38%.10,19,27,28 This study contributes to the existing knowledge by providing new data on the prevalence of adverse fetal outcomes in a specific population of women with SLE, the Emirati population. In recent studies, placental dysfunction has been identified as a crucial contributor to unfavorable fetal outcomes. 29 In women with SLE, investigators have reported a higher incidence of placental abnormalities such as impaired vascularity and thrombosis, potentially due to the systemic inflammation and autoimmunity present in the disease. Such abnormalities have been directly linked to preterm delivery and other adverse fetal outcomes. 29 Importantly, the presence of lupus anticoagulant, a common manifestation of SLE, has also been associated with a higher risk of preterm delivery, thereby highlighting the complex interplay of factors contributing to adverse pregnancy outcomes in these patients. 29 However, further research is necessary to better comprehend the factors contributing to the prevalence of adverse fetal outcomes in women with SLE.
The risk of preterm deliveries in this cohort of women with SLE was found to be associated with hypertension during pregnancy, development of pre-eclampsia and GDM, increased SLE activity during the second trimester, and history of lupus nephritis. Most patients in this study had no active SLE or had mild disease activity before pregnancy. No significant association was observed between the development of adverse fetal outcomes and pre-pregnancy active SLE; however, active SLE during pregnancy was found to be associated with preterm deliveries. Previous studies have revealed the negative effects of disease activity during pregnancy on fetal outcomes.14,22,30 A large multicenter study comprising 385 SLE pregnancies revealed that increased SLE activity and flares during pregnancy were significantly associated with adverse pregnancy outcomes. 22 Both hypertension and the use of antihypertension medication were found to be associated with the development of preterm deliveries in previous studies.14,22,31 These findings suggest that managing SLE activity during pregnancy is crucial for reducing the risk of adverse pregnancy outcomes. Therefore, clinicians should closely monitor disease activity in pregnant women with SLE and adjust their treatment regimen accordingly to prevent or manage flares. In addition, patients should be educated and counseled regarding the importance of compliance with treatment and regular follow-up to minimize the risk of adverse outcomes. Overall, our study findings highlight the need for a multidisciplinary approach involving rheumatologists, obstetricians, and other healthcare professionals to optimize pregnancy outcomes in women with SLE.
Comparison with the general population
One of the strengths of this study is that pregnancies in women with SLE could be compared with those in the general population matched by age. The data confirmed that pregnant women with SLE were at a higher risk for adverse outcomes than those without SLE. These results are consistent with those of previous studies, including a study involving 338 women in China, wherein pregnant women with SLE had a significantly higher risk of adverse pregnancy outcomes, including pregnancy-induced hypertension, pre-eclampsia, and preterm birth, than those without SLE. 32 However, the abovementioned study reported that GDM was more likely to occur in pregnant women without SLE, which contradicts our study finding. This discrepancy may be due, at least in part, to the different diagnostic criteria for GDM applied in our research. Another study in a similar population to that of our cohort revealed that the incidence of GDM, preterm birth, low-birth weight, abortion, and intrauterine growth restriction were all significantly higher in pregnant women with SLE. 19 In our investigation, we observed an increased likelihood of cesarean section deliveries in pregnancies complicated by SLE. This finding aligns with the research conducted by Wu et al., who reported a higher incidence of C-sections among pregnant women with SLE, particularly those with active disease manifestations. 32 Remarkably, a nationwide longitudinal study spanning 18 years also corroborated this trend, documenting a gradual increase in C-section rates among SLE patients. 33 The higher frequency of cesarean deliveries in these studies, including ours, is likely attributable to the emergence of maternal complications such as gestational diabetes, hypertension, and pre-eclampsia. These recurrent observations across multiple studies emphasize the need for vigilant surveillance and personalized care strategies in managing pregnancies complicated by SLE.32–34
Furthermore, pregnancy presents unique challenges for women with SLE, and appropriate management is essential for improving outcomes. In addition to standard obstetric care, women with SLE may benefit from specialized combined SLE/obstetric clinics. To address both maternal and fetal risks associated with SLE, these clinics provide comprehensive care that includes monitoring disease activity, managing medications, and preventing complications, such as pre-eclampsia and preterm birth. By providing a coordinated and multidisciplinary approach to care, combined clinics can help ensure that pregnant women with SLE receive the best possible care to optimize both maternal and fetal outcomes.
Limitations
This study provides novel insights into the prevalence of adverse maternal and fetal outcomes in women with SLE in the Emirati population. However, this study has several limitations. First, this study was retrospective in nature, which may have introduced recall bias, causing an underestimation of certain symptoms or complications. Second, the sample size was relatively small, which limited our ability to detect significant differences between subgroups of patients. Although the findings provide valuable insights into the effects of SLE on pregnancy outcomes, these limitations should be considered when interpreting these results.
Conclusion
This retrospective cohort study revealed that compared with the general population, pregnant women with SLE were at a significantly higher risk for adverse maternal and fetal outcomes, including GDM, maternal hypertension, preterm delivery, and low-birth weight. The development of GDM was significantly associated with the use of oral steroids before and during pregnancy. Risk factors for adverse fetal outcomes included disease activity, lupus nephritis, and development of maternal complications, such as maternal hypertension and pre-eclampsia. These findings suggest the need for multidisciplinary care in the management of pregnant women with SLE to optimize maternal and fetal outcomes. Further research is necessary to better understand the underlying mechanisms of adverse pregnancy outcomes in women with SLE and to develop effective interventions to mitigate these outcomes.
Footnotes
Acknowledgments
We would like to express our gratitude to Reem Al Dhaheri, Manal Al Khanbashi, and Shamma Al Alawi for their valuable contributions during the initial phase of this study. Editorial support (English Language and spelling) was performed by Enago, Crimson Interactive Inc. This assistant was funded by the United Arab Emirates University.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.