
Abstract
Objective
To report the differences in phenotypic characteristics, disease course, and outcome in monogenic and sporadic childhood lupus (SC-lupus) from a single tertiary childhood lupus clinic.
Methods
A descriptive, observational, cross-sectional study was conducted. Data were retrospectively collected at the last follow-up visit on patients with monogenic lupus proven by genetic variants and SC-lupus seen between June 1997 and July 2022. SC-lupus patients were selected by systematic sampling from lupus patients presenting to our lupus clinic; the first patient was chosen randomly, and the subsequent patients were chosen at intervals of three. Data comprised the clinical and laboratory findings, disease activity using the SLEDAI, and damage measured by the pSDI.
Results
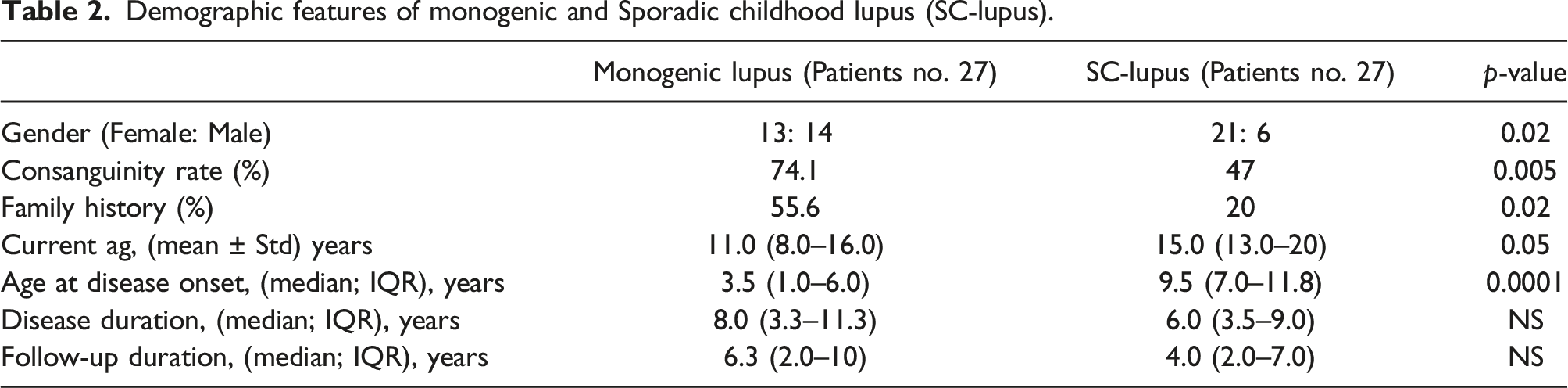
A total of 54 patients with a median disease duration of 6.8 (IQR 3.5–10.5) years were included. There were 27 patients with monogenic lupus and 27 patients with SC-lupus, with a median age at disease onset of 3.5 (IQR 1.0–6.0), and 9.5 (IQR 7.0–11.8), respectively. (p < 0.05). The rate of consanguinity and family history of lupus were higher in monogenic lupus patients. The two groups were comparable. However, monogenic lupus patients showed more gastrointestinal tract symptoms, and failure to thrive (p < 0.05). They also had more infections. The frequency of the autoantibody profile was higher in monogenic lupus patients. Belimumab was more frequently used in monogenic lupus while rituximab in SC-lupus patients. Monogenic lupus patients had a higher mean SLEDAI, but statistically, it was insignificant. Patients with monogenic lupus had greater disease damage, with a higher mean pSDI and a higher mortality rate (p < 0.05).
Conclusion
Patients with monogenic lupus are likely to have an early disease onset and a strong family history of lupus, as well as a guarded prognosis, which is likely due to the disease’s severity and frequent infections. These differences may be related to the high consanguinity rate and underlying genetic variants.
Introduction
Systemic lupus erythematosus (SLE) is a complex autoimmune disease affecting multiple systems and exhibiting a wide range of clinical manifestations. It is characterized by the presence of autoantibodies that target nuclear autoantigens, increased production of type I interferon, and abnormalities in B cell function. 1 The clinical features, genetic findings, and disease course of SLE vary significantly among different age groups and races.2,3 Despite remarkable progress in understanding the etiopathogenesis of SLE, the exact etiology remains unknown. 4
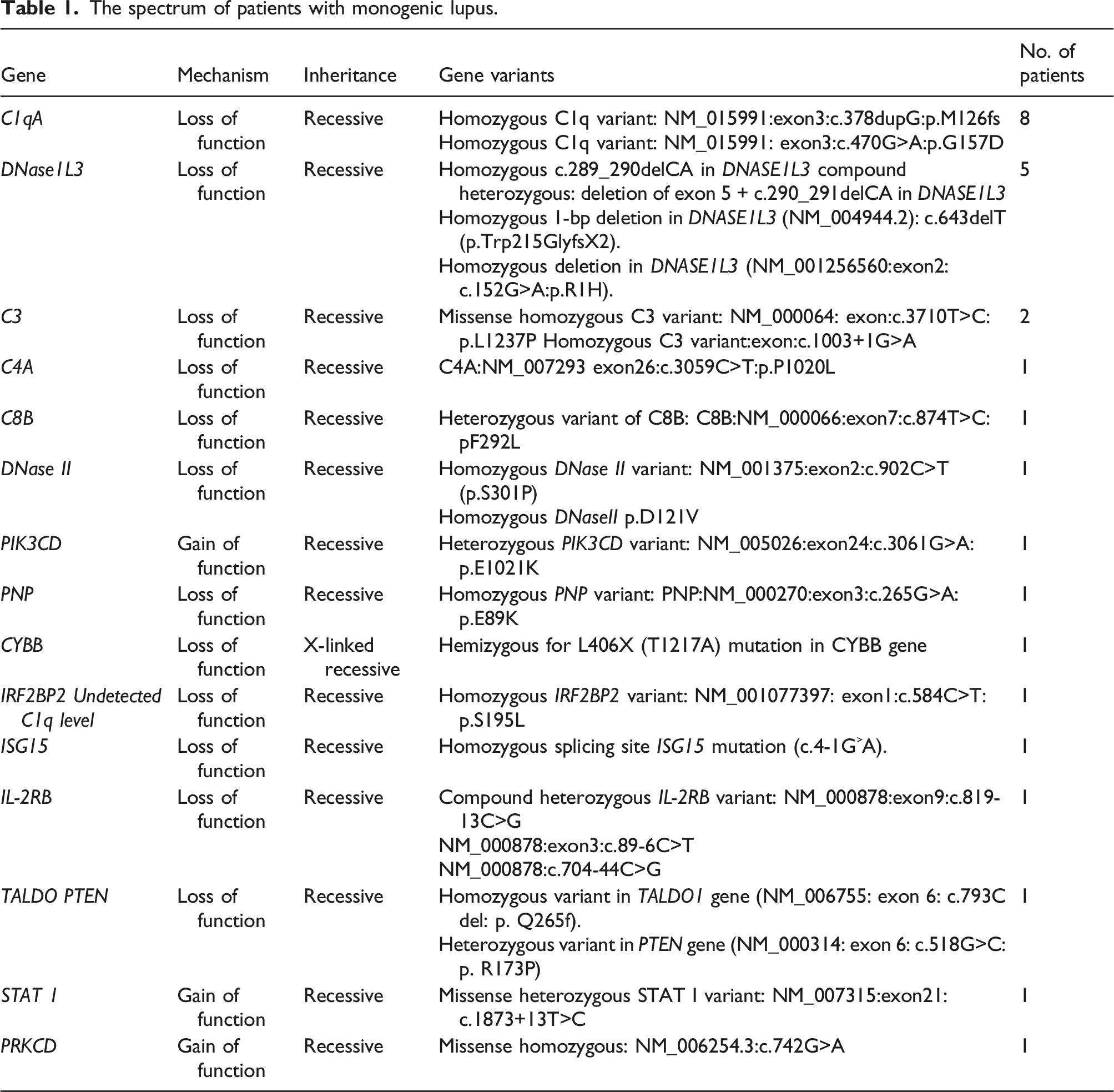
Childhood-onset SLE (cSLE) typically occurs between the ages of 12 and 16 years, rarely appearing before 5 years of age.5,6 Monogenic lupus is a rare form of lupus characterized by an early-onset disease course and a severe phenotype, likely caused by a single gene mutation with a hereditary contribution. Consanguinity, among other risk factors, increases the likelihood of monogenic lupus and should prompt consideration of a monogenic lupus diagnosis in patients with familial lupus.7–9 Advancements in molecular genetic testing have identified several genes associated with lupus or lupus-like, homozygous hereditary defects in early components of the classical complement pathway such as C1q and C4 have been well described to be associated with high susceptibility for development of SLE. However, novel genes continue to be discovered, leading to variations in disease pathogenesis and phenotypes.10–15 Despite substantial data gained in the field of monogenic lupus, limited knowledge is available regarding the variability in disease phenotypes and treatment between cSLE and monogenic lupus.
Our study aimed to report the differences in phenotypic characteristics, disease course, and outcome between monogenic and sporadic childhood lupus (SC-lupus) in a single tertiary childhood lupus clinic.
Materials and methods
This is an observational retrospective study that comprised patients with SC-lupus and monogenic lupus who were seen at at King Faisal Specialist Hospital and Research Center (KFSHRC), Riyadh, Saudi Arabia, from June 1997 to July 2022. We obtained the patient data from our pediatric rheumatology database. For the SC-lupus patients, we employed systematic sampling from lupus patients who visited our lupus clinic. The first patient was chosen randomly, and subsequent patients were selected at intervals of three. The criteria for inclusion were patients under 14 years of age at diagnosis and meeting the EULAR/ACR 2019 classification criteria for SLE.16,17 Furthermore, all monogenic lupus patients included had proven pathogenic gene variants.
At the last follow-up visit, we retrospectively collected data on demographics, clinical manifestations, and laboratory findings including autoantibody profile; disease activity using the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) 18 ; and damage measured by the pediatric adaptation of the Systemic Lupus International Collaborating Clinics American College of Rheumatology Damage Index (pSDI). 19 We excluded patients with familial SLE who lacked confirmed genetic testing and those with insufficient data. Due to the rarity of monogenic lupus, calculating the sample size was not feasible.
Statistical considerations
For this retrospective study, all statistical analyses of the data were conducted using the SAS software package, version 9.4 (Statistical Analysis System, SAS Institute Inc., Cary, NC, USA). Descriptive statistics for continuous variables were reported as mean ± standard deviation, and categorical variables were summarized as frequencies and percentages. The median and interquartile range (IQR) are used when deemed necessary. Continuous variables were compared by independent Student’s t-test, ANOVA, or non-parametric (Mann–Whitney U/Kruskal–Wallis) tests as appropriate, while categorical variables were compared by the Chi-square test. Fisher’s exact probability test was applied when examining variables of low incidence. The level of significance was set at a p-value < 0.05.
Ethical considerations
The study adhered to the principles outlined in the Declaration of Helsinki (2000) and was carried out following the approval of the Ethics Committee of the Research Affairs Council at KFSHRC, under the study protocol RAC# 221105. All clinical and laboratory assessments were performed as part of routine medical care. Prior to blood extraction, the parents provided informed consent for genetic testing, which was integrated into the patient’s healthcare. All collected data was analyzed while ensuring confidentiality, and personal identification was not necessary.
Results
The spectrum of patients with monogenic lupus.
Demographic features of monogenic and Sporadic childhood lupus (SC-lupus).
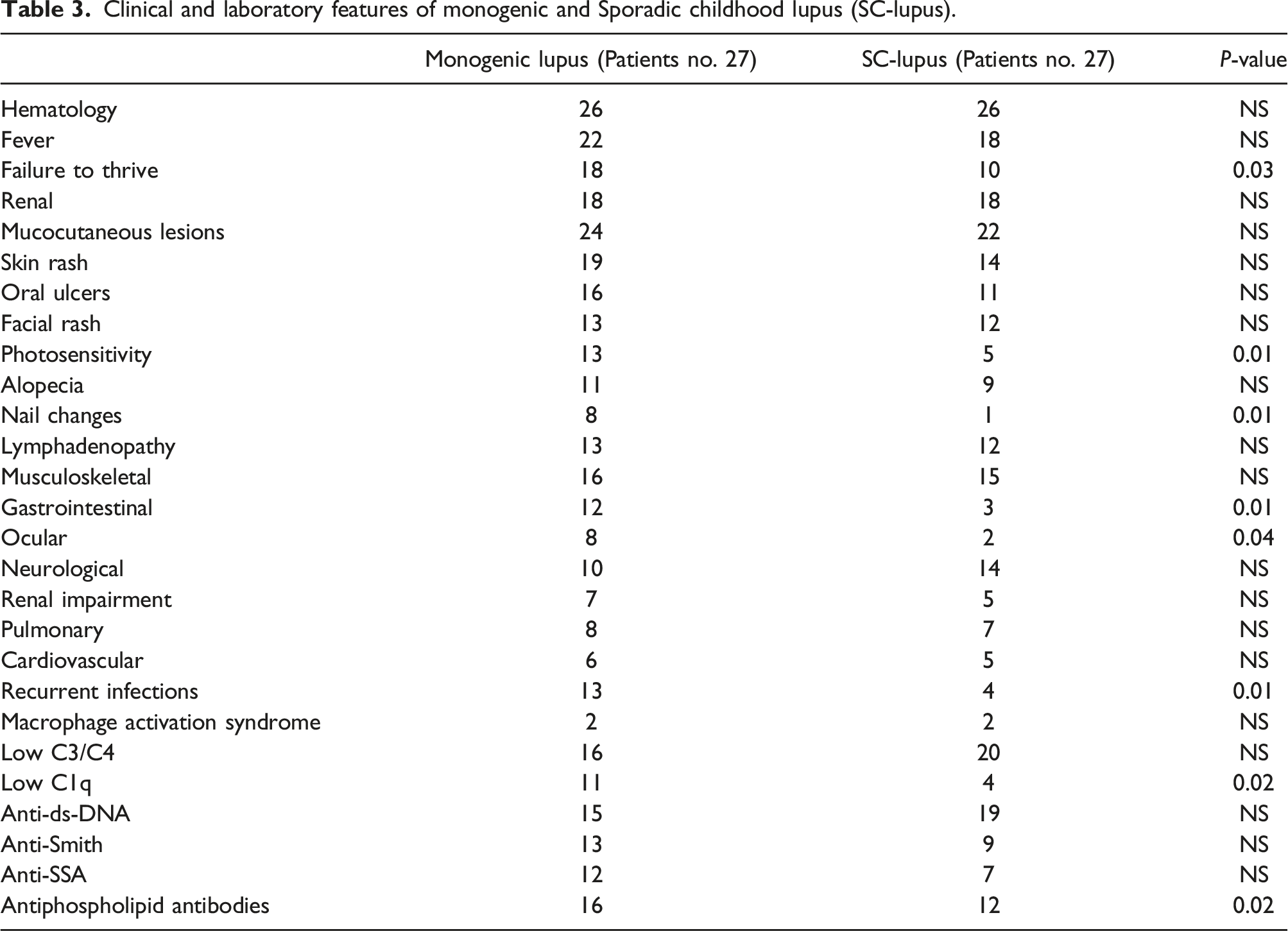
Clinical and laboratory features of monogenic and Sporadic childhood lupus (SC-lupus).
All patients received corticosteroids and hydroxychloroquine. It is noteworthy that belimumab was more frequently used in patients with monogenic lupus, whereas rituximab was more commonly used in SC-lupus patients. Furthermore, methotrexate and Janus kinase inhibitors were mainly used for patients with monogenic lupus. Otherwise, the two groups were comparable in terms of other immunosuppressive drugs.
Treatment and outcome.
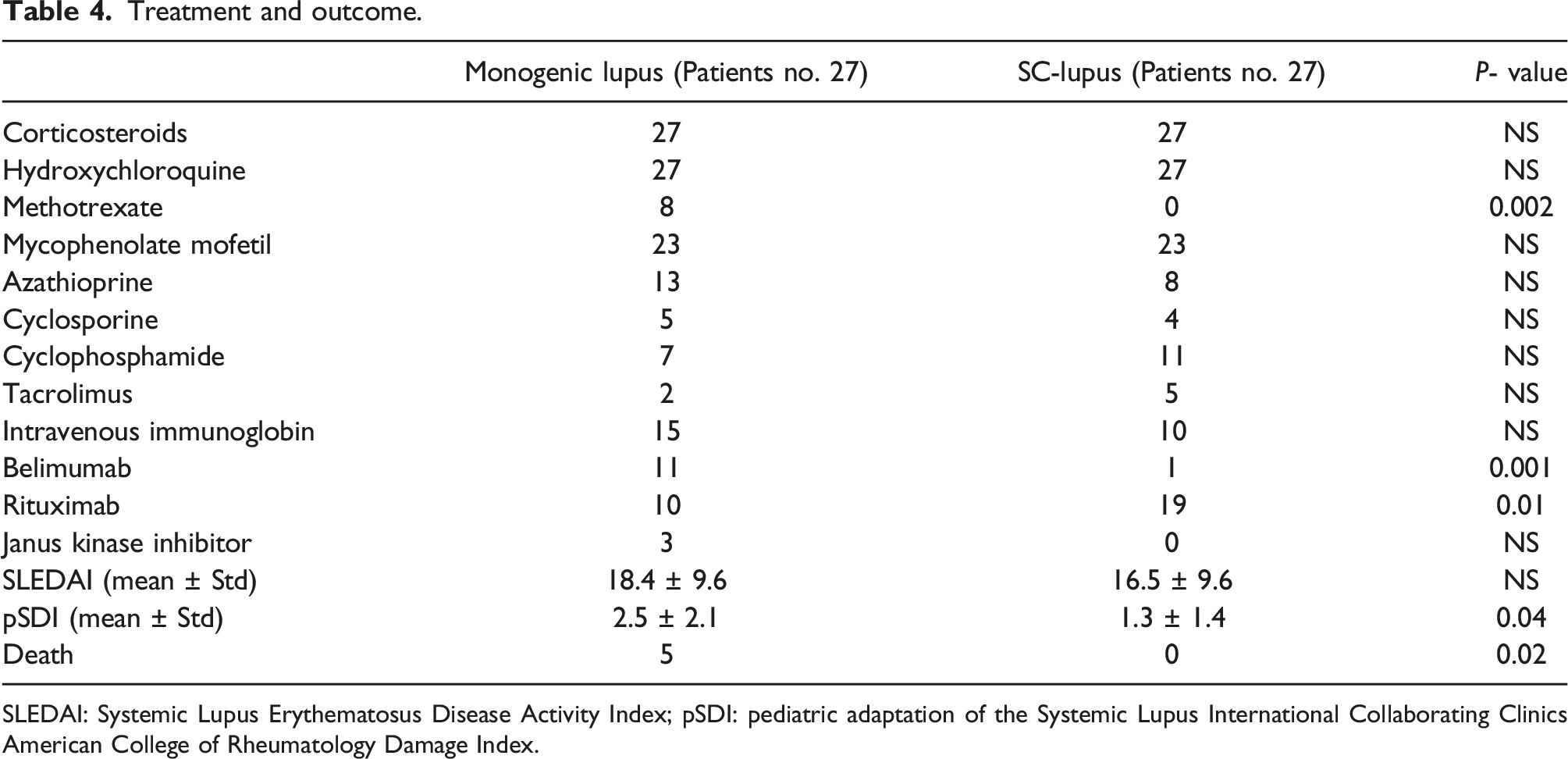
SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; pSDI: pediatric adaptation of the Systemic Lupus International Collaborating Clinics American College of Rheumatology Damage Index.
Discussion
Monogenic lupus is a rare and heritable entity with significant diversity in etiopathogenesis, phenotypic features, and disease progression, and outcomes. Recent developments in molecular genetic testing have contributed to the growing recognition of monogenic lupus worldwide.4,9,20 It can be considered as part of the lupus cluster which encompasses a range of phenotypically distinct entities with variations in age of onset, and severity, and underlying causes, including SLE. 21 Yet, the differences in phenotype and disease progression between monogenic and SC-lupus are not widely recognized and reported. This observational study aimed to compare these differences between patients with monogenic lupus and SC-lupus. Our study included one of the largest cohorts of monogenic lupus patients, revealing significant disparities between the two groups. Patients with monogenic lupus were generally younger and experienced an earlier onset of the disease. The observed female predominance in SC-lupus aligns with the previous reports, whereas no gender preponderance was observed in patients with monogenic lupus. The exact explanation for this discrepancy remains unclear, but it is possible that the high prevalence of familial cases and high consanguinity rate could influence these observations.
In our cohort, patients with monogenic lupus were more likely to have oral ulcers and mucocutaneous lesions. However, statistically significant differences were only found in photosensitivity and nail dystrophy associated with yellowish discoloration, which has been reported in patients with C1q deficiency. 22 Interestingly, gastrointestinal manifestations appeared to be more frequent in patients with monogenic lupus, including recurrent abdominal pain, vomiting, and symptoms resembling gastroenteritis. Additionally, three patients experienced pancreatitis, as confirmed by elevated pancreatic enzymes and ultrasound findings. In comparison to patients with SC-lupus, those with monogenic lupus were not thriving well. The reasons for this are unclear, but it could be partially attributed to the high frequency of gastrointestinal manifestations and the influence of genetic factors. Ocular manifestations were significantly more likely to be seen in patients with monogenic lupus and encompassed features such as cataract, optic disc changes, and retinal abnormalities.
The prevalence of infections within our cohort ranged from 14.8 to 48.2%. Patients with monogenic lupus, however, had a higher likelihood of various infections, indicating an underlying immunedysregulation state. Interestingly, our patients with monogenic lupus and SC-lupus experienced similar prevalence of macrophage activation syndrome.
Overall, patients with monogenic lupus and SC-lupus exhibited comparable autoantibody profiles. However, the antiphospholipid antibody (APL), specifically, IgG anticardiolipin and β2-glycoprotein, was significantly more frequent in monogenic lupus patients. The reasons for this discrepancy remain uncertain; we propose that the high frequency of infections in patients with monogenic lupus may potentially contribute to the development of APL. 23 On the other hand, patients with SC-lupus had a higher prevalence of ds-DNA antibody positivity, although this difference was not statistically significant. Additionally, there were no significant disparities in complement (C3 and C4) levels. However, low C1q levels were more frequent in patients with monogenic lupus, which was anticipated due to the notable prevalence of C1q deficiency patients among our cohort.
Currently, there is no consensus on the therapeutic approach for monogenic lupus. Treatment mainly follows guidelines for childhood lupus and relies on expert opinions. In general, patients with monogenic lupus required more sequential immunosuppressive drugs, with a partial therapeutic response. Corticosteroids, hydroxychloroquine, and mycophenolate mofetil remained the most used medications for both monogenic lupus and SC-lupus. Belimumab and methotrexate were more frequently used in monogenic lupus, primarily for treating mucocutaneous manifestations.
The decision to incorporate belimumab alongside with immunosuppressive drugs was influenced by its accessibility, in addition to emerging evidence highlighting its effectiveness in lupus patients with elevated type I interferon expression. The observed increase in B lymphocyte stimulator (BLyS) and type I interferon mRNA levels among lupus patients was correlated with favorable responses to belimumab. Moreover, our constrained experience has revealed promising response to belimumab in patients with monogenic lupus.24,25 Of note, several related genes are involved in the pathway of complement deficiency and excessive production of interferon-α, both mechanisms studied in lupus pathogenesis.8,10 Regarding rituximab, while its use is off-label for lupus patients, it was accessible at an earlier time frame than belimumab in our institution. It was regarded as the first biologic intervention for lupus patients presenting with renal and neurological involvement. Considering both its early availability and the substantial number of sporadic lupus patients, along with the nature of this work, all these elements could collectively influence the frequency of rituximab usage.
Several anecdotal reports suggest that hematopoietic stem cell transplantation may be considered a potential therapeutic intervention for cases of refractory C1q-deficient monogenic lupus. However, this modality of treatment is a complex and high-risk procedure. However, more studies are required to draw firm conclusions.26,27
Despite comparable disease activity at the last follow-up visits, patients with monogenic lupus had a remarkably higher estimated frequency of accrual damage and mortality rate compared to those with SC-lupus, despite receiving aggressive treatment. This could be attributed to underlying genetic defects and the high prevalence of infections in patients with monogenic lupus.
The main strengths of our study include a relatively large cohort of monogenic lupus from a single center, as well as data was collected from a population with a high rate of consanguinity and a significant prevalence of monogenic lupus. However, our study has limitations, and the results should be interpreted with caution. Data was collected retrospectively over an extended period, and inconsistencies in the therapeutic approach and use of off-label medications were observed due to the lack of guidelines for the treatment.
Conclusions
This study compares a large data on monogenic lupus with SC-lupus in Arab children. It highlights that patients with monogenic lupus tend to experience an early onset of disease, have a strong family history of lupus, and face a guarded prognosis, likely due to the disease severity and frequent infections. These differences may be influenced by the high consanguinity rate and underlying genetic variants. We hope that this report raises awareness of monogenic lupus among health care providers, even in regions with limited access to molecular genetic assessment.
Footnotes
Acknowledgments
Authors are deeply grateful to Ms. Samia AlHashim (Biostatistician) for her great help in the data processing and analysis.
Author’s Contributions
Conceptualization: [Fatima Alkhars, Alhanouf AlSaleem, and Sulaiman M Al-Mayouf]; methodology: [Sulaiman M Al-Mayouf]; Formal analysis: [Sulaiman M Al-Mayouf
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.