
Abstract
Background
Systemic lupus erythematosus (SLE) is a complex autoimmune connective tissue disease (CTD) that is an important cause of devastating pulmonary arterial hypertension (PAH), and persistent progression of PAH can lead to right heart failure, predicting a poor prognosis for SLE patients. Right ventricular-pulmonary arterial (RV-PA) coupling with echocardiography has been demonstrated to be a noninvasive alternative method for evaluating PAH patients' predictive outcomes. Whether the ratio of right ventricular stroke volume (RVSV) to right ventricular end-systolic volume (RVESV) measured by three-dimensional echocardiography (3DE) is a new index of RV-PA coupling has not been discussed as a new predictor for the clinical outcome of systemic lupus erythematosus-associated pulmonary arterial hypertension (SLE-PAH).
Methods
From June 2019 to February 2023, 46 consecutive patients with SLE-PAH were enrolled prospectively, and their clinical data and echocardiographs were studied and analyzed. The control group consisted of 30 healthy subjects matched for age, sex, and body surface area (BSA). The main endpoints of this study were a composite of all-cause mortality and adverse clinical events. Baseline clinical characteristics and echocardiographic assessments were analyzed.
Results
During a median of 24 months (IQR 18–31), 16 of 46 SLE-PAH patients (34.7%) experienced endpoint-related events. At baseline, patients who experienced mortality or adverse events had a worse WHO functional class (WHO FC) and lower anti-double-stranded DNA (dsDNA) antibody levels. The right ventricular (RV) systolic dysfunction in SLE-PAH subjects was significantly worse than that in the healthy control group, especially in SLE-PAH patients in the endpoint event group. Compared to controls, patients with SLE-PAH had a lower RVSV/RVESV ratio. In the group comparison, patients who had experienced an endpoint event had a sequentially worse ratio (1.86 (1.65–2.3) versus 1.30 (1.09–1.46) versus 0.64 (0.59-0.67), p < .001). There were statistically significant associations between the RVSV/RVESV ratio to routine RV systolic function and clinical parameters. The RVSV/RVESV ratio was negatively correlated with the WHO FC (r = −0.621, p < .001) and positively correlated with the anti-dsDNA level. The ROC curve showed that the optimal cutoff for RVSV/RVESV < 0.712 determined a higher risk of poor prognosis. Kaplan‒Meier survival curves showed that an RVSV/RVESV ratio >0.712 was associated with more favorable long-term outcomes.
Conclusions
The 3DE-derived SV/ESV ratio as a noninvasive alternative surrogate of RV-PA coupling was an eximious indicator for identifying endpoint events in SLE-PAH patients and can provide a diagnostic basis for clinical intervention.
Keywords
Introduction
Systemic lupus erythematosus (SLE) is a complex autoimmune connective tissue disease (CTD) characterized by aberrant activity of the immune system that damages various systems and organs. 1 Connective tissue disease-associated pulmonary arterial hypertension (CTD-PAH) is one of the major causes of PAH, accounting for approximately one-fourth of the overall PAH population. Among them, systemic lupus erythematosus-associated pulmonary arterial hypertension (SLE-PAH) accounts for approximately 50% of CTD-PAH cases. 2 PAH is an important cause of cardiovascular disease and a devastating complication of SLE that has high mortality and morbidity.3,4 Right ventricle (RV) function has been validated to be a prognostic factor in patients with SLE-PAH or CTD-PAH.5–9 Therefore, early recognition of myocardial involvement and detection of subclinical cardiac insufficiency are essential for early intervention and prognosis of SLE patients.
Right ventricular pulmonary arterial (RV-PA) coupling represents the ability of the RV to compensate or perform with preserved systolic function with increasing afterload. 10 Invasive hemodynamic evaluation by right heart catheterization (RHC) is the gold standard for the assessment of patients with pulmonary hypertension. Current studies suggest that the ratio of tricuspid annular plane systolic excursion (TAPSE) to pulmonary artery systolic pressure (PASP) examined by echocardiography has been shown to be a noninvasive surrogate of RV-PA coupling and has been incorporated into the 2022 ESC/ERS guidelines for comprehensive risk assessment in pulmonary arterial hypertension. 4 However, patients with limited tricuspid regurgitation signals are not suitable candidates for this approach.
The use of advanced echocardiographic techniques, particularly 3-dimensional echocardiography (3DE), are currently proposed as an approach that is readily available, noninvasive and more sensitive. 3DE-determined RV volumes and ejection fraction (EF) values correlate strongly with CMR when evaluating RV volumes and function and can be considered an alternative technique that overcomes the above limitations.11,12 Recent studies have shown that the ratio of RVSV to RVESV is a powerful predictor of clinical outcome in PH.13,14 Noninvasive evaluation of RV-PA coupling using the RVSV/RVESV ratio measured by 3DE has not been studied in patients with SLE, and information regarding RV-PA coupling and RV function using 3DE is scarce.
The purpose of the present study was therefore to assess RV function and RV-PA coupling in a cohort of patients with SLE using advanced 3DE measurements. Whether the RVSV/RVESV ratio is associated with the development of clinical events in these patients remains to be assessed.
Methods
Patient population
From June 2019 to February 2023, we enrolled consecutive patients with SLE-PAH who were admitted to the Department of Nephrology or Rheumatology at the First Affiliated Hospital of Guangxi Medical University. Patients underwent an extensive multidisciplinary assessment and echocardiography at our center to assess heart structure and function and pulmonary artery pressure. Consecutive patients diagnosed with SLE fulfilled the 1997 American College of Rheumatology criteria. 15
Included patients with SLE were considered to have SLE-PAH if they met the following criteria4,16: (1) tricuspid regurgitation velocity (TRV) > 3.4 m/s measured by transthoracic echocardiography; (2) TRV > 2.9 m/s in combination with signs of pulmonary hypertension; (3) or had a diagnosis of PAH confirmed by RHC.
The exclusion criteria included the following: (1) left heart disease including systolic dysfunction (defined as left ventricle (LV) ejection fraction <52% for men and <54% for women on 2DE); (2) primary cardiomyopathy and moderate to severe valvular heart disease; (3) congenital heart disease; (4) chronic obstructive pulmonary disease, interstitial lung disease and chronic pulmonary thromboembolism; and (5) inadequate echocardiograms. This study finally included 46 patients with SLE-PAH, and the control group consisted of 30 healthy subjects, matched for age, sex, and body surface area (BSA).
The main endpoints of this study were a composite of all-cause mortality and adverse clinical events during follow-up, and all adverse events were recorded. Adverse clinical events included the following: PAH-associated hospitalization with deteriorated RV failure, new PAH drug treatment of intravenous prostacyclin, creation of an atrial septostomy, and performance of lung transplantation. 13 The vital status of all patients was confirmed through a review of medical records. The survival time was calculated from the time of baseline echocardiography to the endpoint or the end of the study.
Patients provided informed consent for the use of clinically collected clinical and echocardiographic data. Ethical approval from the Ethics Committee of the First Affiliated Hospital of Guangxi Medical University was obtained for this study.
Clinical data
Detailed clinical data including demographics, duration of SLE, WHO functional classification (WHO FC), comorbidities, and cardiovascular disease-related factors were recorded based on a review of electronic records at baseline. SLE-related factors and characteristics including SLE-associated autoimmune conditions, SLE medications (glucocorticoids, nonsteroidal anti-inflammatory drugs, immunosuppressive agents, biologics, and PAH therapy), and laboratory tests (autoimmune antibodies, complement, blood counts, cardiac biomarkers, and metabolic markers) were also recorded.
The Safety of Estrogens in Lupus Erythematosus National Assessment-Systemic Lupus Erythematosus Disease Activity Index (SELENA-SLEDAI-2K) was used to assess SLE disease activity. The SLEDAI score was graded according to the following criteria: 0–4 for basic inactivity, 5–9 for mild activity, 10–14 for moderate activity, and ≥15 for severe activity.
Routine transthoracic echocardiography
Standard transthoracic echocardiography was performed by a Philips EPIQ7 ultrasound scanner equipped with a proprietary S5-1/X5-1 probe (Philips Healthcare) according to the current standards of the American Society of Echocardiography. 17 3DE examinations of RV function were assessed as recommended by current guidelines of the right heart in adults. 16
A standard apical four-chamber view was used to evaluate the left ventricular ejection fraction (LVEF) by the Simpson method. An RV-focused apical four-chamber view was used to obtain tricuspid annular plane systolic excursion (TAPSE) by measuring the M-mode and tricuspid valve lateral annular peak systolic velocity (S′) by pulsed-wave tissue Doppler. RV end-diastolic area (RVEDA) and RV end-systolic area (RVESA) were estimated from the apical four-chamber view centered on the RV. The right ventricle fractional area change (RVFAC) was defined and calculated as follows: (RVEDA − RVESA)/RVEDA × 100%.
Based on the current guidelines, 17 the estimated TRV and right atrial pressure (RAP) were used to calculate the pulmonary arterial systolic pressure (PASP) according to the simplified Bernoulli equation (PASP = 4 × TRV 2 + RAP). Patients had a suspected diagnosis of SLE-PAH if PASP≥36 mmHg was assessed by transthoracic echocardiography or was confirmed by RHC. 16
Three-dimensional echocardiography
Adequate 3DE data sets were stored digitally on hard disks for off-line analysis by a quantification system (3DQ software package; QLAB version 12.0; Philips Healthcare). 3D RV volumes and functional indices including RVEDV, RVESV, and RVSV were automatically analyzed and obtained by the QLAB quantification system. RVEF was calculated with the following formula: RVEF = (RVEDV-RVESV)/RVEDV × 100%.
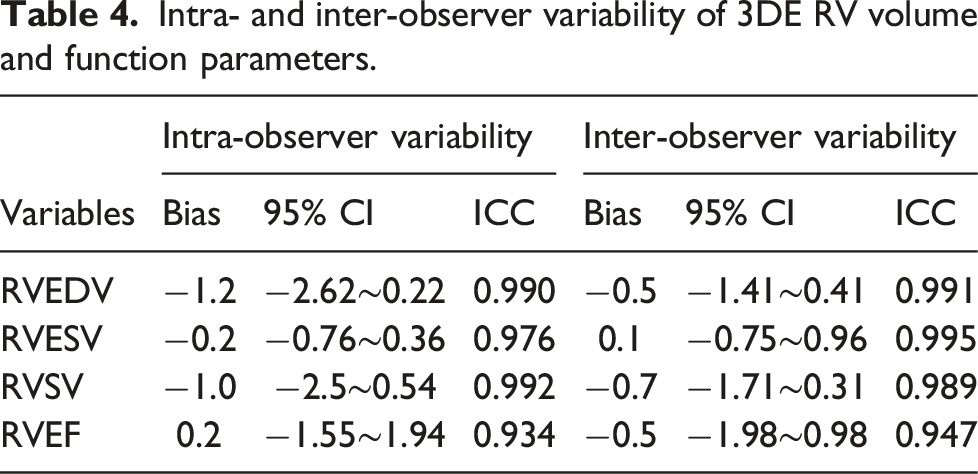
To assess intra- and interobserver variabilities of RV volumes, measurements were re-evaluated in 10 randomly selected patients using Bland–Altman analyses performed by two independent cardiologists.
Statistical analysis
SPSS version 26 software (IBM Corporation, Armonk, NY, United States) and MedCalc version 20 software were used to perform all statistical analyses. The Kolmogorov‒Smirnov test was used to determine the distribution. Continuous variables are reported as the mean ± standard deviation and categorical variables are reported as percentages (frequencies). Comparisons between SLE-PAH patients and control groups were performed using the independent-samples test or Mann–Whitney test for continuous variables, as appropriate, whereas the χ2 test or Fisher’s exact test was used for categorical variables, as appropriate. One-way ANOVA or the Kruskal‒Wallis test was used to compare variables among three groups, and post hoc analysis by Scheffe’s method was performed between groups. Correlations between the RVSV/RVESV ratio and clinical or RV functional parameters were evaluated by the Pearson correlation coefficient or Spearman rank correlation coefficient, as appropriate. Receiver-operator characteristic (ROC) curves were generated for the SV/ESV ratio to determine the area under the curve (AUC), specificity and sensitivity of the optimal cutoff value for the prediction of clinical outcomes. Cumulative event rates were determined by Kaplan–Meier analyses with differences between groups using the log-rank test. Bland–Altman analyses were performed to assess interobserver and intraobserver agreements. For all analyses, a two-tailed p value <.05 was considered statistically significant.
Results
Patient demographics and clinical characteristics
Baseline clinical characteristics of patients in SLE-PAH.
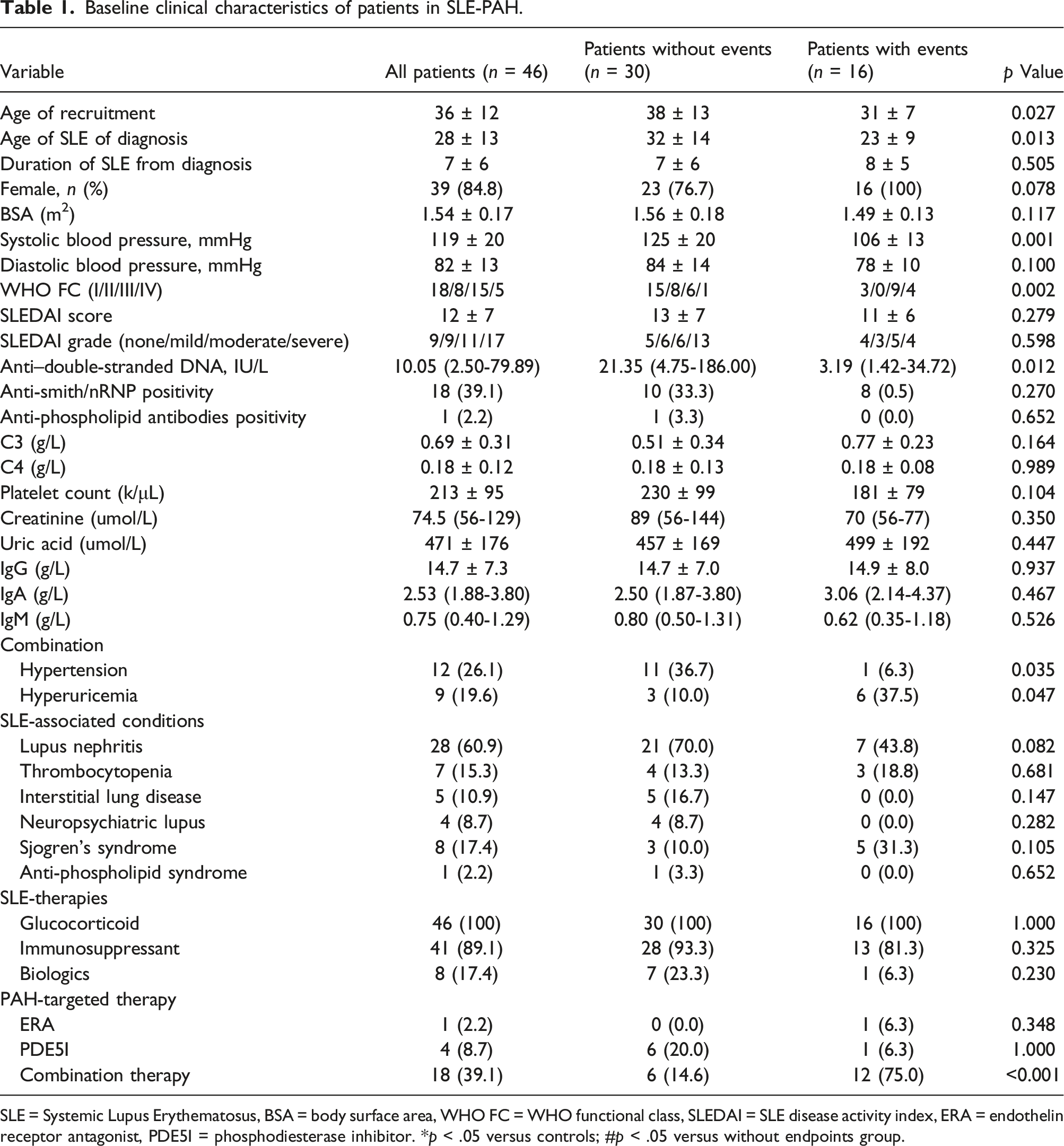
SLE = Systemic Lupus Erythematosus, BSA = body surface area, WHO FC = WHO functional class, SLEDAI = SLE disease activity index, ERA = endothelin receptor antagonist, PDE5I = phosphodiesterase inhibitor. *p < .05 versus controls; #p < .05 versus without endpoints group.
A total of 100% and 89.1% of patients were treated with glucocorticoid and immunosuppressant therapy, respectively. A total of 8 (17.4%) patients received biological agent treatment. At the time of enrollment, 23 patients (50%) had been treated with PAH-targeted therapy: 2.2% received endothelin receptor antagonists (ERAs), 8.7% received phosphodiesterase inhibitors (PDE5is), and 39.1% received combination therapy.
Comparison of baseline characteristics of patients with and without endpoints
The cohort of 46 patients with SLE-PAH was followed for a median of 24 months (IQR 18–31). The time of baseline echocardiography to the development of clinical outcome constituted a median of ∼18 months (IQR 3–25) for 16 patients (34.7%) who experienced the clinical outcome; specifically, 6 (13.0%) patients died; 6 (8.3%) patients had PAH-related hospitalization with increased RV failure; and 4 (6.7%) patients had upgraded PAH drug therapy with intravenous prostacyclin.
The enrolled patients were divided into two groups based on whether an endpoint event occurred. Compared with male patients, older patients and young female patients had a higher risk of developing clinical events. Patients who experienced an endpoint event had a worse WHO FC (p = .002), a lower level of anti-dsDNA (p = .012), and a higher proportion of patients with hyperuricemia (p = .047) and hypertension RV (p = .035) than those who did not experience an endpoint event. In addition, we found that patients with a combination of PAH-targeted drugs at baseline had a higher risk of experiencing an endpoint event than patients with a single PAH-targeted drug (p < .001). The comparison of baseline characteristics of the overall population that did and did not experience an endpoint event is summarized in Table 1.
Comparison of right ventricular remodeling in patients with and without endpoints
Echocardiographic characteristics in healthy control subjects versus SLE-PAH patients with and without endpoint events.
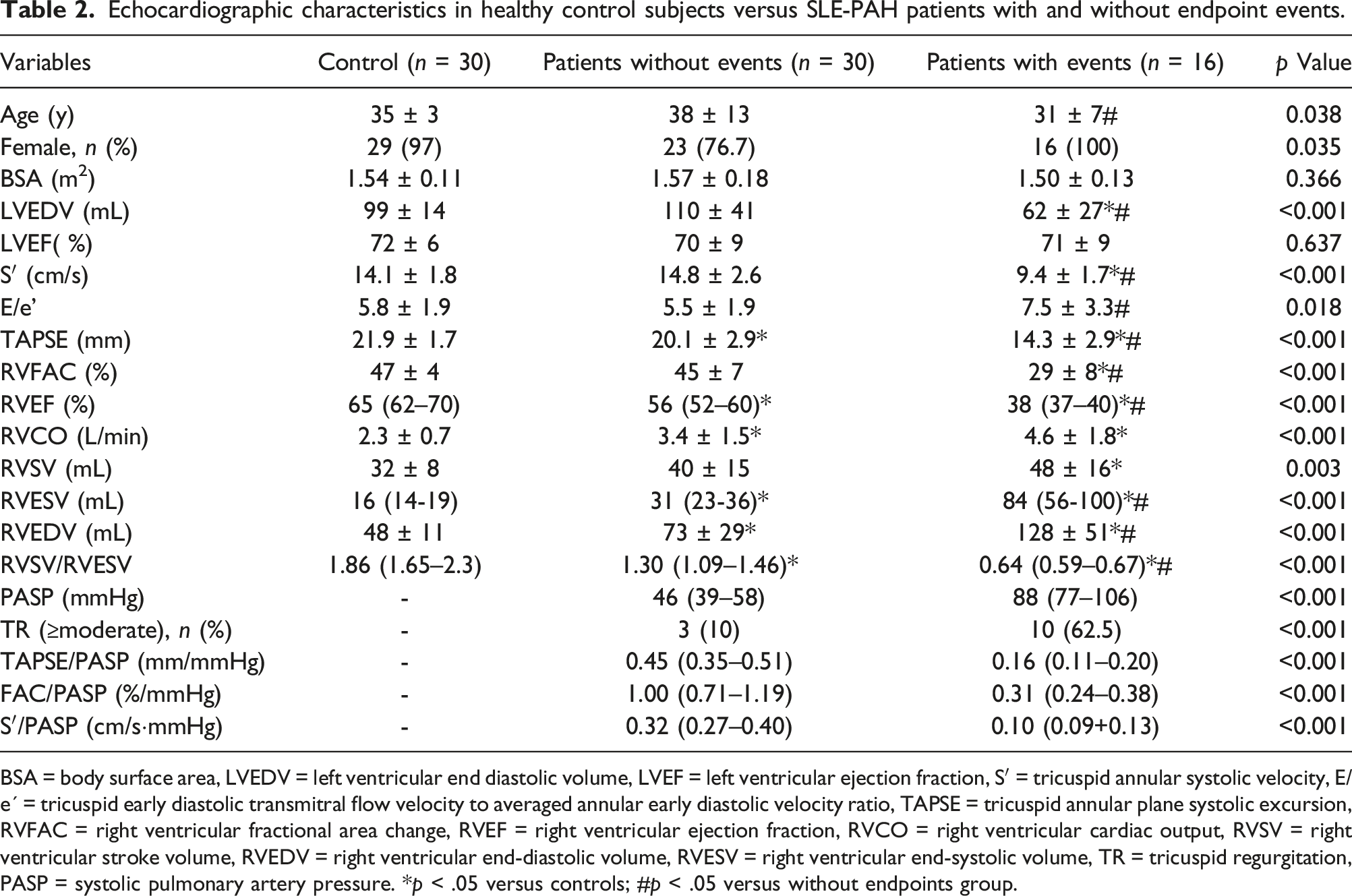
BSA = body surface area, LVEDV = left ventricular end diastolic volume, LVEF = left ventricular ejection fraction, S′ = tricuspid annular systolic velocity, E/e´ = tricuspid early diastolic transmitral flow velocity to averaged annular early diastolic velocity ratio, TAPSE = tricuspid annular plane systolic excursion, RVFAC = right ventricular fractional area change, RVEF = right ventricular ejection fraction, RVCO = right ventricular cardiac output, RVSV = right ventricular stroke volume, RVEDV = right ventricular end-diastolic volume, RVESV = right ventricular end-systolic volume, TR = tricuspid regurgitation, PASP = systolic pulmonary artery pressure. *p < .05 versus controls; #p < .05 versus without endpoints group.
In addition, RV diastolic functional impairments were found in the endpoint event group, as expressed by the lower tricuspid E/e' ratio (5.5 ± 1.9 vs 7.5 ± 3.3, p < .018). There were significant differences in PASP in SLE-PAH patients (p < .001).
Relationship between right ventricular arterial coupling ratio and echocardiographic parameters and clinical parameters
Correlation between the SV/ESV ratio, WHO functional class and clinical parameters and echocardiographic parameters.
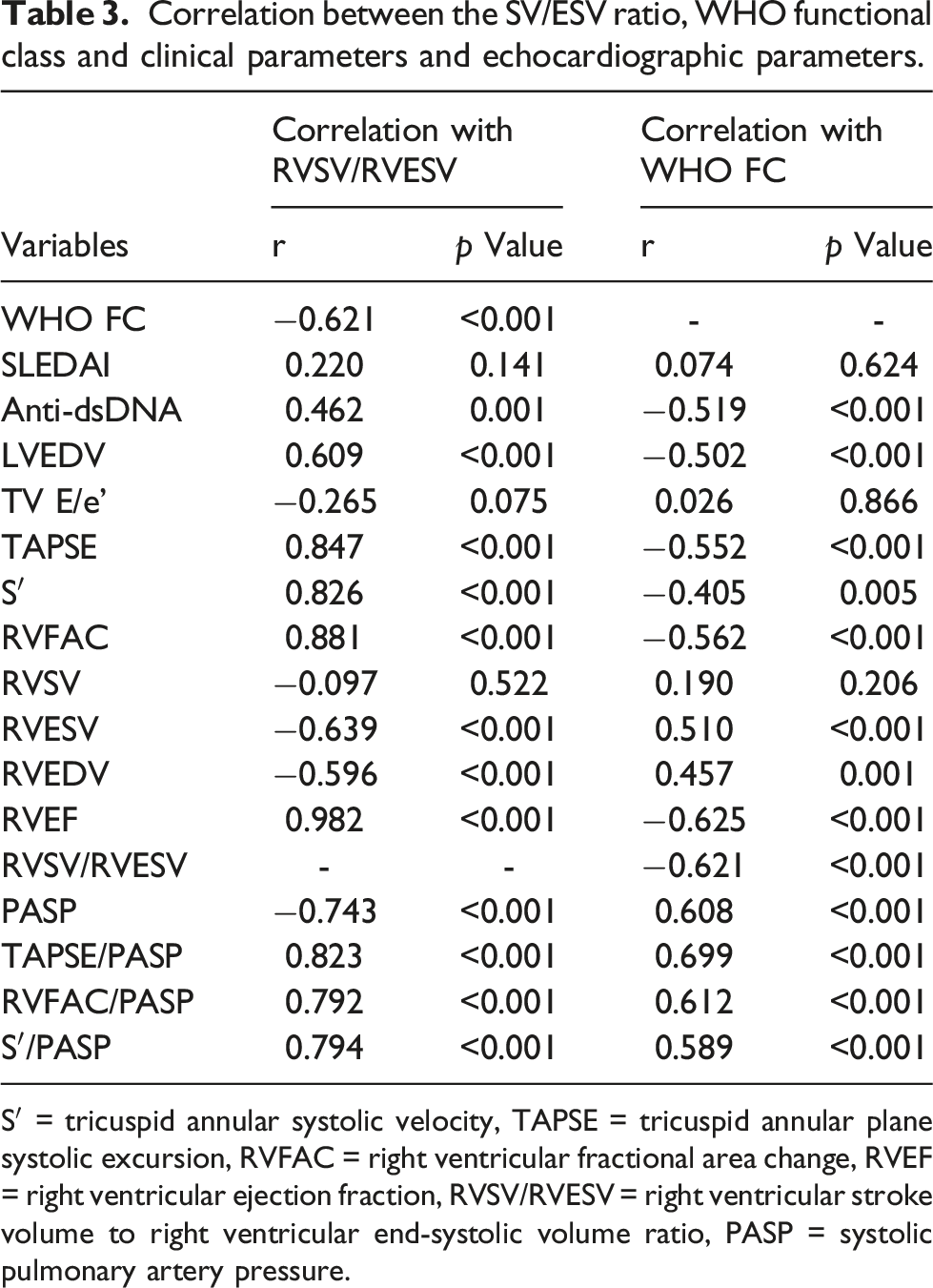
S′ = tricuspid annular systolic velocity, TAPSE = tricuspid annular plane systolic excursion, RVFAC = right ventricular fractional area change, RVEF = right ventricular ejection fraction, RVSV/RVESV = right ventricular stroke volume to right ventricular end-systolic volume ratio, PASP = systolic pulmonary artery pressure.
WHO FC was negatively correlated with conventional RV functional parameters (TAPSE, TV-S′, RVFAC, and RVEF), with WHO FC being the most strongly correlated with RVEF, with a negative correlation (R = −0.625, p < .001). However, there was no correlation between WHO FC and SLEDAI scores, which was not statistically significant.
Diagnostic efficacy of the 3D right ventricular stroke volume/right ventricular end-systolic volume ratio for clinical outcome
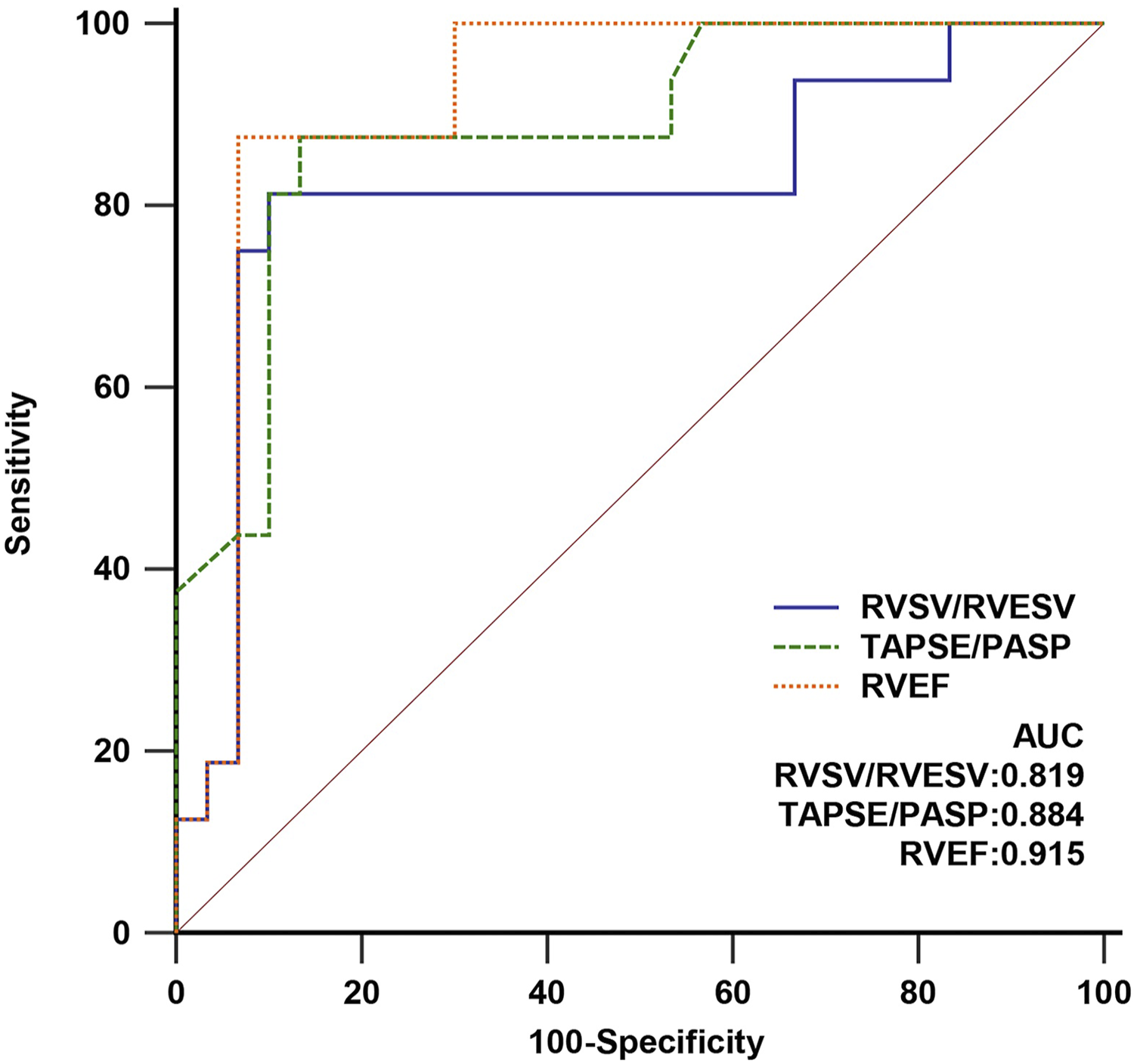
We analyzed the ability of the RVSV/RVESV ratio to discriminate clinical endpoints using ROC analysis (Figure 1). The ROC curve showed that the optimal cutoff for RVSV/RVESV was 0.712, with an area under the ROC curve of 0.819, sensitivity = 81.3%, and specificity = 86.7%. We also plotted the ROC curves for RVEF and TAPSE/PASP (Figure 2): (1) the best cutoff value for RVEF was 46%, the area under the curve was 0.915, sensitivity = 87.5%, and specificity = 93.3%; (2) the best cutoff value for TAPSE/PASP was 0.24, the area under the curve was 0.884, sensitivity = 87.5%, and specificity = 86.7%. There was no statistically significant difference in diagnostic efficacy between the RVSV/RVESV, RVEF and TAPSE/PASP groups. Receiver-operating characteristic curve for the RVSV/RVESV ratio. The optimal cutoff was 0.712 (sensitivity = 81.3%; specificity = 86.7%; area under the curve = 0.819). RVESV, right ventricular end-systolic volume; RVSV, right ventricular stroke volume. Receiver-operating characteristic curve for RVSV/RVESV, RVEF, and TAPSE/PASP. RVESV, right ventricular end-systolic volume; RVSV, right ventricular stroke volume; RVEF, right ventricular ejection fraction; TAPSE, tricuspid annular plane systolic excursion; PASP, systolic pulmonary artery pressure.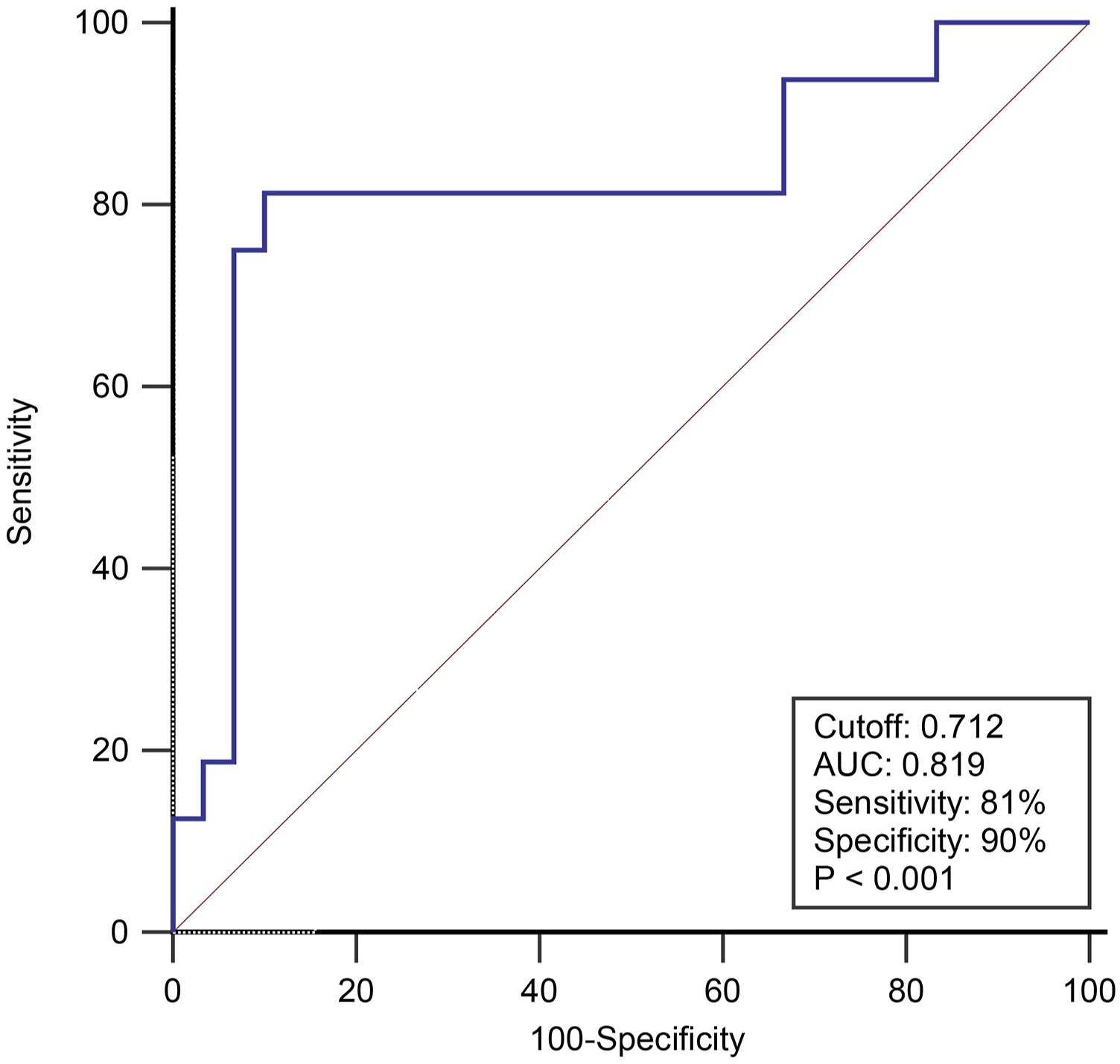
SLE-PAH patients stratified by an ROC dichotomous cutoff value of <0.712 (log-rank p < .001) for RVSV/RVESV showed highly significant differences in Kaplan‒Meier survival curves (Figure 3). The Kaplan‒Meier survival curve showed that an RVSV/RVESV ratio > 0.712 was associated with more favorable long-term outcomes. RVESV, right ventricular end-systolic volume; RVSV, right ventricular stroke volume.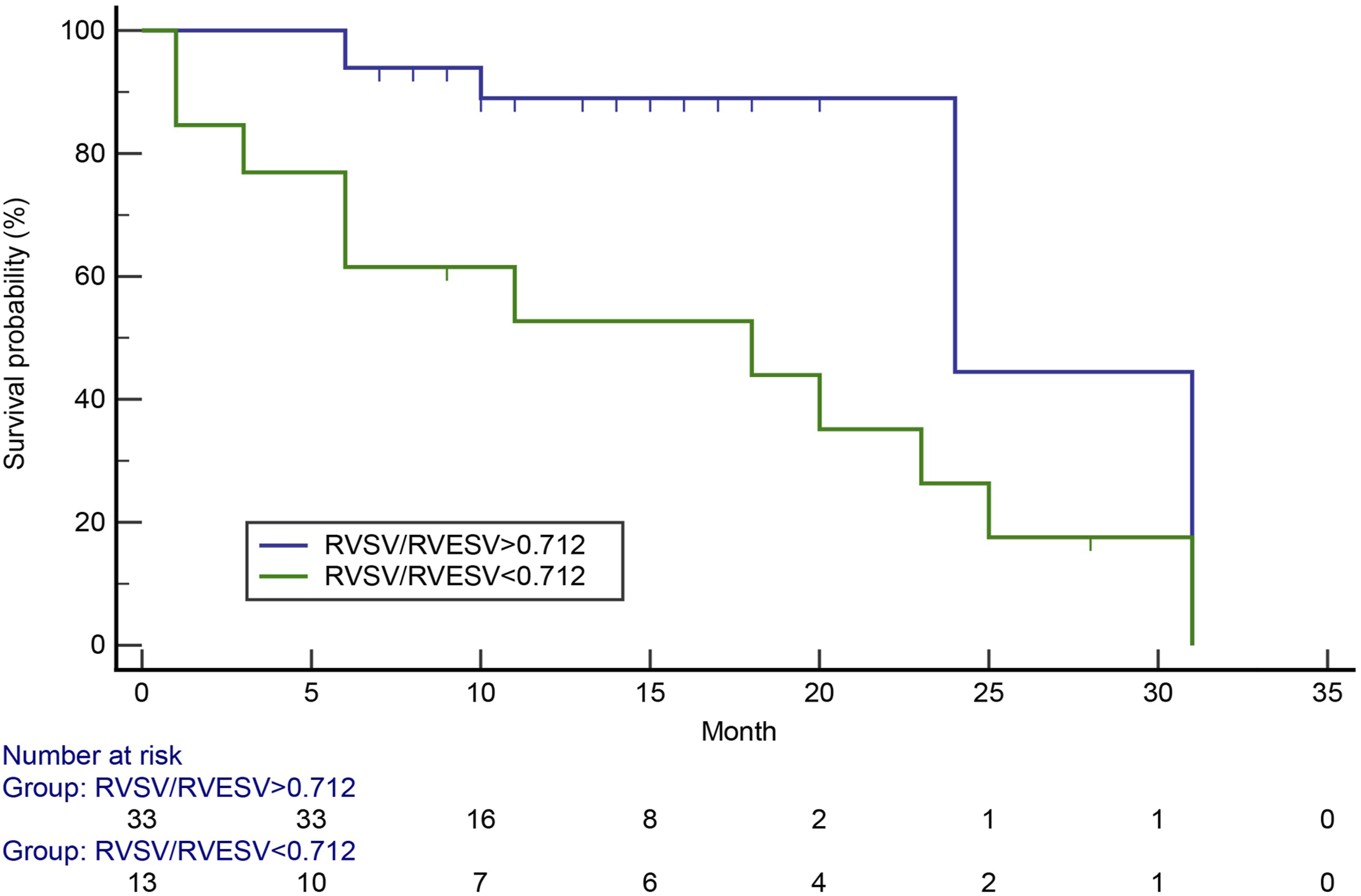
Reproducibility
Intra- and inter-observer variability of 3DE RV volume and function parameters.
Discussion
In this study, we investigated a novel index for the quantification of RV-PA coupling derived from 3D echocardiography. The main findings of our study can be summarized as follows: (1) in patients with SLE-PAH, RV systolic dysfunction was significantly impaired compared with healthy control subjects, and patients with SLE-PAH who experienced endpoint events exhibited more significant WHO FC worsening, reduced levels of anti-dsDNA, greater propensity to apply combination targeted therapy, compromised RV systolic and diastolic function, and impaired coupling; and (2) 3D RVSV/RVESV ratio as a simple noninvasive and reproducible proxy of RV-PA coupling has good diagnostic efficacy for predicting endpoint events.
SLE has been recognized as a major underlying phenotype of connective tissue disease-associated pulmonary arterial hypertension (CTD-PAH) in China. 2 Long-term inflammation and a dysregulated immune system play crucial roles in multiple forms of cardiovascular disease and the pathogenesis of SLE. 18 From a pathophysiological point of view, myocardial ischemia, endothelial dysfunction, ventricular or pulmonary vascular remodeling, and fibrosis pulmonary vascular resistance (PVR) increase, many factors lead to right heart failure, and patients eventually die. 19 Compromised ventricular function in SLE is a recognized predictor of long-term adverse cardiovascular events and clinical outcomes.18,20–23 Specifically, in SLE-PAH, RV dysfunction has been described in terms of impaired systolic and diastolic performance and RV-PA uncoupling.5,22
The invasive right heart catheterization (RHC) measurement remains the gold standard of RV-PA coupling, which analyses the ratio of end-systolic elastance to pulmonary arterial elastances (Ees/Ea) by RV pressure‒volume loops. 10 When Ees/Ea remained at normal values of 1.5 to 2 under resting conditions, RV exhibited RV contractility with the afterload remaining coupled. However, the ratio decreases from normal to <0.8, substantial RV maladaptive remodeling occurs, the RV exhibits eccentric dilatation, worse systolic and diastolic function, and reduced ejection fraction.24,25 The RVSV/RVESV ratio as a novel noninvasive surrogate for Ees/Ea was at least as useful as Ees/Ea in distinguishing pending RV maladaptation.13,14,26
3DE overcomes the limitations of routine 2D echocardiography, quantifies RV geometry and function, and further calculates RV volumes and EF. In the present study, deterioration echocardiography parameters of SLE patients including TASPE, TV-S′, RVFAC, and RVEF indicated RV dilatation and RV dysfunction, especially for the patients in the endpoint event group.
Our study found that the RVSV/RVESV ratio of patients with endpoint events was markedly reduced (0.64 (0.59–0.67)), which implied RV-PA uncoupling and was a sign of RV maladaptation and functional decompensation.
Furthermore, the RVSV/RVESV ratio derived from 3DE was verified to be an outstanding indicator to discriminate endpoint events in the SLE population. Using a cutoff of RVSV/RVESV <0.712, we found that patients were more likely to develop clinical outcomes. This ratio is sensitive and specific in detecting clinical outcomes in SLE-PAH patients. More recently, Axell et al 27 defined the Ees/Ea in either animal models or patients with chronic thromboembolic PH as approximately 0.7, which is the same as the cutoff we identified. In PAH, RVSV/RVESV and RVEF derived from cardiac magnetic resonance imaging were the best independent predictors of outcome; an SV/ESV ratio < 0.534 demonstrated a risk of death at 2 years. 28 A cutoff value for RVSV/RVESV was approximately 0.54, which has been proven to be a predictor of poor prognosis in pediatric patients with PH. 13 The cutoff values of the RVSV/RVESV ratio are comparable in both of the above studies (0.534 and 0.52) which are much lower than the cutoff value in our study. One possible explanation for this finding is that the etiologies of diseases, severity of the diseases, and the small sample size included in the study differed.
Previous studies have demonstrated that the TAPSE/PASP ratio is a crucial surrogate for describing RVPAC and emerged as a prognostic marker of Ees/Ea by RHC.29–31 Importantly, the TAPSE/PASP ratio has been incorporated into the 2022 ESC/ERS PAH guidelines for comprehensive risk assessment. Our study also showed no significant difference in diagnostic efficacy between the three groups of RVSV/RVESV, RVEF, and TAPSE/PASP, suggesting that the RVSV/RVESV ratio has equally good diagnostic efficacy as the classical predictors (RVEF and TAPSE/PASP). Vanderpool et al 14 found that RVSV/RVESV may be more sensitive than RVEF to changes in response to RV function in patients with severe pulmonary hypertension.
In our study, the RVFAC/PASP and tricuspid annular systolic velocity (S′ or TASV)/PASP ratios were also considered indices of RVPAC, and the ratios were significantly lower compared with in patients without endpoint events. The ratios of RVFAC to RV systolic pressure (RVSP) or PASP (RVFAC/RVSP or RVFAC/PASP) have been proven to be of superior prognostic factor than conventional RV systolic function in chronic pulmonary regurgitation patients. 32 In addition, Jentzer et al described the relationship between the lower S′/RVSP ratio and short-term or long-term mortality in cardiac intensive care unit patients. 33 The latest research shows that a low S′/RVSP ratio value can indicate right RVPA uncoupling and impaired functional status in hypertrophic cardiomyopathy patients. 34 Thus far, there are no studies examining the relationship between RVFAC/PASP or RVSP, S′/PASP or RVSP, and Ees/Ea, and more in-depth research needs to be explored.
Therefore, early screening for diagnosis of PAH in patients with SLE is critical for clinical selection of treatment options, and guidelines recommend transthoracic echocardiography as the main method. TRV is currently most commonly used to assess onset of PAH, and reduced RVFAC and TAPSE, elevated right ventricular myocardial work index (RV Tei index), and pericardial effusion are indicative of the extent of PAH. Echocardiographic RVPAC may be a convenient non-invasive and sensitive marker of RV function and early diagnosis of PAH. The 6th World Symposium on Pulmonary Hypertension (WSPH) released a new definition of PAH as post-capillary pulmonary hypertension, which requires mPAP >20 mmHg, Pulmonary arterial wedge pressure (PAWP)≤15 mmHg, and PVR ≥3 WU.4,35 For patients with CTD-PAH, a lower mPAP threshold in the definition of PAH may facilitate realization of early screening and early intervention, and it is recommended to appropriately increase the frequency of screening and to closely observe the degree of disease progression.
The principle of CTD-PAH treatment is to provide early and individualized treatment to maximize the delay of disease progression, minimize organ damage, and ultimately prolong the patient’s survival, improve their quality of life, and improve prognosis to achieve the “double standard” for CTD and PAH.4,36 SLE-PAH-specific therapeutic agents include glucocorticoids, immunosuppressants, and targeted drug therapy. Use of high-dose glucocorticoids in combination with immunosuppressive agents has been shown to be effective in controlling or even “curing” PAH in the early stages of the disease and in those with active disease, especially in patients with SLE or mixed CTD-PAH.37,38 The results of the CSTAR multicenter prospective cohort study on SLE-PAH showed that PAH was achieved earlier with intensive immunosuppressive therapy and the long-term prognosis was significantly improved. 39 Targeted agents have greatly improved the prognosis of patients with PAH, with most phase II/III clinical studies of targeted agents for PAH enrolling a significant proportion of patients with CTD-PAH and with significant benefit in CTD-PAH subgroup analyses in CTD patients.4,40–43 Studies have demonstrated that biologics such as belimumab have a favorable and reliable therapeutic effect in SLE and an acceptable safety profile in long-term studies, but it is mainly works effective in patients with lupus nephritis, and its efficacy on the cardiopulmonary system is unclear. 44
Cohort studies have confirmed that the PAH Risk Stratification Scale is a good predictor of PAH regression in patients with SLE-PAH. 45 Therefore, it is recommended that patients with CTD-PAH should agree to targeted drug monotherapy or combination therapy according to PAH risk stratification, and adjusting the treatment regimen according to PAH risk stratification during regular follow-up is needed to ultimately achieve “low-risk status.” In conclusion, the RVSV/RVESV ratio not only includes information on the RVEF response to RV function and is less dependent on RV preload but also helps to reflect the overall cardiopulmonary vascular interaction status and the effect of RV afterload on RV in patients with PAH. The predictive value of this index in the clinical prognosis of SLE-PAH patients and the evaluation of its efficacy need further study.
Limitations
First, the majority of patients in this study relied on echocardiography to diagnose the occurrence of PAH, and RHC remains the gold standard for the diagnosis of PAH; echocardiographic RV-PA coupling in the current study is based on 3DE, and its reliability has not been widely accepted, and further comparative studies with RHC are needed. Second, the combination targeted therapy regimen was implemented individually for each patient in this study, with different drug doses and frequencies between individuals. Third, due to the small sample size and the number of cases with clinical endpoint events included in this study, regression analysis could not be performed to establish a predictive model to analyze the risk factors for the occurrence of endpoint events in SLE-PAH. Therefore, further studies with larger and multicenter populations should extend the follow-up period and confirm these results.
Conclusion
In conclusion, our data support that the 3DE-derived RVSV/RVESV ratio is a noninvasive alternative to RV-PA coupling for early assessment of RV functional status, identification of RV myocardial involvement and detection of subclinical cardiac insufficiency in patients with SLE-PAH, and is an eximious indicator for identifying endpoint events in SLE-PAH, which can provide a diagnostic basis for clinical intervention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fund of Guangxi Medical and Health Appropriate Technology Development and Promotion Application (S2020030), the National Natural Science Foundation of China (82060051), and the Guangxi Medical “139” Program for Training High-level Backbone Talents (G201903053).