
Abstract
Background
In 2017, belimumab (BEL) was approved in subcutaneous (SQ) administration. The effectiveness after switching from intravenous (IV) to SQ and patient satisfaction in daily clinical practice has not been studied. During the pandemic, patient follow-up and treatment were significantly affected, and some patients need a change from IV to SQ. Our aim was to evaluate daily clinical practice satisfaction to SQ BEL therapy in patients previously treated IV BEL. We hypothesized that SQ BEL in SLE patients previously treated with IV BEL was similar in effectiveness and conferred higher satisfaction.
Methods
Observational, multicenter study, conducted in 7 reference centers in Catalonia. We included stable SLE patients (EULAR/ACR 2019) on treatment with SQ BEL and previous use of IV BEL (at least 3 months on IV BEL before switching). Since there are no well-validated tools for SQ BEL treatment satisfaction, we used RASQ-SQ, validated in patients with lymphoma who switched from IV Rituximab to SQ treatment, and modified for BEL treatment.
Results
Twenty-seven patients were included. The more prevalent clinical manifestations observed were related to the skin and joints and the patients had a mean baseline SLEDAI of 2.96 (SD 2.4) and SLICC score of 0.67 (SD 0.88). The median time from treatment with IV BEL before switching to SQ was 21 months (range). 84% of patients reported confidence in SQ BEL. 85.2% felt that treatment with SQ BEL was convenient or very convenient. 85% felt they had gained time with the change. 89% would recommend the SQ injection to other patients. Disease activity (mean SLEDAI) and remission rates remain stable after switching. No major new adverse effects were reported.
Conclusions
Overall satisfaction, satisfaction with via of administration, and satisfaction with the time taken to receive BEL were higher for SQ BEL treatment. A switching SQ strategy is a reasonable alternative for BEL patients.
Introduction
Systemic lupus erythematosus (SLE) is a chronic and complex autoimmune disease affecting multiple systems and organs. It is characterized by a dysregulated immune response and the production of autoantibodies, leading to inflammation and tissue damage to various parts of the body, including the skin, joints, kidneys, heart, and nervous system. SLE can have a significant impact on the quality of life of affected individuals. 1
B lymphocyte stimulator (BLyS), an important cytokine for B lymphocyte survival, is overexpressed in patients with SLE. 2 Belimumab (BEL) is a monoclonal antibody that specifically targets the BLyS. By inhibiting BLyS, BEL helps regulate the abnormal B-cell activity observed in SLE, thereby reducing autoantibody production and inflammation.3,4 Approval of BEL by regulatory agencies such as the U.S. Food and Drug Administration (FDA) 5 and the European Medicines Agency (EMA) 6 has provided a new treatment option for patients with SLE. Since its approval in 2011, the intravenous (IV) formulation of BEL has been extensively used in the treatment of patients with SLE who have shown an inadequate response to conventional therapies.
In 2017, a subcutaneous (SQ) formulation of BEL received the regulatory approval, providing an alternative route of administration.7,8 The SQ formulation offers potential advantages, such as easier self-administration, increased patient convenience, and potentially reduced healthcare costs. 9 However, the effectiveness of BEL and patient satisfaction after switching from IV to SQ administration in patients with SLE require further investigations. While some studies have established the efficacy and safety of IV BEL, limited data exist regarding outcomes and patient perspectives following the transition to SQ administration.10,11 Understanding the clinical effectiveness, tolerability, and patient satisfaction associated with switching strategy is essential for optimizing SLE treatment and tailoring therapy to individual needs.
Furthermore, the COVID-19 pandemic has significantly squeezed the administration of IV biological therapies, such as BEL, seeking for the reduction of hospital visits and minimizing the risk of infection for vulnerable patients. This has led to the need for some patients to switch to SQ BEL therapy, which can be self-administered at home or by a caregiver.
Few studies have assessed patient´s satisfaction when transitioning from IV to SQ treatment in rheumatoid arthritis (RA) patients, and the available results are contradictory, depending on patient characteristics mainly in favor of the SQ route.12–16 In this context, BEST-LUPUS (BElimumab Switching Therapy in patients with well controlled systemic LUPUS erythematosus) aimed to explore the effectiveness and patient satisfaction of switching from IV to SQ BEL administration in patients with SLE. By assessing disease activity, treatment response, and patient-reported outcomes (PROs), we aimed to provide valuable insights into clinical outcomes and patient experiences with the SQ formulation.
Methods
Patient selection
A multicenter observational study was conducted, collecting data from 7 different rheumatology departments from reference centers in Catalonia, Spain, between September and December 2022. The study enrolled stable SLE patients (EULAR/ACR 2019 criteria) 17 who had been receiving treatment with SQ BEL and had previously received at least 3 months of treatment with IV BEL before switching to SQ administration.
Data collection
Patient demographic and clinical data were collected, including age, gender, disease duration, SLE disease activity, organ involvement, and previous and concomitant medications, including glucocorticoids use. Disease activity was assessed using the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI). 18 Cumulative damage was assessed using the Systemic Lupus International Collaborating Clinics Scale (SLICC). 19 Data recorded in the patients electronic medical records during their last visit, meanwhile BEL was administered IV, were retrospectively collected. In addition, data recorded at 3, 6, and 12 months after the switch to SQ BEL in those patients who met the required time frame were collected retrospectively. Clinical and laboratory data from the last visit with SQ BEL, as well as satisfaction data related to the switch, were collected during the patient enrollment visit.
Given the lack of well-validated tools for assessing treatment satisfaction specifically in patients receiving SQ BEL treatment, we employed the use of the Rituximab Subcutaneous Administration Satisfaction Questionnaire (RASQ-SQ). 20 The RASQ-SQ has been previously validated for assessing treatment satisfaction in patients with lymphoma who transitioned from IV rituximab to SQ treatment. Recently, we evaluated the utility of RASQ-SQ in RA patients who transitioned from IV to SQ rituximab treatment with satisfactory results. 21 To adapt the questionnaire for BEL treatment, we made necessary modifications to ensure its relevance and applicability [supplementary material].
The RASQ-SQ consists of a 17 structured questions designed to evaluate various aspects of treatment satisfaction, including convenience, comfort, injection site reactions, and overall treatment preference. It assesses both objective measures, such as the ease of self-administration and the occurrence of injection site reactions, as well as subjective measures, including patient-reported preferences and satisfaction levels.
Statistical analysis
Descriptive analysis was carried out according to the distribution of the categorical and quantitative variables. Statistical analysis was done using IBM SPSS Statistics for Windows v27 (IBM Corp., Armonk, NY). Ethical approval was obtained (HCB20211187), and all participants provided informed consent prior to study enrollment.
Results
Patient characteristics
A total of 27 patients were included, with 85.2% being female and having a mean age of 45.9 ± 12.5 years Figure 1 summarizes the study design with the number of patients included in each of the visits recorded. Study design overview. SLE: systemic lupus erythematosus. IV BEL: intravenous belimumab. SQ BEL: subcutaneous belimumab. N: number of patients. RAS-SQ: modified Rituximab Subcutaneous Administration Satisfaction Questionnaire for belimumab.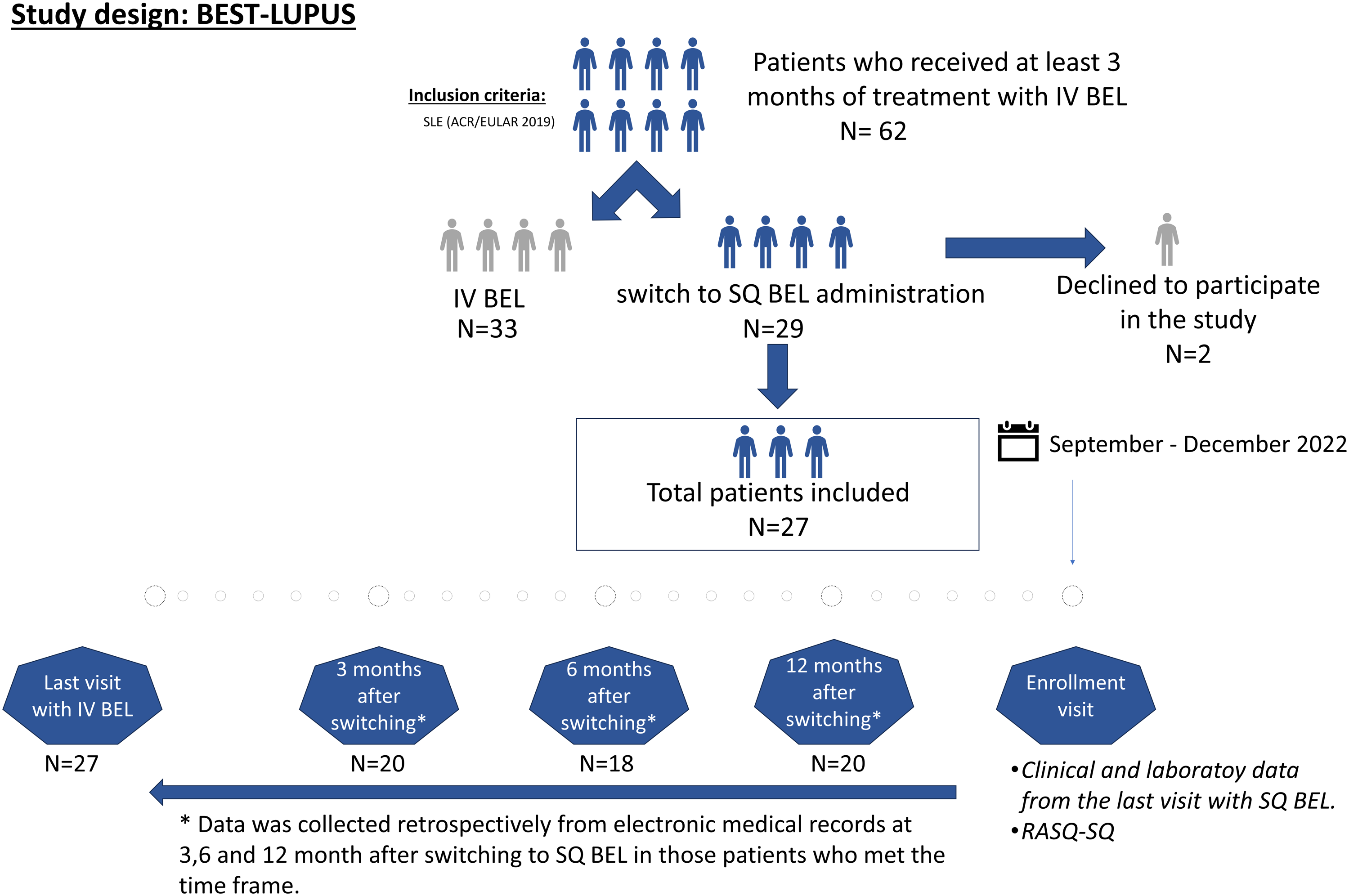
General characteristics.
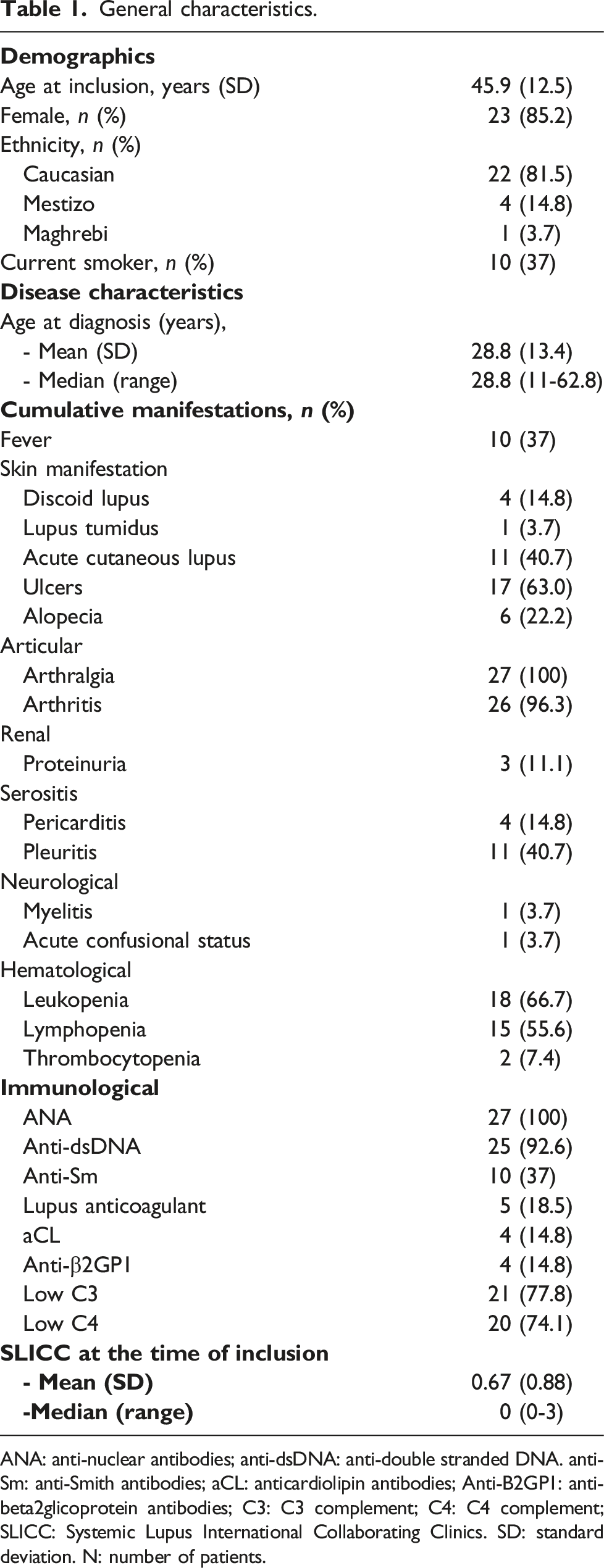
ANA: anti-nuclear antibodies; anti-dsDNA: anti-double stranded DNA. anti-Sm: anti-Smith antibodies; aCL: anticardiolipin antibodies; Anti-B2GP1: anti-beta2glicoprotein antibodies; C3: C3 complement; C4: C4 complement; SLICC: Systemic Lupus International Collaborating Clinics. SD: standard deviation. N: number of patients.
Clinical evaluation after switching
Evaluation of disease activity measured by SLEDAI and concomitant medication at the moment of the last IV belimumab, 3, 6, and 12 months of SQ belimumab and the las visit with SQ belimumab.
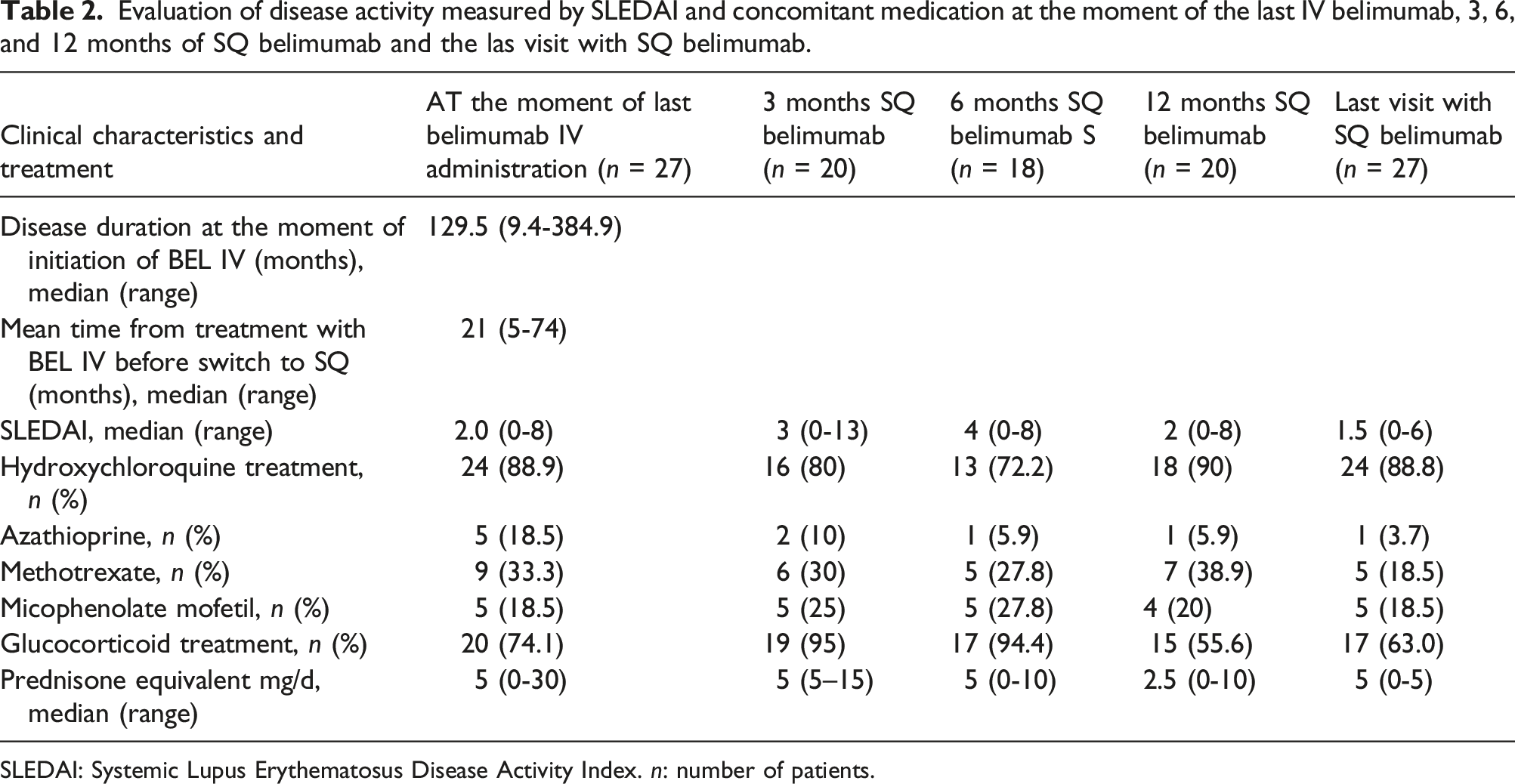
SLEDAI: Systemic Lupus Erythematosus Disease Activity Index. n: number of patients.
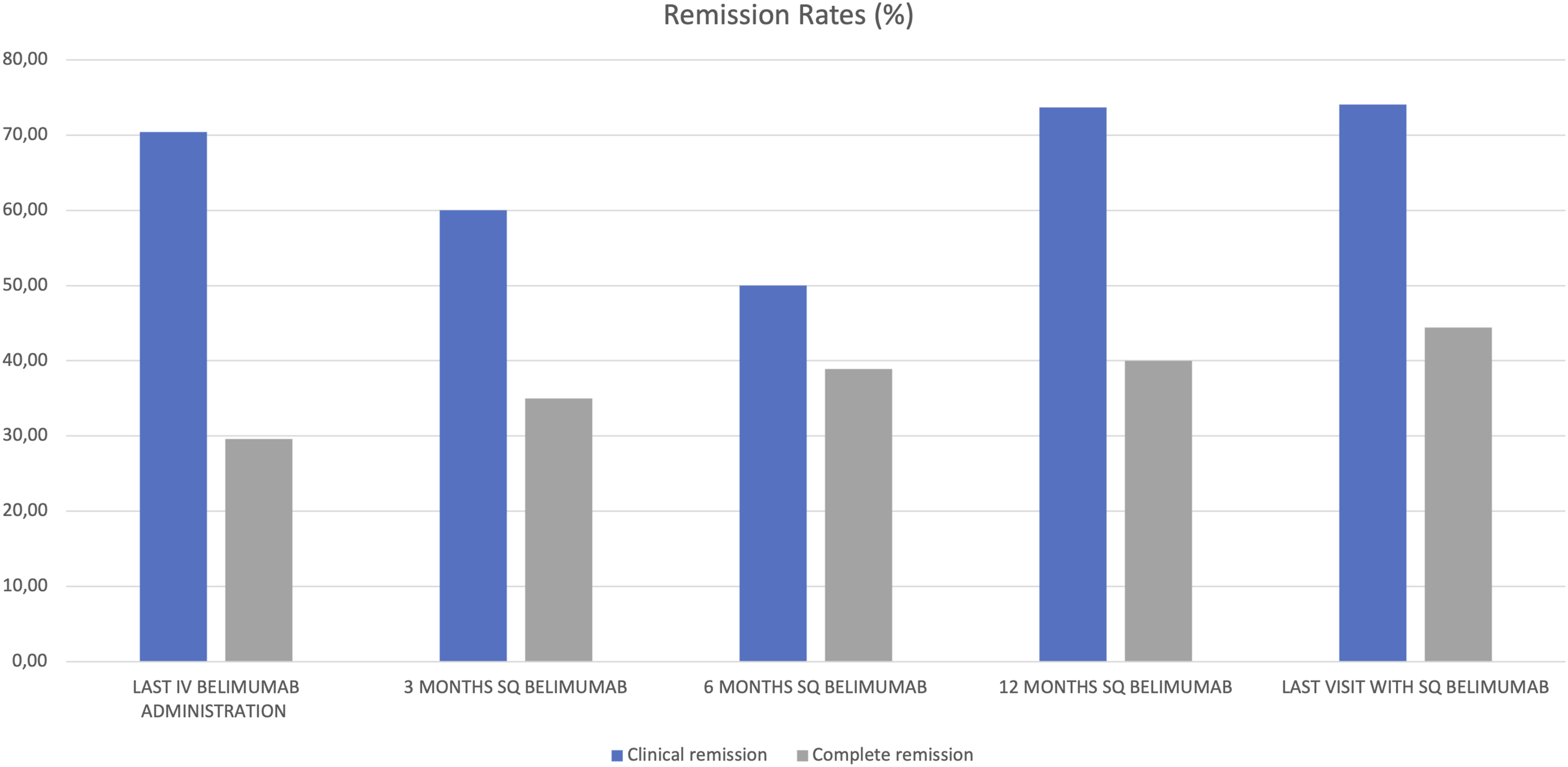
Remission rates at the moment of the last IV belimumab, 3, 6, and 12 months of SC belimumab and the las visit with SQ belimumab. Clinical remission: clinical-SLEDAI = 0 and <5 mg/d prednisolone (or equivalent); Complete remission: SLEDAI = 0 and <5 mg/d prednisolone (or equivalent).
Patients’ satisfaction
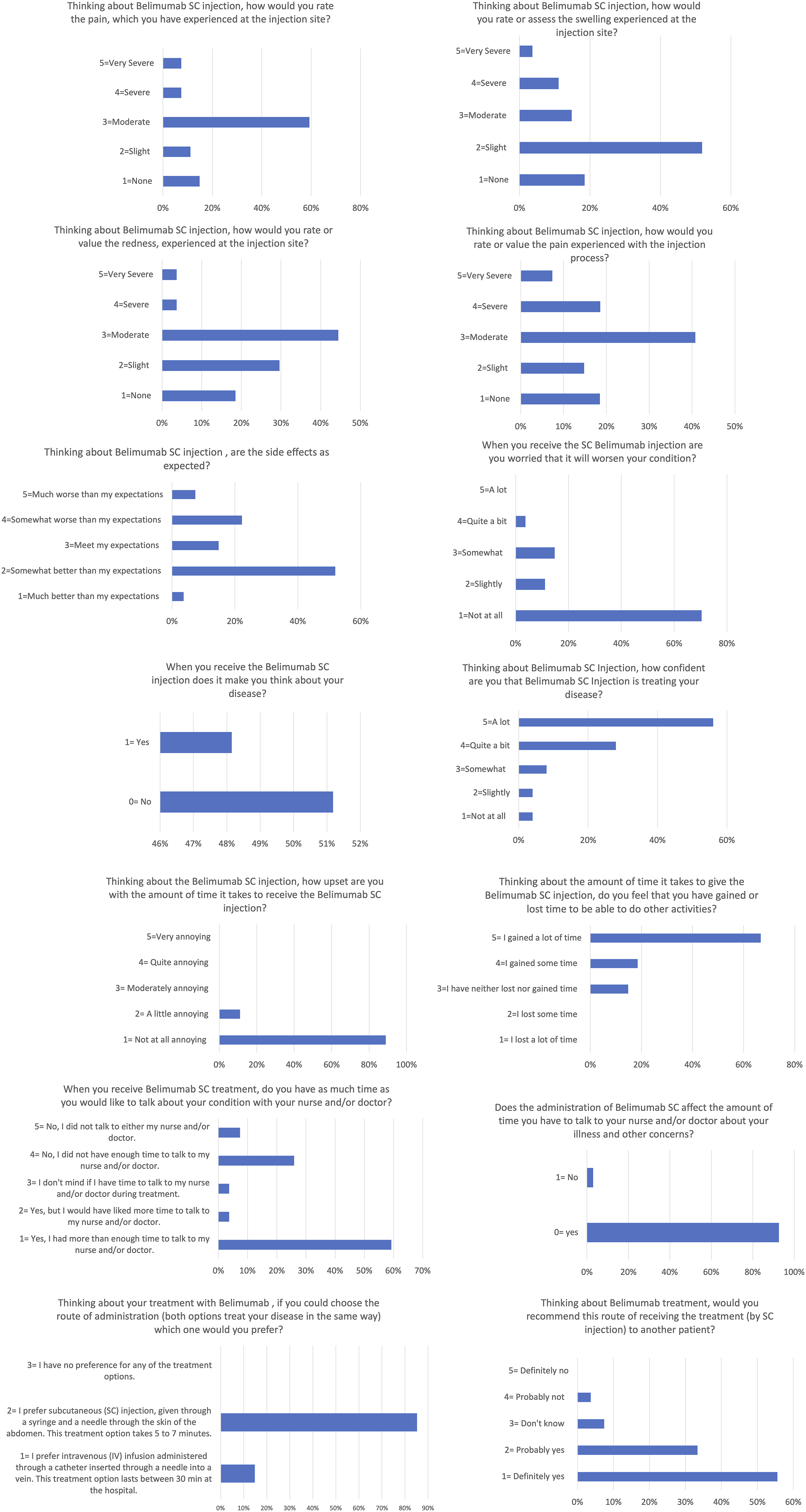
Patient satisfaction with the shift was very high. In total, 80% of the patients were satisfied with the change (Figure 3). More than 85% of patients reported that the treatment with SQ BEL was convenient or very convenient, and 84% reported confidence in SQ BEL. Furthermore, 81% of patients did not feel restricted by the treatment, and 85% felt they had gained time with the change. Additionally, nearly 90% of patients did not find the time it took to administer the treatment bothersome. Regarding injection problems, only a few patients reported moderate, severe, or very severe issues related to the injection. However, when asked if these problems were as expected, 29.6% found that the injection-related issues were worse than expected. One of the negative aspects reported by patients was that they found SQ administration modified the former relationship between patients and healthcare personal for illness issues and concerns. However, 85.2% of the patients preferred SQ treatment (Figure 4, supplementary material). Question 1 of the modified RASQ-SC for belimumab results shown are percentages of patients. Graphical representation of questions 2-17 of the modified RASQ for belimumab. Results shown are percentages of patients.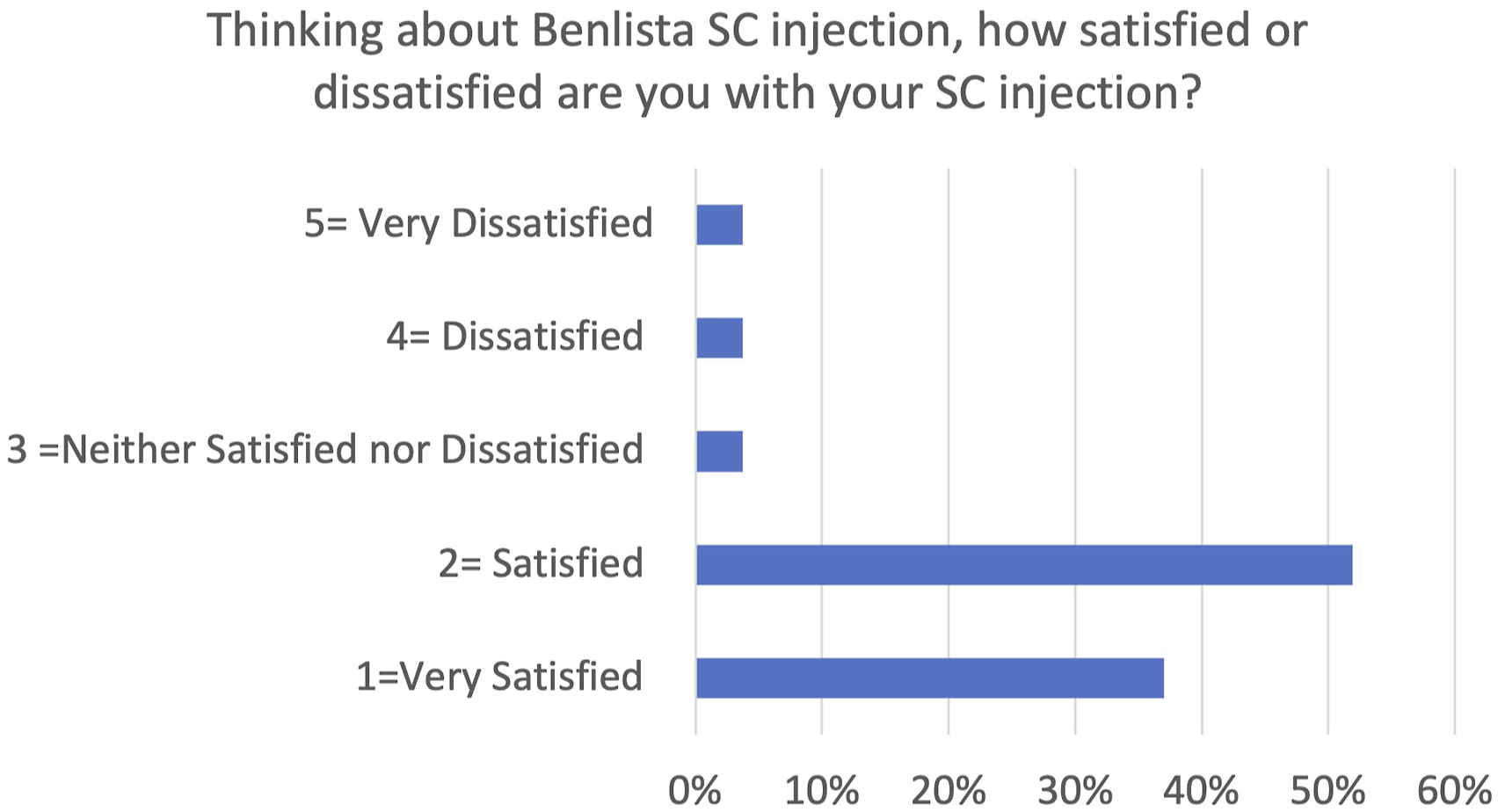
Discussion
Our study reveals that overall satisfaction, satisfaction with the route of administration, and satisfaction with the time taken to receive BEL are high for SQ BEL treatment.
Patient satisfaction plays an important role in the effectiveness of treatment in chronic inflammatory diseases, such as SLE.22,23 Therefore, it is very important to actively include patients in therapeutic decisions. 24 Patient satisfaction affects adherence to treatment, engagement in self-care, and overall quality of life. Taking into account patient´s satisfaction, physicians and healthcare professionals can improve the patient–physician relationship and provide better patient care. 25
Since its approval, BEL has become an important therapeutic tool for patients with SLE. 26 Previous studies have demonstrated the effectiveness of both IV and SQ administration. However, there is no evidence for the clinical outcomes of patients switching from IV to SQ BEL. This study provides information on patient treatment satisfaction after switching to SQ BEL application. SQ therapy offers many potential advantages compared to IV treatments. This is even more important during times such as the COVID-19 pandemic, when hospital visits increase the risk of infection and limited access to the facilities. By choosing for SQ therapy, patients can minimize their visits to infusion centers, lowering the risk of hospital-acquired infections and reducing their exposure to COVID-19 during travel.
BEST-LUPUS study confirmed that a vast majority of patients (88%) were generally satisfied with the change in the treatment route of administration showing confidence in the medication (84%). Another point to highlight from our study was the patient’s perception of having gained time with the change of the route of administration. By reducing time invested in hospital attendance, patients save time and may follow with their active life, performing their daily activities more comfortably. This can have a positive impact on patient’s mental and emotional well-being as well as their ability to participate in social and work activities. Tolerability was high. In most cases, the pain, redness, and swelling experienced were mild or slight. Furthermore, these patients did not experience worsening of disease activity, reinforcing the idea that switching to the SQ strategy is a reasonable alternative for patients with BEL. The fact that the patients trusted the treatment and did not experience side effects is a highlight of this study. As a negative aspect, our patients felt that the change reduced the time available to communicate with the health professionals. We here strongly support the design of specific teaching materials for the safe and self-administration of the drug, preventing the patient feeling neglected when we use SQ treatments.
Our findings are consistent with existing literature. Two small studies have been published evaluating the preference of lupus patients treated with BEL regarding the IV or SQ route. The cross-sectional study conducted as part of a phase IIb open-label, multi-dose trial of SQ BEL (NCT02124798) yielded similar results. 11 This study revealed that 96% of participants preferred the SQ auto-injector over IV infusion due to its convenience. Similarly, in a real-world clinical practice study, nine patients with SLE who were receiving IV BEL were transitioned to SQ BEL, and their satisfaction was assessed. 10 All nine patients had anticipated the approval of SQ BEL and agreed to switch their treatment with the support of their healthcare providers. Over a 6-month period, all patients maintained stable disease activity and functional status, with no recorded disease progression and with a high degree of satisfaction with the change in treatment. 10
Those results are not surprising though, while SQ route of administration is commonly recognized as being more convenient, requiring less time, and seamlessly fitting into patients daily routines compared to IV infusions. 27 However, in studies assessing patients’ preferences and satisfaction with the change in route of administration from IV to SQ in other chronic diseases, such as RA, the results are not consistently in favor of the SQ route. 12 Studies examining preferences and satisfaction with anti-TNF in RA differences were found according to the age of the patients, with older patients preferring the administration of IV treatment. 12 Furthermore, differences are also observed between those who were newly introduced to the treatment and those who were already undergoing it. Naïve patients displayed preference for SQ administration over IV in accordance with health professionals. On the other hand, patients who were already receiving treatment showed a preference for their current route of administration. 13 Importantly, is to note that the switch from IV TNF-α inhibition to SQ applications often involves a change in the medication itself, which can influence patients’ perception, including the fear of losing treatment efficacy due to the medication change. On the other hand, differences were also seen based on the age of the patients, with the youngest preferring the administration of SQ treatment. Another study by Desplats et al. 14 aimed to assess the reasons behind patients’ decisions to continue with IV infusions or switch to SQ injections of abatacept (ABA) and tocilizumab (TCZ). They found that patients who rejected the switch to SQ administration of TCZ and ABA primarily did so due to fears associated with the unfamiliar SQ route. Conversely, those who accepted the switch found the SQ route more convenient. In Daood et al.’s study, 15 object was to assess the efficacy and patient satisfaction of switching from IV TCZ to SQ TCZ in patients with rheumatologic conditions (81% RA patients) during the COVID-19 pandemic. A total of 37 patients were included in the study, and it was found that 26 patients had to revert to IV treatment. The primary reason for discontinuation was disease activity. Among the 11 patients who continued with SQ treatment, 3 indicated higher dissatisfaction with SQ administration. In our center, we conducted a study similar to this one, evaluating the satisfaction of RA patients who transitioned from IV rituximab treatment to SQ rituximab administration due to the pandemic. The results obtained showed comparable levels of patient satisfaction with the change in treatment route. The SQ administration of rituximab was found to be effective and safe in patients with RA. A reduction of 80% in hospital stay duration was observed, with a high level of patient satisfaction. 21
In other conditions like juvenile idiopathic arthritis, the impact of SQ administration of TCZ on patient satisfaction and disease control has also been studied. Based on the patient satisfaction questionnaire, 8 out of the 9 patients reported satisfaction with SQ administration, highlighting improvements in quality of life, school performance, and reduced school absenteeism. 16 In addition to rheumatology, other chronic diseases such as inflammatory bowel disease, patient satisfaction with the change in route of administration has been evaluated, including during the COVID-19 pandemic, and has shown a preference for the SQ route. 28 In studies of patients with lymphoma, that the RASQ has been used to assess patient preference and satisfaction with SQ versus IV administration of rituximab, it has been observed that patient satisfaction was higher with SQ administration. 29
Our study has some limitations. Although our study has a small sample size, is the biggest group of patients reported so far switched from IV to SQ BEL. Special caution is necessary when extrapolating the results to a larger population. The small sample size may affect the consistency and reliability of the findings. In addition, it should be noted that in our cohort of patients there are few patients with renal involvement. Future studies should also include this type of patients for whom BEL is already approved. Our study was conducted during pandemic years. It should also be assessed outside of the pandemic period, where patients could be influenced by the fear of contagion from going to the hospital leading to a preferential bias toward SQ administration. RASQ-SQ questionnaire is a well-validated satisfaction tool in patients with lymphoma treated with SQ rituximab but not in patients with SLE. Since there are no validated questionnaires to assess satisfaction of the change of IV to SQ therapies in SLE, we used the RASQ as a reasonable tool for switching strategies in biological therapies. The development of a specific and validated questionnaire would be necessary to assess patient satisfaction regarding the route of administration among SLE patients treated with BEL. Therefore, future studies with larger sample sizes and with well validated tools are required to confirm and strengthen our results.
Conclusions
Patient satisfaction with changes in medication administration is an essential element for a successful switching strategy. An earlier implementation of biological therapies during the treatment approach in SLE suggested recently in EULAR guidelines highlights the relevance of patients’ preferences among treatment options. The inclusion of patients’ perspectives can improve medical care by considering their needs, preferences, and experiences. By considering patient satisfaction, physicians can improve shared decision-making and provide personalized care.
These findings support the feasibility and acceptability of switching from IV BEL to SQ BEL treatment in patients with SLE, without any other direct issues such as worsening in the disease activity or safety concerns.
Supplemental Material
Supplemental Material - Satisfaction and effectiveness of switching from intravenous to subcutaneous belimumab treatment in daily clinical practice
Supplemental Material for Satisfaction and effectiveness of switching from intravenous to subcutaneous belimumab treatment in daily clinical practice by Beatriz Frade-Sosa, Tarek Carlos Salman-Monte, Javier Narváez, Irene Peralta, Sebastian Sandoval, Berta Magallares, Sergi Heredia, Nuria Sapena, Anne Riveros-Frutos, Alejandro Olivé, Hector Corominas, Josefina Cortés-Hernández, and Jose A Gómez-Puerta in Lupus
Footnotes
Acknowledgments
The authors wish to express their gratitude for the collaboration of the CAPICAT-MAS group, which is affiliated with the Catalan Society of Rheumatology.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GSK did not participate either in the design, manuscript preparation or results discussion. BFS received funds from Korean Rheumatology Society for the presentation of this project at Lupus International meeting, Seoul, May 2023. The author has received funding for attending educational courses. TSM received honorariums from GSK for lectures less than US$10.000 per year. JN received honorariums from GSK for lectures less than US$10.000 per year. IP No conflicts of interest for this article. SS No conflicts of interest for this article. BM received honorariums from GSK for lectures less than US$2.000 per year. SH received honorariums from GSK for lectures less than US$10.000 per year. NS No conflicts of interest for this article. ARF No conflicts of interest for this article. AO No conflicts of interest for this article. HC Presentations, collaborations, congress grants, consultancies: Galapagos, Roche, BMS, Fresenius-Kabi, UCB, Pfizer, Novartis, Abbvie, Gebro, Jansen, MSD, AstraZeneca, and Biogen. JCH received honorariums from GSK for lectures less than US$10.000 per year. JAGP received honorariums from GSK for lectures less than US$10.000 per year.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.