
Abstract

Sir,
The efficacy and safety of belimumab, a human antibody inhibiting the biological activity of the B-cell activating factor, in the treatment of patients with systemic lupus erythematosus (SLE) and lupus nephritis (LN) has been reported.1–4 Since glucocorticoid (GC) toxicity is a major concern in the treatment of SLE and LN, it is recommended that the use of GC be minimized and even withdrawn. 5 Thus, the add-on use of belimumab may be a viable option for the optimal management of SLE.1–4 However, little data is available regarding the implications of the use of belimumab in a “real-world” setting for the treatment of childhood-onset SLE (cSLE).6,7 In this context, we read with great interest a paper by Roberts et al. 7 in this journal. For the past 5 years, we have also used belimumab add-on treatment in nine patients with cSLE. Notably, three patients received belimumab as an add-on in an induction regimen comprising GC, mycophenolate mofetil (MMF), and hydroxychloroquine (HCQ). We found that belimumab was effective for successful and relatively rapid dose reduction of the concomitantly administered GC in these patients compared with patients who received the same induction regimen without belimumab.
Clinical characteristics of children with systemic lupus erythematosus who received induction therapy with belimumab (Group A) and without belimumab (Group B).
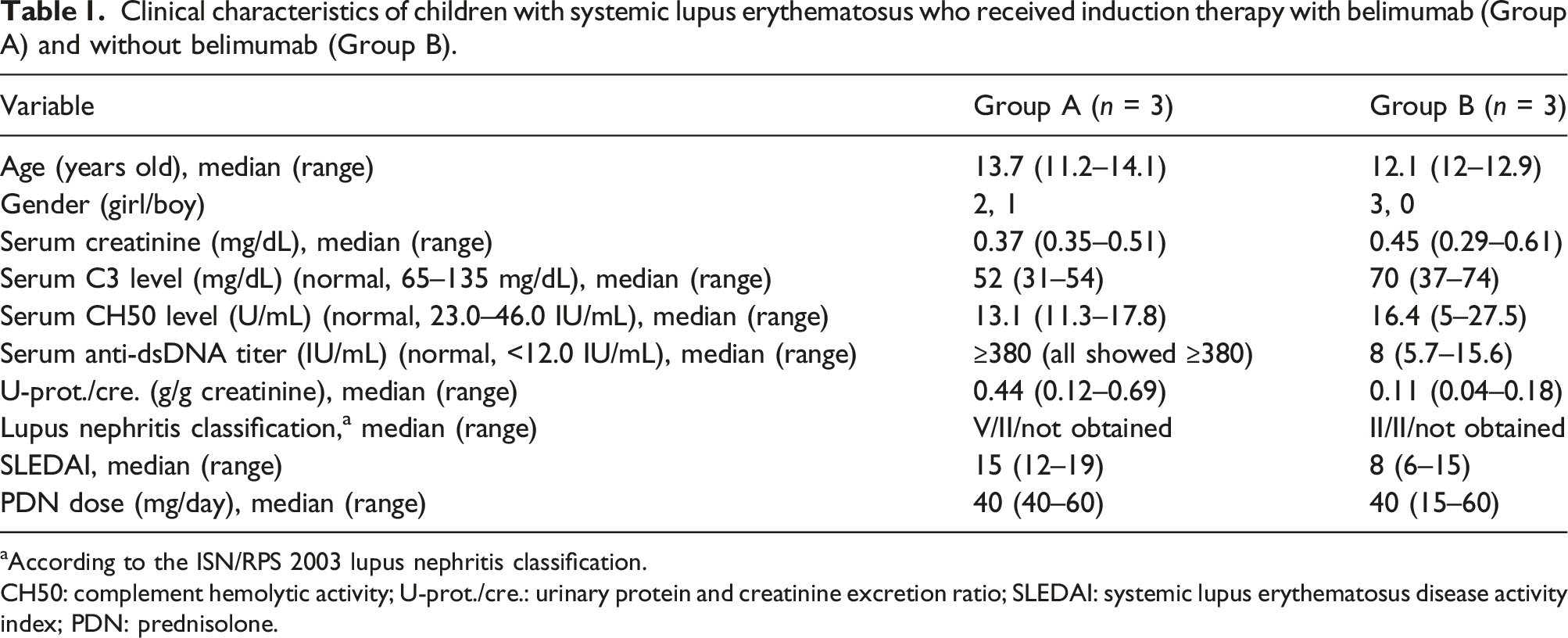
aAccording to the ISN/RPS 2003 lupus nephritis classification.
CH50: complement hemolytic activity; U-prot./cre.: urinary protein and creatinine excretion ratio; SLEDAI: systemic lupus erythematosus disease activity index; PDN: prednisolone.
To date, early add-on use of belimumab as induction therapy in selected patients with SLE has rarely been reported. 8 Considering the mechanism of action of belimumab, we think that the early add-on use of the drug may be an attractive choice for managing patients with SLE in a real-world setting for long-term favorable outcomes, particularly in cSLE. In this context, we confirmed the successful and rapid dose reduction of concomitantly administered GC without flares in our patients possibly because of early belimumab add-on use. Thus, further studies on the early add-on use of belimumab in a larger number of patients with cSLE are warranted.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from patients’ parents for the scientific publication of this report.