
Abstract
Objectives
For appropriate glucocorticoid (GC) reduction, we investigated the optimal strategy including baseline factors that could reduce GC more than 50% with 96 weeks of belimumab.
Methods
This is a retrospective cohort study of Kakogawa Central City hospital from 2019 to 2023. We identified SLE patients who were receiving 200 mg of belimumab weekly by subcutaneous injection for 96 weeks. The background at baseline, trends in clinical indicators, and factors involved in GC reduction were statistically analyzed. Finally, univariate and multivariate logistic analyses were carried out to identify baseline factors associated ≥50% GC reduction at 96 weeks.
Results
Forty-seven patients were enrolled, with a median daily prednisolone of 5 mg. Almost 90% of them received concomitant immunosuppressants and/or hydroxychloroquine. Serological indices, daily GC dose, and SLEDAI-2K scores showed significant improvement in 96 weeks. At baseline, a significant negative correlation has been shown between the daily dose of GC and the duration from onset or last flare, as well as C4 levels. At 96 weeks, GC reduction rate and SLEDAI-2K scores were negatively correlated with duration from onset or last flare to initiation of belimumab. Mycophenolate mofetil use was significantly frequent in patients with lupus nephritis (LN), which also correlated with the frequency of past flares. In addition, LN presence was associated with higher SLEDAI-2K scores at 96 weeks, and baseline SLEDAI-2K ≥10 was associated with significantly higher GC dose at 96 weeks. Univariate analysis of the factor contributing to achieving ≥50% GC reduction at 96 weeks has pointed shorter disease duration and higher daily GC dose at baseline as significant variables. Finally, we performed a multivariate analysis by combining above two items with age, which extracted the higher daily GC dose at baseline as a significant variable (OR (95% CI) 1.25 (1.00 to 1.56), p = .047).
Conclusions
Our study showed that a delay in belimumab initiation led to higher SLEDAI-2K score and difficulty in achieving a 50% GC reduction at 96 weeks. Since GC-related adverse events increase with long-term administration of GC though with small daily doses, we proposed here that belimumab should be started in combination with higher daily prednisolone.
Introduction
Systemic lupus erythematosus (SLE) is a chronic, systemic autoimmune disease of unknown cause that presents with a variety of organ involvement. The patient population is distributed across all age groups, while it is more prevalent in young people. Patients with SLE are treated with glucocorticoid (GC) in combination with immunosuppressants such as cyclophosphamide and mycophenolate mofetil (MMF). 1 Recent advances in SLE treatment strategies have improved the mortality rate; Mak et al. reported that the 10-year survival rate improved from 63.2% to 91.4% between 1950 and 2000. 2 Despite the improved prognosis, however, GC is associated with various adverse events (AEs) including infections, osteoporosis, and atherosclerosis.3,4 Importantly, higher daily or cumulative doses of GC induces more AEs and organ damage, and worse mortality and quality of life.5,6
In recent years, it is recommended that patients with SLE and their physicians work together to aim for remission with as little GC as possible.7,8 Although GCs should be reduced in combination with other therapeutic agents for preventing AEs,9,10 disease flares associated with GC withdrawal also causes organ damage and worsen mortality and QOL.11,12
A real-world data suggests that reducing the daily prednisone dose to 5 mg or less results in less subsequent impairment and maintaining the dose below 5 mg results in less frequent flares. 13 Alternatively, a report also shows such impairments at prednisolone daily doses of 4.42 mg or more, so it is clear that GC should be reduced where possible. 14 Although slow GC dose reduction exhibits a positive effect in reducing flare-ups, 15 it is still necessary to wean patients off GC as early as possible in order to prevent an increase in cumulative GC dose leading to AEs, to the extent that there is no flare of the disease. 16
In 2017, belimumab was approved in Japan as the first biologic for the treatment of SLE. It reduces disease activity and flare rates by inhibiting B cell activating factor (BAFF), also it is effective for GC reduction.17–20 Furthermore, belimumab has fewer disease flares and less progression of organ damage with long-term use.21–23 Thus, belimumab therapy is one of the essential treatment strategies to rapidly reach the minimum GC dose, but the optimal timing for initiating belimumab is not yet clear.
In this study, we retrospectively analyzed therapeutic outcomes of belimumab for SLE patients during GC reduction and discussed the optimal timing of starting belimumab.
Methods
Study design and setting
This is a retrospective cohort study using electronic medical record data of Kakogawa Central City hospital from January 1, 2019 to October 31, 2023. The Kakogawa Central City Hospital is a core hospital of the region and covers a population of approximately half a million with approximately 2000 annual outpatients’ visits in the rheumatology department. The study protocol was approved by the Ethics Committee of Kakogawa Central City hospital (#2022-25, 6 December 2022), and they waived informed consent as the nature of the retrospective design.
Participants
We investigated electronic medical records to identify SLE patients who were receiving belimumab for 96 weeks as of October 2023. Inclusion criteria for the study was a definite diagnosis according to the 2019 ACR/EULAR classification criteria 23 and has received GC at the time of belimumab initiation. Five Japanese board-certified rheumatologists performed regular checkups, including blood tests related to disease activity, and determined the dosage of GC and immunosuppressants. The treatment was based on shared decisions with the patient in accordance with the principles of treat to target strategy. If remission could not be reached, the goal was set as Lupus Low Disease Activity State (LLDAS). 24 With antimalarials if not contraindicated and immunosuppressants if possible, the GC dose was to be the minimum to control disease.
Belimumab was introduced at a dose of 200 mg once a week by subcutaneous injection in all patients. Except for the initial hospital administration, patients self-injected. Presence or absence of severity of flare was evaluated by Safety of Estrogens in Lupus Erythematosus National Assessment (SELENA)- SLE Disease Activity Index (SLEDAI) flare composite index. 25
Data collection
At the time of belimumab initiation, the following data were collected; age, sex, disease duration, daily GC dose, C3, C4, anti dsDNA antibody titers, SLEDAI-2K, SLEDAI-2K ≥ or <10, with or without LN, time from onset or last flare to belimumab initiation, with or without concomitant hydroxychloroquine (HCQ), and concomitant immunosuppressants. Trends in complement 3 (C3) levels, complement (C4) levels, and double-strand DNA (dsDNA) antibody titers, SLEDAI-2K scores, daily GC dosage, and GC reduction rate compared to baseline were examined at the start of belimumab, at 48 and 96 weeks. Incidences of GC-related AE which required hospitalization or flare during the course were also followed.
Statistical analysis
We described the patients’ characteristics using median and interquartile range (IQR) for continuous variables and number and percentage (%) for categorical variables.
The data collected at baseline and after treatment were compared using the Wilcoxon’s signed rank test and Mann-Whitney U test for continuous variables, Pearson’s chi-test or Fisher’s exact test was used to compare the differences between categorical variables. Correlation analysis between two variables was performed using Spearman’s rank correlation. Univariate and multivariate logistic regression analyses were carried out to identify factors associated with GC reduction of ≥50%. Variables with p < .1 in univariate logistic regression analyses were included in multivariate and the results were reported as Odds ratios (ORs) with 95% CIs. Multivariate logistic regression model’s prediction performance was also reported, including the Hosmer–Lemeshow goodness-of-fit test, a receiver operating characteristic (ROC) curve. Data were statistically significant at a value of p < .05. Statistical analyses were performed by SPSS version 26 (IBM Corp, Armonk, NY, USA).
Results
Patients background at belimumab initiation
Ninety-nine patients had received belimumab as of October 2023, 54 of whom had been on the treatment for 96 weeks. Four of these patients were excluded because of no concomitant GC and another three patients because of interruption due to pregnancy. Then 47 patients were included in this study, the median age of them were 44 years (interquartile range (IQR), 37 to 51), 88% were female. The median disease duration is 14 years (4 to 19), median daily prednisolone dose was 5 mg (4 to 9) at baseline. The median SLEDAI-2K score was 6 (3 to 8), with 21% of patients scoring 10 or higher.
Patient background at baseline.
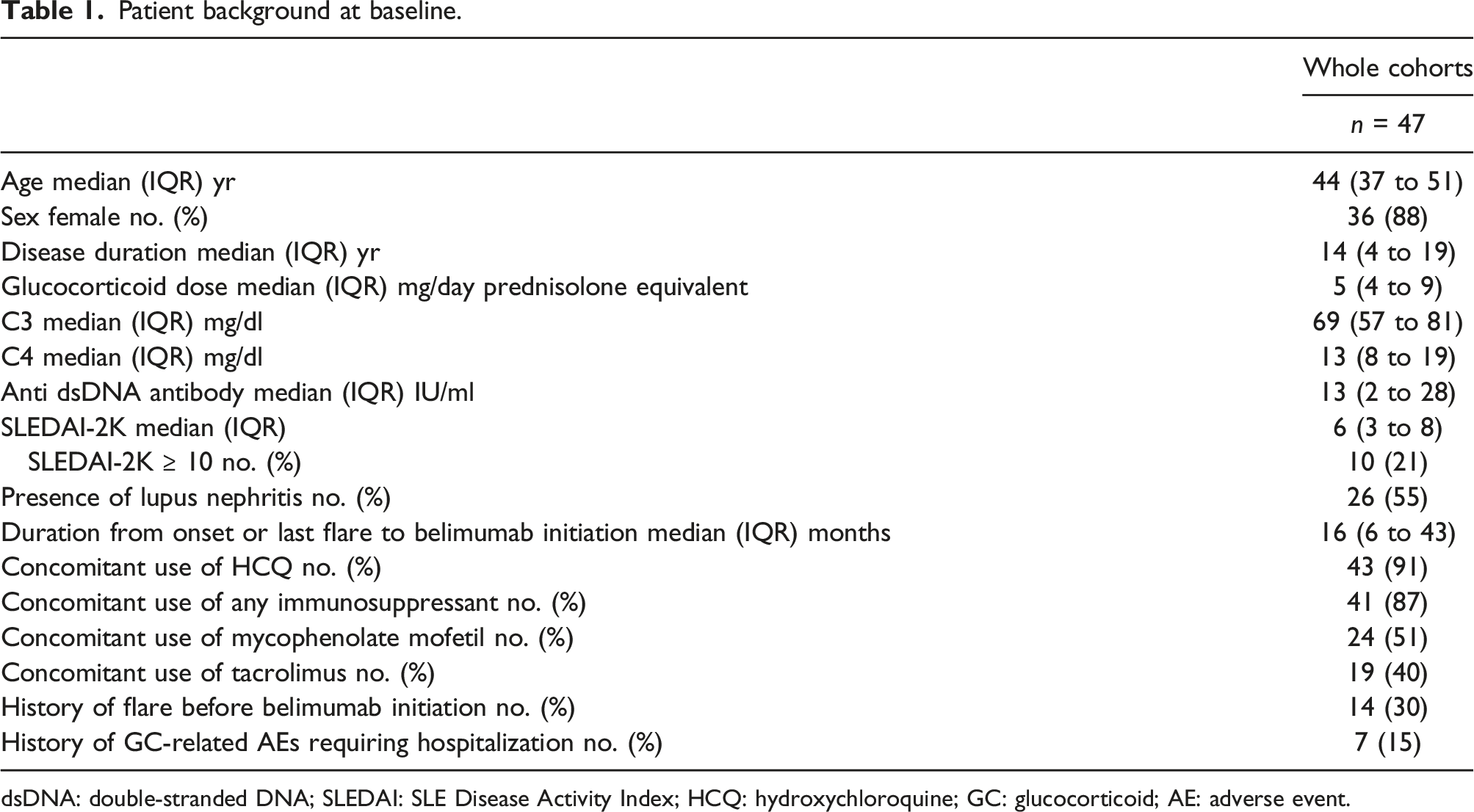
dsDNA: double-stranded DNA; SLEDAI: SLE Disease Activity Index; HCQ: hydroxychloroquine; GC: glucocorticoid; AE: adverse event.
Changes in clinical indicators at belimumab initiation, week 48 and 96
When compare the changes in clinical indicators after belimumab initiation, significant improvements were found in complement, dsDNA antibody titers and SLEDA I-2K scores at both 48 and 96 weeks, as well as in daily GC dose and GC reduction rate (Figure 1). Changes in clinical indicators at belimumab initiation, at 48 and 96 weeks. (a) Serum C3 levels. (b) Serum C4 levels. (c) Serum anti-dsDNA antibodies. (d) Daily prednisolone dosage. (e) Prednisolone reduction rate compared to baseline. (f) SLEDAI-2K scores. dsDNA: double-stranded DNA; GC: glucocorticoid; SLEDAI: SLE Disease Activity Index.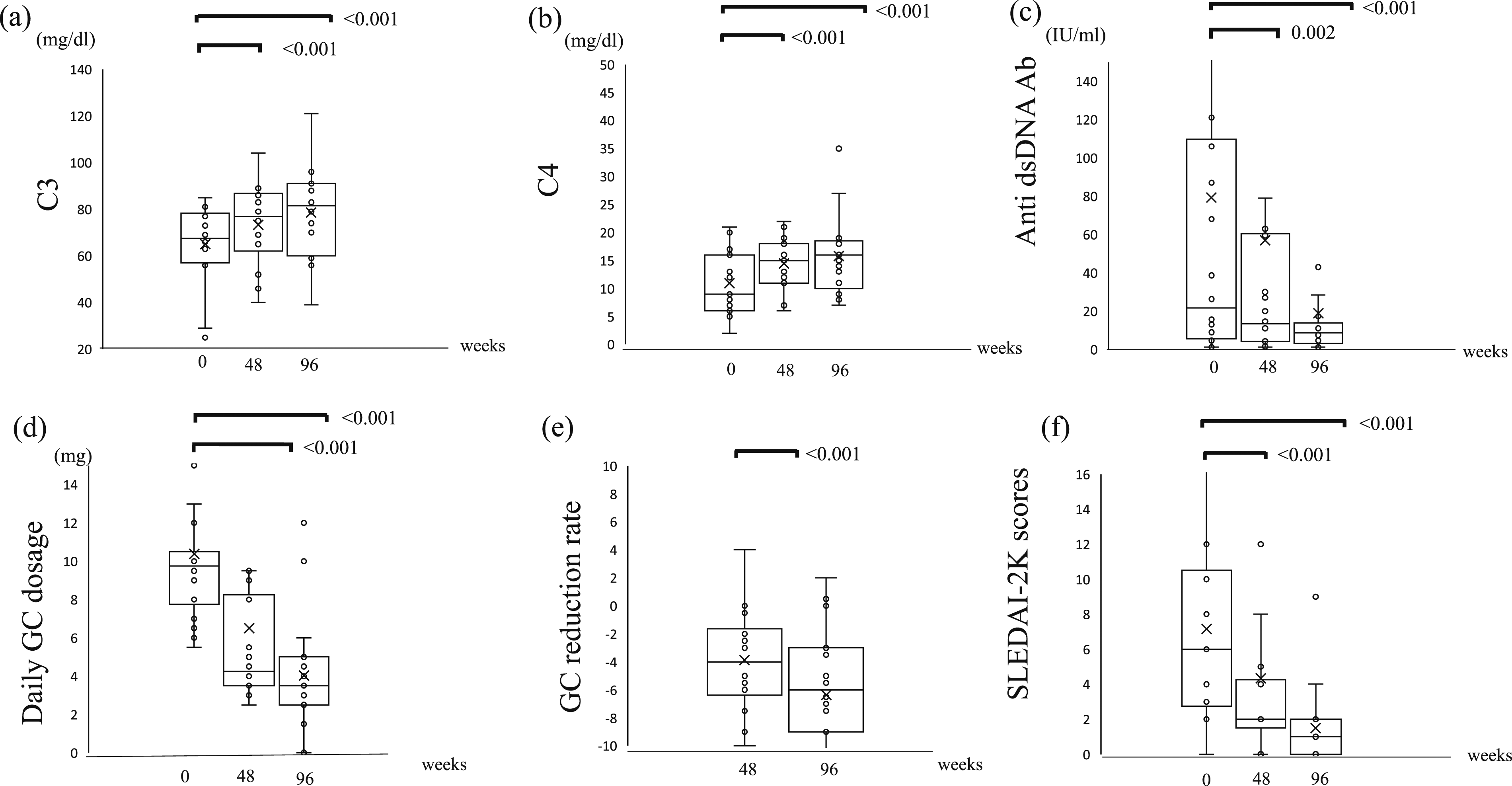
Correlations between daily GC dose, disease duration (from disease onset or last flare to belimumab initiation) and clinical status.
At baseline, daily GC dose showed a significant negative correlation with disease duration from onset or last flare to belimumab initiation (rho = −0.509, p < .001) and a negative correlation with C4 level (rho = −0.305, p = .042). (Figure 2(a)). We found that baseline daily GC dose did not correlate with SLEDAI-2K scores or GC reduction rate at 96 weeks, while disease duration from onset or last flare to belimumab initiation had a significant positive correlation with SLEDAI-2K scores at 96 weeks (rho = 0.337, p = .021), as well as a significant negative correlation with GC reduction rate (rho = −0.372, p = .001) at 96 weeks (Figure 2(b)). Correlation between daily GC dose at baseline or disease duration from disease onset or last flare to belimumab initiation and clinical status A) at baseline or B) at 96 weeks * = p < .05. dsDNA: double-stranded DNA; GC: glucocorticoid; SLEDAI: SLE Disease Activity Index.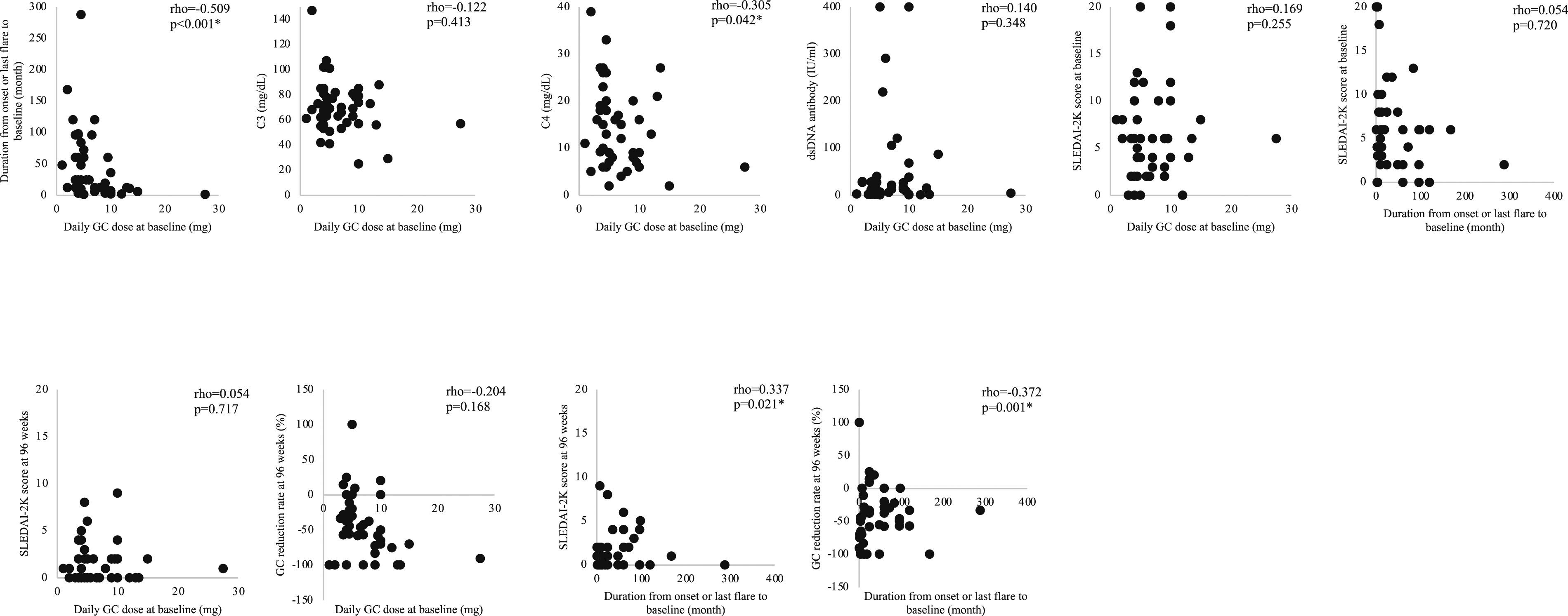
The impact of concomitant immunosuppressants (MMF and TAC) and clinical status (presence or absence of LN and SLEDAI-2K scores ≥ or <10) on GC reduction.
At baseline, 71% of patients taking MMF had LN and significantly more flares before starting belimumab (p = .045); however, disease duration, daily GC dose, and disease activity were not associated with MMF administration. There were also no differences in daily GC dose, GC reduction rates, disease activity, and flare after belimumab initiation at 96 weeks.
The impact of concomitant immunosuppressants (MMF and TAC) and clinical status (presence or absence of LN and SLEDAI-2K scores ≥ or <10) on GC reduction.
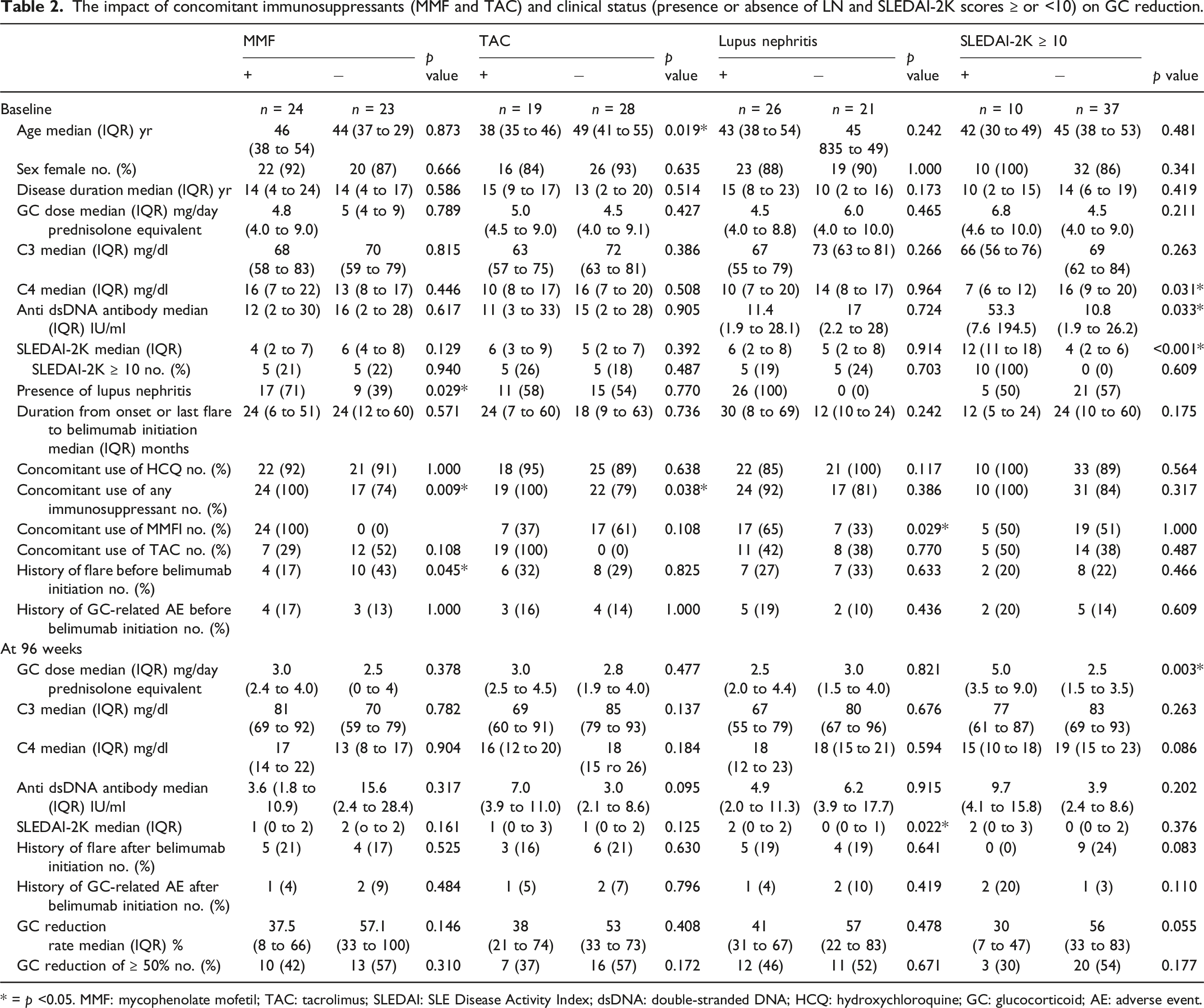
* = p <0.05. MMF: mycophenolate mofetil; TAC: tacrolimus; SLEDAI: SLE Disease Activity Index; dsDNA: double-stranded DNA; HCQ: hydroxychloroquine; GC: glucocorticoid; AE: adverse event.
Univariate and multivariate logistic regression analyses to assess the factors associated with ≥50% GC reduction at 96 weeks
Univariate and multivariate logistic regression analyses to assess the factors associated with ≥50% GC reduction at 96 weeks.
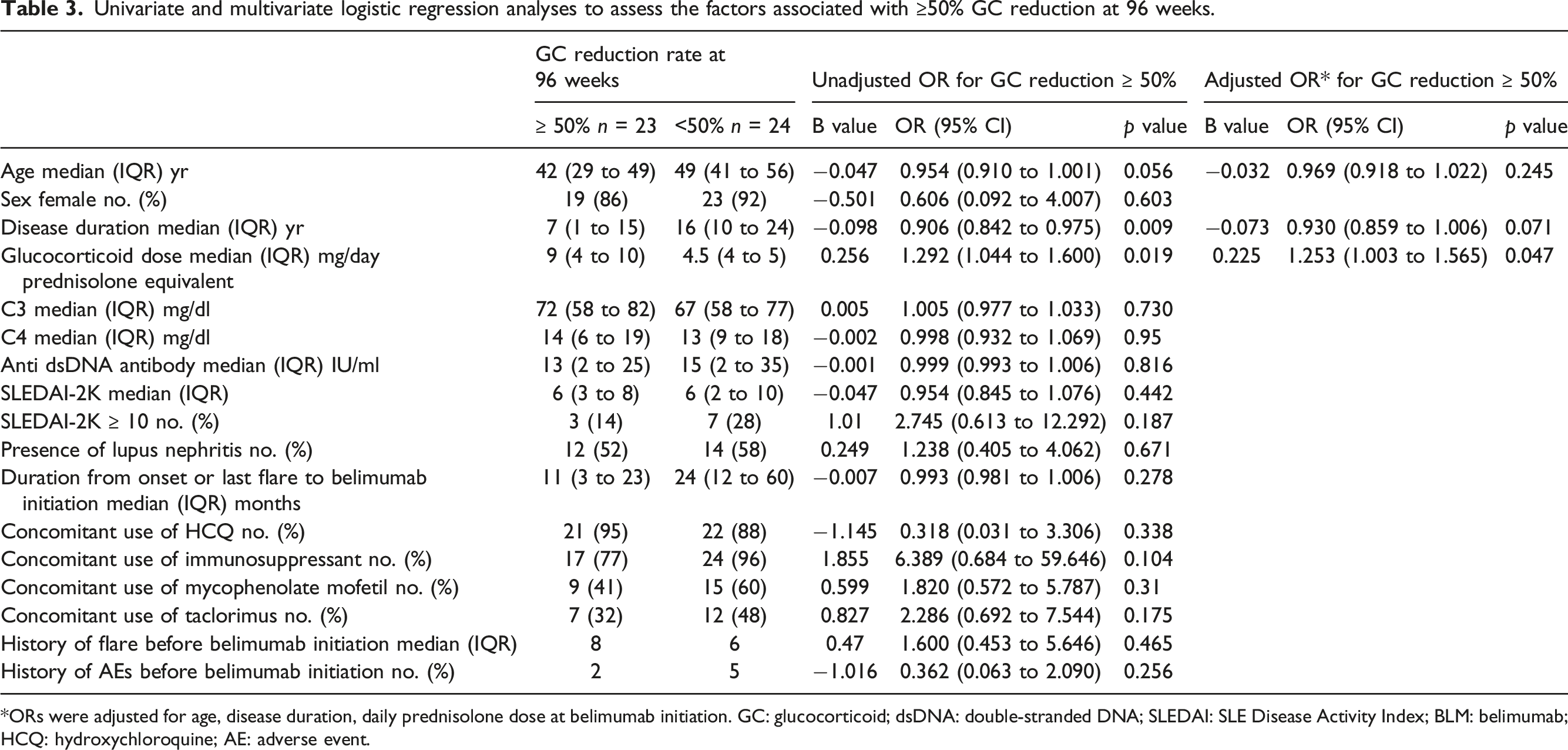
*ORs were adjusted for age, disease duration, daily prednisolone dose at belimumab initiation. GC: glucocorticoid; dsDNA: double-stranded DNA; SLEDAI: SLE Disease Activity Index; BLM: belimumab; HCQ: hydroxychloroquine; AE: adverse event.
Throughout the observation period, we found 7 mild/moderate flares and 1 severe flare (Hemolytic anemia requiring methylprednisolone pulse therapy) There were 7 flares in the 96 weeks prior to belimumab initiation, a non-significant decrease of p = .084 on Pearson’s chi-test, not a single case of belimumab discontinuation due to flare. There were 3 hospitalizations due to GC-related AEs during the observation period, the same number as in the 96 weeks prior to belimumab administration.
Discussion
In our study, 47 SLE patients had median disease duration of 14 years, and almost 90% of them were on a combination of immunosuppressants and/or HCQ, with median prednisolone dose of 5 mg per day. Ninety-six weeks of belimumab treatment significantly reduced disease activity and achieved GC reduction regardless of GC doses, concomitant immunosuppressants, and presence or absence of LN, SLEDAI-2K score ≥ or <10 at belimumab initiation. When belimumab was initiated in combination with higher GC dose, in particular, we found that the subsequent GC reduction rate was high, irrespective of disease activity. We also found that combined use of belimumab reduced GC to lower doses than reached with other concomitant medications.
After reaching low dose of GC, GC withdrawal is not attempted to avoid disease flare-up in many cases. However, recent reports have suggested that achieving GC discontinuation, even for a short period, is effective for reducing future organ damages 26 ; thus, treat-to-target strategy is highly recommended for continuous GC reduction. 8 The effectiveness of belimumab as a tool for achieving this recommendation is consistent with many previous studies, which have reported that belimumab can reduce flares, GC dose, and decrease disease activity in Asian SLE patients.20,27 The patients in this study had median disease duration of 14 years, but even in patients with a disease duration of 20 years or longer, one-point GC- free status may be related to less chronic damage accrual. Therefore, further GC reduction should be attempted in patients with longer disease duration. 26
Although many reports suggest that belimumab is more effective in serologically active patients, our study shows that GC reduction is feasible even in patients who were not markedly serologically active at the belimumab initiation. In fact, recent reports suggest that belimumab is effective in serologically inactive patients,28,29 support our findings.
We did not experience any flare cases that led to discontinuation of belimumab. One case, classified as a severe flare, was started on belimumab due to increased disease activity during GC reduction. Thereafter, this patient improved with methylprednisolone pulse therapy and a temporary increase in GC dose. Reducing or discontinuing GC has been reported to increase the risk of flare more than continuing maintenance therapy, but does not increase the risk of a major flare. 30 Moreover, GC-induced organ damages are less common in patients who discontinue GC than in patients on GC maintenance therapy, and this provides the rationale that even low-dose GC should be discontinued. 15
Previously, Tani C et al. reported that GC withdrawal could be achieved an average of 6 years after the last flare, and Moroni G et al. reported that GC withdrawal after a median remission of 52.8 months was more likely to be maintained thereafter.31,32 However, our study suggests that concomitant use of belimumab early from the disease onset or final flare, even at higher daily GC doses, is advantageous for GC reduction at 96 weeks. In addition, the SLEDAI-2K score and GC reduction rate at 96 weeks were negatively correlated with the duration of disease at the time of belimumab initiation, suggesting that delayed induction of belimumab resulted in prolonged disease activity and time to reduce GC. Furthermore, LN is associated with a higher SLEDAI-2K score at 96 weeks, and median GC dose at 96 weeks was higher in cases with SLEDAI-2K ≥10 at baseline. Thus, we can recommend that starting belimumab, in early therapeutic intervention even with high dose GC, for patients with LN or SLEDAI-2K ≥10.
Because this was a retrospective study, no strict criteria were set for the concomitant drug and GC dosage. However, the high rate of concomitant HCQ and immunosuppressants at baseline and adequate prescriptions of MMF for LNs suggest that the cohort under study is properly treated along with recent recommendations. Also, the higher GC dose at belimumab initiation is associated with shorter disease duration and lower C4, suggesting that the baseline GC dose is not excessive. We would like to establish for evaluation with continued observation whether treatment with belimumab and subsequent reduction in GC would reduce flare or GC-related AEs.
Here, our results propose that belimumab should be started in combination with higher daily prednisolone to achieve ≥50% GC reduction after 96 weeks. Moreover, since GC-related AEs increase with long-term administration of GC even with small daily doses, it is important to note that early initiation of belimumab is effective for subsequent GC reduction.
Footnotes
Acknowledgments
The authors would like to thank the attending rheumatologists of the cases included in this study.
Authors’ contributions
All authors participated in the interpretation of study results and in the drafting, critical revision, and approval of the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TY has been paid as a speaker for GSK. AH received financial grants from ASAHI KASEI PHARMA, CHUGAI PHARMACEUTICAL CO. LTD, Eli Lilly Japan K.K.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.