
Abstract
Objective
To evaluate the possible reversibility of PAH to a normopressoric state in SLE after induction immunosuppressive (IS) and predictors of response.
Methods
We retrospectively evaluated all SLE-PAH patients who underwent IS therapy at our center. PAH reversion was defined as the normalization of pulmonary arterial pressure (PAP), either by the presence of systolic PAP <40 mmHg on echocardiogram or mean PAP <20 mmHg on right heart catheterization (RHC). SLE patients were divided in Reversion and No-Reversion of SLE-PAH groups for comparative analysis at baseline and after IS.
Results
Among 2,074 SLE patients, 28 SLE-PAH received IS therapy (1.3%). Ten patients (35.7%) achieved SLE-PAH reversion. Demographic data, disease duration, SLEDAI-2K, and SDI Damage scores were similar between Reversion and No-Reversion of SLE-PAH groups (p > 0.05). At baseline, Reversion of SLE-PAH had lower sPAP (p = 0.032), lower right ventricle dilatation (p = 0.003) and hypokinesia (p = 0.017) frequencies on echocardiogram, and also lower BNP levels (p = 0.041) and risk stratification score (p = 0.014). Hemodynamic parameters were similar among groups (p > 0.05). After IS, a significant decrease in CRP levels was identified only in Reversion of SLE-PAH (p = 0.013), although both groups had a significant reduction in SLEDAI-2K (p < 0.05). Both groups had significant improvement in risk stratification score (p = 0.009 and p < 0.001) with a better survival rate in Reversion of SLE-PAH (p = 0.047).
Conclusion
This is the first study that identified that more than one third of SLE-PAH had a complete reversion of PAH after IS therapy with a significant impact on their survival. These findings strongly support the notion of an underlying inflammatory etiology of this condition, which reinforces the use of immunosuppressive treatment for all SLE patients at PAH onset.
Keywords
Introduction
Pulmonary arterial hypertension (PAH) is a rare condition characterized by progressive remodeling of small pulmonary arteries, resulting in an increase in pulmonary vascular resistance and subsequent right heart failure. 1 Connective tissue disease is an important etiology of PAH, accounting for approximately 20-25% of all PAH cases.2–4 Notably, among all connective tissue diseases, systemic sclerosis and systemic lupus erythematosus (SLE) are the most important diseases associated with PAH.2–4
The prevalence of PAH varies widely, ranging from 0.5% to 17.5% in SLE, depending on the diagnostic method for its definition.2,5,6 Considering only invasive diagnosis, the prevalence of PAH in SLE is around 4%7,8. Importantly, PAH significantly impacts the prognosis of SLE patients, 9 leading to a decrease in 5-years survival rates by more than 20%.10–12
Pulmonary vascular remodeling in SLE associated PAH (SLE-PAH) is believed to primarily involve immune and inflammatory mechanisms rather than a fibrotic process.13–15 This hypothesis is supported by observed clinical improvement in a significant proportion of SLE-PAH patients following immunosuppressive (IS) treatment, as identified in case reports and series.2,11,16–21 However, inconsistencies in improvement criteria have been observed in these previous studies,2,11,16–21 which precludes definitive conclusions about the true effectiveness of IS therapy in SLE-PAH. In fact, variable levels of reduction in pulmonary artery pressures and clinical improvement were the most frequently reported parameters in those studies.2,11,16–21 Reversibility of pulmonary arterial hypertension (PAH) to normal pulmonary artery pressure has never been used as the primary outcome after IS therapy; thus, the rate of pressure normalization in these patients remains to be determined.
The aim of the present study was to identify the rate of complete reversion of SLE-PAH, defined by the normalization of pulmonary artery pressures after IS induction therapy, and to determine predictors of reversibility.
Methods
This was a retrospective analysis of all patients diagnosed with SLE-PAH and treated with induction immunosuppressive therapy identified from our prospective electronic database with 2074 SLE patients regularly followed at the outpatient clinic of the Rheumatology Division, Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Sao Paulo, SP, Brazil, from 2000 to 2021. In 2000, we established a standard electronic protocol consisting of comprehensive clinical and laboratorial evaluations for each patient at intervals of 1 to 6 months. The present study was approved by the Ethics Committee for Research Projects Analysis of Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil (# 41739620.8.0000.0068).
All SLE patients fulfilled the 1997 SLE criteria 22 and also the 2012 Systemic Lupus International Collaborating Clinics (SLICC) classification criteria 23 evaluated retrospectively. The presence of pulmonary arterial hypertension (PAH) was defined by transthoracic echocardiogram (TTE) due to a systolic pulmonary arterial pressure (sPAP) higher than 40 mmHg, associated with symptoms (dyspnea, syncope), or signs of right ventricular (RV) dysfunction (increased BNP levels and/or echocardiographic signs of RV failure), without evidence of left heart disease. SLE patients who underwent right heart catheterization (RHC) were considered as having SLE-PAH in the presence of a mean pulmonary artery pressure (mPAP) > 20 mmHg with pulmonary artery wedge pressure (PCWP) <= 15 mmHg, and pulmonary vascular resistance (PVR) > 2 Wood units (WU) in the absence of significant lung disease or chronic thromboembolic disease based on the pulmonary scintigraphy and/or chest tomography. 24
All patients included in this study received IS therapy for this condition, irrespective of concurrent use of targeted PAH therapies in accordance with the last guidelines. 25 Since 2002, PAH has been considered a vascular manifestation of SLE, as suggested by some small studies,17,18 and in 2008 Jais et al.'s demonstrated a positive response to immunosuppressive (IS) therapy in these patients. 20 Since that period, our group has consistently used IS therapy in all patients with PAH associated with SLE.
PAH reversal was defined by normalization of sPAP (<40mmHg) on TTE or of mPAP (<20 mmHg) on RHC after IS therapy. Based on this reversal criteria, SLE patients were classified into two groups: Reversion of SLE-PAH and No-Reversion of SLE-PAH.
SLE-PAH patients with persistent PAH after IS (No-Reversion of SLE-PAH group) and those with high baseline risk of mortality, defined by simplified risk calculator from Registry to Evaluate Early and Long-term Pulmonary Arterial Hypertension Disease Management (REVEAL Lite 2.0 risk score), 26 were also followed at the Pulmonary Circulation Unit, Pulmonary Division, Heart Institute University of São Paulo Medical School São Paulo Brazil. These patients were treated in accordance with current guidelines and availability of treatments.24,25
Data were collected at baseline (PH onset) and after a minimum of 6 months following IS induction therapy. The collected data encompassed age of SLE diagnosis, demographic data, disease duration, clinical and laboratorial features, immunologic/autoantibodies characteristics, IS therapy, presence of antiphospholipid syndrome, hemodynamic and echocardiographic data. Disease activity and damage of disease were assessed using the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) 27 and Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SDI), respectively, and were calculated at baseline and at after IS therapy. 28 Low disease activity was defined as an SLEDAI-2K score ≤4, 27 while high disease activity was defined by an SLEDAI-2K score ≥10. 29 Damage was considered present if SDI ≥1, with PH not included in the final score. 28 Mortality Risk stratification was performed according to REVEAL Lite 2.0. 26 The final score classifies patients into low, intermediate, or high risk of mortality within 1 year, with scores of 1–5, 6–7, and >8 points corresponding to low, intermediate, and high risk, respectively. 26
Statistical analysis
Continuous variables are presented as median and interquartile range, while categorical variables are expressed by percentage. For comparison between groups, we used Mann–Whitney test for the continuous variables and Chi-square or Fisher’s exact tests for the categorical variables, as appropriate. Survival during time is described through Kaplan-Meier curves and compared using log-rank test. All statistical analyses were performed using SigmaStat 14.5 (Systat Software Inc). p values lower than 0.05 were considered significant.
Results
In our SLE cohort, 30 patients were initially identified. However, two were excluded due to alternative causes for PAH: one had interatrial communication and the other schistosomiasis. Thus, 28 SLE-PAH who received IS therapy at PAH onset were identified among 2074 SLE patients regularly followed in our center (1.3%). All these 28 SLE patients had sPAP higher than 40 mmHg at TTE, and in 17 (60.7%) of them, the PAH diagnosis was further confirmed by RHC.
Demographic, clinical and inflammatory data for the whole cohort and according to the reversibility classification.
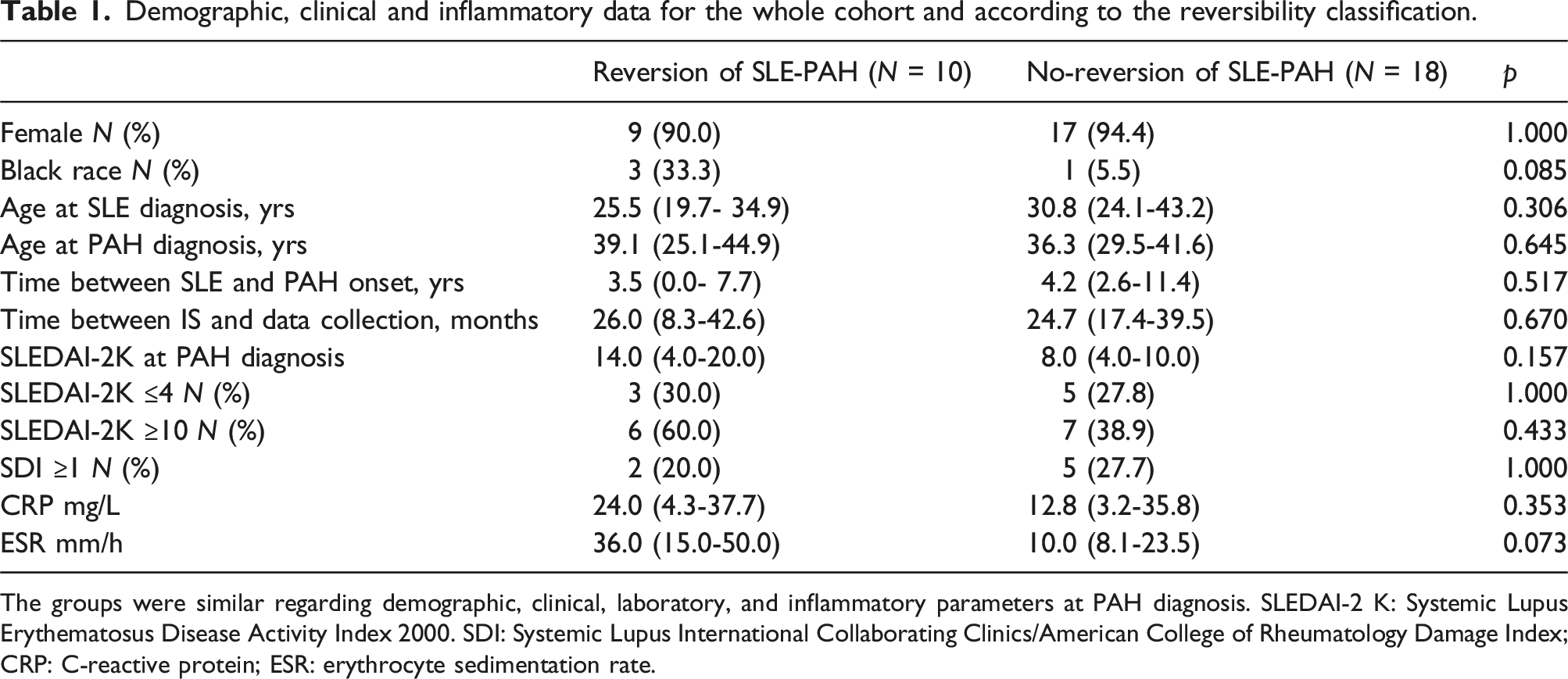
The groups were similar regarding demographic, clinical, laboratory, and inflammatory parameters at PAH diagnosis. SLEDAI-2 K: Systemic Lupus Erythematosus Disease Activity Index 2000. SDI: Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate.
Demographic, clinical, and laboratory data of both groups are demonstrated in Table 1. The mean age at study entry was comparable (p = 0.456) with a clear predominance of female gender in both groups. Only one patient had tobacco smoke exposure. PAH was identified within the first 5 years of the disease in almost two-thirds (64.3%) of all included SLE-PAH patients and the mean time was alike in Reversion and No-reversion group (p = 0.517).
Regarding 2012 SLICC parameters for SLE diagnosis, serositis and acute cutaneous lupus were the most frequent manifestations with a comparable frequency in both groups (7 (70%) versus 11 (61.1%), p = 0.703 and 7 (70%) versus 12 (66.7), p = 1.000, respectively), whereas articular involvement was more frequent in the No-Reversion group (6 (60%) versus 17 (94.4%), p = 0.041). Around 30% of patients in both groups had renal disorder (p = 1.000). Antiphospholipid Syndrome was diagnosed in one (10%) patient among Reversal of PAH-SLE group and two (11%) cases were registered in the other group (p = 1.000), despite a frequency of 40% and 27.7% (p > 0.05) of Antiphospholipid antibodies in each group. One patient exhibited segmental pulmonary thrombosis despite the absence of antiphospholipid antibodies. Regarding autoantibodies data, anti-Ro was the most frequently observed (80 vs 83%), followed by anti-dsDNA (70% vs61%) and anti-RNP (40% vs 50%) with a similar occurrence in patients with and without reversal (p > 0.05).
The analysis of the SLE activity and damage scores revealed no significant differences between the two groups (Table 1). Both groups had similar proportions of patients with low disease activity (30.0% in the Reversion group vs 27.8% in the No-Reversion group; p = 1.00), indicating that the main indication for immunosuppressive (IS) treatment was primarily due to PAH in these patients. For the remaining 70%, with SLEDAI-2K >4, IS was indicated due to multiorgan SLE disease activity. At the time of PAH diagnosis, although the Reversion group had a numerically higher total SLEDAI-2K score (p > 0.05), no statistically significant differences were found among the various activity parameters. The frequencies of pleurisy (40% vs 11.1%; p = 0.147), pericarditis (30% vs 11.1%; p = 0.315), renal flare (30% vs 22.2%; p = 0.674), and positive anti-dsDNA antibodies (70% vs 44.4%; p = 0.254) were higher in the Reversion group but did not reach statistical significance. In terms of other clinical manifestations, acute cutaneous manifestations and arthritis occurred in 40% and 30% of patients in the Reversion group compared to 27.8% in both cases in the No-Reversion group (p = 0.677 and p = 1.000, respectively). Other organ activities were rare, with fever reported in one patient from each group, one seizure in the Reversion group, one case of vasculitis and two of myositis in the No-Reversion group. In terms of laboratory data, leukopenia was observed in 30% of the Reversion group compared to 22.2% in the No-Reversion group (p > 0.05). Thrombocytopenia was present in 10% of the Reversion group and 16.6% of the No-Reversion group (p > 0.05). Regarding inflammatory markers, both groups exhibited similarly elevated levels of CRP and ESR, with no statistically significant differences (p > 0.05).
Baseline hemodynamic, functional and risk stratification parameters in Reversion of SLE-PAH group and no-Reversion of SLE-PAH group.
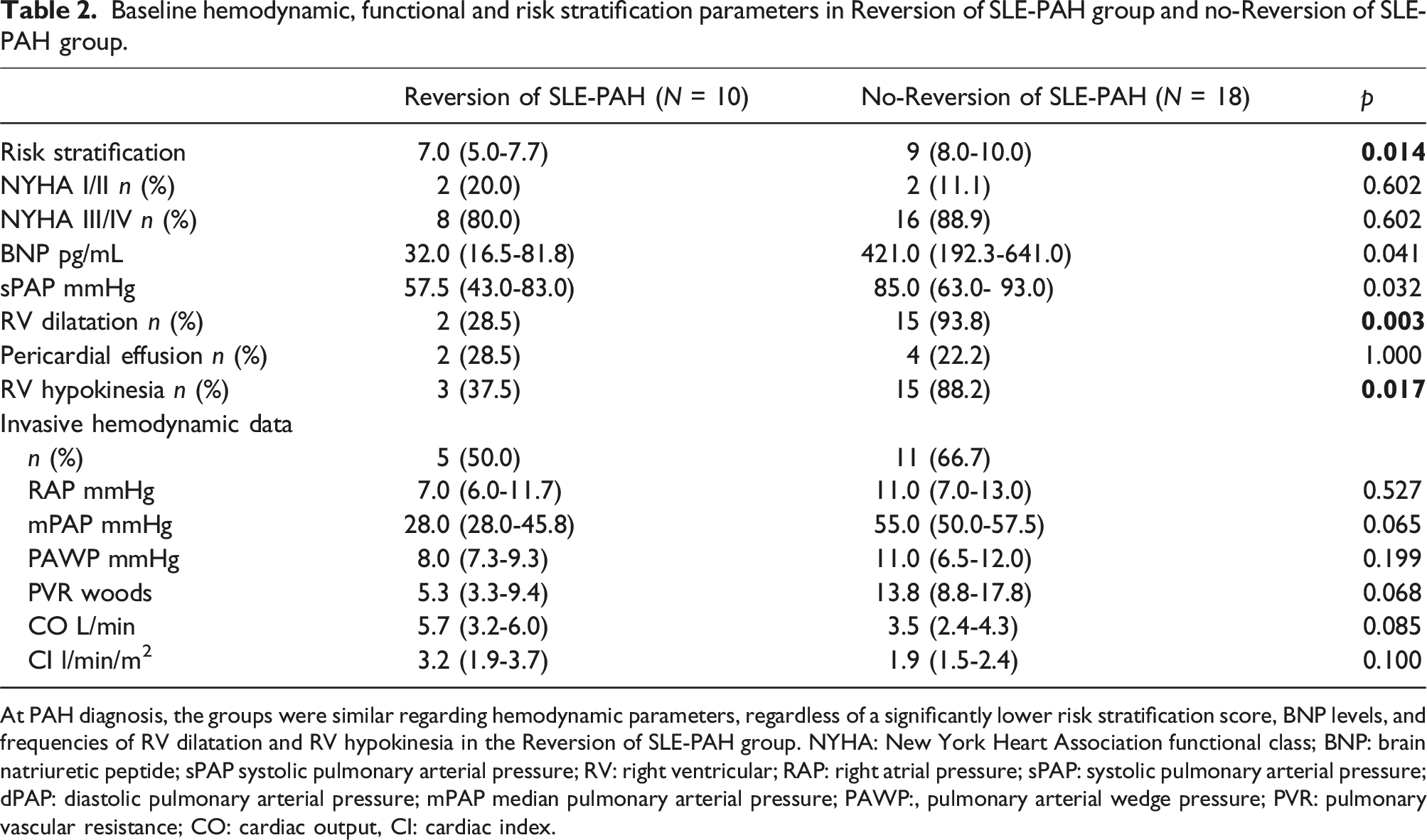
At PAH diagnosis, the groups were similar regarding hemodynamic parameters, regardless of a significantly lower risk stratification score, BNP levels, and frequencies of RV dilatation and RV hypokinesia in the Reversion of SLE-PAH group. NYHA: New York Heart Association functional class; BNP: brain natriuretic peptide; sPAP systolic pulmonary arterial pressure; RV: right ventricular; RAP: right atrial pressure; sPAP: systolic pulmonary arterial pressure; dPAP: diastolic pulmonary arterial pressure; mPAP median pulmonary arterial pressure; PAWP:, pulmonary arterial wedge pressure; PVR: pulmonary vascular resistance; CO: cardiac output, CI: cardiac index.
TTE parameters indicated a lower sPAP (p = 0.032), lower frequencies of RV dilatation. Concerning hemodynamic parameters, assessed via RHC, the numerically better hemodynamical status of Reversion groups was not statistically significant and the groups were considered similar concerning mPAP, pulmonary vascular resistance (PVR), cardiac output (CO), and cardiac index (CI) (p > 0.05) [Table 2].
All patients received glucocorticoid (GC) as initial treatment. The time between the PAH diagnosis and initiation of IS was 3.4 (0.5-19.9) months and was similar between groups (p > 0.05). Methylprednisolone pulses were similarly used in both groups [4 (44.4%) versus 8 (42.1%), p = 1.000]. There was no significant difference in the daily oral prednisone dose between the two groups. Intravenous cyclophosphamide (IVCYC) was the most common IS used as induction therapy (67.9% of all patients), with similar frequencies between groups, six patients (60.0%) in the Reversion and 13 (46.4%) in the No-Reversion SLE-PAH group (p = 0.678). The cumulative doses of IVCYC were also comparable (6.8 g vs 6.0 g, p = 0.701). Azathioprine was used by 20.0% of patients in the reversal group and 22.2% in the non-reversal group (p = 0.800), while mycophenolate was administered to 20.0% and 11.1% of patients in the respective groups (p = 0.667). Concomitant PAH therapy was significantly more common in the No-Reversion SLE-PAH, four out of ten (40%) in the reversal Group versus seventeen (94.4%) in No-Reversal PAH-LES (p = 0.007). Combination therapy, involving two or more medications for PAH, was used in 21 (75%) of treated patients. Sildenafil was the most commonly used drug, observed in the non-reversal group (64.7% vs 25.0%, p = 0.272).
Changes in SLEDAI and laboratorial data after immunosuppression in Reversion of SLE-PAH group and no-Reversion of SLE-PAH group.
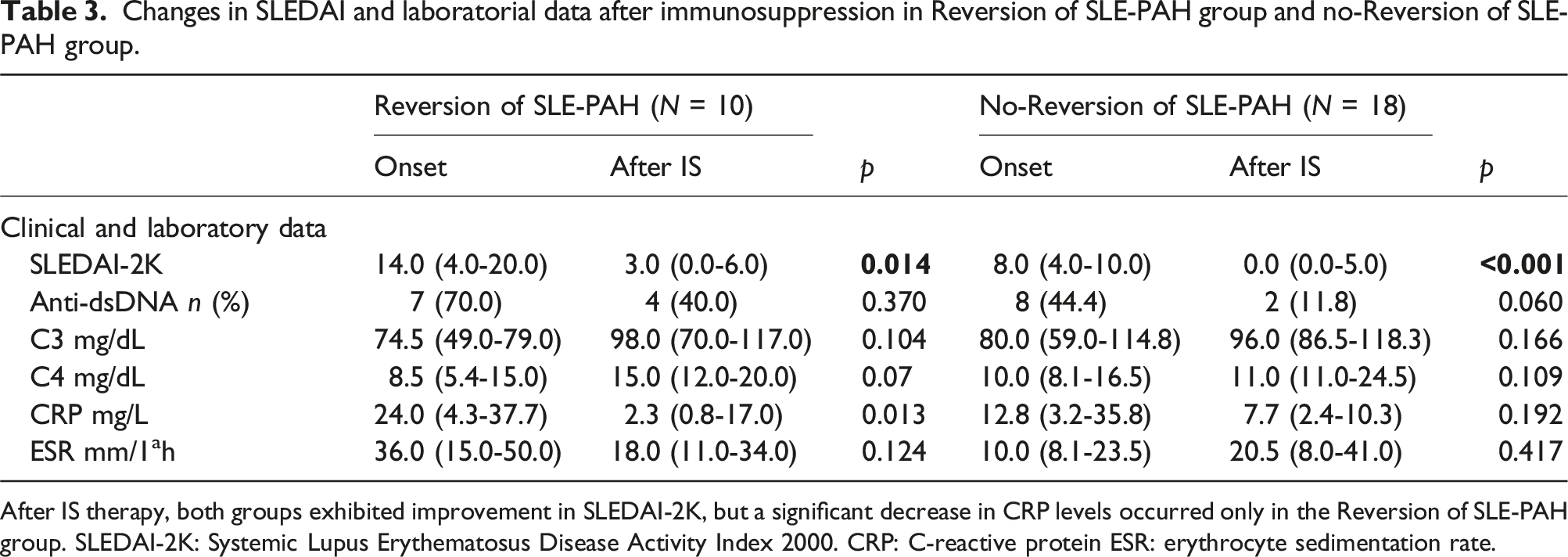
After IS therapy, both groups exhibited improvement in SLEDAI-2K, but a significant decrease in CRP levels occurred only in the Reversion of SLE-PAH group. SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index 2000. CRP: C-reactive protein ESR: erythrocyte sedimentation rate.
Changes of PAH parameters after immunosuppression in Reversion of SLE-PAH group and No-Reversion of SLE-PAH group.
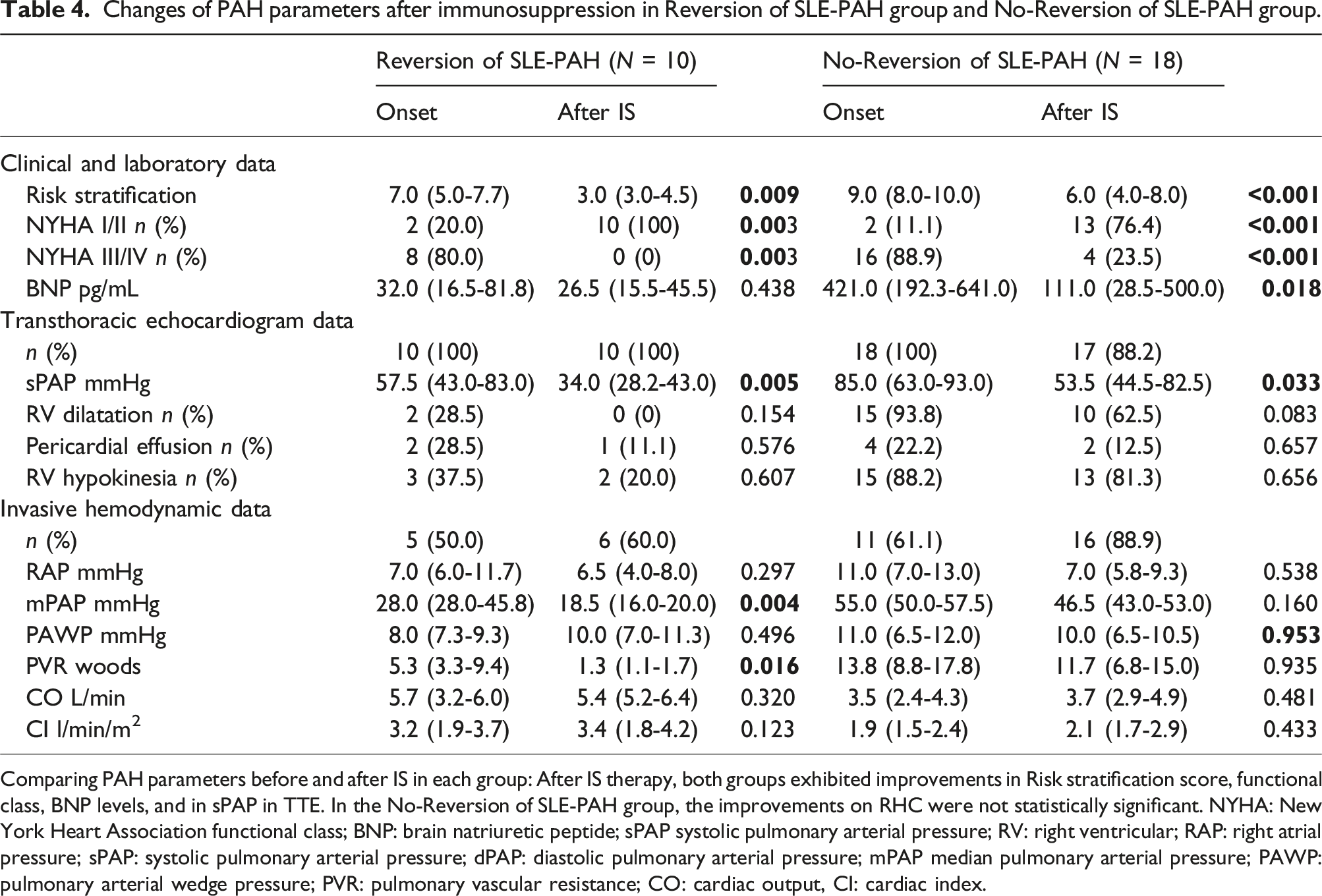
Comparing PAH parameters before and after IS in each group: After IS therapy, both groups exhibited improvements in Risk stratification score, functional class, BNP levels, and in sPAP in TTE. In the No-Reversion of SLE-PAH group, the improvements on RHC were not statistically significant. NYHA: New York Heart Association functional class; BNP: brain natriuretic peptide; sPAP systolic pulmonary arterial pressure; RV: right ventricular; RAP: right atrial pressure; sPAP: systolic pulmonary arterial pressure; dPAP: diastolic pulmonary arterial pressure; mPAP median pulmonary arterial pressure; PAWP: pulmonary arterial wedge pressure; PVR: pulmonary vascular resistance; CO: cardiac output, CI: cardiac index.
As illustrated in Figure 1, the Reversion of SLE-PAH group had a better survival compared to the No-Reversion of SLE-PAH group (p = 0.047). All deaths occurred in the No-Reversion of SLE-PAH group (n = 6) and all of them occurred in the first 2 years after PAH onset. Survival analysis according to PAH reversibility in Reversion of SLE-PAH group and No-Reversion of SLE-PAH group. Survival analysis according to PAH reversibility: The Reversion of SLE-PAH group exhibited better survival compared to the No-Reversion of SLE-PAH group. All deaths occurred in the first 2 years after PAH onset.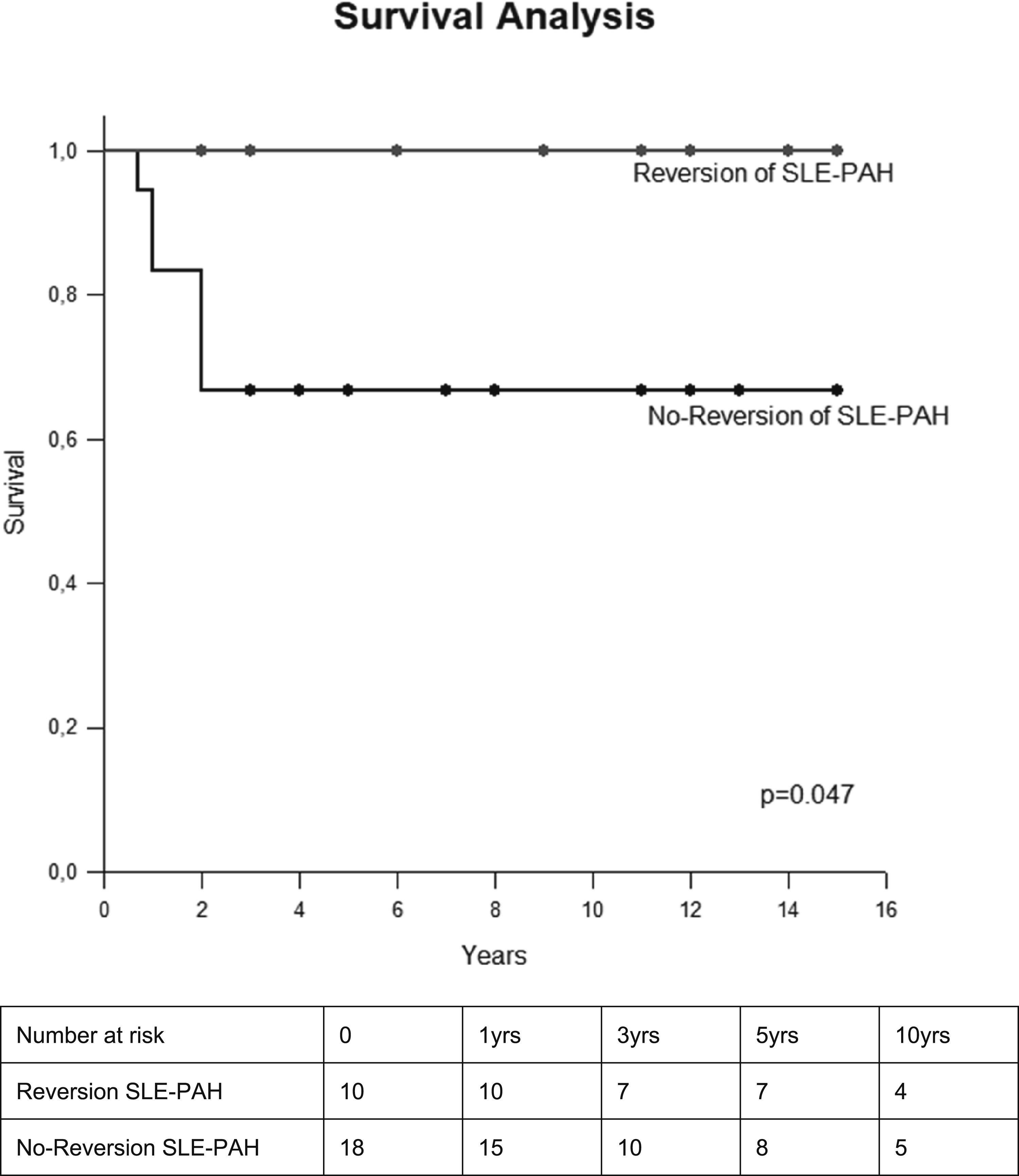
Discussion
This groundbreaking study is the first to demonstrate that more than one third of SLE patients with established PAH may experience a reversible transition to a normal PAP status. This finding contrasts with other forms of PAH considered an irreversible and progressive disease.
In reference to the characteristics of all SLE-PH patients, the most prevalent manifestations included arthritis, acute cutaneous lupus, serositis and the presence of anti-Ro antibodies. These findings align with previous studies that have established an association between serositis, the presence of anti-Ro, and anti-RNP with SLE-PAH.2,12,30–32 A predictive model assessing PAH in SLE also highlighted that acute/subacute cutaneous lupus and arthritis were linked with PAH development, particularly in the presence of anti-Ro/La and anti-RNP antibodies. 30
The inflammatory nature of PAH in SLE33–35 is reinforced by the present study since most of our patients exhibited active disease at onset of PAH, along with high SLEDAI2-K scores and elevated CRP/ESR levels. This observed pattern aligns with the proposed inflammatory hypothesis model for PAH 33 where the simultaneous diagnosis of both conditions supports the likelihood of vasculitic phenotype. 33 This particular phenotype has probably a more favorable outcome following IS therapy. 33
Importantly, in the present cohort, the reversibility of PAH appears to be more associated with severity of PAH rather than with the overall disease activity. In fact, none of the specific SLE activity parameters showed a significant correlation with PAH reversibility. Moreover, about one third of the patients in the Reversion of SLE-PAH group had PAH reversal despite presenting with low disease activity. Consistent with this finding, previous series assessing improvement rather than reversibility following IS therapy also reported that baseline factors such as better functional class and less severe hemodynamic values were not associated with SLEDAI scores.11,20 On the other hand, a crucial observation in the present study is the identification that higher mortality risk score, signs of RV dysfunction, such as elevated BNP levels, and the presence of RV dilatation and hypokinesia in TTE, were associated with absence of reversibility. The worse hemodynamic parameters (PVR, CO, CI) in the No-reversal of PAH, though notable, did not attain statistical significance. This may be attributed to the small sample size and further study with a large number of patients are necessary to confirm this finding.
Regarding treatment, previous small studies have suggested the beneficial effects of IS in association with PAH therapies in SLE-PAH.11,17–21 We confirmed and extended this observation demonstrating that IS induction therapy combined with PAH targeted therapies promoted a significant improvement and even complete reversal of this condition, as indicated by the change in risk stratification score. In fact, the predictive performance of REVEAL Lite was recently validated in SLE-PAH, 36 and this is the first study that used this validated risk score to evaluate the response after IS therapy in SLE-PAH.
Interestingly, the reduction of CRP levels after IS therapy was associated with the PAH reversibility. A significant decrease in CRP level was observed only in the Reversion of SLE-PAH group, whereas CRP levels remained stable in the other group, even though both studied groups presented similar decreases in SLEDAI-2K scores. CRP level was previously related to RV dysfunction in TTE parameters among SLE patients. 37 According to this finding, we hypothesize that CRP levels could be a potential marker of PAH activity in SLE patients, as suggested in other forms of PAH.38–40 Previous studies reported that patients with idiopathic PAH often exhibit elevated serum levels of cytokines, such as IL-1-b, IL-6, IL-8, chemokines38,39 and CRP levels.39,40 Of note, this latter parameter has been proposed as a prognostic parameter since it has been linked to severity and mortality in idiopathic, 40 congenital, 41 and thromboembolic pulmonary hypertension. 40 Considering all the evidence, the present study suggests a potential role for CRP as an inflammatory marker of PAH in SLE patients, despite not being an indicator of disease activity in SLE. 42
Another significant contribution of the present report is the unequivocal demonstration of SLE PAH reversibility. This finding suggests a paradigm shift from the concept that this condition is exclusively defined solely as damage in SDI score 28 and proposed its inclusion in the activity score of lupus. This alteration has practical clinical importance, emphasizing that IS therapy should always be considered in SLE-PAH patients.
In line with this recommendation, we observed that the persistence of PAH had a notable negative impact on survival rates. The Reversion of SLE-PAH group exhibited a 100% survival rate, while among patients with persistent PAH, the pooled 1- and 3-years survival rates were 94.4% and 66.7% respectively. These findings align with the well-established knowledge on the impact of PAH on the survival of SLE patients.11,43–45 Accordingly, a recent systematic review and meta-analysis of SLE-PAH that included 323 SLE patients, reported the pooled 1-, 3-, and 5-years survival rates of 88% (95% CI, 0.80-0.93), 81% (95% CI, 0.67-0.90), and 68% (95% CI, 0.52-0.80). 45
One strength of this study is the homogeneity of the lupus patients classified according to established criteria 23 and the use of standardized clinical electronic prospective protocol established in our clinic. These factors may have minimized potential biases associated with the retrospective nature of our study. Despite the relatively small sample size, it’s noteworthy that this study boasts the largest cohort among Western studies specifically examining the impact of immunosuppressive therapy in SLE patients with PAH. Additionally, as a retrospective study, we lacked robust information on exercise capacity, such as the six-minute walk test, an important parameter in disease assessment. Moreover, in the evaluation of PAH, another limitation of the study was the inclusion of patients without invasive hemodynamic evaluation, which was partially addressed by including only patients who had TTEs with sPAP≥40 mmHg. This test was reported to have a high sensitivity and specificity in predicting PAH in SLE.2,46 In addition, all patients included were symptomatic and/or those with features of RV overload (RV dilatation or hypokinesia or high BNP levels); and, indeed, there were no discrepancies in diagnosis between TTE and RHC in patients who underwent both procedures. Another limitation was the lack of a placebo group, preventing us from determining the precise effect size of IS in PAH-SLE. Nonetheless, considering the known progression of other forms of PAH, it is unlikely that the observed normalization of PAP would have occurred without IS therapy.
In conclusion, this is the first study that unequivocally establishes the potential complete reversibility of PAH in SLE patients after induction IS therapy particularly in those with less severe cardiac involvement and its positive impact on the survival of these patients. Our findings also highlighted the possible inflammatory nature of this condition and thus the importance of its appropriate management for all patients with this complication. Further studies should be performed to confirm and expand our knowledge about mechanisms and other therapies of PAH in SLE.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (#305242/2019–9 to EB; #303116/2022–6 to SGP; and #303378/2022–0 to EFB).