
Abstract
Objective
Cognitive impairment (CI) in systemic lupus erythematosus (SLE) is quite common and is an important prognostic factor due to its severity. The aim of our study was to determine the proportion and type of CI in SLE and to identify associated risk factors.
Methods
We performed a cross-sectional study (January - March 2022). Participants included SLE patients and controls (No-SLE). SLE patients were subdivided into those with and those without CI to identify associated risk factors. CI was defined based on the results of eight specific tests assessing various cognitive functions, with MMSE used for overall cognitive assessment. Impairment was indicated by abnormalities in at least five of these eight functions.
Results
Our study included 60 lupus and 40 non-lupus participants. The median disease duration of patients in the SLE group was 72 months (interquartile range: 24 – 150 months). The proportion of cognitive impairment in SLE was 31.7%. The comparative study of cognitive functions between the two groups of participants with and without SLE concluded that executive functions and verbal fluency were more impaired in the lupus group compared to the non-lupus group. It also concluded that there were no statistically significant differences in attention and concentration, episodic memory, working memory, calculation, visuospatial and visuoconstructive activity, or judgement. In the multivariate analysis, patients with SLE have a significantly higher risk of CI (Adjusted OR 3.76, 95% CI: 1.217 – 11.621) compared to non-SLE individuals. Each additional year of age increases the risk by 4.4% (Adjusted OR 1.044, 95% CI: 1.008 – 1.082). For factors associated with CI in SLE, the multivariate analysis concluded that the duration of corticosteroid therapy, by months, had an adjusted OR equal to 1.009 (CI (95%): 1.000–1.018), and the duration of education, by years, had an adjusted OR equal to 0.857 (CI (95%): 0.736–0.999).
Conclusion
Screening for CI in lupus patients is important, especially for those with factors associated with these disorders such as prolonged duration of corticosteroid therapy and shortened schooling.
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease with a wide range of clinical expressions. Neurological involvement in SLE is quite frequent and represents an important prognostic factor due to its severity. Cognitive impairment (CI) is quite common and heterogeneous in its clinical presentation and severity. The proportion of CI in SLE is 5–79%. 1 CI is one of the central neurological manifestations that may be related to SLE and has been included in the 1999 American College of Rheumatology (ACR) nomenclature. 2 Their causes are often multiple and interrelated. Few studies have investigated CI in SLE.
In SLE, the high risk of cerebrovascular and cardiac events, immune dysregulation, and pro-inflammatory cytokines contribute to and increase the risk of CI. SLE and CI, which share a chronic inflammatory character, may accelerate the progression to dementia.3–5
CI is sometimes overlooked by clinicians. Nonetheless, CI has a significant impact on patients’ emotions and functional outcomes, and it is intimately related to their quality of life. CI affects the social, family, and professional integration of patients and can have repercussions on medical follow-up, treatment adherence, and compliance.6,7 Prioritising the early detection of CI in lupus patients can prevent irreversible damage and also benefit society by lowering the expenses associated with their functional impairment.
The objectives of this study were to determine the proportion and type of cognitive disorders in SLE and to identify the risk factors associated with cognitive impairment in patients with systemic lupus erythematosus.
Methods
Study design
We carried out a cross-sectional study in the Internal Medicine Department of the Habib Thameur University Hospital in Tunis from January to March 2022.
Patients
We included participants who were being followed in our Internal Medicine Department for SLE and/or chronic disease (hypertension, diabetes, and thyroid disease) and healthy participants. All participants were over 18 years of age. We did not include participants with clinically and/or radiologically confirmed central neurological involvement or systemic granulomatosis and/or primary systemic vasculitis, or those with stroke, psychosis, seizures, and a self-reported cognitive complaint. To ensure patients with a stroke were not included, all participants had no history of stroke, no clinical neurological signs suggestive of stroke, and underwent a cerebral (computed tomography) CT scan that revealed no evidence of either recent or past stroke. SLE and Sjogren’s disease were the only autoimmune connective tissue diseases that were included in our study. We excluded participants who requested to leave the study. We studied the demographic, clinical, biological, and therapeutic characteristics of the participants.
Study groups
The participants in this study were divided into two groups: • SLE group included participants followed for SLE (according to the ACR 1997 revised classification criteria
8
). • No-SLE group included participants free of SLE: patients followed for chronic diseases and healthy volunteers. SLE was excluded in participants from this group following a medical history evaluation, physical examination, complete blood count, urinalysis, and chest radiography.
To identify the factors associated with CI in SLE, we subdivided patients with SLE into two groups: • The wCI group included lupus patients with CI. • The woCI group included lupus patients without CI.
Assessment of cognitive functions
Overall cognitive efficiency was assessed with the mini-mental state examination (MMSE). We used a validated version in Arabic Tunisian dialect.9,10 Cognitive functions were assessed as follows: attention and concentration were assessed by the Zazzo test, 11 calculation by a subtraction test (100-7= , etc.), working memory by the Digit Span Task, 12 episodic memory by the Tunisian Verbal Learning Test (adaptation of the Californian Verbal Learning Test),13,14 visuospatial and visuoconstructive function by the Clock Drawing Test, 15 executive functions by the Frontal Assessment Battery (FAB), 16 judgement by the explanation of three proverbs, and verbal fluency by the Phonetic and Categorical Verbal Fluency Test (according to age, gender, and education level of Cardebat D. 1990). 17
In our study, the presence of at least five abnormal cognitive functions out of the eight examined cognitive functions was considered cognitive impairment. 18
All patients were screened for depressive symptoms according to their respective ages: the Beck-II Depression Inventory (21 items) in Arabic19,20 for participants under 65 years old, or the Geriatric Depression Scale (30 items) in Arabic21,22 for elderly participants.
Statistics analysis
Statistical analyses were performed using the SPSS 26.0 trial version. Quantitative variables were summarised by the mean ± standard deviation, median values (25% and 75% percentiles). Qualitative variables were presented as numbers and percentages. The presence of a difference between the independent groups in terms of categorical variables was examined using the Pearson Chi-square test or Fisher’s exact test. Before the comparison of quantitative variables, it was checked whether the assumptions of the parametric test were satisfied or not. While conformity to the normal distribution was assessed using the Kolmogorov-Smirnov (or Shapiro-Wilk) test, homogeneity of variances was assessed using the Levene test. The presence of a difference between the independent groups in terms of quantitative variables was investigated using the Student's t-test for independent samples in the case that the assumptions of the parametric test were met and using the Mann-Whitney U test in the case that these assumptions were not met. For the identification of factors associated with cognitive disorders, the adjusted Odds Ratio (OR) was calculated with multivariate analysis, performing a binary logistic regression using as co-variables: variables with a statistically significant difference between the SLE and No-SLE groups, those with a p-value ≤0.10 and a forced variable that is age. After comparing the wCI and woCI groups, the Odds Ratio (OR) of factors associated with CI in SLE was calculated. The multivariate analysis was analysed by a binary logistical regression using as co-variables: variables with a statistically significant difference between the wCI and woCI groups and those with a p-value ≤0.10. The level of significance was set up at p ≤ 0.05.
Ethical considerations
All participants agreed and signed informed consent. Consent to publish has been obtained from all participants. This study was presented to the ethics committee of Habib Thameur University Hospital and received its approval (Project Reference: HTHEC-2021-21).
Results
Demographic, clinical and biological characteristics of participants.
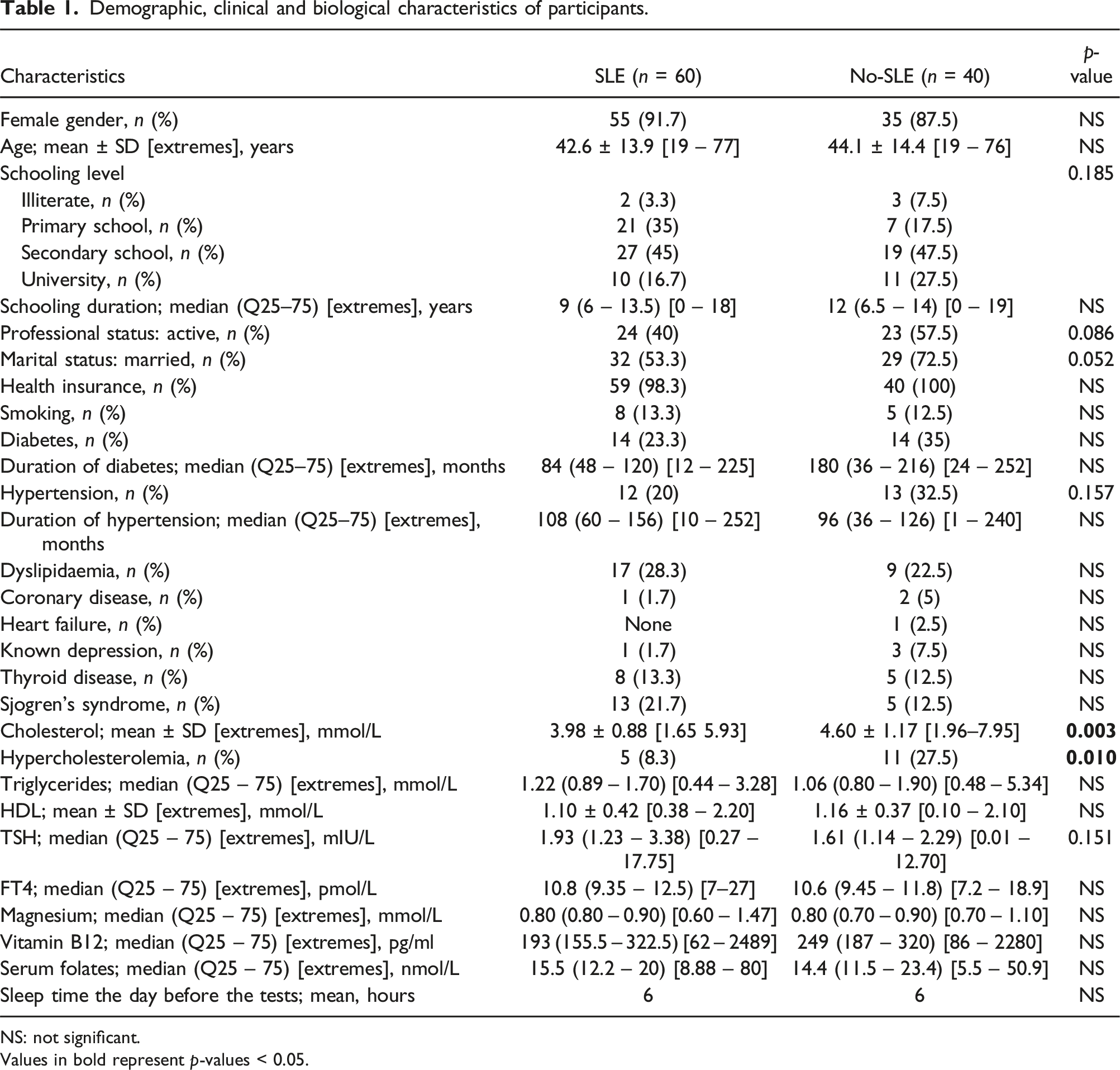
NS: not significant.
Values in bold represent p-values < 0.05.
The comparative study between the two groups concluded a lower median MMSE score for the SLE group compared to the No-SLE group, 25 and 27.5, respectively; p = 0.029. The mean FAB score was lower in the SLE group compared to the No-SLE group, 13.56 ± 4.03/18 versus 15.37 ± 2.84/18, respectively (p = 0.024); and a lower mean score of alternate fluency and motor sequence in SLE compared with No- SLE, respectively 2.0 ± 1.0 versus 2.5 ± 0.7; p = 0.006; and 2.1 ± 1.1 versus 2.6 ± 0.7; p = 0.014. The proportion of altered executive functions was higher in the SLE group compared to the No-SLE group, respectively 58.3% versus 37.5%; p = 0.041. The correlation study for lupus patients (SLE group) between the MMSE score and the FAB score showed a strong positive correlation (r = 0.593; p < 0.001). The proportion of pathological verbal fluency was higher in the SLE group compared to the No-SLE group, 26.7% versus 10% respectively; p = 0.041. The comparative study of the number of impaired cognitive functions found a higher mean in the SLE group compared to the No-SLE group, 3.41 ± 1.79 versus 2.57 ± 1.78 respectively; p = 0.023. The proportion of cognitive impairment (≥5 of 8 impaired cognition functions) was higher in the SLE group compared to the No-SLE group, respectively 31.7% versus 12.5%; p = 0.028.
The median BECK II score was higher in the SLE group (n = 55) compared to the No-SLE Group (n = 36), respectively 13 (Q25–75: 9.5 – 22.5) [extremes: 0 – 44] versus 7 (Q 25%–75%: 4.5 – 12) [ extreme: 2 – 52]; p = 0.001. The median GDS score was lower in the SLE group (n = 5) compared to the No-SLE group (n = 4), respectively 4 (Q25%–75%: 4 – 14) [extremes: 4–14] versus 8 (Q 25-75: 5 – 10.5) [extreme: 4 - 11]; p = 0.905. Based on the Beck-II score or the GDS score, the proportion of depressive symptoms was higher in the SLE group compared to the No-SLE group, 71.7% versus 35% respectively; p < 0.001. The correlation study for lupus patients (SLE group) between MMSE score and BECK II score showed a low negative correlation (r = −0.448; p = 0.001). The correlation study for lupus patients (SLE group) between the FAB score and the BECK II score showed a low negative correlation (r = −0.434; p = 0.001).
Comparative analysis of cognitive functions and depressive symptoms assessment of participants in the lupus group and non-lupus group.
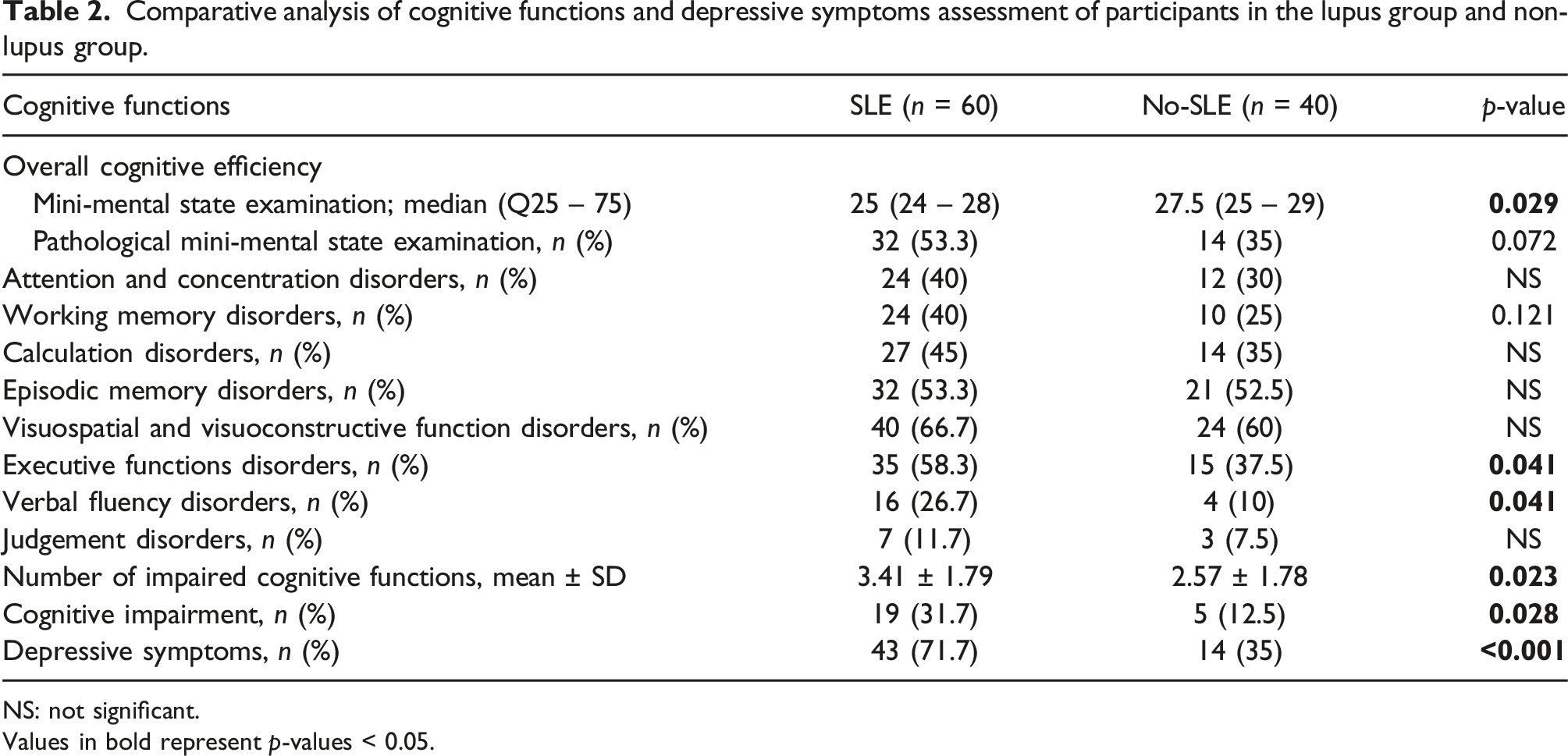
NS: not significant.
Values in bold represent p-values < 0.05.
A multivariate analysis of factors associated with cognitive impairment, adjusted for hypercholesterolemia, Sjögren’s syndrome, and marriage.

Values in bold represent p-values < 0.05.
Comparative analysis of epidemiological characteristics, comorbidities, and diagnostic criteria ACR 1997 between two SLE groups with and without cognitive impairment.
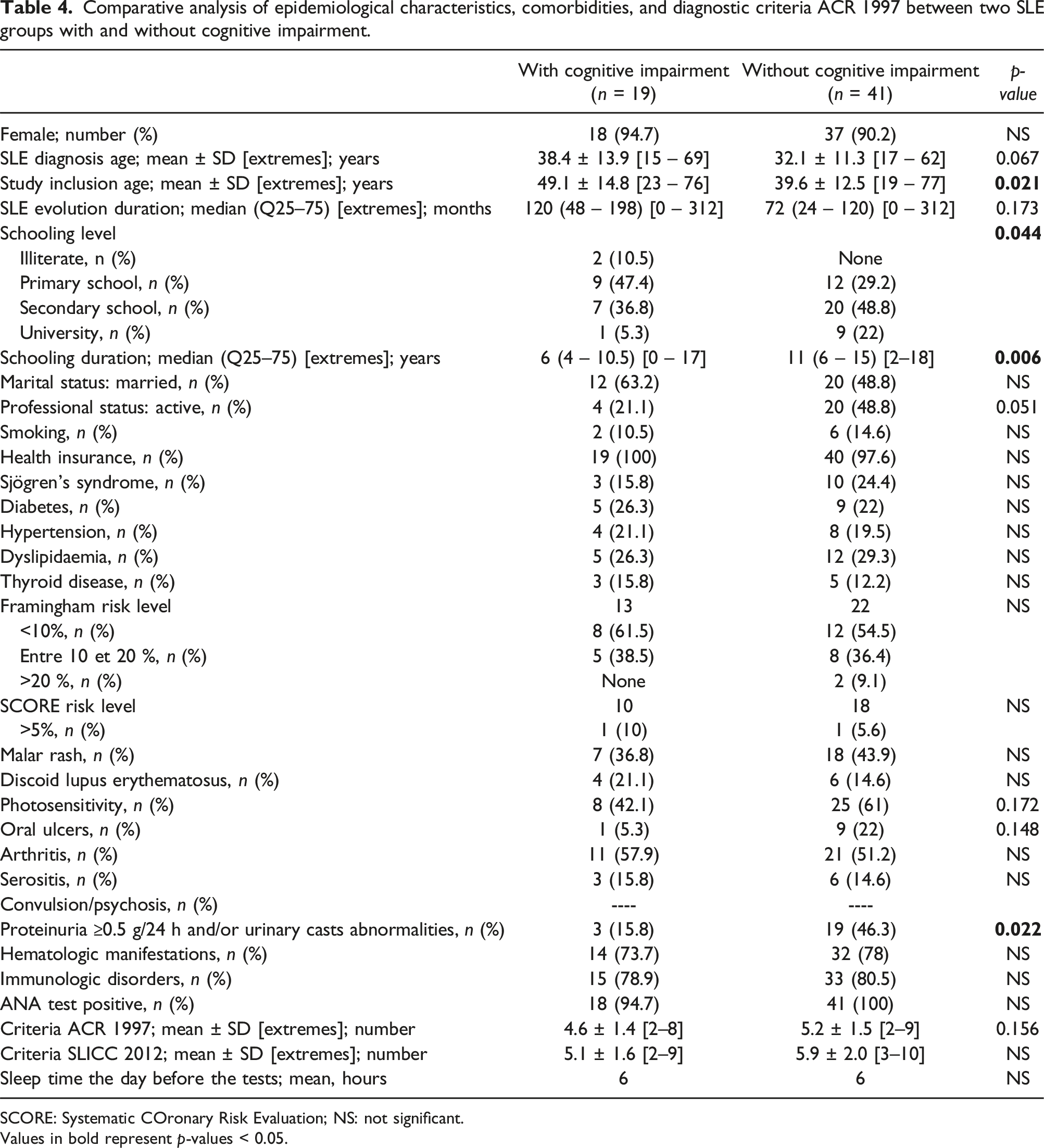
SCORE: Systematic COronary Risk Evaluation; NS: not significant.
Values in bold represent p-values < 0.05.
Comparative study of cumulative systemic manifestations, immunological data, biological data, and therapeutic data between the two SLE groups with and without cognitive impairment.
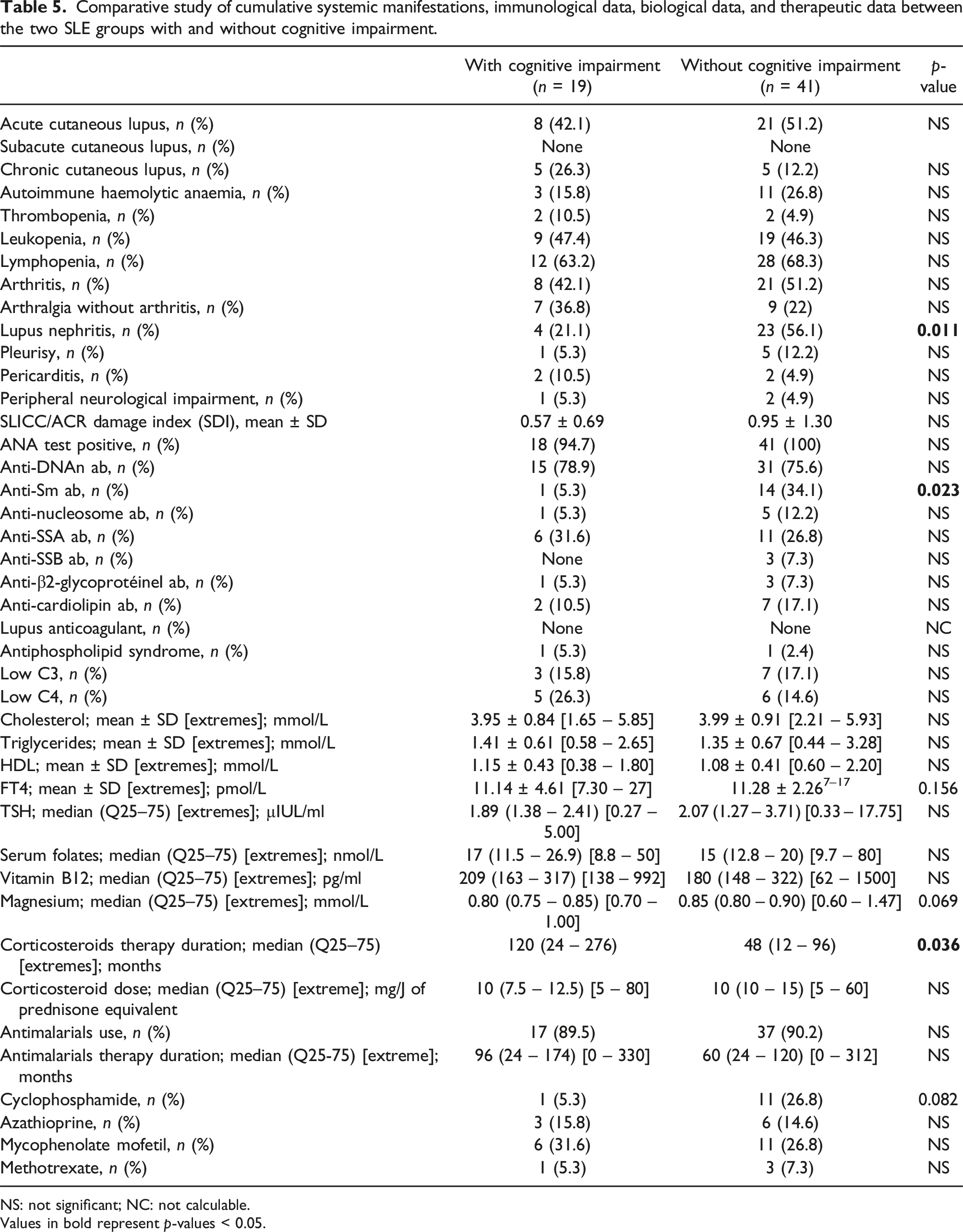
NS: not significant; NC: not calculable.
Values in bold represent p-values < 0.05.
The proportion of depressive symptoms in the wCI and woCI groups was not significantly different, 78.9% versus 68.3% respectively; p = 0.394.
Age-adjusted multivariate analysis of factors associated with cognitive impairment in systemic lupus erythematosus.

Discussion
To ensure inclusivity, our study included illiterate participants, who were accommodated using tests not reliant on literacy, such as the Clock Drawing Test, and provided oral instructions for other assessments. The proportion of illiterate participants was 3.3% in the SLE group and 7.5% in the No-SLE group (non-significant p-value). This approach aimed to minimize potential biases and accurately reflect cognitive impairment across different literacy levels.
The literature indicates that it is challenging to ascertain the proportion of CI in SLE. The small number of studies, the various definitions of CI that the authors chose, and the selection of neuropsychological instruments would all help to explain this. Depending on the series, the proportion of CI in SLE is quite variable, 5–79%. 1 Al Rayes H et al. demonstrated that this high variability was secondary to the studied lupus population, the neuropsychological tools used, and the number of domains affected to diagnose a CI. In this study, we defined cognitive dysfunction using the criteria for severe cognitive impairment (deficits in five or more cognitive domains), as this threshold allows us to identify individuals with significant and pervasive cognitive deficits. 18 This approach enhances the specificity of our findings and ensures that the identified cases of CD reflect a level of impairment with considerable clinical and functional relevance.
The pathological cognitive functions in our study were essentially executive functions and verbal fluency. Rare are the studies that have specified the cognitive areas (domains) affected by SLE. Although there is no specific profile of CI in patients with SLE, studies have shown that verbal and non-verbal learning, as well as working memory, are the areas most affected, followed by deficits in simple attention and psychomotor speed.
Executive functions (planning and multitasking) are also affected in SLE patients. Kozora et al. found a high incidence of non-verbal learning, memory, and verbal fluency disorders. 23 Mahdavi Adeli et al. noted that the areas most affected were orientation, memory, language, and executive function. 24 Anxiety and depression are mainly correlated with areas included in the MMSE test. 25
Yue et al. found that the most frequently affected areas were delayed recall (80.5%), abstract generalisation (79.2%), repetition, and fluency of language (76.6%). 26 Tomietto et al. showed that the areas most involved were memory (50%), complex attention (42.3%), and executive functions (26.9%). 25 Appenzeller et al. found that the cognitive areas most affected were memory and executive functions (planning, organisation, and working memory). 27 These patients suffered from depression and anxiety and continued to experience all these difficulties over the course of a year. Patients with depression and anxiety tended to have difficulties in more complex cognitive areas such as memory and executive functions.
In 10 case-control studies, a battery of extensive neuropsychological tests was used to identify cognitive impairment in 41 out of 266 healthy persons (15.4%) and 182 out of 483 SLE patients (37.7%). SLE patients had a higher risk of developing CI compared to healthy subjects, with an RR of 2.80 (95% CI: 2.06–3.81). 1 These results are quite close to our results. Generally, the prevalence of subjective cognitive complaints may exceed that of objective cognitive impairments. This discrepancy can be attributed to patients potentially overstating their symptoms or conflating specific cognitive functions, such as memory (both working and episodic), with attention and concentration. In our study, the significant proportion of cognitive impairments observed among participants who did not report cognitive difficulties could be due to a lack of awareness or difficulty articulating cognitive issues. Typically, patients link cognitive disorders predominantly with memory problems. However, our findings revealed that executive function and verbal fluency—functions less frequently acknowledged by patients—were more severely impaired compared to the control group.
Several studies have noted that cognitive impairment may affect patients with Sjögren’s disease. Our study included participants with Sjögren’s disease in both the SLE group and the non-SLE group (21.7% vs 12.5%, p-value not significant). To account for the potential influence of Sjögren’s disease on cognitive impairment, we conducted a multivariate analysis with Sjögren’s disease as a covariate. The analysis demonstrated that SLE and age were significant risk factors for cognitive impairment, while Sjögren’s disease was not found to have a significant impact.
In our investigation, factors associated with cognitive impairment in lupus patients were longer corticosteroid therapy duration and shorter schooling duration. Some studies have shown a significant correlation between a reduced number of years of study and an increased risk of CI. Yue et al. showed that patients with a short schooling period had consistently lower cognitive performance. 26 Lupus patients with a longer duration of study had a lower risk of developing cognitive impairment compared to those with a shorter duration. A Pakistani study showed that the level of education was not associated with CI in SLE. 28 Glucocorticoids, which are the pillar of SLE treatment, have been identified as risk factors for CI. The association between prednisone and CI varied from study to study, ranging from a significant association 29 to the absence of a significant association. 30
Several factors associated with CI in SLE were reported, such as male sex, age, lupus disease duration, unemployment, a higher disease activity score, the presence of antiphospholipid antibodies, obesity, dyslipidaemia, and poor sleep quality.
Our study was designed with careful patient selection and controlled environmental factors, though these choices introduce certain limitations. The monocentric nature of our research and the moderate sample size resulted from our stringent non-inclusion criteria. We did not include patients with central neurological involvement, psychosis, seizures, stroke, or spontaneous cognitive complaints, as well as those with connective tissue diseases other than systemic lupus erythematosus (SLE) and Sjögren’s disease, to maintain a more homogeneous study population.
Additionally, we limited the study duration to 3 months to minimise the influence of extended external events on our findings. Conducting the study within a single season also helped to reduce the impact of seasonal variability. While these decisions were made to ensure rigour, they should be considered when interpreting the generalisability of our findings.
Conclusions
Our study showed that the proportion of CI in SLE was not negligible. Executive function disorders and verbal fluency disorders were the majority of cognitive functions affected in SLE. Our study identified that SLE and age were factors associated with CI. So, lupus patients would be a population at risk of developing CI. Hence the need to diagnose cognitive disorders in patients with SLE at best at the asymptomatic stage or at mild cognitive impairment. Our study identified two modifiable risk factors for CI in lupus patients, namely the duration of corticosteroid therapy and schooling duration. Reducing the duration of corticosteroid therapy and increasing the length of schooling in SLE could reduce the risk of developing CI.
Footnotes
Acknowledgments
We would like to acknowledge the kind contributions of our volunteers’ and patients’ time.
Author contributions
All authors contributed to the drafting or revising of the article for important intellectual content. All authors approved the final version of the article to be published. Study conception and design: ABB, MS, FD, IR, IA, BBD, HB, ZA, FB. Acquisition of data: ABB, MS. Analysis and interpretation of data: ABB, MS, FD, IR, IA, BBD, HB, ZA, FB.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.