
Abstract
Background
Mycophenolate mofetil (MMF) is widely used to treat systemic lupus erythematosus (SLE), particularly in cases with severe and organ-threatening complications such as lupus nephritis. However, multiple reports have documented lymphoproliferative disorder (LPD) in patients with SLE undergoing MMF therapy, predominantly developing in the central nervous system and requiring aggressive treatment, including chemotherapy, radiation, and surgery.
Case Report
We herein report the case of a 58-year-old female patient with SLE who developed cervical, hepatic hilar, and para-aortic lymphadenopathy 8 years after initiating MMF treatment. Histopathological examination of the left cervical lymph node revealed features consistent with polymorphic LPD. MMF was discontinued, and after 2 months of surveillance, the enlarged lymph nodes regressed without need for additional treatment.
Conclusion
To the best of our knowledge, this is the first reported case of MMF-associated LPD occurring outside the central nervous system in a patient with SLE, which resolved spontaneously upon MMF withdrawal. Clinicians should remain vigilant regarding the possibility of MMF-associated LPD when administering MMF to patients with SLE.
Keywords
Background
Patients with systemic lupus erythematosus (SLE) are known to have an elevated risk of developing lymphoproliferative disorder (LPD). 1 Although the pathogenesis remains unclear, immune deficiency resulting from SLE itself or from immunosuppressive therapy is considered a potential cause of LPD. It is hypothesized that a compromised immune system leads to impaired antitumor immunity or increased susceptibility to Epstein-Barr virus (EBV) reactivation, thereby resulting in the uncontrollable proliferation of aberrant lymphocytes.2,3 Mycophenolate mofetil (MMF) is an antimetabolite immunosuppressant widely used in the treatment of SLE, particularly lupus nephritis. However, MMF use increases the risk of LPD in patients who have undergone organ transplantation or have autoimmune diseases. 4 In patients with SLE, multiple cases of MMF-associated LPD have been reported, all of which primarily developed in the central nervous system (CNS) and required aggressive treatment.5–17 This report details a case of a female with SLE who developed MMF-associated LPD with generalized lymphadenopathy outside the CNS, and achieved spontaneous remission solely with the discontinuation of MMF.
Case presentation
A 58-year-old female Japanese patient with a 35-year history of SLE, complicated by lupus nephritis class Ⅳ(G)-A + class Ⅴ and lupus mastitis, visited our hospital for a routine check-up, complaining of a swelling on the left side of the neck. The patient did not suffer from fever or malaise. Her treatment consisted of 2 g of MMF and 200 mg of hydroxychloroquine (HCQ) daily for the past 8 years, during which SLE remained well controlled, with an SLE disease activity index 2000 (SLEDAI-2K) of 0/105. The patient had an anti-DNA antibody titer of <10 IU/mL (47 IU/mL at the time of SLE onset) as determined by the radioimmunoassay method, and an antinuclear antibody titer of <1:40 (1:640 with a homogenous and speckled pattern at the time of SLE onset). Before the initiation of MMF and HCQ, the patient had received immunosuppressive therapy with intravenous cyclophosphamide, mizoribine, and tacrolimus, more than 8 years prior to the development of LPD (Supplementary Figure 1).
Ultrasound examination revealed multiple enlarged bilateral cervical lymph nodes. A decline in the lymphocyte counts from 1620/μL 1 year prior to the current examination to 940/μL was noted, alongside an increase in the C-reactive protein (CRP) levels from 0.11 mg/dL to 0.73 mg/dL over the same period. Computed tomography (CT) revealed enlarged cervical, hepatic hilar, and para-aortic lymph nodes (Figure 1(a) and (b)); however, no lesions were observed on brain magnetic resonance imaging. Histological analysis of a biopsy specimen of the left cervical lymph node revealed an absence of follicular structures with notable proliferation of small to medium-sized CD3 (+) lymphoid cells and partial mingling of relatively large T cells and B cells (Figure 2(a) to (d)). EBV-encoded small RNA was negative on in situ hybridization of the lymph node specimen, and human herpes virus-8 was negative on immunohistochemical staining. Based on these findings, other iatrogenic immunodeficiency-associated LPD was diagnosed according to the World Health Organization classification, with histological features consistent with polymorphic LPD. Computed tomography findings. (a, b) Multiple enlarged lymph nodes (arrow) observed in the left cervical (a) and para-aortic (b) region at the time of onset. (c, d) Regression of the left cervical (c) and para-aortic (d) lymph nodes observed 2 months after MMF discontinuation. Histological findings of the left cervical lymph node. (a) 40x hematoxylin-eosin (HE) staining revealed an absence of follicular structures in the lymph node. (b) 200x HE staining showed a proliferation of small to medium-sized lymphoid cells and partial mingling of relatively large T cells and B cells. (c) 200x CD20 immunohistochemical (IHC) staining demonstrated the distribution of CD20 (+) B cells. (d) 200x CD3 IHC staining demonstrated the distribution of CD3 (+) T cells.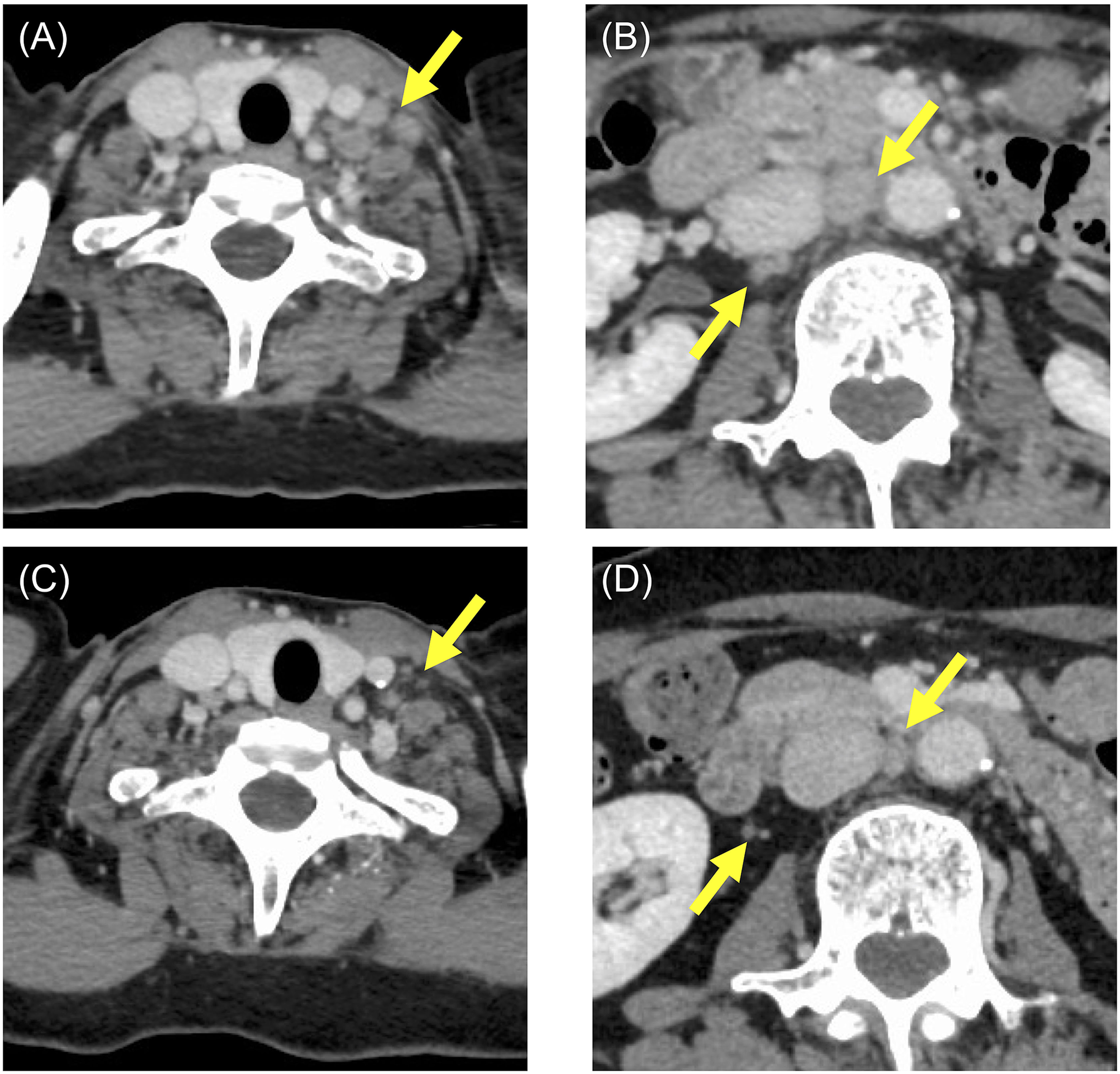

MMF therapy was discontinued, and after 2 months of close surveillance, follow-up CT revealed spontaneous regression of the cervical, hepatic hilar, and para-aortic lymph nodes (Figure 1(c) to (d)). Lymphocyte count (2200/µL) and CRP level (0.22 mg/dL) also normalized. Azathioprine was initiated 5 months after MMF discontinuation (Supplementary Figure 1). 19 months after discontinuing MMF therapy, the patient is currently receiving HCQ and azathioprine, without experiencing an SLE flare or LPD recurrence.
Discussion
Clinical characteristics of previous cases of MMF-associated LPD in patients with SLE and other autoimmune diseases.
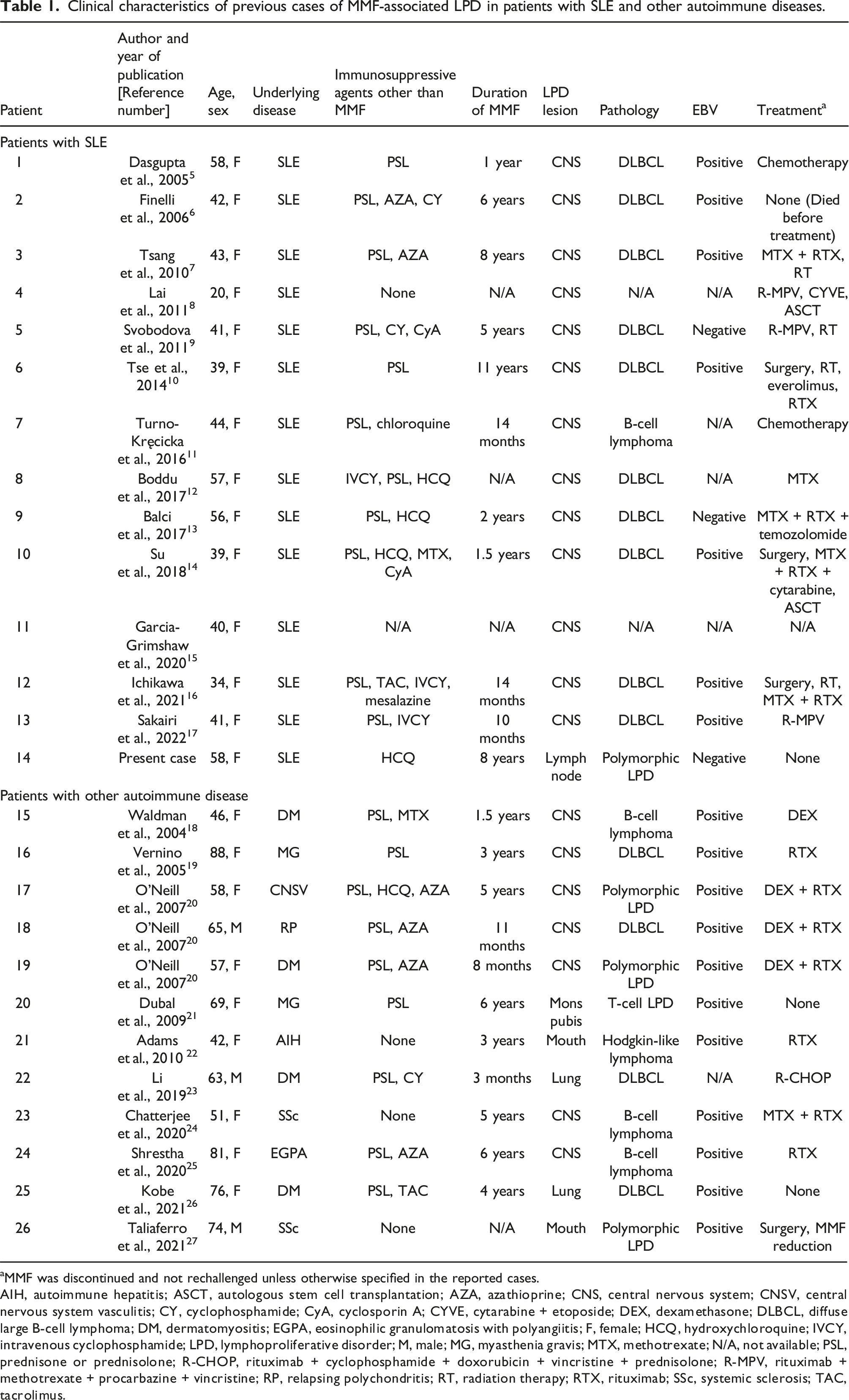
aMMF was discontinued and not rechallenged unless otherwise specified in the reported cases.
AIH, autoimmune hepatitis; ASCT, autologous stem cell transplantation; AZA, azathioprine; CNS, central nervous system; CNSV, central nervous system vasculitis; CY, cyclophosphamide; CyA, cyclosporin A; CYVE, cytarabine + etoposide; DEX, dexamethasone; DLBCL, diffuse large B-cell lymphoma; DM, dermatomyositis; EGPA, eosinophilic granulomatosis with polyangiitis; F, female; HCQ, hydroxychloroquine; IVCY, intravenous cyclophosphamide; LPD, lymphoproliferative disorder; M, male; MG, myasthenia gravis; MTX, methotrexate; N/A, not available; PSL, prednisone or prednisolone; R-CHOP, rituximab + cyclophosphamide + doxorubicin + vincristine + prednisolone; R-MPV, rituximab + methotrexate + procarbazine + vincristine; RP, relapsing polychondritis; RT, radiation therapy; RTX, rituximab; SSc, systemic sclerosis; TAC, tacrolimus.
Similar cases of MMF-associated LPD have been reported in 12 patients with autoimmune diseases other than SLE (Table 1).18–27 Among these, five cases involved non-CNS LPDs occurring in the lung, mouth, and mons pubis.21–23,26,27 Three cases exhibited a pathological feature consistent with polymorphic LPD,20,27 and one case was identified as T-cell LPD. 21 Spontaneous remission was achieved in two cases solely through MMF withdrawal,21,26 whereas one case was administered only dexamethasone in addition to MMF discontinuation. 18
Histological analysis of the present case revealed a polymorphic LPD pattern; however, EBV-encoded small RNA were not detected, unlike previous cases of MMF-associated LPD with SLE, which predominantly involved EBV-related diffuse large B cell lymphomas (DLBCL). 17 Among the 13 previously reported cases, 11 were identified as DLBCL, while the pathology of the remaining two cases was unspecified. EBV status was reported as positive, negative, and not mentioned in seven, two, and four cases, respectively. Interestingly, a pathological feature of polymorphic LPD has been associated with a favorable prognosis in patients with rheumatoid arthritis (RA) who developed methotrexate (MTX)-associated LPD. 28 This observation aligns with the outcome of the current case, which demonstrated self-remission following the withdrawal of MMF therapy.
In the current case, a gradual decrease in the lymphocyte counts and an increase in CRP levels were observed before LPD development, both of which promptly resolved after the discontinuation of MMF. A similar trend was reported by Inui et al. in patients with RA who developed MTX-associated LPD, where early lymphocyte recovery 2 weeks after MTX withdrawal predicted a spontaneous regression of LPD at 1 month. 29 In the present case, the lymphocyte count increased from 940/μL to 1870/μL 1 month after MMF withdrawal, and to 2200/μL after 2 months. Lymphadenopathy regressed 1 month after the discontinuation of MMF, with confirmation by CT imaging 2 months later. These findings suggest that the observation made by Inui et al. may also be relevant to MMF-associated LPD; however, further studies are required to confirm this hypothesis.
Conclusions
Clinicians should be aware of the possibility of LPD occurring in patients with SLE receiving MMF. The present case demonstrated that MMF-associated LPD can occur in the lymph nodes outside the CNS. When MMF-associated LPD is suspected, the possibility of spontaneous regression should be considered, as this may help avoid unnecessary and potentially harmful treatment, particularly when polymorphic LPD is histologically diagnosed and recovery of the lymphocyte counts is observed following MMF withdrawal.
Supplemental Material
Supplemental Material - Reversible lymphoproliferative disorder in systemic lupus erythematosus treated with mycophenolate mofetil: A case report and literature review
Supplemental Material for Reversible lymphoproliferative disorder in systemic lupus erythematosus treated with mycophenolate mofetil: A case report and literature review by Hiroto Tomoda, Muneo Nakaya, Seiichiro Nakabeppu, Hiroaki Miyoshi, Koichi Ohshima and Yuji Miyoshi in Lupus
Footnotes
Author’s Note
A part of this case report was presented in an oral session at the 690th Kanto Region Meeting of the Japanese Society of Internal Medicine on October 14, 2023.
Authors’ contributions
Y.M., H.T., and M.N. contributed to the patient’s care. S.N, H.M, and K.O. reviewed the pathological findings. Y.M. conceived the study. H.T. prepared the manuscript. All authors critically reviewed and revised the manuscript for intellectual content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
The clinical data used and/or analyzed during the current case report are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.