
Abstract
Systemic lupus erythematosus (SLE) is characterized by multiple organ involvements. One notable manifestation of SLE is thyroid disease, which has been documented in various studies with significant variability in prevalence and presentation. Observational studies have indicated that thyroid dysfunction, particularly autoimmune thyroid disease (AITD) characterized by hypothyroidism, is commonly associated with SLE. Despite these observation, the exact relationship between SLE and thyroid disease still remain poorly understood. Several factors may contribute to the pathogenesis of SLE companied with AITD, including genetic susceptibility, environmental influences, pharmacological agents, infections and immune system dysregulation. In light of these considerations, we conducted a review of the literature to observe the associations and potential mechanisms linking thyroid disease to SLE. This review aims to shed light on the complexities of these interrelated conditions and provide insights into their co-occurrence.
Keywords
Introduction
Globally, the three most prevalent disease types are cancer, heart disease and autoimmune diseases, with autoimmune disorders affecting approximately 8% of the population. 1 Autoimmune diseases encompass a category of conditions in which the immune system mistakenly targets healthy cells in the body, triggered by immune responses to specific antigens. Systemic lupus erythematosus (SLE) is a chronic autoimmune disease which presents with diverse clinical symptoms, affecting the skin, mucosa, kidneys (known as lupus nephritis, LN), musculoskeletal system, hematopoietic system, nervous system and other parts of the body. 2 While the involvement of the kidneys, nerves or lungs commonly garners attention from clinicians and patients due to their severity, thyroid involvement is often ignored due to its non-specific clinical manifestations (Figure 1).
Numerous studies have indicated a higher prevalence of thyroid disease, particularly autoimmune thyroid disease (AITD) characterized by hypothyroidism, is significantly higher in patients with SLE than in the general population.3–6 This phenomenon is associated with autoimmune manifestations and may also be associated with autoimmune lupus erythematosus, however, the exact association between thyroid autoimmunity and SLE remains to be elucidated. Furthermore, SLE patients accompanying with thyroid dysfunction have an increased risk of subsequent events. 7 Analyzing the associations between SLE and thyroid disease could significantly impact the long-term management of SLE.
This review focuses on exploring the associations and shared mechanisms between thyroid disorders and SLE. We aim to raise awareness among clinicians and patients regarding the importance of monitoring the thyroid function after an SLE/LN diagnosis. Additionally, we encourage basic researchers to conduct more in-depth studies on the molecular mechanisms of thyroid disease in SLE.
Associations between SLE and thyroid disease
Thyroid disease encompasses a range of common endocrine disorders, characterized by diverse manifestation, including changes in thyroid hormone secretion (hypo- or hyper-function), alterations in thyroid size or tissue structure (benign nodules, malignant tumors and diffuse goiter), and other forms of disease. The non-specific nature of certain manifestations of thyroid disease, for example, fatigue, weight change, dry hair, etc. can easily be mistaken for SLE symptoms.
Review of the cohort studies of SLE with thyroid disease.
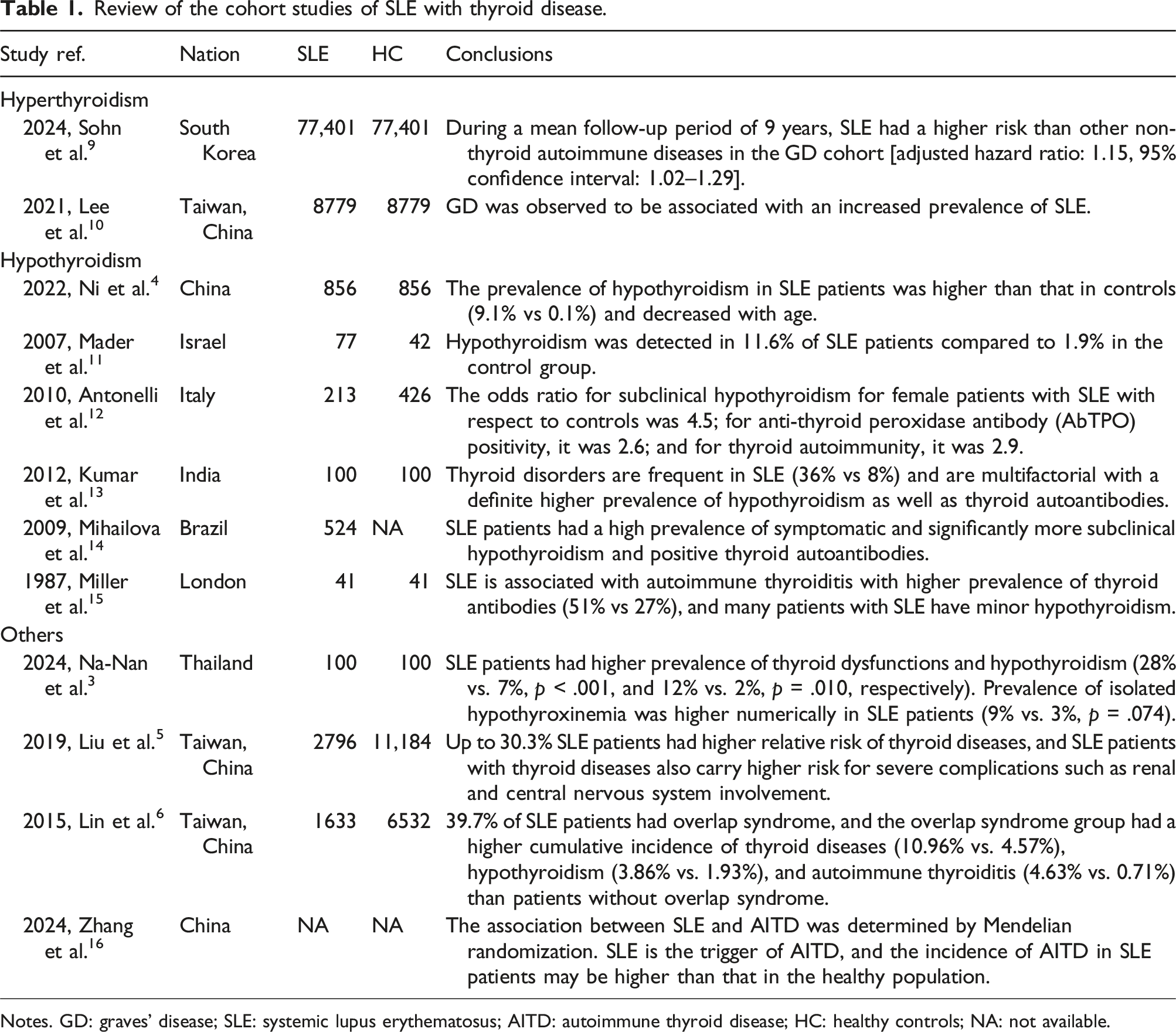
Notes. GD: graves’ disease; SLE: systemic lupus erythematosus; AITD: autoimmune thyroid disease; HC: healthy controls; NA: not available.
These associations suggest a possible common pathogenic mechanism between thyroid disease and SLE and emphasize the need for regular evaluation of thyroid function in patients with SLE.
SLE and hypothyroidism
Hypothyroidism, caused by insufficient synthesis, secretion or biological effects of thyroid hormones, has a significantly higher incidence in patients with SLE compared to the healthy population. SLE Disease Activity Index (SLEDAI), one of the most commonly used indicators to assess the global disease activity and severity of SLE, covered multiple systems and clinical manifestations. 2 Patients with hypothyroidism exhibit greater SLEDAI scores and more severe kidney damage. Studies have shown that SLE patients with subclinical hypothyroidism, if left untreated, exhibit elevated immune activity, increased SLEDAI scores, and a higher incidence of organ damage. In contrast, the administration of thyroid hormone therapy improves immune activity, disease activity and organ damage, suggesting a potential influence of thyroid hormone metabolism on SLE. 27 Notably, serum levels of free triiodothyronine was negatively correlated with the acute activity index score of lupus nephritis (r = −0.228, p < .05). 28 Different age groups and genders within the SLE population demonstrate varying rates of combines hypothyroidism, with a particularly high prevalence observed in younger patients and a greater incidence among women. SLE patients younger than 20 years have the highest rates of combined hypothyroidism (odds ratio/OR 8.38, 95% confidence interval/CI: 2.71–26.01, p < .05). Compared to male patients, women with SLE are more likely to experience clinical or subclinical hypothyroidism. Among men with SLE, the incidence of hypothyroidism is also higher compared to healthy male controls (OR: 5.26, 95% CI: 3.61–7.68, p < .05). 29 Domingues et al. found that SLE patients who are positive for anti-Smith antibodies are more likely to have hypothyroidism, indicating a possible immune connection between these two diseases. 30 A retrospective study including 77 SLE patients and 52 healthy controls showed a high prevalence of hypothyroidism (8.7%) among SLE patients, however, there was no significant difference in the levels of anti-thyroglobulin or thyroid peroxidase antibodies between these two groups. 11
SLE and autoimmune thyroid disease (AITD)
Autoimmune thyroid disease (AITD) represents a group of T cell-mediated, organ-specific autoimmune disorders characterized by the immune system’s loss of tolerance to thyroid antigens. 31 The prevalence of AITD is estimated to be approximately 5%. 32 AITD, includes Graves’ disease, Hashimoto’s thyroiditis (HT) and other variants, and has been reported at varying incidences in SLE patients. 31 Most existing studies indicate that the prevalence of thyroid diseases in SLE is significantly increases for hypothyroidism, while the prevalence of hyperthyroidism remains relatively unchanged, and some studies even suggest a lack of association between SLE and hyperthyroidism.33,34 The mechanisms triggering the autoimmune attack on the thyroid are still under investigation. The reported incidence of ATID ranging from 3.9% to 24% and anti-thyroid antibodies from 11% to 51% in SLE. 35
In a study conducted in Brazil, Posselt et al. reported a prevalence of HT in SLE patients of 12.6%, compared to 5.6% in the general population. They also found that SLE patients with HT exhibited fewer facial rashes and higher levels of anti-Sm antibodies. Furthermore, the risk of developing HT was found to be two-fold higher in patients with SLE compared to the overall cohort. 36 In a Chinese study, Liu et al. identified an inverse correlation between FT3 levels and disease activity in patients with SLE and HT. 37 Domingues et al. found that SLE patients with HT and hypothyroidism, as opposed to those with hyperthyroidism, demonstrated higher disease activity and more severe organ damage. The levels of 24-h urinary protein and serum creatinine in LN patients were elevated compared to those with normal thyroid function. 30 Franco et al. noted that the prevalence of confirmed autoimmune hypothyroidism in SLE patients was 12%. Additionally, smoking and Sjögren’s Syndrome have been identified as predictors of the development of autoimmune hypothyroidism in SLE patients. 38
However, the pathological mechanisms underlying the relationship between SLE with thyroid disease remain complex, and the precise nature of these mechanisms is still not fully understood. Previous studies have suggested that the shared genetic background and altered immune environment may predispose SLE patients to hypothyroidism, although some scholars contest this finding. In light of these considerations, we reviewed the previous studies concerning the common pathogenesis of SLE and thyroid disorders.
The shared potential mechanisms between SLE and thyroid disease
Inflammatory response
In SLE, the immune response in patients is activated, and chemokines released by immune cells disseminate throughout the body via blood circulation. The thyroid gland, as a highly vascularized target organ, exposes autoantigens in response to injury, thereby exacerbating the immune response and contributing to the occurrence of hypothyroidism. Clinical manifestations of SLE.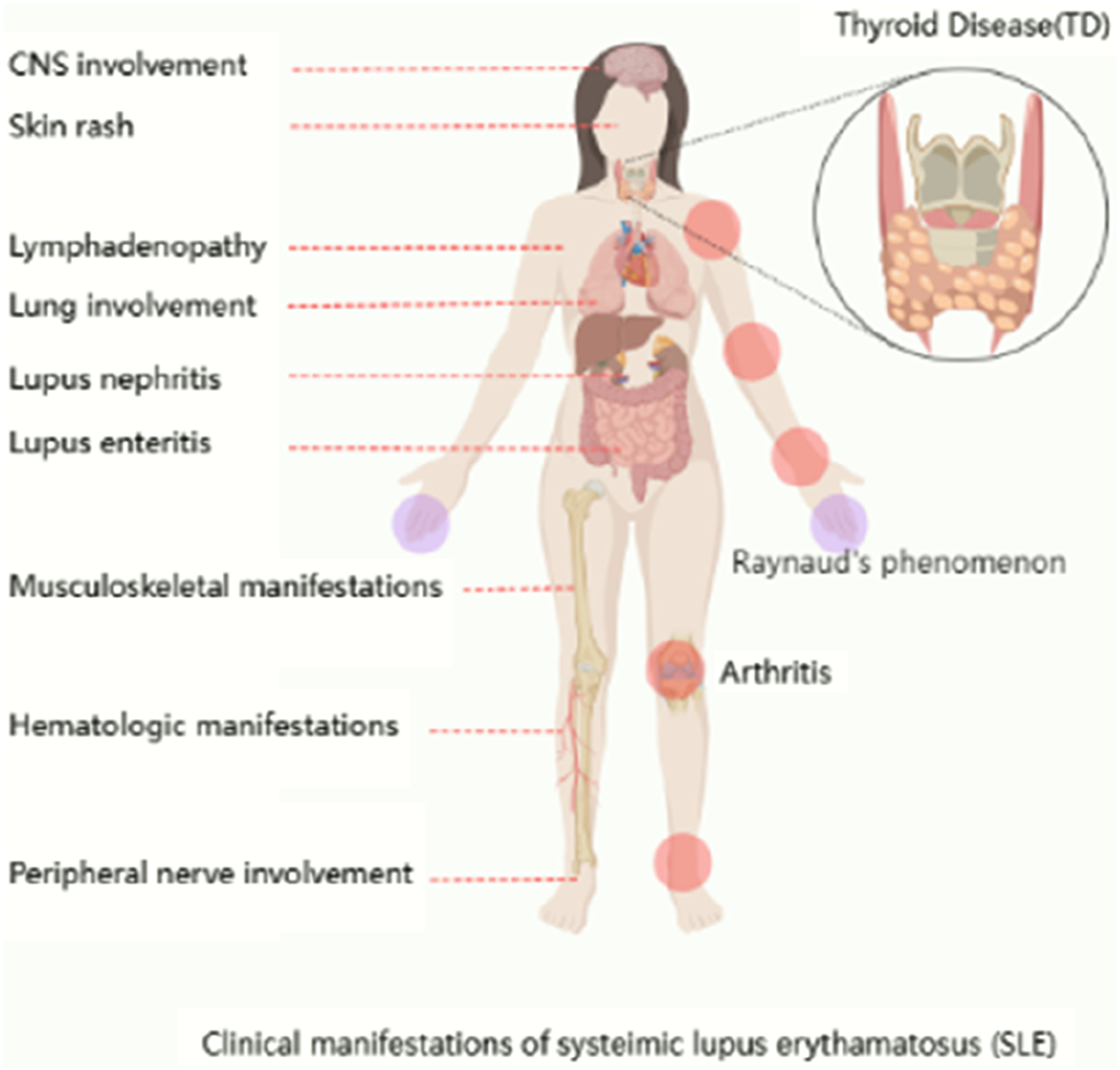
Thyroid hormones, particularly thyroid stimulating hormone (TSH), serve as critical indicators for diagnosing thyroid diseases. Both SLE and AITD are immune system disorders that share certain histocompatibility antigens, which may contribute to their co-occurrence.
39
SLE induces immune dysfunction, resulting in impaired T cells activity and hyperactivity of B cells. This hyperactivity produces a substantial number of autoantibodies that directly damage the thyroid gland (as Shown in Figure 2). Consequently, the gland’s ability to synthesize thyroid hormones is diminished, ultimately leading to conditions such as hypothyroidism or AITD.38,40 Furthermore, nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) is a critical pathway for immune cell expression, blocking this pathway can downregulate pro-inflammatory cytokine, such as tumor necrosis factor-α. Studies have confirmed that TSH can activate the NF-κB pathway in macrophages, exacerbating immune and inflammatory responses.
41
TSH also enhances the inflammatory response in macrophages, promotes T cell proliferation, inhibits thyroxine-induced T cell apoptosis, and stimulates B cell antibody production. In patients with subclinical hypothyroidism, levothyroxine supplementation to correct abnormal TSH levels can improve immune-related indicators.42,43 Common mechanisms of SLE and AITD.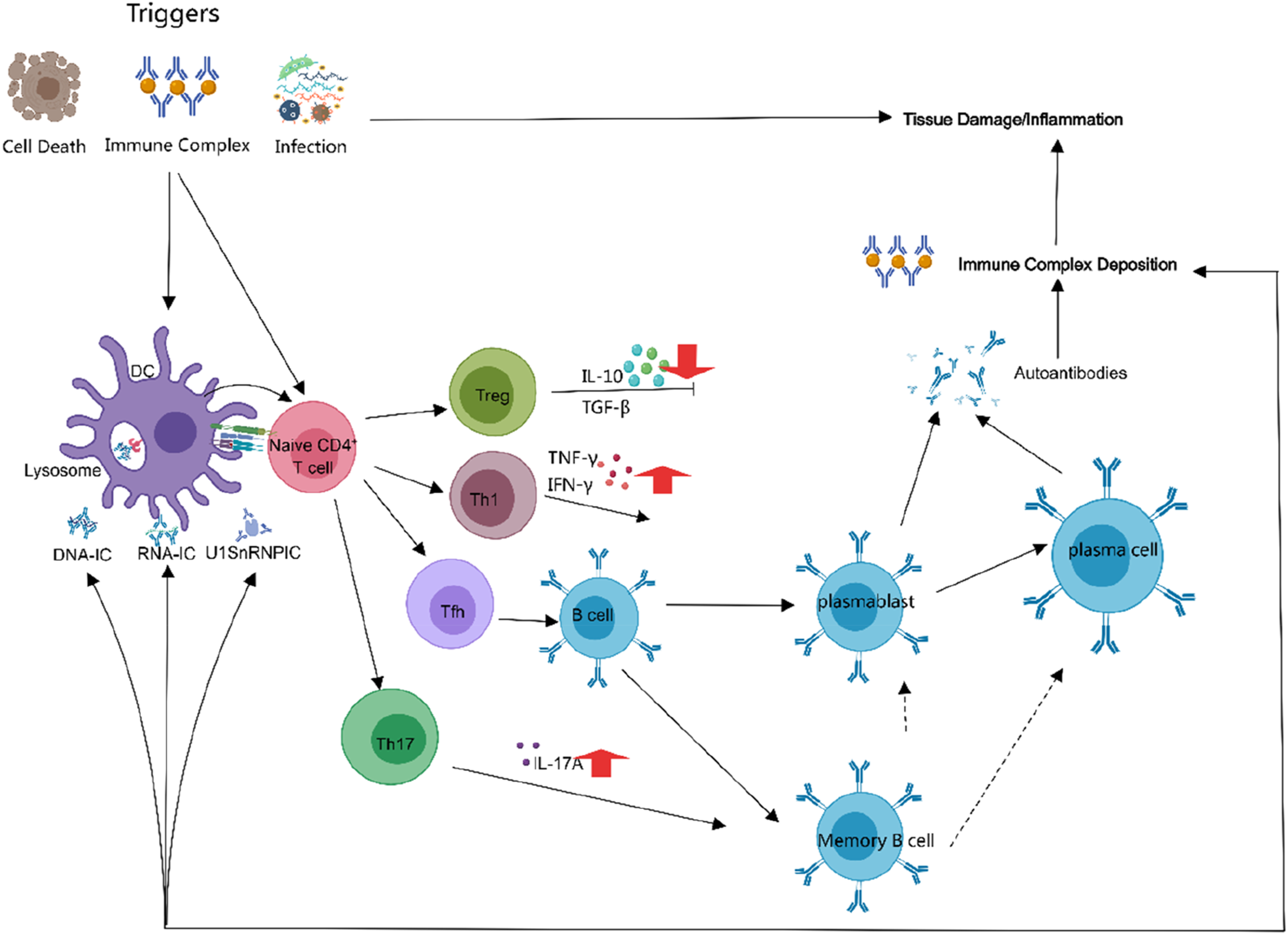
The interleukin (IL) family is closely related to SLE and AITD. The type-II interferon, namely interferon-gamma (IFN-γ), is associated with the onset and progression of SLE as a classic lupus-causing factor. IFN-γ is produced in response to interleukin-12 (IL-12), which mediates the differentiation of helper T cell 1 (Th1). 44 One of its primary effects is the differentiation of B lymphocytes into autoantibody-producing cells and the activation of macrophages.45,46 IL-17A, a pro-inflammatory cytokine produced by activated T lymphocytes, mediates pro-inflammatory effects by activating the chemotaxis of monocytes and neutrophils, increasing the production of other pro-inflammatory cytokines and adhesion molecules, as well as generating autoreactive antibodies.47,48 Ren et al. found that IL-17 in the untreated GD group were significantly higher than those in the control group, and decreased after remission. 49 IL-23 influences T cell phenotype by inducing extrafollar helper T cell differentiation, limiting regulatory T (Treg) cell differentiation, promoting Th17 differentiation, and driving the production of B cell autoantibodies. Previous clinical studies have found that IL-23 is positively correlated with SLEDAI scores in SLE patients and positively correlated with TSH levels in AITD patients.50,51
Although some studies suggest a theoretical immunological link between SLE and thyroid disease, it’s not yet clear how the inflammatory immune state that causes SLE affects thyroid disease. Further research into this mechanism is needed.
Genetic abnormality
The application of genetic technologies, such as genome wide association study (GWAS), has facilitated the identification of common susceptibility genes associated with comorbid diseases. Several studies have identified shared genetic abnormalities between SLE and thyroid disease. Research has revealed that a genetic overlap between SLE and AITD, notably R620 W polymorphism of the PTPN22 gene. 52 A family study also found that 5q14.3-15 locus is a susceptible gene region for both SLE and AITD. 53 Additionally, human leukocyte antigen (HLA) DR2, 54 DR3, 55 DR8, 56 along with non-HLA genes, for example, IRF8 57 and CTLA-4, 58 have been reported to be associated with SLE complicated with AITD. Furthermore, the Akt/mTOR signaling pathway appears to play a significant role in both diseases. Exposure to diisononyl phthalate, particularly at high doses, may exacerbate oxidative stress and activate the Akt/mTOR pathway, subsequently inhibiting normal autophagy and increasing the expression of IL-17 in the thyroid, thereby contributing to the aggravation of AITD. 59 In SLE, the expression of Akt/mTOR pathway-related proteins (P85, Akt, p-Akt, m-TOR, p-mTOR, etc.) is up-regulated in both mouse and human mesangial cells, which is implicated in the pathogenesis of LN.60,61
These associations underscore the critical role of genetic factors in these autoimmune conditions, suggesting that common pathways may be activated due to similar genetic susceptibilities. However, these observational studies are susceptible to confounding variables and reverse causation.
Lifestyle and environmental factors
The “multiple hit” hypothesis describes the interactions between SLE and TD. In this context, there is an intersection of genetic predisposition, immune disorders, environmental factors, and metabolic abnormalities.24,62,63
Gaseous pollutants, including sulfur oxides, nitrogen oxides, carbon monoxide and ozone, are risk factors for both thyroid disease and SLE.64,65 Additionally, smoking serves as a common risk factor for SLE and AITD,65,66 exhibiting a dose-dependent effect in AITD due to competition for iodine uptake by thiocyanates present in cigarette smoke. 67 Perricone et al. found that in a cohort of lupus nephritis patients, smokers had a significantly shorter median time to end-stage renal disease compared to non-smokers. 68 Pesticide may also pose a shared risk factor for SLE and AITD69,70; however, the pathogenicity of pesticides remains unconfirmed due to limitations such as patients’ self-reported recall of specific pesticide exposure and confounding factors, including exposure duration, ultraviolet rays, and other chemicals. Furthermore, factors such as iodine intake, alcohol consumption, low selenium levels, low vitamin D levels, and infections, are implicated in the pathogenesis of TD. 26 Occupational exposure, exogenous estrogen, ultraviolet radiation, and infections, are also associated with the pathogenesis of SLE. 70 The potential interactions of these factors with comorbid diseases remain unknown and require further exploration.
Collectively, these insights highlight the complex interplay of various environmental factors contributing to both SLE and AITD, paving the way for further research aimed at unraveling the intricate mechanisms underlying these autoimmune diseases and exploring potential therapeutic interventions.71,72
Summary
Both SLE and AITD are significant autoimmune disorders that impact global health. Numerous studies have demonstrated that individuals with SLE are more susceptible to thyroid diseases, particularly hypothyroidism associated with AITD, compared to the general population. Inflammatory responses and immune dysregulation play crucial roles in the pathogenesis of both conditions. Additionally, environmental factors and genetic predisposition may also be influential. Understanding and actively monitoring thyroid function in patients with SLE can facilitate early detection and management of potential dysfunction, thereby reducing associated risks.
Footnotes
Author contributions
Lin-Lin Li: Review studies, original draft preparation and manuscript revision; Qiu-Rui Li and Lu Li: Review studies; Hui-Xia Cao & Feng-Min Shao: Manuscript revision. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by Youth Science Fund Project of Henan Natural Science Foundation (Number: 242,300,420,407), and the Award Recipient is Dr. Lin-Lin Li.