
Abstract
Introduction
Maintenance of immunosuppressants (IST) is critical for sustaining remission in lupus nephritis (LN) patients. However, long-term use is associated with an increased risk of side effects such as infection. Yet, early IST withdrawal also poses a high risk of flare. This study aims to provide an overview of the impact of optimal IST withdrawal in patients with LN who have achieved remission.
Method
We conducted a systematic review of randomized controlled trials (RCTs) and observational studies regarding the discontinuation of IST in patients with proliferative LN who had been in remission for at least 1 year. Data from PubMed, ProQuest, and Web of Science were extracted on patient demographics, baseline characteristics, treatment regimens, and outcomes, including flare rates, renal function, and biopsy findings. The risk of bias was assessed using the Newcastle-Ottawa Scale and the JADAD Score.
Results
Five studies with 310 patients were included. The mean age of participants ranged from 26 to 38 years. Overall, flares following IST withdrawal occurred in an average of 28.7% of patients. Between the two groups (flare and no-flare), baseline serum creatinine was comparable, but baseline proteinuria and C3 & C4 levels were varied across studies. The duration of lupus before study entry was approximately 4-10 years, with a duration of complete remission of 12-59.5 months before IST withdrawal. Follow-up periods ranged from 24 to 215 months. The Biopsy Activity Index and Chronicity Index at baseline also showed variation but generally indicated a higher level of chronic damage in the flare group.
Discussion
Discontinuation of IST is feasible but may be associated with an increased risk of severe flares, often requiring reintroduction of induction therapy. Careful assessment and monitoring of both histologic and clinical activity are essential when evaluating remission and considering IST withdrawal, as a low activity index may guide safer withdrawal strategies.
Conclusion
IST withdrawal is feasible in patients with LN who have achieved remission, but careful monitoring is required due to the risk of relapse and potential progression of chronic kidney damage. Histological confirmation and predictive tools may support safer withdrawal decisions.
Introduction
Lupus nephritis (LN) represents one of the most morbid complications of systemic lupus erythematosus (SLE), occurring in 33%–55% of cases. Clinical manifestations of LN include asymptomatic proteinuria, nephritic syndrome, nephrotic syndrome, and rapidly progressive glomerulonephritis. In both America and Europe, the implementation of modern immunosuppressive therapies has improved the 10-year renal survival rate to 80%–90%.1,2 While advancements in treatment have improved the prognosis of LN, patients continue to experience considerable challenges, such as the risk of infections and malignancies. The therapeutic approach to LN is primarily determined by the pathological classification of renal histopathological lesions. In patients with proliferative LN, treatment is typically divided into two phases: an induction phase and a maintenance phase. The induction phase aims to control renal inflammation to achieve renal remission. Subsequently, the maintenance phase intends to sustain remission and prevent renal flares. 3 The gold-standard maintenance therapy usually includes either mycophenolate mofetil (MMF) or azathioprine (AZA), often accompanied by the gradual discontinuation of low-dose corticosteroids. The inclusion or continuation of antimalarial drugs, such as hydroxychloroquine, is also recommended. 4
Although these treatments are important, the optimal duration of immunosuppressive therapy (IST) in patients with proliferative LN remains unclear, and the potential for discontinuing IST in patients who have achieved remission is still under debate. Evidence suggests that reducing or discontinuing IST before 18 months may be associated with a high risk of flare and subsequent organ damage. 5 However, the prolonged continuation of IST poses the risk of adverse effects such as cardiovascular events, infections, and malignancies. 6 This systematic review aims to evaluate existing evidence on the outcomes of IST withdrawal in patients with proliferative LN, to inform clinical decision-making and guide future research on the best practices for managing therapy withdrawal in this population.
Methods
This systematic review was conducted according to the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 7 and was registered in the PROSPERO database under the registration number CRD42024547770.
Eligibility criteria
All study types were considered for inclusion, except for case reports or series. For this study, the inclusion criteria were as follows: patients aged 18 years or older with biopsy-proven proliferative lupus nephritis (type III/IV) who had been in complete response for at least 12 months; initial induction treatment with high-dose corticosteroids and either intravenous cyclophosphamide or MMF, followed by current maintenance immunosuppressive therapy (IST) with azathioprine (≥50 mg/day) or MMF (≥1000 mg/day) or mycophenolate sodium (≥720 mg/day) or Calcineurin inhibitor 8 ; and documentation of complete response and lupus nephritis flare, that can be defined with any reappearance of renal inflammation, which can manifest as either clinical symptoms or laboratory findings, including an increase in proteinuria, hematuria, or decline in kidney function. 1 Exclusion criteria included individuals in the preconception stage, pregnant patients, those with end-stage renal disease or on routine hemodialysis, and patients with a history of kidney transplant.
Search strategy and study selection
A comprehensive literature search was conducted until August 19, 2024, using databases such as PubMed, Web of Science, and Proquest. The search terms used were: (“lupus nephritis”) OR ((lupus erythematosus, systemic ) AND ((“kidney”) OR (“renal”))) OR (“lupus nephritic”) AND ((“glucocorticoid*”) OR (“corticoster*”) OR (“prednisone”) OR (“methylprednisolone*”) OR (“prednisolone”) OR (“steroid*” [All Fields)) AND ((“immunosuppression* therapy”) OR (agent*, immunosuppressive) OR (“azathioprine”) OR (“immunosuppressive agents”) OR (“mycophenolic acid”) OR (“mycophenolat*”) OR (“cyclosporine*”) OR (“tacrolimus”) OR (“voclosporin*”)) AND ((“taper*”) OR (“withdrawal*”) OR (“discontinuation”) OR (“stop*”) OR (“duration*”) OR (“wean*”)). After removing duplicates, titles and abstracts were screened for relevance, followed by full-text retrieval and further screening based on the inclusion criteria. Two reviewers independently conducted the screening process. Additional studies were identified through citation searching. Additional studies were identified through citation searching.
Data extraction
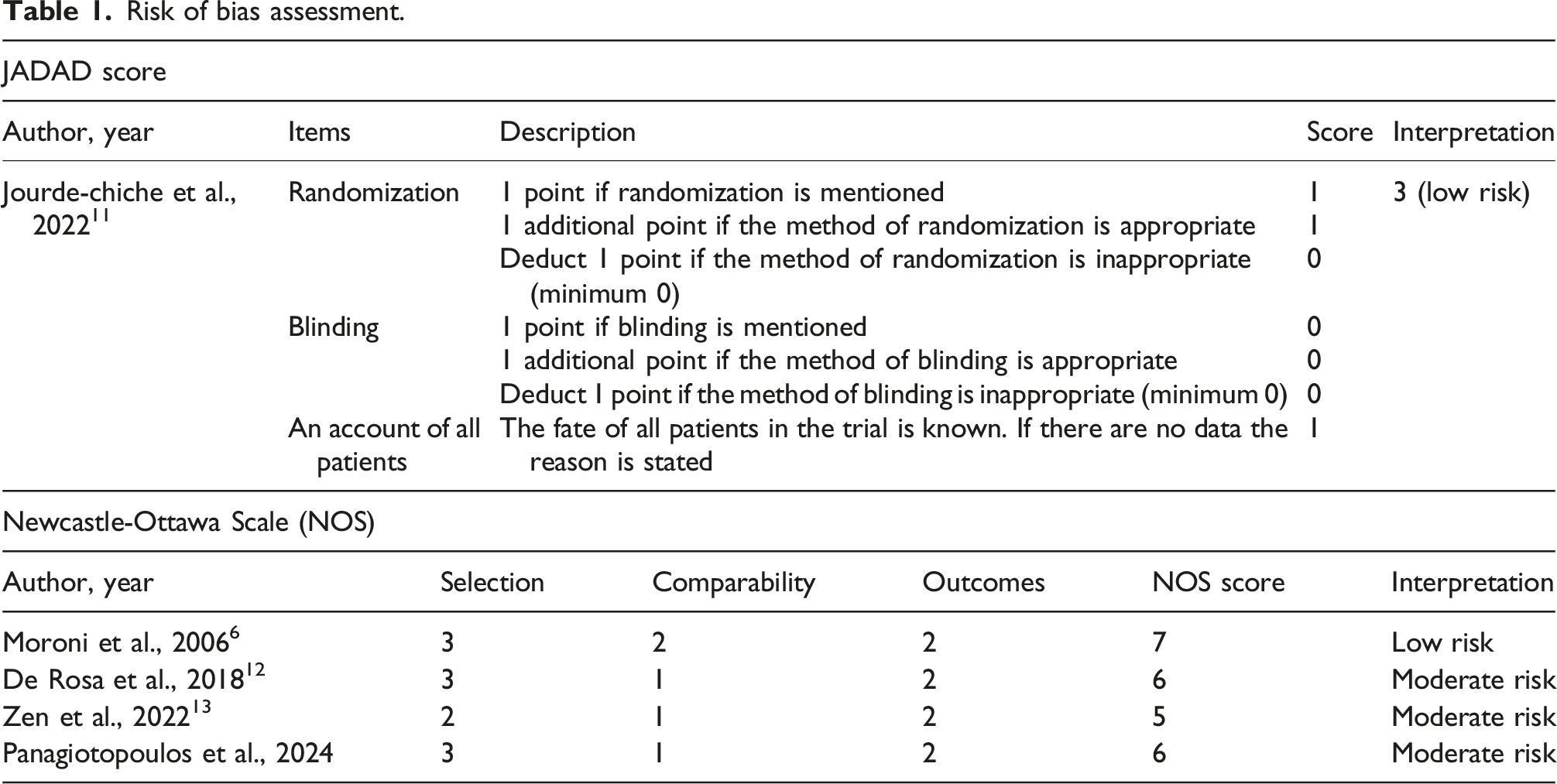
Risk of bias assessment.
Quality assessment
The quality of the included studies was independently assessed by two authors. Random clinical trials were evaluated using the JADAD Score, 9 while observational studies were evaluated using the Newcastle-Ottawa Assessment Scale. 10 The critical appraisal results indicated that none of the included studies had a high risk of bias, as detailed in Table 1. Any disagreements were resolved by a third reviewer.
Statistical analysis
Due to the heterogeneity of the included studies, a meta-analysis can not be performed. Instead, the extracted data were organized into a table and analyzed using descriptive statistics.
Results
Following an extensive literature search, this review incorporated five relevant studies, including one RCT
11
and four observational studies,6,12–14 involving a total of 310 patients. The study selection process is illustrated in Figure 1. PRISMA flowchart.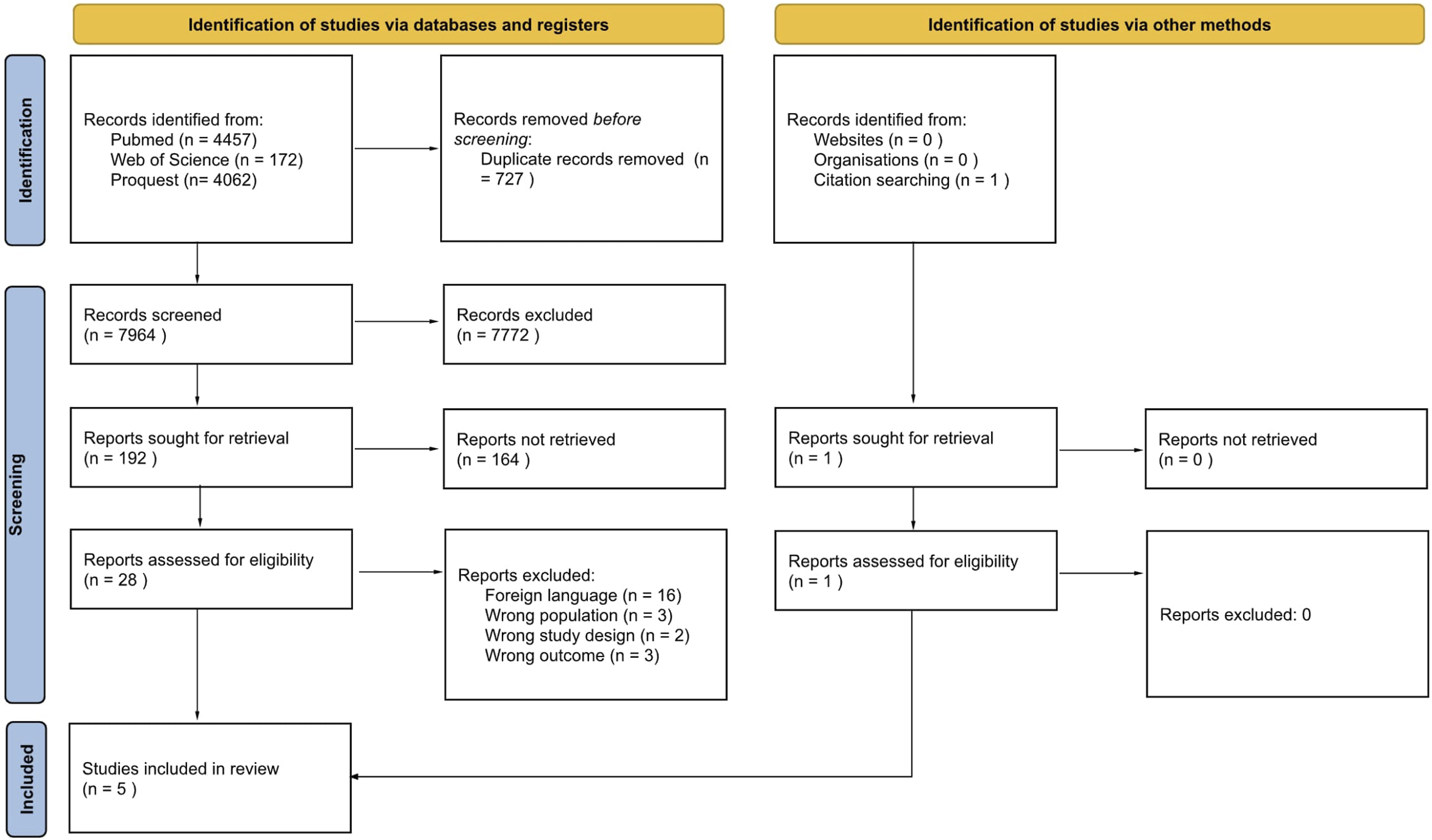
Baseline characteristics
Baseline characteristics of included studies.
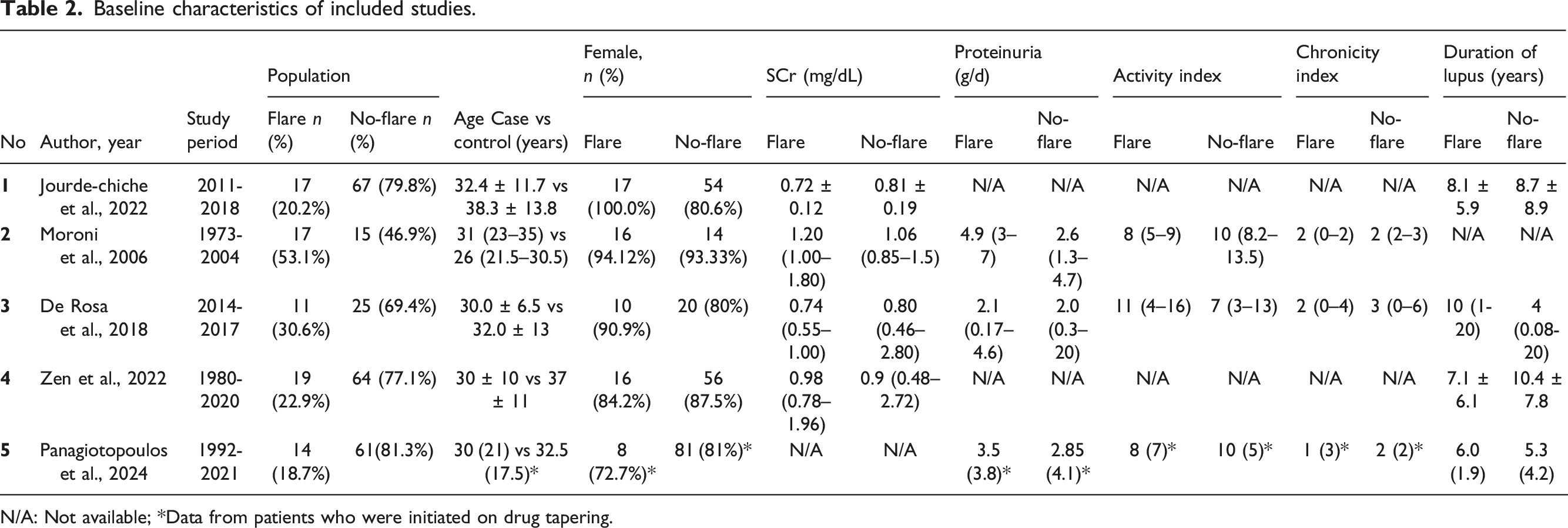
N/A: Not available; *Data from patients who were initiated on drug tapering.
Baseline clinical characteristics
Serum creatinine levels, which indicate kidney function, varied across the studies. In the study by Jourde-Chiche et al. (2022), 11 the flare group had a mean SCr of 0.71 ± 0.15 mg/dL, slightly lower than the no-flare group (0.81 ± 0.19 mg/dL). Moroni et al. (2006) 6 reported median SCr values of 1.20 mg/dL (range 1.00–1.80) for the flare group and 1.06 mg/dL (range 0.85–1.5) for the no-flare group. De Rosa et al. (2018) 12 and Zen et al. (2022) 13 also showed similar SCr values. Panagiotopoulos et al. (2024) 14 found no difference in eGFR between flare and no-flare groups at baseline, 12 months post-diagnosis, at the start of tapering, and at IST discontinuation, indicating that SCr was assessed as it is used to calculate eGFR. Furthermore, proteinuria, as the key marker of kidney damage in LN, was reported to be higher in the flare group by three studies. In the study by Moroni et al. (2006), 6 the flare group exhibited higher proteinuria levels with a median of 4.9 g/day (range 3–7), compared to 2.6 g/day (range 1.3–4.7) in the no-flare group. De Rosa et al. (2018) 12 reported similar proteinuria levels between the flare (2.1 g/day) and no-flare (2.0 g/day) groups, although with a broader range in the no-flare group. Panagiotopoulos et al., 2024 14 also reported higher proteinuria at baseline in the flare group (3.5 g/day) versus the no-flare group (2.85 g/day), significantly higher proteinuria at 12 months post diagnosis in the flare group (0.85 g/day) versus the no-flare group (0.2 g/day), and at tapering initiation in the flare group (0.19 g/day) versus the no-flare group (0.16 g/day). However, Panagiotopoulos et al. found no significant difference in proteinuria between those who flared (0.36 g/day) and those who did not (0.16 g/day; p value = .10) after IST discontinuation.
Anti-dsDNA antibodies that were associated with disease activity in SLE were reported in three studies. Jourde-Chiche et al. (2022) 11 found that 76.5% of patients in the flare group tested positive for these antibodies, compared to 53.8% in the no-flare group. De Rosa et al. (2018) 12 reported positive anti-dsDNA antibodies in 81.8% of the flare group and 80.0% of the no-flare group. Zen et al. (2022) 13 presented median anti-dsDNA levels, which were slightly higher in the flare group (10 IU/mL) than in the no-flare group (8 IU/mL). Panagiotopoulos et al. (2024) 14 found no significant difference in anti-dsDNA positivity between the flare (83.3%) and no-flare group (85.9%) at baseline.
Complement levels, specifically C3 and C4, were measured in some studies. Jourde-Chiche et al. (2022)
11
noted low C3 levels at inclusion in 37.5% of the flare group, compared to only 6.3% in the no-flare group, with similar low C4 levels observed in both groups. De Rosa et al. (2018)
12
measured C3 and C4 levels twice, at 6 months before biopsy and at the second biopsy. It reported median initial C3 levels (89 mg/dL) and subsequent C3 levels (100 mg/dL) in the flare group versus initial
The SLEDAI, which measures disease activity, was reported in three studies. Jourde-Chiche et al. (2022) 11 showed a higher SLEDAI score in the flare group (3.1 ± 2.6) compared to the no-flare group (1.6 ± 1.4). De Rosa et al. (2018) 12 also reported a higher median SLEDAI score in the flare group (11) compared to the no-flare group (7). Panagiotopoulos et al. (2024) 14 reported a similar median SLEDAI-2K at baseline between the flare and the no-flare groups (both at 2). At tapering initiation, the flare group had a higher median SLEDAI-2K (2 vs 0) compared to the no-flare group; this may relate to flare during tapering initiation only. At IST discontinuation, while the flare group had a higher SLEDAI-2K (1 vs 0), this difference was not statistically significant. Instead, the significant predictor for post-IST discontinuation flares was SLEDAI-2K 12 months before IST DC (2 vs 0, p = .026; OR = 1.7, p = .013). In addition, other included studies also reported Activity Index and Chronicity Index, which measure the severity and duration of kidney damage, were reported by Moroni et al. (2006), 6 De Rosa et al. (2018), 12 and Panagiotopoulos et al. (2024). 14 Moroni et al. (2006) 6 found that the Activity Index was slightly higher in the flare group compared to the no-flare group. De Rosa et al. (2018) 12 reported similar trends, with slightly higher scores in the flare group for both Activity Index and Chronicity Index. At baseline, Panagiotopoulos et al. (2024) 14 reported a higher, but insignificant, activity index and chronicity index in the no-flare group compared to the flare group. Panagiotopoulos et al. (2024) 14 did not report repeated kidney biopsy, though. Last but not least, the duration of lupus, when reported, was fairly similar between flare and no-flare groups, with averages and medians typically within a few years of each other. Jourde-Chiche et al. (2022) 11 reported a mean duration of lupus of 8.1 ± 5.9 years in the flare group and 8.7 ± 8.9 years in the no-flare group. Zen et al. (2022) 13 found a shorter mean duration in the flare group (7.1 ± 6.1 years) compared to the no-flare group (10.4 ± 7.8 years). Other than the SLEDAI Score, Panagiotopoulos et al. (2024) 14 also evaluate DORIS and LLDAS status at 12 months before IST discontinuation and at IST discontinuation. Most patients who achieved clinical and complete remission remain stable after IST tapering and discontinuation. The number of patients with DORIS complete remission at 12 months before IST discontinuation who had flared was 15.3% (4 out of 26 patients), and at IST discontinuation was 15.5% (7 out of 45 patients). Similar findings were also found related to LLDAS who had flared (26% at 12 months before IST discontinuation vs 27% at IST discontinuation).
IST withdrawal and its outcomes
IST withdrawal and its outcomes.
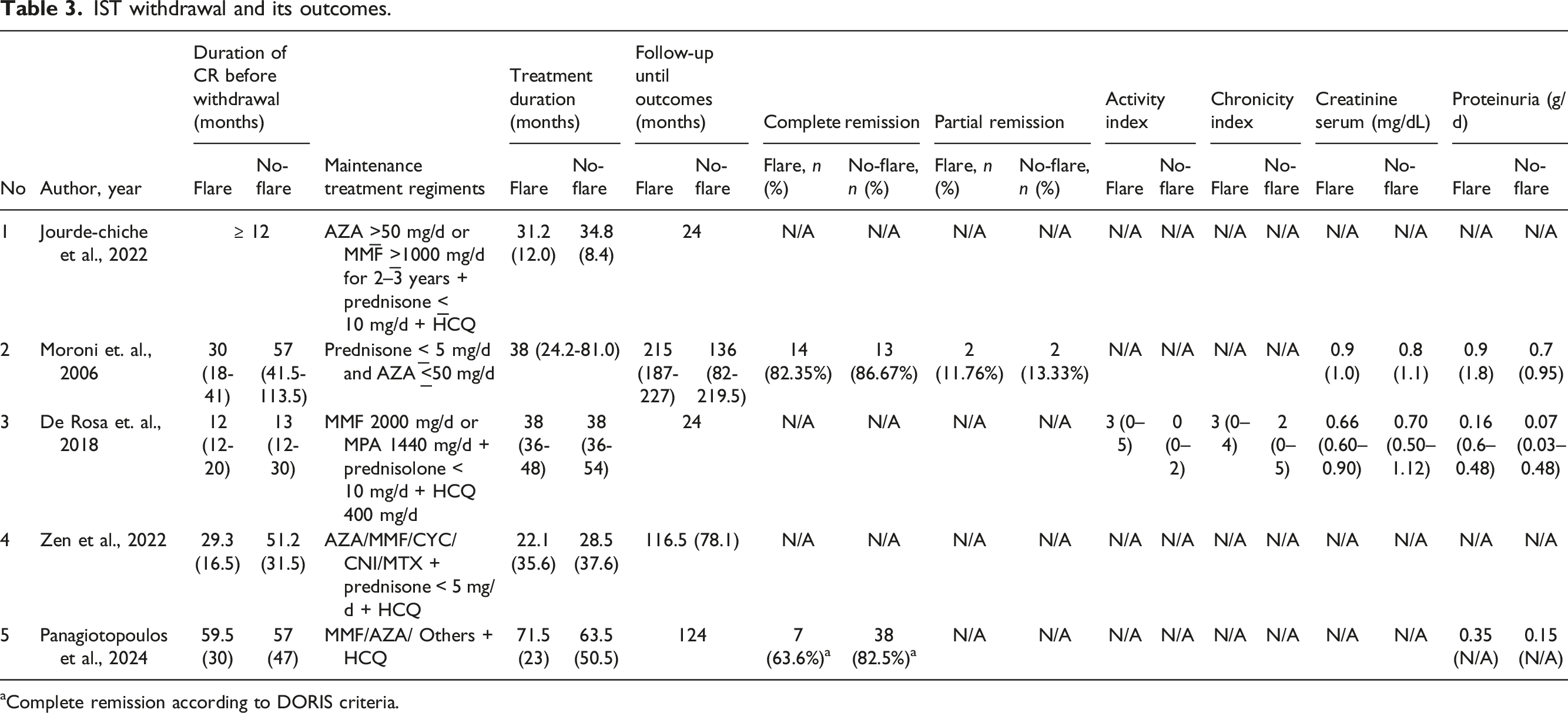
Complete remission according to DORIS criteria.
Across the included studies, flare rates and remission outcomes were variable. Moroni et al. (2006) 6 reported that complete remission occurred in 82.35% of flare patients and 86.67% of no-flare patients. Partial remission was less common. Panagiotopoulos et al. (2024) 14 also reported similar findings, in which complete remission was found in 71% of the flare group and 75% of the no-flare group at 12 months post-diagnosis. In addition, the DORIS complete remission occurred in 63.6% of the flare patients and 82.5% of the no-flare patients at IST discontinuation. From all the available studies, only the study by De Rosa et al. (2018) 12 implemented a repeated kidney biopsy before discontinuing immunosuppressants, where the discontinuation of immunosuppressants was carried out regardless of the repeat biopsy results. This study reported that the activity index was elevated in patients who eventually experienced flares, compared to those who did not. The chronicity index was also higher in the flare group, suggesting more significant long-term damage in these patients.
Monitoring serum creatinine is also critical to assess kidney function. In the included studies, creatinine levels were generally preserved between the flare and no-flare groups. For example, in Moroni et al. (2006), 6 the mean creatinine level was 0.9 mg/dL in flare patients and 0.8 mg/dL in non-flare patients, suggesting that renal function remained relatively preserved in both groups. However, in the study from Rosa et al. (2018), 12 slight variations were noted, with flare patients showing a lower median creatinine level (0.66 mg/dL) compared to the no-flare group (0.70 mg/dL). In addition, Moroni et al. (2006), 6 documented that proteinuria levels at the end of observation period were slightly higher in the flare group (0.9 g/day) compared to the no-flare group (0.7 g/day), indicating greater protein loss during periods of active disease, which aligns with increased renal inflammation. However, De Rosa et al. (2018) 12 noted a less pronounced difference in proteinuria between flare and no-flare patients (0.16 g/dL vs 0.07 g/dL). Similarly, Panagiotopoulos et al. (2024) 14 also reported that patients with renal flares after IST discontinuation had higher proteinuria levels at the end of follow-up (EFU) (0.35 g/day vs 0.15 g/day, p = .04) compared to those without renal flares. Despite preserved renal function, careful proteinuria evaluation is essential in patients who had flares during the IST withdrawal protocol.
Discussion
General finding
The findings from the included studies revealed that patients in the flare groups were generally younger and exhibited higher SCr levels, more pronounced proteinuria, and greater disease activity, as indicated by higher SLEDAI scores and increased anti-dsDNA positivity. The proportion of female patients was consistently high in both flare and no-flare groups, aligning with the epidemiology of lupus nephritis, which predominantly affects women. 15 The age discrepancy may suggest a potential association between younger age and flare propensity, though all studies have inconsistent findings. Despite the differences in active disease markers, the duration of lupus and chronicity indices were similar across both groups. This suggests that the long-term, chronic aspects of lupus nephritis were comparable between patients who eventually experienced flares and those who did not. It also suggests that disease chronicity might not be a key determinant of flare status, reinforcing the need to explore other clinical and immunological markers for predicting lupus flares.6,11–13
Risk factors for flare after IST withdrawal
From the included studies, we identified several clinical and laboratory risk factors for flare after IST withdrawal. Both higher SLEDAI-2K score and high activity index pose increased risk of flare as mentioned in Jourde-Chiche et al. (2022), 11 De Rosa et. al. (2018), 12 and Panagiotopoulos et al. (2024). 14 Both Panagiotopoulos et. al. (2024) 14 and Zen et. al. (2022) found that discontinuation of HCQ use aggravates the risk of flares. Moroni et. al (2006) 6 found that flare is associated with shorter duration of treatment and complete remission period before withdrawal. In addition, according to Zen et al. (2022), 13 younger age IST withdrawal may contribute to flare occurrence. Other flare risk factors based on laboratory findings are higher UPCR at baseline, lower serum C3, higher eGFR, and lower serum albumin. 11
Clinical implications of IST withdrawal
The decision to withdraw immunosuppressive therapy (IST) in lupus nephritis (LN) management carries significant clinical implications because of the potential risk of triggering disease flares. Flares can be severe and may necessitate the reintroduction of induction therapy, which can be both physically taxing and psychologically distressing for patients. However, studies have demonstrated that IST withdrawal does not always result in adverse outcomes, suggesting that, with careful patient selection and monitoring, it may be a feasible option.16,17 Key to the successful withdrawal of IST is the careful assessment of chronicity and activity indices in LN patients. For instance, high chronicity indices combined with low activity indices may suggest a scenario where IST withdrawal could be safely considered. This combination implies that the disease has reached a stage where chronic damage is present, but ongoing inflammation is minimal. However, baseline AI and CI do not necessarily reflect the risk of relapse at the time of IST withdrawal. In such cases, the risk of flare because of premature IST discontinuation may be lower, making withdrawal a more feasible option. 18 However, if ongoing inflammation is present, even at low levels, the risk of flare remains significant, underscoring the need for cautious management. Previous studies stated that patients with elevated serum creatinine levels, persistent proteinuria, reduced complement levels, and the presence of anti-Sm antibodies were more prone to experiencing flares after IST discontinuation19,20.
Flare rates following IST withdrawal remain a critical concern. While some patients who achieve complete remission can maintain disease stability after IST discontinuation, others may experience a flare, requiring the reintroduction of aggressive therapy. Understanding the factors that contribute to flare is crucial for guiding IST withdrawal decisions. 21 For example, patients who flare after IST withdrawal and subsequently achieve remission again may face a different prognosis than those who do not experience a flare, underscoring the need for individualized treatment plans. In addition to the risk of flare-ups, prolonged IST use presents its own set of challenges, particularly concerning the risk of life-threatening infections and the overall therapy burden. Balancing the need to prevent disease flares with the risks of long-term IST is a delicate task that requires careful consideration of each patient’s personalized circumstances.22,23
Recommendations for future directions
Incorporating patient-centered approaches is essential in the decision-making process for IST withdrawal. Despite emerging definitions for remission and low disease activity, individualized care based on patient history, comorbidities, and medication tolerance should guide treatment strategies. One of the most pressing challenges is the absence of validated predictive models to accurately stratify flare risk. Although markers such as SLEDAI-2K, complement levels, and proteinuria provide some prognostic insight, their predictive power remains suboptimal. Given the complexities associated with IST withdrawal, future guidelines should emphasize that IST withdrawal can be a viable option for certain patients, provided they are closely monitored. Watchful monitoring during IST tapering and discontinuation is essential to promptly identify signs of flare and to reintroduce therapy as needed before significant and irreversible renal damage occurs. The findings of Panagiotopoulos et al.'s (2024) study suggest that flares during tapering, rather than after discontinuation, are associated with unfavorable long-term renal outcomes. Clinicians should employ a personalized approach, taking into account the patient’s disease history, current health status, and response to previous treatments. A critical area of focus is the balance between the risks of adverse events associated with prolonged IST and the therapy burden on patients. 19 Continuous HCQ treatment is mandatory to mitigate flare risk as described by numerous studies (Moroni et al, 2006; Zen et al, 2022; Panagiotopoulos et al, 2024).
The importance of repeated kidney biopsy evaluations in confirming histological remission before IST withdrawal is also crucial. Notably, there is often a discrepancy between clinical remission and histologic findings. This finding is particularly important as it challenges the sole reliance on clinical remission markers, such as proteinuria, which may not entirely represent ongoing renal damage. Although clinical remission often leads to a reduction in immunosuppression, histological findings from repeat biopsies may show persistent inflammation or worsening chronicity, which are critical for guiding ongoing treatment decisions. Clinical remission alone may not equate to histologic remission, which is a more reliable indicator of immunologic quiescence. Previous studies that combined kidney biopsy with clinical data have demonstrated that this approach can reduce the duration of immunosuppressive therapy while achieving a lower flare rate and improved kidney and patient survival outcomes compared to management based solely on clinical data.5,13,24
By incorporating repeated biopsy evaluations into the management algorithm, a more personalized approach can be developed, potentially slowing CKD progression by addressing both active inflammation and chronic damage. Combining histological evidence with clinical indicators provides a more robust foundation for making informed decisions about therapy withdrawal, reducing the risk of flare, and ensuring that these decisions are based on comprehensive, evidence-based assessments. This strategy may also help in identifying patients at higher risk of flare-ups or progression to chronic kidney disease, thus enabling preemptive adjustments in therapy.4,25 By integrating these recommendations into clinical practice, healthcare providers can better navigate the complexities of IST withdrawal in LN management, ultimately improving patient outcomes through more personalized and evidence-based care.
Study strengths and limitations
This systematic review offers a comprehensive analysis of the impact of IST withdrawal in LN patients who have achieved remission, incorporates a diverse range of study designs, and rigorously assesses study quality. However, it is limited by the small number of existing studies with significant heterogeneity among them and the lack of long-term follow-up data with standardized, evaluated parameters. It may limit the generalizability of the findings. Hence, larger and well-designed studies are needed to confirm these findings and provide more robust insights into the benefits of IST withdrawal in LN patients.
Conclusion
While IST withdrawal is feasible for certain patients, it carries the risk of flare, necessitating close monitoring, especially during drug tapering. The findings indicate that flare is associated with a higher disease activity index, even in patients who appear to be in clinical remission. This underscores the importance of close monitoring and a comprehensive evaluation when considering IST withdrawal. Clinical remission alone may not indicate true immunologic quiescence, highlighting the need to incorporate serological and histological assessments—particularly kidney biopsy findings—into decision-making. Personalized treatment strategies should be guided by an integrated approach. Future research should focus on identifying optimal patient selection criteria and the timing of IST withdrawal, with an emphasis on integrating repeated kidney biopsy evaluations into clinical practice to guide personalized treatment strategies.
Supplemental Material
Supplemental Material - Immunosuppressive therapy withdrawal in lupus nephritis, is it possible? A systematic review
Supplemental Material for Immunosuppressive therapy withdrawal in lupus nephritis, is it possible? A systematic review by Stefanus Gunawan Kandinata, Awalia, Yuliasih, Lita Diah Rahmawati, Cahyo Wibisono Nugroho, Arinditia Triasti Putri, Angela Kimberly Tjahjadi, Mega Kahdina and Mandana Nikpour in Lupus.
Footnotes
Author Contributions
All authors met the authorship criteria. They had a substantial contribution to the conception and design of the work and the acquisition and interpretation of the data used for the work. They were involved in revising a draft of this work, gave final approval of this version to be published, and are accountable for all aspects of the work in ensuring accuracy and integrity.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.