
Abstract

Dear Editor,
Patients with systemic lupus erythematosus (SLE) often suffer from cutaneous LE (CLE), which is divided into acute (ACLE), subacute (SCLE), or chronic (CCLE). 1 Antimalarials are the cornerstone of treatment, with corticosteroids and disease modifying anti-rheumatic drugs reserved for severe cases. 1 While intravenous immunoglobulin (IVIg) has been used to treat nearly all manifestations of SLE, there is limited evidence for the use of IVIg in treating severe, skin-predominant SLE in hospitalized patients.2,3 Here, we describe a series of inpatients with SLE and severe cutaneous involvement refractory to standard immunosuppressants whose conditions rapidly improved with IVIg.
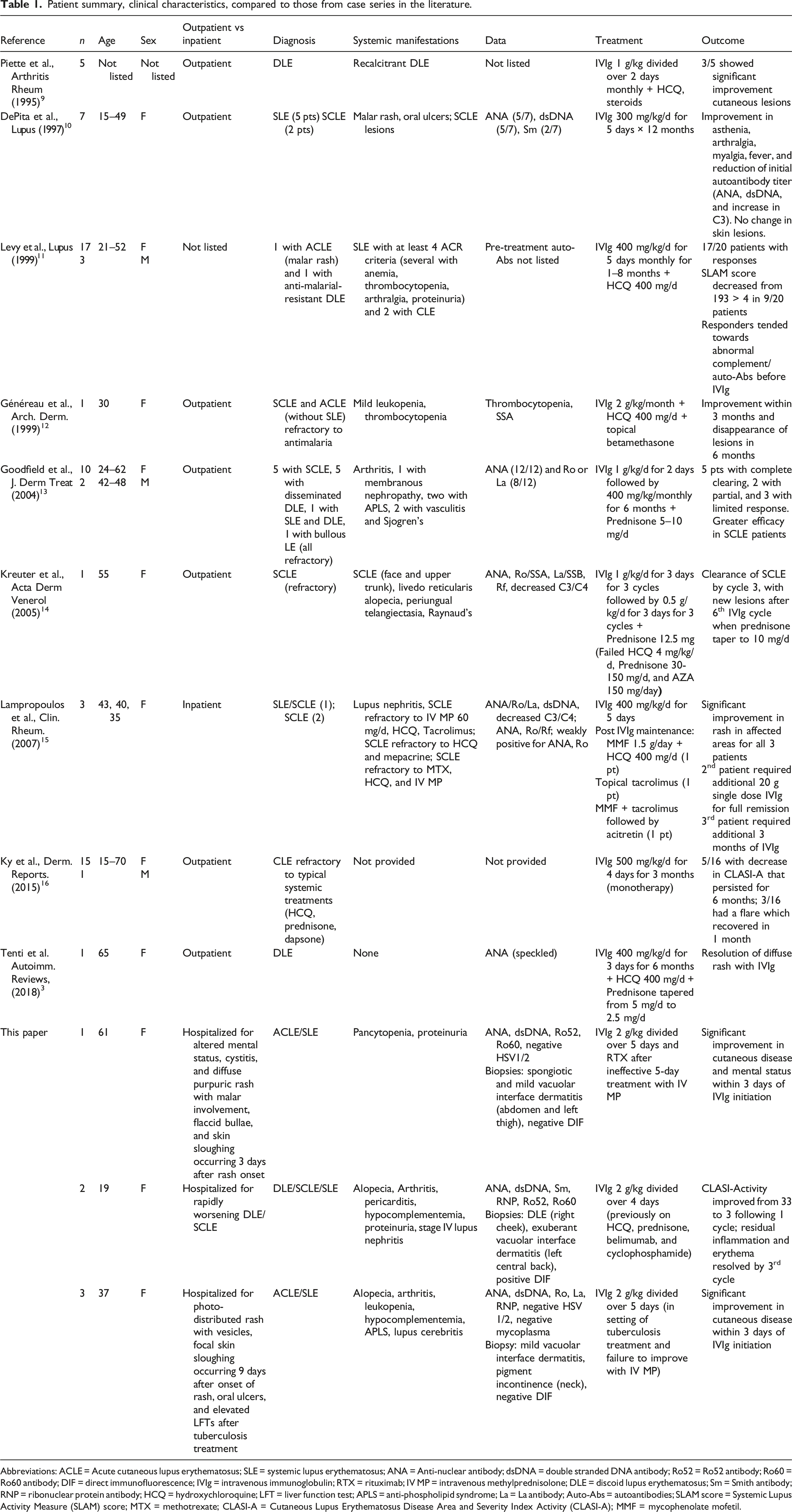
Clinical image of rapidly worsening cutaneous lupus erythematosus in three hospitalized patients with SLE before and after IVIg treatment. (A and B) Malar rash on face and diffuse cutaneous involvement of torso on Case 1, with dusky macules and patches, multiple scattered bullae, and positive Nikolsky sign. (C) Additional bullae formation on left arm on 1 mg/kg methylprednisolone prompting change in therapeutic strategy to IVIg. (D) Improvement of rash on left arm after 4 days of 2 g/kg IVIg treatment. (E) Hyperpigmented, thin scaly plaques on the torso of Case 2 surrounded by peripheral erythema suggestive of rapidly worsening DLE/SCLE. (F) Resolution of inflammation with residual hyperpigmentation 2 weeks after 3rd cycle of IVIg 2 g/kg. (G and H) On Case 3, new flaccid vesicles (G, red arrow) forming on day 4 of intravenous 2 mg/kg methylprednisolone treatment, with subsequent development of focal positive Nikolsky sign on neck and upper chest (H), prompting a change in treatment to IVIg. (I) Resolution of rash after 4 days of 2 g/kg IVI.g. Patient summary, clinical characteristics, compared to those from case series in the literature. Abbreviations: ACLE = Acute cutaneous lupus erythematosus; SLE = systemic lupus erythematosus; ANA = Anti-nuclear antibody; dsDNA = double stranded DNA antibody; Ro52 = Ro52 antibody; Ro60 = Ro60 antibody; DIF = direct immunofluorescence; IVIg = intravenous immunoglobulin; RTX = rituximab; IV MP = intravenous methylprednisolone; DLE = discoid lupus erythematosus; Sm = Smith antibody; RNP = ribonuclear protein antibody; HCQ = hydroxychloroquine; LFT = liver function test; APLS = anti-phospholipid syndrome; La = La antibody; Auto-Abs = autoantibodies; SLAM score = Systemic Lupus Activity Measure (SLAM) score; MTX = methotrexate; CLASI-A = Cutaneous Lupus Erythematosus Disease Area and Severity Index Activity (CLASI-A); MMF = mycophenolate mofetil.
Nine out of 10 prior reports describe clinical improvement in patients with CLE treated with IVIg. Only two describe the efficacy of IVIg for acute facial CLE (Table 1). However, none describes the use of IVIg for patients with SLE with severe, skin-predominant disease requiring hospitalization. Here, we show that IVIg may be an effective and safe therapy for such patients, particularly in those with high autoantibody burdens. While the predominant mechanism of action of IVIg in CLE is unknown, IVIg exerts diverse immunomodulatory activities. In cases of CLE driven by autoantibodies, IVIg may mitigate disease by saturating the neonatal Fc receptor, thereby reducing the half-life of autoantibodies. In ACLE, anti-CD95 (FAS) antibodies in IVIg preparations may block the CD95-CD95 L interactions involved in keratinocyte death and acantholysis. 6 In CCLE/SCLE, which are known to have an elevated Type I interferon signature, 7 IVIg has been shown to outcompete pathogenic immune complexes from binding to Fcγ receptor IIa on cutaneous plasmacytoid dendritic cells, thereby blunting downstream activation of toll-like receptors 7 and 9 that otherwise stimulate production of interferon-α. 8 Future studies on the use of IVIg could inform additional management and treatment strategies.
Footnotes
Acknowledgments
We are grateful to our patients for their willingness to share their clinical photographs and hospitalization course in this series.
Jun Kang is supported by the Dermatology Foundation Medical Dermatology Career Development Award.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Reprint requests
Jun Kang.