
Abstract
Introduction
Systemic Lupus Erythematosus (SLE) is a chronic autoimmune disease that often manifests during productive years and frequently involves the central nervous system (CNS), including cognitive dysfunction, which occurs at twice the prevalence of the general population. While the Montreal Cognitive Assessment (MoCA) is effective for detecting mild cognitive impairment, no reliable biomarkers that indicate SLE patients at risk of cognitive dysfunction exist. Neuron-specific enolase (NSE), a specific marker of neuronal cell damage, has been shown in several studies to be highly expressed in cognitive dysfunction. This study serves as a preliminary investigation to examine the relationship between serum NSE levels and cognitive function in SLE patients.
Methods
A cross-sectional study was conducted from January to August 2024 at Hasan Sadikin General Hospital, including SLE patients aged 18–55 years meeting the EULAR/ACR 2019 criteria. Exclusion criteria included pregnancy, neurological disorders (e.g., CNS infections, neurodegenerative diseases, stroke, epilepsy, head trauma), psychiatric conditions, substance abuse, systemic metabolic disorders, malignancy, other autoimmune diseases, or HIV. Cognitive function was assessed using MoCA-Indonesian version (MoCA-Ina) and serum NSE levels were measured. Associations between serum NSE and MoCA-Ina scores were analyzed using Spearman’s correlation (p < .05).
Results
Eighty-one participants (median age 32 years; 93.8% female) were included. Cognitive dysfunction (MoCA-Ina <26) was identified in 38.3%. Median serum NSE levels were higher in participants with cognitive dysfunction compared to those with normal cognition (14.0 ng/mL vs 12.7 ng/mL). Serum NSE levels showed a negative correlation with MoCA-Ina total scores (r = −0.225, p = .022) and executive function (r = −0.204, p = .034). Cognitive dysfunction was also associated with longer disease duration and a history of seizures.
Conclusion
This study demonstrates a significant association between neuronal injury, as indicated by elevated serum neuron-specific enolase (NSE) levels, and cognitive impairment in SLE patients, with a particular impact on executive function. Longitudinal studies incorporating neuronal biomarkers are essential to provide deeper insights into the progression of cognitive dysfunction in SLE patients.
Introduction
Systemic Lupus Erythematosus (SLE) is a chronic autoimmune disease that causes inflammation in connective tissues. SLE has a propensity to affect any organ or tissue in the body, leading to highly variable clinical manifestations across patients. Although SLE can occur across all age groups, it is more commonly observed between the ages of 15 and 45 years. 1 The prevalence of cognitive dysfunction among SLE patients is twice as high as in the general population. 2 Cognitive dysfunction is frequently reported as a significant complaint by SLE patients, negatively impacting their socioeconomic functioning, employment, and overall quality of life. 3
The pathomechanism of cognitive dysfunction is complex and not yet fully understood. After decades of research, it is now believed that the neuropsychiatric SLE (NPSLE) manifestations are associated with intricate mechanisms. Genetic factors, blood–brain barrier (BBB) dysfunction, vascular lesions, multiple autoimmune antibodies, cytokines, and neuronal cell death are all thought to contribute to these manifestations.3,4 The identification of reliable neural biomarkers to detect structural neuronal damage in cognitive dysfunction in SLE is currently needed to indicate SLE patients at risk of cognitive impairment.
Neuron-specific enolase (NSE) is a glycolytic enzyme found in neurons, typically confined to the cell body and not secreted under normal conditions. When neurons are damaged, NSE is released into the extracellular space and cerebrospinal fluid (CSF), making it a valuable biomarker for neuronal injury. Elevated NSE levels correlate with neuronal loss and disease progression, highlighting its potential for detecting and tracking cognitive impairment in SLE patients. Neuron-specific enolase levels were elevated in both the CSF and serum, which appears to be a good marker reflecting the severity of neurological compromise and poorer outcomes in brain-injured patients.5,6 However, NSE in CSF decreased significantly over time in storage condition, hence plasma NSE serves as a valid experimental biomarker, enabling the quantification of neuronal injury levels through a non-invasive approach.7–9 Given the paucity of research on the correlation between NSE levels and cognitive dysfunction in SLE patients, as well as the potential clinical benefits of measuring NSE in these patients, this study aims to investigate the relationship between serum NSE levels and cognitive function in SLE patients.
Materials and methods
We performed a cross-sectional study at the rheumatic outpatient clinics of Hasan Sadikin General Hospital, Bandung, Indonesia. Data were collected from January 2024 to August 2024. We recruited only participants aged from 18 to 55, who were documented in the SLE registry, diagnosed by a rheumatologist based on the 2019 EULAR/ACR criteria, for a minimum of 6 months, with a minimum education level of high school or 12 years of schooling. Informed consent was obtained from all participants in this study. All patients with pregnancy, history of neurological disorders (e.g., CNS infections, neurodegenerative diseases, stroke, epilepsy, multiple sclerosis, head trauma), psychiatric conditions, substance abuse, systemic metabolic disorders (uremia, infections, pulmonary or cardiac decompensation), on benzodiazepine therapy, malignancy, other autoimmune diseases or HIV were excluded. Sociodemographic, clinical, and therapeutic data were collected. In addition, we obtain recent laboratory tests from registry data, such as anti-dsDNA and Complement 3 (C3). Disease activity of SLE was measured using the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI). 10 The Systemic Lupus International Collaborating Clinics/American College of Rheumatology (SLICC/ACR) Damage Index (SDI) was calculated based on organ damage that occurred after diagnosis with SLE. 11 This study was approved by the Ethics Committee of Hasan Sadikin General Hospital (Ethics Approval Number: DP.04.03/D.XIV.6.5/20/2024) on January 23, 2024. All participants provided written informed consent prior to enrolment in the study.
Peripheral blood samples were drawn to evaluate serum levels of Neuron-specific Enolase (NSE) and were processed immediately and stored in the refrigerator at the Clinical Pathology Laboratory at Hasan Sadikin General Hospital with a stable temperature of −20°C. The NSE serum was performed by enzyme-linked immunosorbent assay (ELISA) technique according to the manufacturer’s manual from Elabscience Biotechnology Co., Wuhan, China.
The Montreal Cognitive Assessment - Indonesian version (MoCA-Ina) was used to assess the cognitive function of all subjects. A score ≤25 is considered positive for cognitive impairment based normal cut-off point of 26 for a healthy person in our local MoCA-Ina validation study. 12 This is in line with the study by Paez-Venegas et al., which demonstrated the high sensitivity (84%) and specificity (100%) of the MoCA in identifying cognitive decline in SLE patients compared to standardized neuropsychological batteries. 13 The Beck Anxiety Inventory (BAI) and the Beck Depression Inventory-II (BDI-II) were used to identify the presence of anxiety or depression. A BAI score greater than 25 indicates clinically significant symptoms of anxiety, meanwhile a BDI-II score greater than 28 reflects clinically significant symptoms of depression. 14
Data in numerical variables were presented as mean (SD) for parametric data and median (IQR) for non-parametric data, while categorical variables were exposed in frequency and prevalence rate. The Mann-Whitney U test, Unpaired t test, Chi Square and Fisher-Exact were used to analyze the characteristics. In addition, Spearman Rank test was used in investigating the association between categorical variables. A significance level of 5% was adopted, and all statistical analyses were performed using the SPSS statistical program version 23.0.
Results
Participant characteristic
Demographic, clinical characteristics, laboratory, cognitive function in SLE patients.
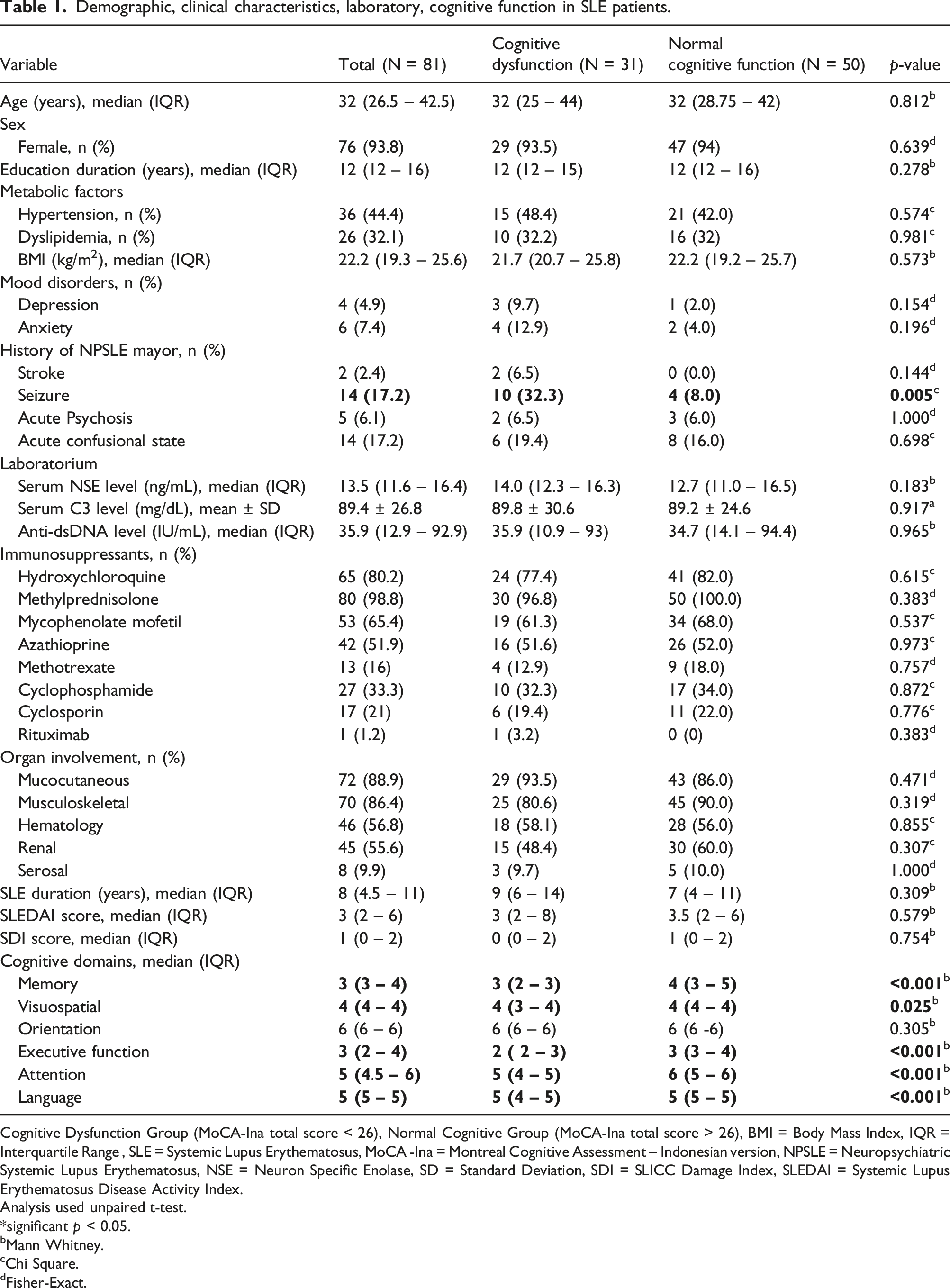
Cognitive Dysfunction Group (MoCA-Ina total score < 26), Normal Cognitive Group (MoCA-Ina total score > 26), BMI = Body Mass Index, IQR = Interquartile Range , SLE = Systemic Lupus Erythematosus, MoCA -Ina = Montreal Cognitive Assessment – Indonesian version, NPSLE = Neuropsychiatric Systemic Lupus Erythematosus, NSE = Neuron Specific Enolase, SD = Standard Deviation, SDI = SLICC Damage Index, SLEDAI = Systemic Lupus Erythematosus Disease Activity Index.
Analysis used unpaired t-test.
*significant p < 0.05.
bMann Whitney.
cChi Square.
dFisher-Exact.
A significant finding was the prevalence of a history of seizures as a major neuropsychiatric manifestation of SLE, which showed that the cognitive dysfunction group had a higher incidence of seizures (32.3%) compared to the normal cognitive group (8.0%), with a statistically significant difference (p = .005). In the group with mood disorders such as depression and anxiety, although the prevalence of mood disorders was higher in the cognitive dysfunction group, the difference was not statistically significant.
On the other hand, serum NSE levels, along with various other laboratory parameters, including C3 and anti-dsDNA, did not show significant differences between the two groups. There were also no significant differences in the use of immunosuppressants, SLE-related organ involvement, or disease duration between the groups. However, we found a positive correlation between total MoCA-Ina score with education duration (r = 0.327, p = .003), but no significant correlation with patient age (r = −0.163, p = .146). Cognitive function domains assessed in the MoCA-Ina, were significantly different between the normal and impaired cognitive function groups, except for the orientation domain.
Serum NSE levels and cognitive function in SLE patients
The correlation between serum NSE levels and cognitive function in SLE patients.
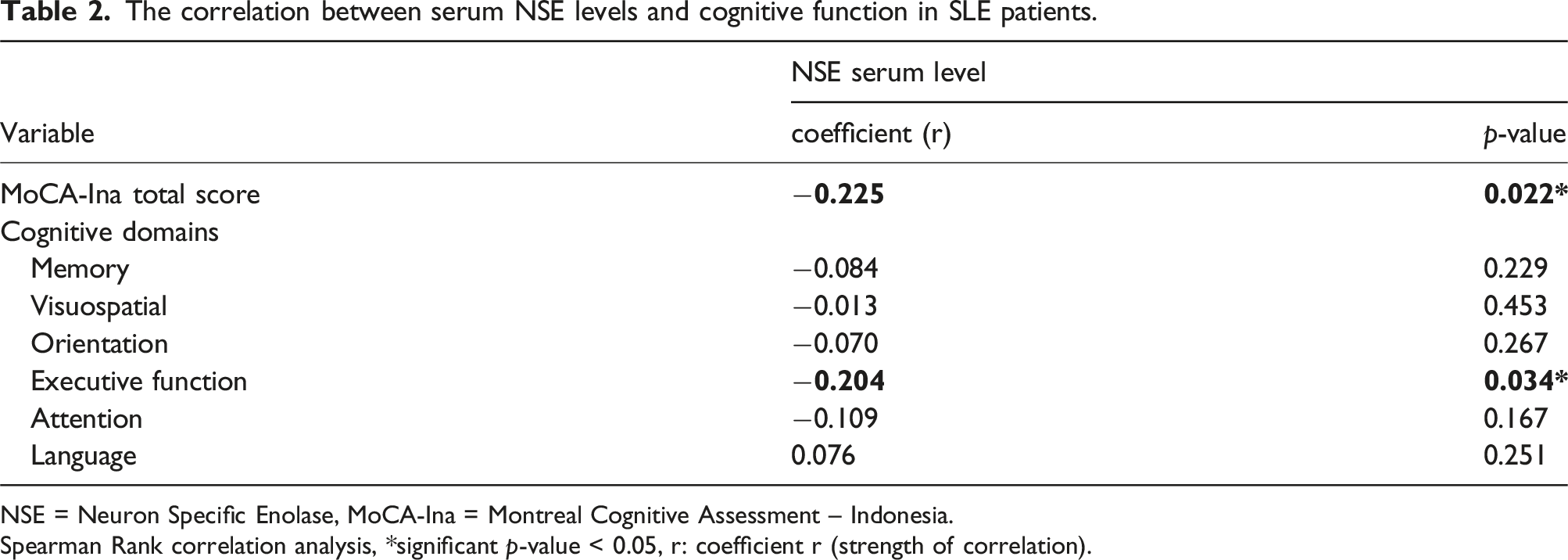
NSE = Neuron Specific Enolase, MoCA-Ina = Montreal Cognitive Assessment – Indonesia.
Spearman Rank correlation analysis, *significant p-value < 0.05, r: coefficient r (strength of correlation).
Correlation serum NSE levels, cognitive function and clinical parameters in SLE patients
The correlation between clinical parameters with serum NSE levels and MoCA-Ina scores in SLE patients.
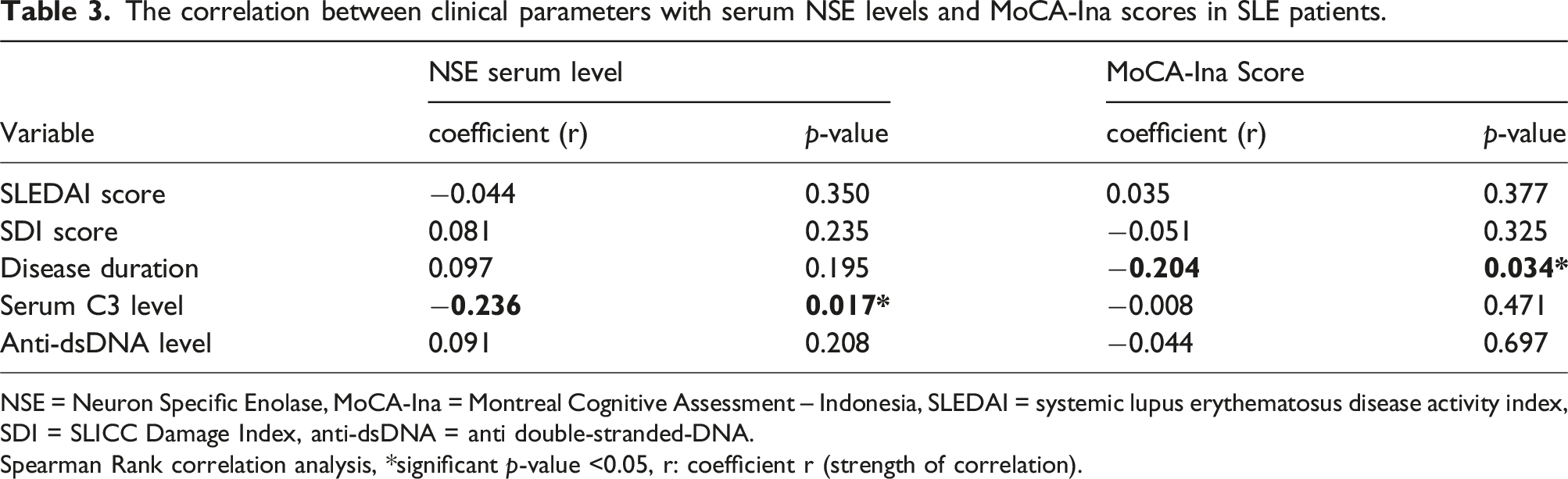
NSE = Neuron Specific Enolase, MoCA-Ina = Montreal Cognitive Assessment – Indonesia, SLEDAI = systemic lupus erythematosus disease activity index, SDI = SLICC Damage Index, anti-dsDNA = anti double-stranded-DNA.
Spearman Rank correlation analysis, *significant p-value <0.05, r: coefficient r (strength of correlation).
Discussion
In this study, it was found that SLE patients were of productive age with a median age of 32 years with ages ranging from 19 to 54 years and the majority were female, 76 (93.8%). The age and gender characteristics of the subjects in this study were in line with global SLE data. 1 A total of 15 (18.5%) patients from the total subjects had experienced SLE from the age of under 18 years or childhood-onset SLE. This is similar to previous studies where pediatric-onset SLE accounted for 15%–20% of all lupus patients. The study also showed that a group of young adults with a diagnosis of childhood-onset SLE showed a high prevalence of cognitive dysfunction. 15 In this study, it was found that 46.7% of patients with childhood-onset SLE experienced cognitive dysfunction. An association between cognitive dysfunction and loss of grey matter volume (GMV) and white matter volume (WMV) was found in patients with childhood-onset SLE. 16
In this study, a positive correlation was shown between the duration of education and the total MoCA-Ina score. The level of education was one of the factors that influenced the decline in cognitive function in SLE patients, 17 as in research conducted by Nantes et al., which showed that every 1-year increase in education could reduce the probability of cognitive decline by up to 19%. 18 The level of education could directly influence cognitive reserve, which is defined as the ability of the brain to withstand damage due to pathological conditions, thereby delaying the clinical manifestation of a pathology. 19
The age variable in several previous studies showed a negative correlation with cognitive performance.20,21 Age was not found to be related to cognitive function in this study, which was different from previous studies which may be due to the average age of patients in this study being younger than previous studies and the age restrictions (18 - 55 years old) on patients were included to avoid bias in cognitive function decline due to aging.
Mood disorders have been evaluated in several studies regarding their association with cognitive function in SLE patients. In this study, it was found that 4.9% of SLE patients had depression and 7.4% had anxiety. Findings that were not much different were found in the study of Bai et al. which found SLE comorbidity in the form of depression and anxiety, respectively 8% and 11.9%. 22 This was lower than the study by Raghunath et al., which found comorbidity of depression and anxiety in SLE patients, 37% and 27%, respectively. 20 A meta-analysis study by Moustafa et al., found a combined total prevalence rate of 35.2% for depression and 24.2% for anxiety. This variability may be due to a lack of standardization of definitions and metrics used to measure depression and anxiety. 23
In this study, it was found that a previous history of neuropsychiatric SLE in the form of seizures had a significant difference between the cognitively normal and impaired groups. In the study of Raghunath et al., analysis of individual disorders in the neuropsychiatric SDI domain, seizures were associated with an increased prevalence of cognitive dysfunction. 20
In the context of SLE, a widely accepted explanation for the development of seizures in neuropsychiatric SLE includes the role of autoantibodies in the CNS. Two studies described the induction of autoantibodies causing focal or diffuse damage to the CNS, most of which could be attributed to aPL antibodies, although they could be extrapolated to other antibodies. Brain structural changes could be associated with the development of seizures, such as the local scarring associated with a chronic inflammatory condition or secondary to damage from a thrombotic event. 24 These processes have emerged as a key contributor to cognitive dysfunction by disrupting neural networks and the loss of synapses following the brain injury. 25
In this study, it was found that the prevalence of stroke developed after SLE diagnosis was found in 2.4%, and only in the impaired cognitive function group. The stroke incidence rate found was not much different compared to previous cohort studies which found a stroke incidence of 3.1% in the SLE population. 26 The prevalence of stroke in the SLE ranged from 2% to 19%, while the incidence ranged from 5.8 to 25.3 new cases per 1000 persons. Large differences between previous studies may be explained by various factors, such as duration of follow-up, race, age, and study design. 27
The incidence of acute psychosis occurred in 0.6%–11% of SLE patients. 28 Similar results were found in this study, 6.1% had a history of acute psychosis in SLE patients. Psychosis in SLE can occur either as a result of neuro-lupus or the drugs used to treat it (e.g., glucocorticoids and chloroquine). 29 Anti-P antibodies can also cross-react with NMDAR, resulting in psychosis, although the presence of anti-P is not always associated with neuropsychiatric manifestations of SLE. 30 A total of 17.2% of patients in this study experienced a history of acute confusional state. An acute confusional state is one of the rare manifestations of neuropsychiatric SLE and is associated with increased morbidity and mortality. The prevalence of acute confusional state in SLE was reported to be around 4%–7%. This condition can occur due to CNS infection, metabolic changes, and changes in treatment, especially corticosteroids. 31 The use of corticosteroids and immunosuppressants in this study showed no significant differences between the normal and impaired cognitive groups. The relationship between corticosteroids and cognitive dysfunction remains a controversial topic. In a previous study, SLE patients with and without corticosteroid use were found to have poorer decision-making capacity compared with healthy controls. 16
Cognitive dysfunction affects 20%–80% of SLE patients, both those with clear CNS involvement and those without.16,32 In this study, we found that 38.3% of SLE patients experienced cognitive function impairment. A comparison of cognitive domain scores between normal and impaired cognitive groups found significant differences in the domains of memory, visuospatial, executive function, attention, and language. Similar results were found by Yue et al., who compared the cognitive function domains of SLE patients based on the MoCA. 33
To our knowledge, this is the first study to specifically examine serum NSE levels and cognitive function in SLE patients. In this study, an inverse correlation was found between serum NSE levels and the total MoCA-Ina score (r = −0.225, p 0.022). Serum NSE levels have also been studied in a population of type 2 diabetes mellitus patients who experience cognitive dysfunction, where pathomechanical features similar to SLE patients occur, due to inflammatory processes and vascular factors. 34 In the study of Yu et al., they found that serum NSE levels had a significant negative correlation with MMSE total score, the median serum NSE value in the cognitive impairment group was 14.55 with an IQR of 12.00 – 17.57. 35 This is not much different from the value obtained in this study, with a median of 14.0 with an IQR of 12.3–16.3.
The autoimmune mechanism in systemic lupus erythematosus (SLE) contributes to blood–brain barrier (BBB) dysfunction, allowing the entry of circulating autoantibodies into the central nervous system (CNS). This can trigger neurotoxic processes that lead to cognitive impairment.3,36 Neurotoxicity in SLE is thought to cause injury in several brain regions, particularly along the periventricular and frontal white matter tracts, as well as in the frontal cortical, parahippocampal areas, and subcortical grey matter structures—regions known to be critical for cognitive processing and frequently affected in SLE patients.16,17,37 Damage or death of neuronal and glial cells results in the release of intracellular enzymes such as neuron-specific enolase (NSE), leading to elevated serum NSE levels.35,38 Increased serum NSE is associated with neuronal injury within the CNS and may correlate with cognitive decline.35,39–42 While cognitive dysfunction in SLE is heterogeneous—affecting domains such as memory, attention, processing speed, and verbal fluency—executive dysfunction is often considered a hallmark cognitive feature in patients with SLE.2,16,43,44
In this study, a significant inverse correlation was observed between serum NSE levels and the executive function domain (r = −0.204, p = .034), but no significant correlation was found with other cognitive domains (p > .05). Impairment in executive function is a hallmark of cognitive dysfunction in SLE.16,43,44 Studies have shown that during executive function tasks, increased contralateral cerebellar-frontal activity compensates for disrupted cortico-basal ganglia-thalamic-cortical circuits in SLE patients. Diffusion tensor imaging (DTI) studies indicate that reduced fractional anisotropy (FA) in the cingulate region is significantly associated with limitations in executive function. Moreover, lower FA in the anterior corona radiata, thalamic radiation, and right external capsule correlates with poorer overall cognitive function and diminished executive skills in SLE patients.16,37
A previous study by Hawro et al. demonstrated decreased serum neuron-specific enolase (NSE) levels, reflecting chronic pathological conditions of the nervous system, in NPSLE subjects compared to those without neuropsychiatric involvement. However, when examining specific subtypes of cognitive impairment in SLE patients, NSE levels were found to be decreased in individuals with dementia (cognitive impairment
Structural topology changes in the brain, as shown by Ao et al., revealed significantly reduced structural connectivity in the prefrontal gyrus and cingulate areas in patients with neuropsychiatric SLE compared to non-neuropsychiatric SLE patients. 45 Cognitive function relies on the efficient operation of distributed brain networks interconnected by white matter (WM). Disruptions in WM structural connectivity can impair these networks, leading to cognitive dysfunction via a “Disconnection Syndrome.” This phenomenon is similarly observed in the pathology of small vessel disease, which is characterized by early deficits in executive function and processing speed. 46
A notable finding of this study is the underdiagnosis of cognitive dysfunction in clinical practice, even in settings where annual SDI assessments are routinely performed. Among the 31 patients identified with cognitive dysfunction based on the MoCA-Ina evaluation, only 3 (9.6%) had their cognitive impairment documented in the SDI scoring. This observation is consistent with the findings of Raghunath et al., who reported that cognitive dysfunction was recognized in only 8% of cases using SDI assessments. 20
The disease duration of SLE was found to have a negative correlation with cognitive function in this study. Similarly, Wiseman et al. reported worse cognitive function associated with longer SLE duration, in their study population and exhibited higher mean diffusivity (MD) levels on diffusion tensor MRI. Significantly elevated MD levels were observed across all WM tracts, indicating a decline in WM microstructural integrity.47,48
This study found a negative correlation between serum NSE levels and C3 levels. This may reflect a neurotoxicity process triggered by complement activation. The neurotoxic effects of complement activation products have been demonstrated through their potential to induce apoptosis in experimental animal models by increasing the expression of cerebral glutamate receptors and through the upregulation of inducible nitric oxide synthase, Tumour Necrosis Factor Receptor-1 (TNFR1), and Intercellular Adhesion Molecule-1 (ICAM-1) expression. 3 The fact that only C3 and AP50 are associated with diffuse NPSLE is particularly intriguing and may not be influenced by concurrent disease activity. In murine models of lupus cerebritis, targeted and selective inhibition of the alternative complement pathway is effective, leading to the hypothesis that the alternative complement pathway may play a role in the pathogenesis of diffuse NPSLE in patients. 49
The relationship between disease activity and cognitive dysfunction in SLE remains controversial, with studies reporting inconsistent findings. 24 In this study, the absence of correlation between disease activity, MoCA performance, and serum NSE levels may be explained by the fact that SLEDAI reflects immune activity at a single point in time, whereas neuronal injury and cognitive dysfunction represent cumulative and potentially chronic processes. Similarly, no correlation was observed between SDI scores, serum NSE levels, and MoCA performance. This may be due to the differing temporal focus and sensitivity of these measures. While SDI captures cumulative, irreversible organ damage, it lacks the ability to detect subtle or early central nervous system involvement. In contrast, MoCA evaluates current cognitive function, and NSE may reflect subclinical or recent neuronal injury. Additionally, disease duration did not correlate with serum NSE levels but showed an inverse correlation with MoCA performance. This finding may indicate that while NSE reflects active neuronal injury, longer disease duration is associated with progressive, low-grade neurodegeneration or vascular damage, which contributes to cognitive decline over time.
This study has several notable limitations. First, its cross-sectional design restricts the ability to assess longitudinal changes or causal relationships between serum NSE levels and cognitive function in patients with SLE. While the MoCA-Ina serves as a practical screening tool for early cognitive impairment, comprehensive neuropsychological testing remains the gold standard for cognitive assessment in this population. The relatively small sample size and predominance of patients with mild disease activity may limit the generalizability of the findings to the broader SLE population. Additionally, the absence of data regarding corticosteroid and immunosuppressive therapy, particularly cumulative and daily dosages, may have hindered a more detailed evaluation of their potential impact on cognitive outcomes and biomarker levels. The study also lacked advanced neuroimaging techniques, such as functional MRI or PET scans, which could have provided valuable insights into the structural and functional brain changes associated with cognitive dysfunction in SLE. Furthermore, NSE levels were measured solely using ELISA without confirmatory testing via alternative methods. Finally, the findings require external validation in larger, independent cohorts to confirm their broader applicability.
Conclusion
In conclusion, serum NSE levels might serve as a potential biomarker for quantifying neuronal damage in the brains of SLE patients, particularly in relation to executive dysfunction. Cognitive function in this population appears to be influenced by factors such as disease duration, educational level, and a history of NPSLE, particularly seizure. Routine cognitive function assessments using the MoCA test, in conjunction with SDI score evaluations, are recommended for early detection and monitoring of cognitive dysfunction in SLE patients.
Future studies should include a more diverse population of SLE patients, encompassing a broader range of disease activity, to better capture the full spectrum of cognitive dysfunction and its potential correlation with serum NSE levels across varying severities of the disease. Based on the findings of this study, exploring the utility of serum NSE levels as a predictor of long-term cognitive outcomes is crucial and can be achieved through longitudinal follow-up of patients with normal cognitive function at baseline who exhibit elevated serum NSE levels. Advanced neuroimaging modalities, such as functional MRI or PET scans, should be considered in future research to investigate structural and metabolic alterations in the brain that contribute to cognitive dysfunction in SLE patients.
Footnotes
Acknowledgments
The authors would like to express their gratitude to all participants for their contributions to this study. We also appreciate the assistance of dr. Hans Albertus and Novita Purnamasari, S. Psi., M. Psi in data collection of this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.