
Abstract
Objective
To detect the expression levels of TWEAK and CD163 in monocytes from the peripheral blood of patients with systemic lupus erythematosus (SLE) complicated with renal involvement (SLE+RI) and to explore the application value of TWEAK and CD163 in the diagnosis of SLE and SLE+RI.
Methods
The expression levels of TWEAK and CD163 in the monocytes of 70 SLE patients and the control group were determined by real-time fluorescence quantitative polymerase chain reaction (RT‒qPCR). To analyse the relationship between TWEAK/CD163 expression levels and laboratory examination and clinical manifestations in monocytes of SLE+RI patients. The sensitivity and specificity of TWEAK and CD163 for the diagnosis and differential diagnosis of SLE+RI were analysed by receiver operating characteristic (ROC) curves. Western blot experiments were used to evaluate the protein expression of TWEAK and CD163 in monocytes.
Results
The expression levels of TWEAK and CD163 in monocytes were significantly greater in the SLE group than in the healthy control (HC) and rheumatoid arthritis (RA) groups. The expression levels of TWEAK and CD163 in monocytes from anti-double-stranded DNA antibody (anti-dsDNA)-positive patients and patients with proteinuria were respectively greater than those from anti-dsDNA-negative patients and patients without proteinuria. The expression levels of both genes were significantly lower after treatment than before treatment in the SLE+RI group (p < 0.05). The expression levels of TWEAK and CD163 in monocytes were positively correlated with the SLE activity score (SLEDAI) in the SLE+RI group. ROC curve analysis revealed that the area under the curve (AUC) of TWEAK expression was 0.869 in the SLE+RI group. The AUC of CD163 in the SLE+RI group was 0.792, the combined expression of TWEAK and CD163 was 0.842 in the SLE+RI group. TWEAK and CD163 protein expression in monocytes from patients with SLE+RI was significantly increased compared with that in controls.
Conclusion
The expression levels of TWEAK and CD163 are increased in SLE patients, and the expression levels in SLE+RI patients are greater than those in SLE-RI patients. These findings are closely related to disease activity, autoantibody production and clinical symptoms and can be used as biomarkers for the diagnosis and activity of SLE+RI.
Introduction
Systemic lupus erythematosus (SLE) is a common chronic systemic autoimmune disease with an unknown aetiology and is more common in women of childbearing age. 1 SLE renal involvement (SLE+RI) refers to immune damage to the kidneys due to SLE with corresponding clinical manifestations. Epidemiological studies indicate that renal involvement occurs in up to 70% of SLE patients, with 10%–30% progressing to renal failure,2,3 whereas early renal impairment in SLE patients is often insidious, and its early diagnosis is particularly important. 4 The weak inducer of tumour necrosis factor apoptosis (tumour necrosis factor-like weak inducer of apoptosis (TWEAK)), a new member of the TNF ligand superfamily, can be expressed in a variety of tissues and cells in the human body. Previous studies have shown that TWEAK plays an important role in the pathogenesis of lupus nephritis and can better distinguish between lupus nephritis and non-SLE nephritis.5,6 The haemoglobin-specific scavenger receptor (HbSR), also known as CD163, is a member of the scavenger receptor cysteine-rich (SRCR) superfamily. It is a membrane surface protein that is specifically expressed on M2 macrophages and is involved in the pathogenesis and progression of renal damage in patients with SLE.7,8 Researchers have reported that TWEAK shares similar regions of molecular structure with haemoglobin-bound globin (Hb-Hp). There are 44 interaction sites between TWEAK and CD163. TWEAK can bind to CD163 as a selective ligand and interact with it.9–11 Monocytes play a key role in the onset and progression of lupus nephritis. Immunohistochemical analysis revealed that monocyte macrophages infiltrate the renal interstitium and glomerulus in lupus nephritis patients and that the degree of infiltration is related to the adverse outcome of renal function and the severity of proteinuria. 12 However, the expression of TWEAK and CD163 in monocytes from SLE+RI patients and whether TWEAK and CD163 are involved in the development of SLE+RI have not been reported. Our research highlights the value of the expression levels of TWEAK and CD163 in peripheral blood monocytes from patients with SLE+RI and provides reference values for the participation of TWEAK and CD163 in the occurrence and development of renal involvement in SLE.
Materials and methods
Subjects
Laboratory measures and clinical characters of SLE + RI, SLE-RI, RA and HC.
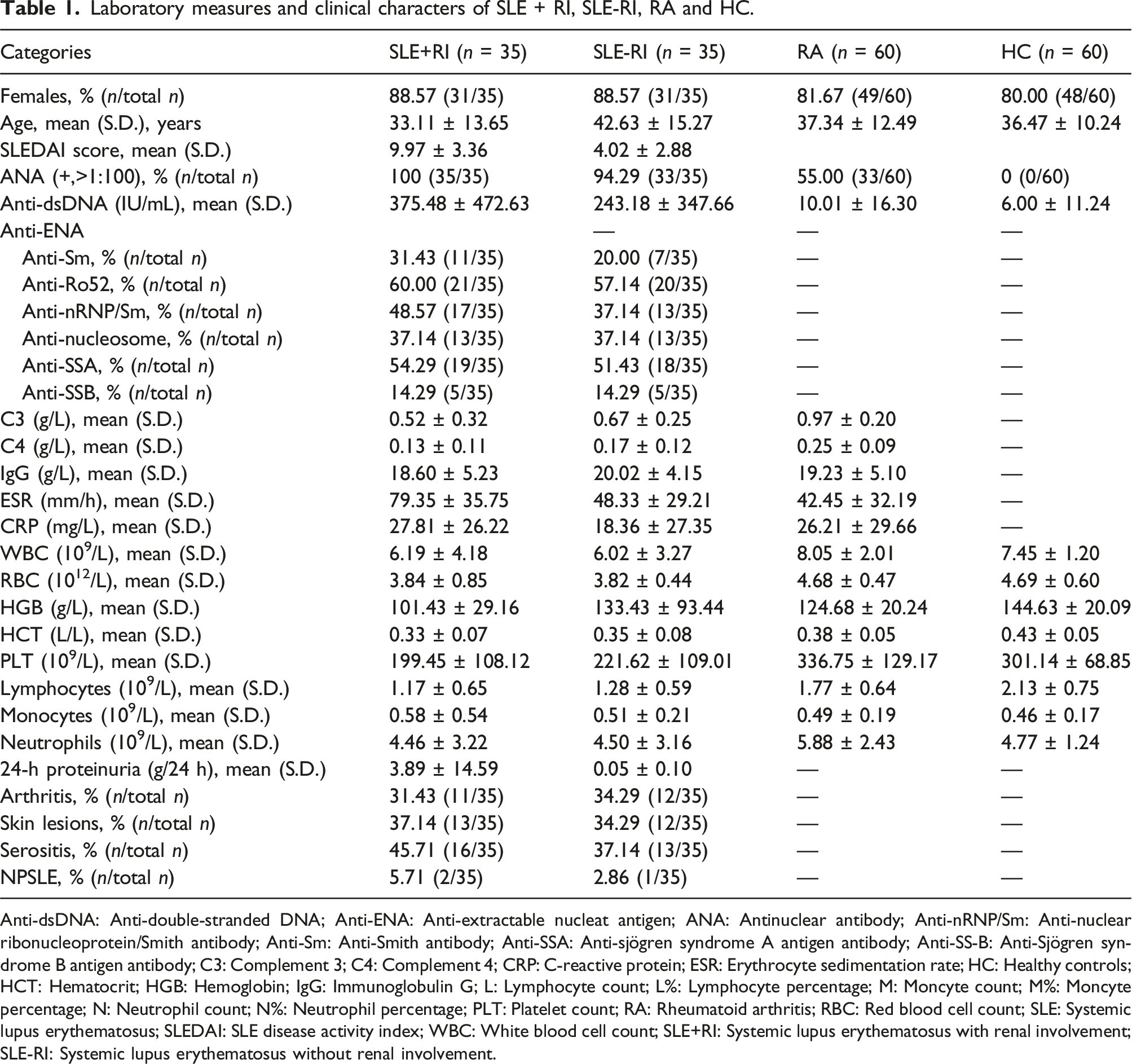
Anti-dsDNA: Anti-double-stranded DNA; Anti-ENA: Anti-extractable nucleat antigen; ANA: Antinuclear antibody; Anti-nRNP/Sm: Anti-nuclear ribonucleoprotein/Smith antibody; Anti-Sm: Anti-Smith antibody; Anti-SSA: Anti-sjögren syndrome A antigen antibody; Anti-SS-B: Anti-Sjögren syndrome B antigen antibody; C3: Complement 3; C4: Complement 4; CRP: C-reactive protein; ESR: Erythrocyte sedimentation rate; HC: Healthy controls; HCT: Hematocrit; HGB: Hemoglobin; IgG: Immunoglobulin G; L: Lymphocyte count; L%: Lymphocyte percentage; M: Moncyte count; M%: Moncyte percentage; N: Neutrophil count; N%: Neutrophil percentage; PLT: Platelet count; RA: Rheumatoid arthritis; RBC: Red blood cell count; SLE: Systemic lupus erythematosus; SLEDAI: SLE disease activity index; WBC: White blood cell count; SLE+RI: Systemic lupus erythematosus with renal involvement; SLE-RI: Systemic lupus erythematosus without renal involvement.
Extraction of total RNA from monocytes and cDNA synthesis
Peripheral blood samples (2 mL) were drawn from the median cubital vein with an ethylene diamine tetraacetic acid (EDTA) anticoagulated vacutainer from all the patients and healthy controls. Peripheral blood mononuclear cells (PBMCs) were extracted with Ficoll isolation, and monocytes were extracted according to the standard procedure of CD14+ cell magnetic bead sorting reagent (Stemcell Corporation, USA). Total RNA was extracted from all the subjects via the TRIzol reagent (Invitrogen, USA) protocol, and diethyl pyrocarbonate (DEPC)-treated distilled water was used to dissolve the RNA. One millilitre of the extracted total RNA was taken, and the RNA was reverse transcribed to cDNA using a PrimeScript reverse transcription kit (TaKaRa, Japan) according to the manufacturer protocol.
Real-time quantitative polymerase chain reaction (RT‒qPCR)
Primers used for RT-qPCR analysis.

Western blotting
Monocytes were lysed in 100 μL of cold lysis buffer and kept on ice on a shaking platform for 30 min. After centrifugation at 12,000 r/min for 10 min, the supernatants were transferred to a fresh tube and stored at −80°C. Protein concentrations were determined with a BCA Protein Assay Kit (Santa Cruz Biotechnology, CA, USA). For each sample preparation, 60 μg of total protein was mixed in Laemmli loading buffer, boiled for 5 min, separated by 10% SDS–PAGE, and then transferred to PVDF blotting membranes (Millipore, Massachusetts, USA). The membranes were blocked with Tris-buffered saline–Tween/1% nonfat dry milk and incubated with goat antibodies specific for TWEAK (1:3000 dilution, R&D Systems, Inc.), rabbit antibodies specific for CD163, and β-actin (all from Santa Cruz Biotechnology, California, USA) overnight at 4°C. After a final incubation with a 1:5000 dilution of horseradish peroxidase-conjugated secondary antibodies (Zhongshan Biotechnology, Beijing, China) for 1 hour at room temperature, the samples were exposed to X-ray film from 30 s to 3 min to visualize chemiluminescent proteins using a Bio-Rad gel imager (Hercules, California, USA). Each sample was run in triplicate.
Clinical parameters of patients with SLE
To evaluate whether the two target genes could serve as relevant biomarkers for assessing SLE disease activity, correlation analyses were performed to examine the relationships between the expression levels of these genes and the clinical features of SLE, including neuropsychiatric lupus, pericarditis, pleuritis, visual impairment, fever, rash, oral ulcers, and kidney injury. Additionally, various laboratory indicators, including white blood cell count (WBC), red blood cell count (RBC), haemoglobin (HB) level, platelet count (PLT), neutrophil percentage (N%), lymphocyte percentage (L%), routine urine parameters (protein, tube type), 24-hour urinary protein level, C-reactive protein (CRP) level, immunoglobulin G (IgG) level, complement components (C3, C4) levels, erythrocyte sedimentation rate (ESR), antinuclear antibody (ANA) level, anti-double-stranded DNA antibody (anti-dsDNA) level, and antiextractable nuclear antigen (ENA) antibody profiles, were analysed. The expression levels of these two genes were further correlated with the SLE Disease Activity Index (SLEDAI) and the renal SLEDAI (r-SLEDAI), which include four kidney-related parameters (haematuria, pyuria, proteinuria, and urinary casts), to assess the degree of renal involvement. Each parameter in the r-SLEDAI is assigned four points, resulting in a total score ranging from 0 to 16.
Statistical analysis
Statistical analysis was performed using the SPSS 23 software. The data were analysed for normality and homogeneity of variance using the Kolmogorov‒Smirnov test (KS test) and Bartlett test, respectively. If the data had a normal distribution and equal variance, a t test was used for comparisons between data; if the data did not conform to a normal distribution or variances, a nonparametric test was used for data comparisons between two groups, and a Wilcoxon test was used between paired samples. Correlations between each clinical characteristic of the candidate TWEAK or CD163 and the newly diagnosed SLE disease group or the SLE+RI disease group were analysed using Pearson correlation analysis or Spearman correlation analysis. Finally, the receiver operating characteristic (ROC) curve and area under the curve (AUC) were used to evaluate the diagnostic efficacy of the candidate TWEAK and CD163 for the newly diagnosed SLE disease group and SLE+RI disease group. A two-sided p value < 0.05 indicated a statistically significant difference.
Results
The expression levels of monocyte TWEAK and CD163
The RT‒PCR results revealed that the expression level of TWEAK in monocytes in the SLE disease group (SLE+RI and SLE-RI) was significantly greater than that in the HC and RA disease control groups (p < 0.001; Figure 1(a)). Similarly, the expression level of CD163 in monocytes from the SLE disease group was significantly greater than that in monocytes from the HC and RA disease control groups (p = 0.002, p = 0.004; Figure 1(d)). Furthermore, the expression levels of TWEAK and CD163 in monocytes from patients with SLE+RI were significantly greater than those in monocytes from patients with SLE-RI (p < 0.001, Figure 1(b); P = 0.024, Figure 1(e)). The TWEAK and CD163 expression levels in anti-dsDNA-positive SLE monocytes were significantly greater than those in anti-dsDNA-negative monocytes (p = 0.002, Figure 1(c); p = 0.007, Figure 1(g)). CD163 expression in SLE patients with proteinuria monocytes was significantly greater than that in SLE patients without proteinuria (p < 0.001, Figure 1(f)). Additionally, the expression levels of TWEAK and CD163 in monocytes from the SLE disease group after treatment were significantly lower than those in monocytes from the SLE disease group before treatment (p = 0.004 Figure 1(h); p = 0.006 Figure 1(i)). (a, d) Scatterplot of different expression of TWEAK and CD163 in monocytes from peripheral blood of newly diagnosed total SLE; (b, e) Scatterplot of different expression of TWEAK and CD163 in monocytes from peripheral blood of SLE+RI; (c, g) Scatterplot of different expression of TWEAK and CD163 in monocytes from peripheral blood of SLE with anti-dsDNA+ and anti-dsDNA-; (f) Scatterplot of different expression of CD163 in monocytes from peripheral blood of SLE with protein+ and protein-; (h, i) Scatterplot of different expression of TWEAK and CD163 in monocytes from peripheral blood of SLE+RI before treatment and SLE+RI after treatment. SLE-new: newly diagnosed patients with systemic lupus erythematosus; SLE+RI: SLE patients with renal involvement; SLE-RI: SLE patients without renal damage; RA-new: Newly diagnosed patients with rheumatoid arthritis; HC: healthy control; anti-dsDNA+: Anti-double-stranded DNA positive; anti-dsDNA-: Anti-double-stranded DNA negative; before: patients with SLE+RI before treatment; after: Patients with SLE+RI were treated; patients with proteinuria (protein+), patients without proteinuria (protein-).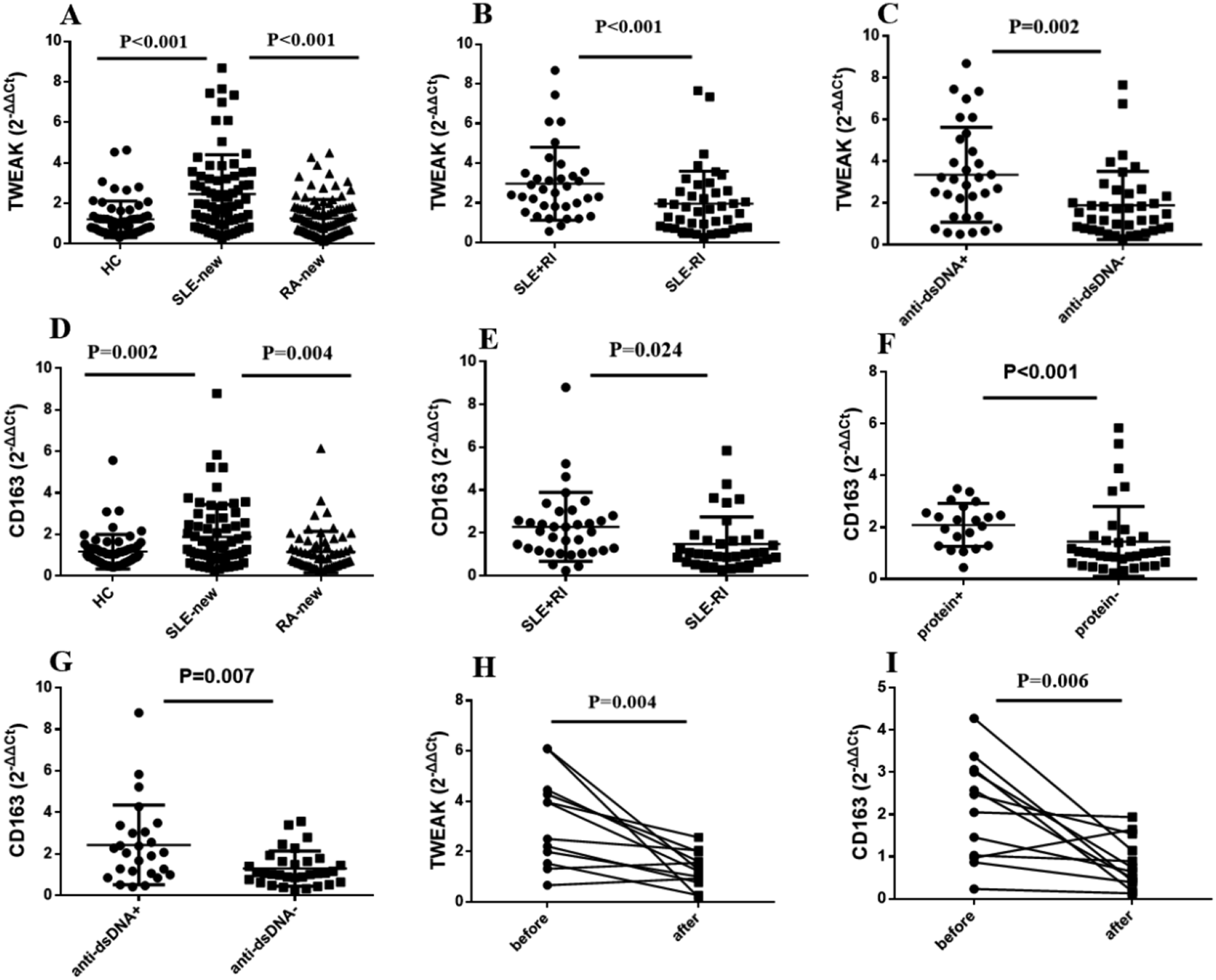
Relationships between the expression levels of monocyte TWEAK and CD163 and the clinical parameters of SLE
The results indicate that the TWEAK expression level in SLE monocytes was positively correlated with the SLEDAI (rs = 0.217, p < 0.001; Figure 2(a)) and negatively correlated with the WBC (rs = −0.288, p = 0.007; Figure 2(b)), RBC (rs = −0.290, p = 0.026; Figure 2(c)), C3 (rs = −0.321, p = 0.011; Figure 2(d)), and C4 level (rs = −0.199, p = 0.010; Figure 2(e)). The CD163 expression level in SLE monocytes was positively correlated with the SLEDAI (rs = 0.187, p = 0.034; Figure 2(f)) and negatively correlated with the WBC (rs = −0.146, p = 0.002; Figure 2(g)), N (rs = −0.133, p = 0.033; Figure 2(h)), and C3 level (rs = −0.352, p = 0.018 Figure 2(i)). (a-e) Correlation between TWEAK expression level and clinical features in monocytes from peripheral blood of newly diagnosed total SLE; (f-i) Correlation between CD163 expression level and clinical features in monocytes from peripheral blood of newly diagnosed total SLE. C3: Complement 3; C4: Complement 4; N: Neutrophil count; PLT: Platelet count; RBCRed blood cell count; SLEDAI: SLE disease activity index; WBC: White blood cell count.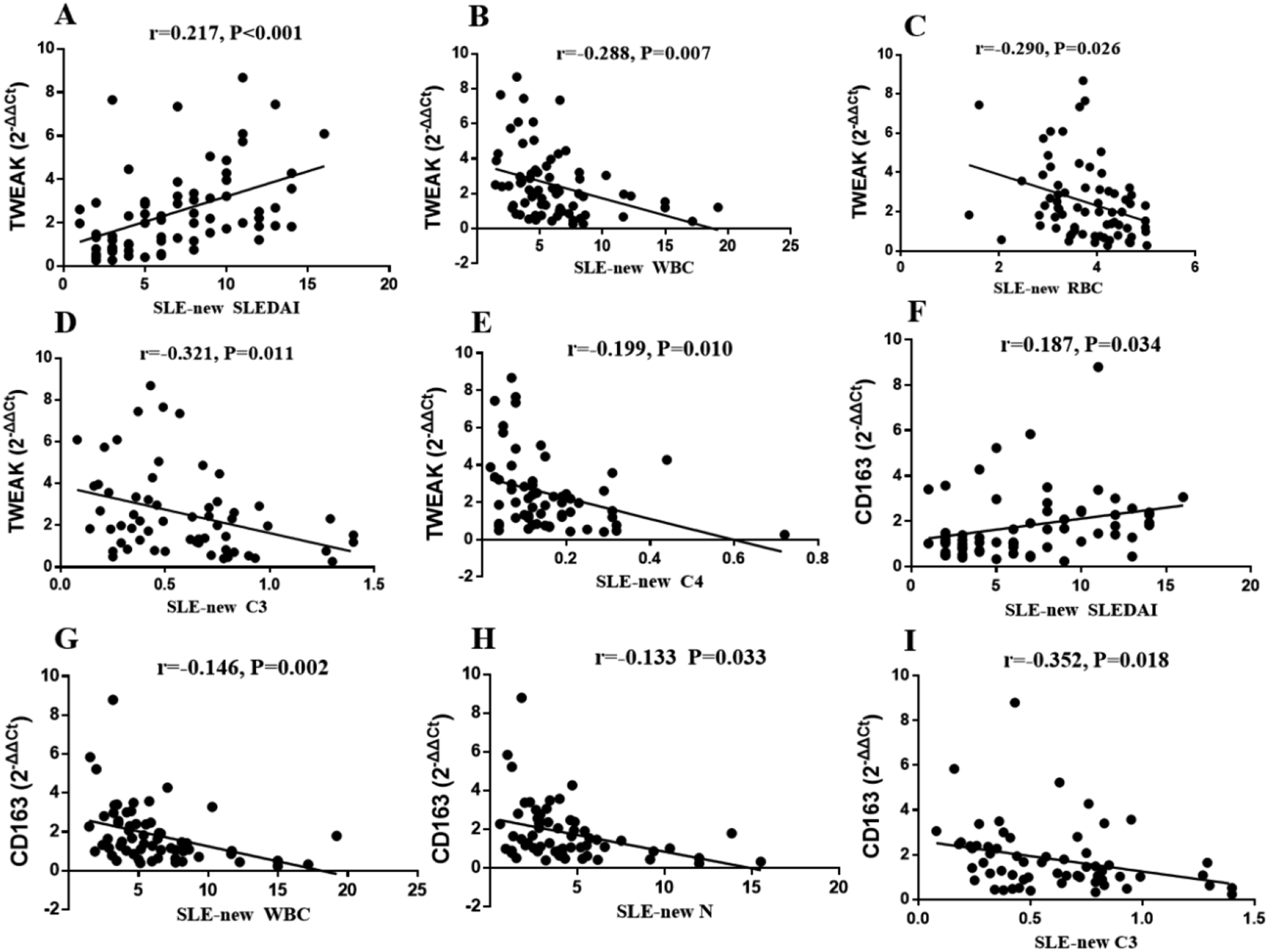
The TWEAK expression level in SLE+RI monocytes was positively correlated with the SLEDAI (rs = 0.245, p = 0.003; Figure 3(a)) and negatively correlated with the RBC (rs = −0.253, p = 0.014; Figure 3(b)), PLT (rs = −0.223, p = 0.004 Figure 3(c)), and C3 level (rs = −0.133, p = 0.031 Figure 3(d)). CD163 expression in SLE+RI monocytes was negatively correlated with the WBC (rs = −0.247, p = 0.042; Figure 3(e)), PLT (rs = −0.252, p = 0.015; Figure 3(f)), M level (rs = −0.288, p = 0.012; Figure 3(g)), and C3 level (rs = −0.246, p = 0.021; Figure 3(h)). In addition, we also found a positive correlation between TWEAK and CD163 expression in monocytes from SLE+RI patients (Figure 3(i)). (a-d) Correlation between TWEAK expression level and clinical features in monocytes from peripheral blood of newly diagnosed SLE+RI patients; (e-h) Correlation between CD163 expression level and clinical features in monocytes from peripheral blood of newly diagnosed SLE+RI patients; (i): Correlation between TWEAK and CD163 expression level in monocytes from peripheral blood of newly diagnosed SLE+RI patients. C3: Complement 3; C4: Complement 4; N: Neutrophil count; M: Moncyte count; PLT: Platelet count; RBC: Red blood cell count; SLEDAI: SLE disease activity index; WBC: White blood cell count.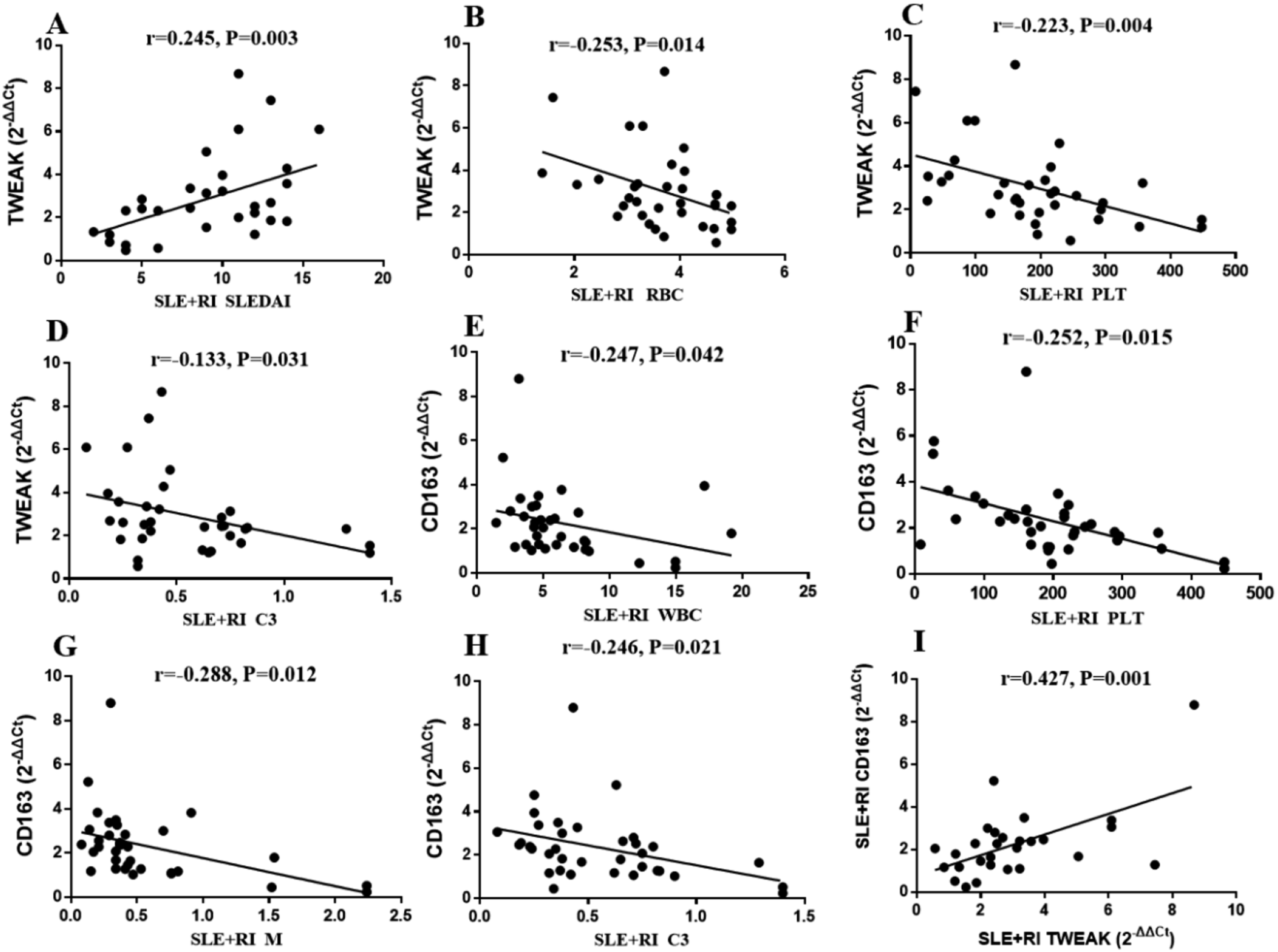
The diagnostic value of TWEAK and CD163 expression in monocytes for SLE and SLE+RI
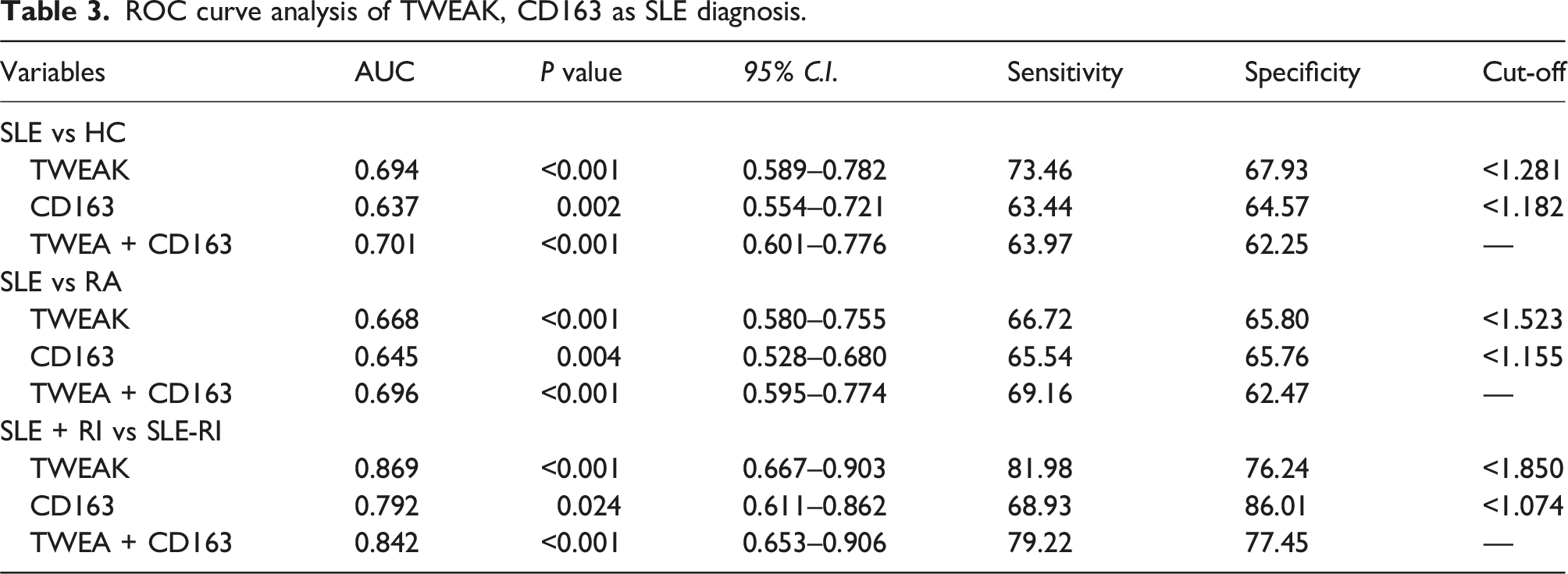
ROC curve analysis revealed that the AUCs of TWEAK expression in distinguishing patients with SLE from HCs and those with RA were 0.694 and 0.668, respectively. The AUC of TWEAK expression in distinguishing the SLE+RI group from the SLE-RI group was 0.869. A risk score based on CD163 was subsequently analysed in newly diagnosed SLE patients and individuals in the HC and RA groups. The results revealed that the areas under the curve (AUCs) for the risk score for distinguishing CD163-positive patients from HCs and patients in the RA group were 0.637 and 0.645, respectively. The AUC of CD163 expression in the SLE+RI group was 0.792. Furthermore, the AUCs for the risk score of the combination of TWEAK and CD163 in SLE patients from the HC group and the RA group were 0.701 and 0.696, respectively. The combined expression of TWEAK and CD163 had an AUC of 0.842 for distinguishing the SLE+RI group from the SLE-RI group (Figure 4(a)–(c)). The 95% confidence intervals, sensitivity, specificity, and cut-off value information are shown in Table 3. (a, b) ROC curves of TWEAK and CD163 in peripheral blood monocytes for diagnosis of SLE; (c) ROC curves of TWEAK and CD163 in peripheral blood monocytes for diagnosis of SLE+RI. SLE-new: newly diagnosed patients with systemic lupus erythematosus; SLE+RI: SLE patients with renal involvement; SLE-RI: SLE patients without renal damage; HC: healthy control. ROC curve analysis of TWEAK, CD163 as SLE diagnosis.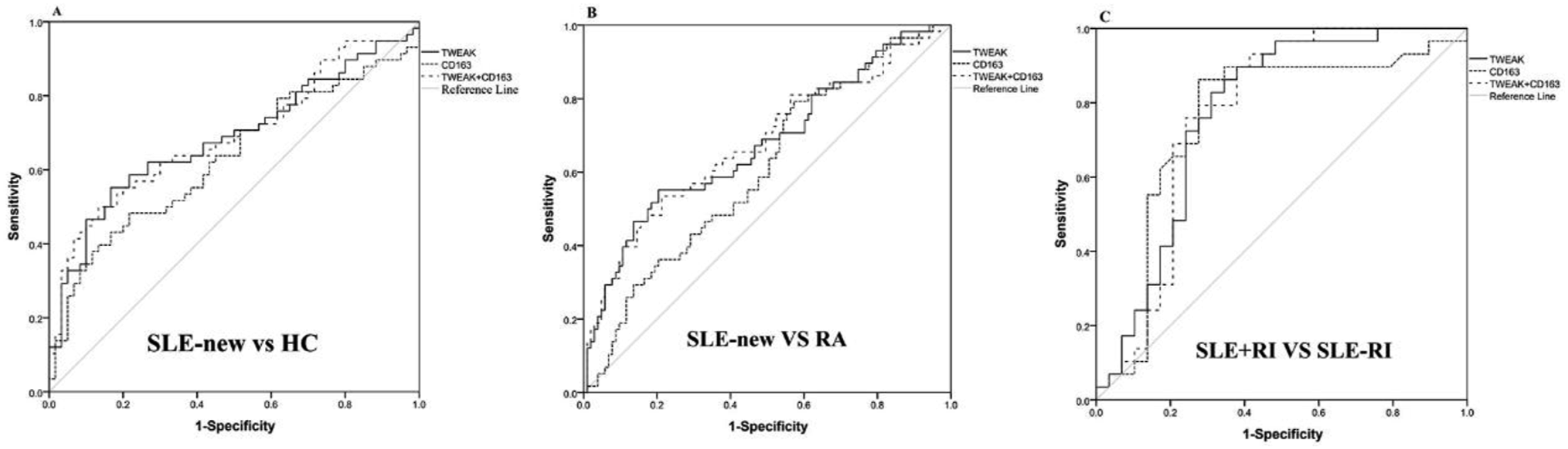
Protein expression of TWEAK and CD163 in SLE+RI monocytes
Our results revealed that the TWEAK protein in monocytes from the peripheral blood of SLE patients was significantly upregulated compared with that in monocytes from patients from the RA group and the HC group. The TWEAK protein level in monocytes from patients with SLE+RI was significantly greater than that in monocytes from patients with SLE-RI. Moreover, CD163 protein expression in these patients’ monocytes exhibited the same trend as TWEAK did (Figure 5). (a) The protein expression of TWEAK in each group; (b) The protein expression of CD163 in each group. SLE+RI: SLE patients with renal involvement; SLE-RI: SLE patients without renal involvement; RA: rheumatoid arthritis; HC: healthy control.
Discussion
Early disease identification and accurate monitoring remain significant clinical challenges in SLE management. As disease progression is often irreversible, timely therapeutic intervention becomes crucial for slowing disease progression and improving patient outcomes. 16 Therefore, an increasing number of researchers have focused on the study of disease markers in recent years. Disease markers, such as proteins, autoantibodies, genes, and small molecules or intermediates of metabolism, are well known, and most of these markers are related to the course and efficacy of SLE and can be used for its diagnosis and monitoring. 17
TWEAK, a new member of the TNF ligand superfamily, can be expressed in a variety of human tissues and cells, and its expression is significantly increased in tissues associated with acute and chronic inflammation and injury. An interesting study published in 2021 indicated that blocking TWEAK expression can significantly reduce the production of inflammatory factors and proteinuria in the kidney tissue of LN model mice and can alleviate pathological damage. 18 CD63 is a transmembrane glycoprotein that exists only on the cell membrane of mononuclear macrophages; it is involved in various immune activities in the body and is also associated with the occurrence of various autoimmune diseases. 19 An increasing body of evidence indicates that the level of soluble CD163 is elevated in patients with chronic inflammatory diseases such as acute kidney injury, autoimmune encephalomyelitis, and lupus nephritis.20–22 Moreover, CD163 has been shown to be the second scavenger receptor of TWEAK. Although the exact effect of the TWEAK/Fn14/CD163 axis on disease development has not been fully elucidated, increasing evidence indicates that the TWEAK/Fn14/CD163 axis is involved in the autoinflammatory pathological processes of various tissues and cells. However, the expression of TWEAK and CD163 in the monocytes of patients with lupus nephritis is still controversial. In this study, the expression levels of TWEAK and CD163 in monocytes from patients with SLE+RI were first investigated for their clinical significance and value in the diagnosis of SLE+RI, at the same time providing a reference for the potential interaction of TWEAK and CD163 in the occurrence and development of SLE+RI.
In this study, we found that the expression levels of TWEAK and CD163 were greater in monocytes from SLE patients than in those from RA patients, and their expression levels in the SLE+RI group were also significantly greater than those in the SLE-RI group, indicating that these two targets could not only distinguish SLE patients from HCs and RA patients but also distinguish SLE+RI patients from SLE-RI patients. These findings suggest that TWEAK and CD163 may be potential markers of SLE+RI and may be involved in the occurrence and development of SLE+RI. In addition, our results showed that the expression levels of TWEAK and CD163 in newly diagnosed SLE+RI patients were significantly reduced after effective treatment, which also indicates that these two targets may be used as prognostic indicators to evaluate their therapeutic effect in SLE+RI patients. Evidence from multiple teams also supports the hypothesis that blocking the TWEAK/Fn14 pathway is an attractive new treatment for a variety of human autoimmune/chronic inflammatory diseases, including lupus, RA, and multiple sclerosis. 23
Furthermore, we found that the expression levels of TWEAK and CD163 in patients with SLE+RI were associated with C3 and C4 levels; WBC, PLT, SLEDAI, and treatment response, which reflects disease activity and severity. Notably, their expression is correlated with the content of anti-dsDNA, which is also a commonly used diagnostic index for monitoring the disease activity of SLE+RI. These results indicate that the expression levels of TWEAK and CD163 are increased in monocytes from peripheral blood of patients with SLE + RI and may be used as novel biomarkers for new-onset SLE+RI diagnosis and prognosis evaluation.
In addition, ROC curves were used to analyse the diagnostic value of TWEAK expression in this study. The AUC of TWEAK expression between the SLE+RI and SLE-RI groups was 0.869, and the sensitivity and specificity were 81.98% and 76.24%, respectively. The combination model of TWEAK and CD163 had an AUC of 0.842, a sensitivity of 79.22% and a specificity of 77.45% between the SLE+RI and SLE-RI groups. All the above results showed that the expression levels of TWEAK and CD163 in monocytes from peripheral blood of patients with SLE+RI were closely related to the activity and severity of SLE+RI, which could be used not only as indicators for the diagnosis and differential diagnosis of SLE and SLE+RI but also as indicators for evaluating the severity of SLE SLE+RI. Finally, we found that TWEAK and CD163 protein expression in monocytes from patients with SLE+RI was significantly increased, which was consistent with the RNA expression results. Additionally, TWEAK and CD163 expression in the monocytes of SLE+RI patients was positively correlated. Although CD163/TWEAK has been found to play a crucial role in the development of atherosclerosis, whether these two factors are involved in the occurrence and development of renal involvement in SLE is still unknown. 24 Understanding this relationship will improve the potential of CD163/TWEAK as a disease marker and will help provide many clues for the development of SLE+RI treatments in the future. At present, most studies are limited to the expression of soluble TWEAK and CD163 in blood samples and urine samples,25,26 and no comprehensive analysis has been conducted on the correlation between the gene expression levels and disease activity in monocytes and various clinical indicators or on the combination of these two target molecules. This study provides reference values for this purpose.
Notably, this study has several limitations. The number of SLE patients was small, and the sample size of SLE patients should be expanded in the future, especially the sample size of patients with SLE+RI.
Conclusions
In conclusion, the expression of TWEAK and CD163 was significantly increased in peripheral blood monocytes of SLE patients and SLE+RI patients and was also closely related to disease activity, haematological involvement and renal involvement severity; thus, TWEAK and CD163 can be used as potential diagnostic and differential diagnostic markers for SLE and SLE+RI. As research progresses, further investigations into the TWEAK–CD163 interaction may elucidate its precise role in the pathogenesis of SLE-related renal damage, potentially revealing novel therapeutic targets.
Footnotes
Acknowledgements
We would like to acknowledge the help from Dr Rui Wu at department of rheumatology, the First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, China.
Author contributions
Lu Zhang was mainly responsible for the project design and experimental data analysis; Lulu Zeng played a guiding role in writing and researching; Tingting Zeng mainly took charge of data processing; Qianbin Dai mainly took charge of collecting blood samples; Yao Zhou was mainly responsible for collecting clinical data; Qing Luo played a guiding role in project guidance and providing financial support; Junming Li also played a guiding role in project guidance and providing financial support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Plan Project of the Education Department of Jiangxi Province (GJJ200107), the Science and Technology Plan Project of the Education Department of Jiangxi Province (GJJ2200210), and the Health Commission Research Project of Jiangxi Province of China (202310455).
Ethical statement
Data Availability Statement
Additional data are made available in supplementary tables of this manuscript; we will supply the relevant data in response to reasonable requests.