
Abstract
Objective
Cervical cancer remains a leading cause of death among women of childbearing age despite the proven efficacy of screening in reducing mortality rates. Women with systemic lupus erythematosus (SLE) are at a higher risk for cervical cancer but tend to have lower screening rates. This study aimed to assess cervical cancer screening (CCS) rates and identify factors influencing screening uptake among Korean women of childbearing age with SLE.
Methods
Women aged 20-49 with SLE and age matched controls, randomly selected at a 1:5 ratio, were identified from the 2016-2017 Korean National Health Insurance Service-National Health Information Database (NHIS-NHID). Data from 10,981 women with SLE and 54,905 controls eligible for National Health Screening Program (NHSP) in 2018-2019 were analyzed. The CCS rate was determined based on participation in Papanicolaou test among eligible individuals for NHSP. Logistic regression was used to estimate odds ratios (ORs) for factors associated with CCS uptake.
Results
The CCS rate was significantly lower in women with SLE compared to controls (49.6% vs 52.1%, P < .0001). Logistic regression revealed that younger age, lower income, self-employment or medical aid insurance, and rural residence were associated with reduced CCS uptake in both groups. The highest CCS uptake occurred in the 40-44 age group for both women with SLE (OR 5.09, 95% CI 4.17-6.22) and controls (OR 4.65, 95% CI 4.26-5.07). Comorbidities increased CCS uptake among controls (OR 1.18, 95% CI 1.13-1.23), but were associated with mild non-significant decrease in uptake among women with SLE (OR 0.96, 95% CI 0.87-1.04).
Conclusion
National CCS program is often underutilized by Korean women of childbearing age with SLE, particularly among those with lower income and those of rural residency. Targeted interventions are needed to improve screening rates and address the unique challenges faced by this high-risk population.
Introduction
Cervical cancer is a leading cause of death among women of childbearing age worldwide, despite being preventable through regular screening and early detection. In 2020, the World Health Organization (WHO) reported 604,127 new cervical cancer cases and 341,831 related deaths globally, with the greatest burden in low- and middle-income countries. 1 The Papanicolaou (Pap) test has been instrumental in reducing cervical cancer incidence and mortality in high-income countries, especially when integrated into nationwide screening programs.2,3 However, significant disparities persist in screening participation, particularly among lower socioeconomic groups and ethnic minorities.4–7
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease characterized by systemic inflammation and immune dysregulation, predominantly affecting women of reproductive age.8,9 Studies show that women with SLE face a significantly higher risk of developing cervical cancer.10,11 primarily due to immune dysfunction caused by the disease and long-term use of immunosuppressive therapies such as corticosteroids and cyclophosphamide.12,13 Routine cervical cancer screening (CCS) is critical for early detection in this high-risk group. However, despite their vulnerability, women with SLE report suboptimal CCS.14–19 Previous studies on this topic have been limited by small sample sizes, single-institution data, or survey-based approaches, leaving gaps in understanding screening behaviors within this population. There is limited research on CCS rates among women of childbearing age with SLE, a group more likely to receive immunosuppressive therapy due to increased disease activity during this time.20–22
This study aimed to evaluate CCS rates via Pap test among Korean women of childbearing age with SLE using a nationwide health information database. It also sought to identify sociodemographic, clinical, and healthcare-related factors influencing CCS uptake, comparing these findings to age-matched controls.
Methods
Study design and data source
A cross-sectional study was conducted using data from the Korean National Health Insurance Service-National Health Information Database (NHIS-NHID) between 2016 and 2019. The Korean NHIS, a single-payer system, provides health coverage to nearly the entire population of Korea. The NHIS-NHID comprises five key databases: eligibility, national health screening, healthcare utilization, long-term care insurance, and healthcare provider information. These databases include details on income-based insurance contributions, residential areas, national health screenings, inpatient and outpatient care (diagnoses and treatments), claims data, and healthcare providers.
Since 2008, the NHIS has offered biennial general health screenings for all adults aged 20 and older through National Health Screening Program (NHSP). As part of this initiative, the National Cancer Screening Program (NCSP) has provided free CCS via Pap test to women aged 20 and above since 2016. Eligibility for these screenings is determined by the National Health Insurance Corporation (NHIC), which directly notifies eligible individuals. Screenings are conducted at NHIC-designated medical institutions, and the results are submitted to the NHIS. For this study, data from January 1, 2016, to December 31, 2019, were analyzed to avoid potential biases in health screening rates caused by the COVID-19 pandemic.
Study population
Prevalent cases of women aged 20-49 with SLE were identified using the NHIS-NHID data from 2016 to 2017. To serve as a control group, age-matched women without rheumatic diseases (RD) were randomly selected from the same database at a 1:5 ratio. RD was defined as including SLE, seropositive rheumatoid arthritis (SPRA), and ankylosing spondylitis (AS), which are common among women of childbearing age. SLE, SPRA, and AS were identified with the diagnostic codes M05, M32, and M45, respectively, based on the ICD-10 codes. Individuals eligible for NHSP during 2018-2019 were identified from the NHIS-National Health Screening Database.
Outcome measures
The primary outcome was the Pap test rate. The Pap test rate was calculated as the number of individuals with Pap test results divided by the total number of eligible subjects for NHSP. Variables such as age, income, medical insurance type, residential district, and comorbidities were obtained from the 2018 NHIS-NHID database. Comorbidities, including hypertension (HT), diabetes mellitus (DM), hyperlipidemia (HLD), and cancer, were identified using ICD-10 codes: I10-I12/I15 for HT, E10-E14 for DM, E78 for HLD, and C* for cancer.
Statistical analysis
A descriptive analysis summarized the characteristics of the study population. Categorical variables were presented as frequencies and percentages, while continuous variables were reported as means with standard deviations (SD). Unadjusted and multiple logistic regression analyses estimated odds ratios (ORs) for factors associated with CCS. Statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA), with P-values <.05 considered statistically significant.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of the National Health Insurance Service Ilsan Hospital, South Korea (NHIMC 2024-01-017), and conducted according to the principles of the Declaration of Helsinki. Since the database used in this study contains anonymized data for research purposes, informed consent was not required.
Results
Characteristics of the study population
Baseline characteristics of the study population.
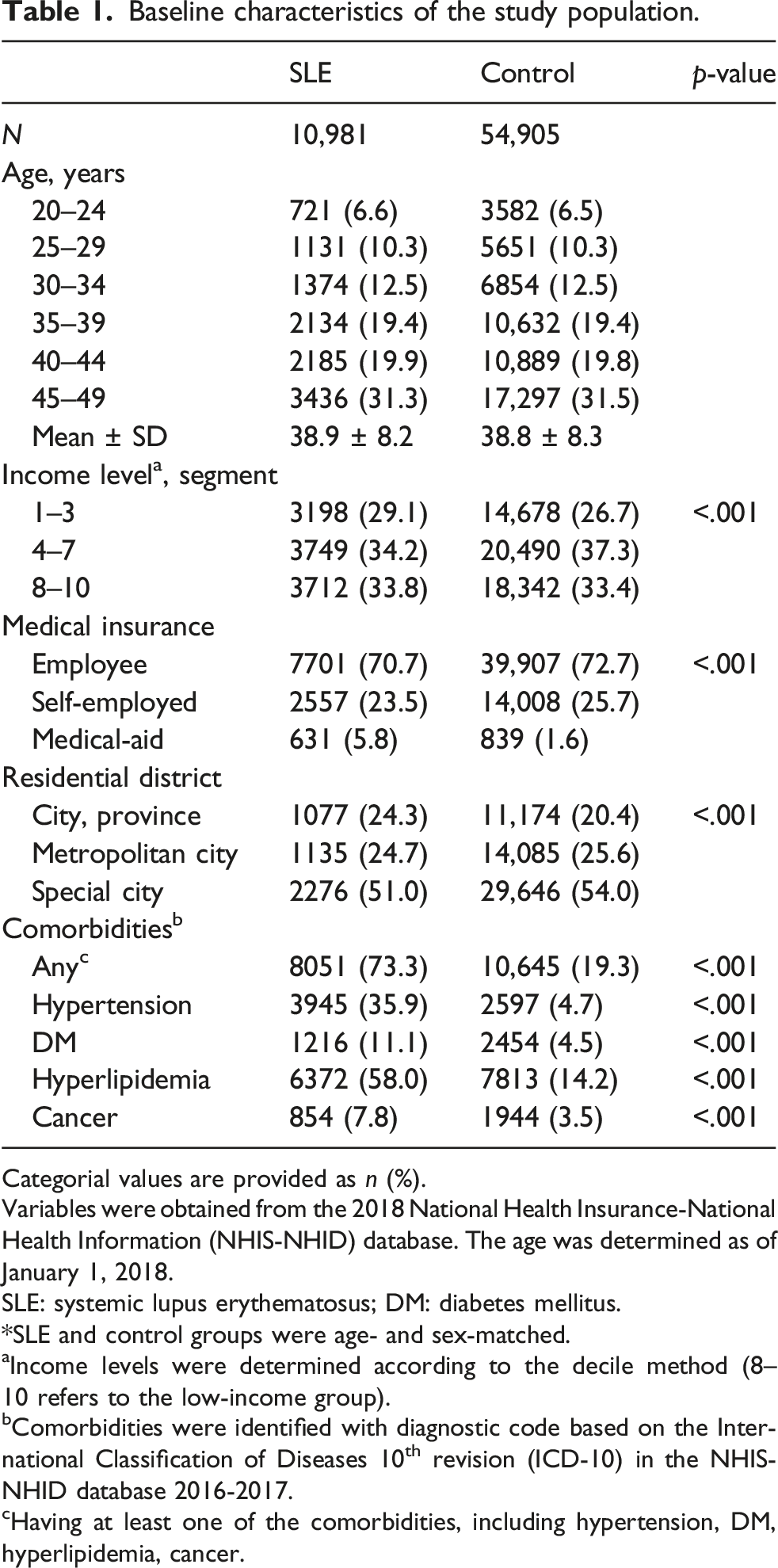
Categorial values are provided as n (%).
Variables were obtained from the 2018 National Health Insurance-National Health Information (NHIS-NHID) database. The age was determined as of January 1, 2018.
SLE: systemic lupus erythematosus; DM: diabetes mellitus.
*SLE and control groups were age- and sex-matched.
aIncome levels were determined according to the decile method (8–10 refers to the low-income group).
bComorbidities were identified with diagnostic code based on the International Classification of Diseases 10th revision (ICD-10) in the NHIS-NHID database 2016-2017.
cHaving at least one of the comorbidities, including hypertension, DM, hyperlipidemia, cancer.
Cervical cancer screening rates
CCS rate was significantly lower in women with SLE than in the controls (49.6% vs 52.1%, P < .0001). Although the Pap test was included in the NHSP, its uptake was significantly lower compared to overall health screening rates in both the SLE group and the controls (Figure 1). National Health Insurance (NHIS) health screening and cervical cancer screening participation rates (2018–2019) among women of childbearing age with SLE compared to controls. *p value <.0001. SLE: systemic lupus erythematosus; Pap: Papanicolaou.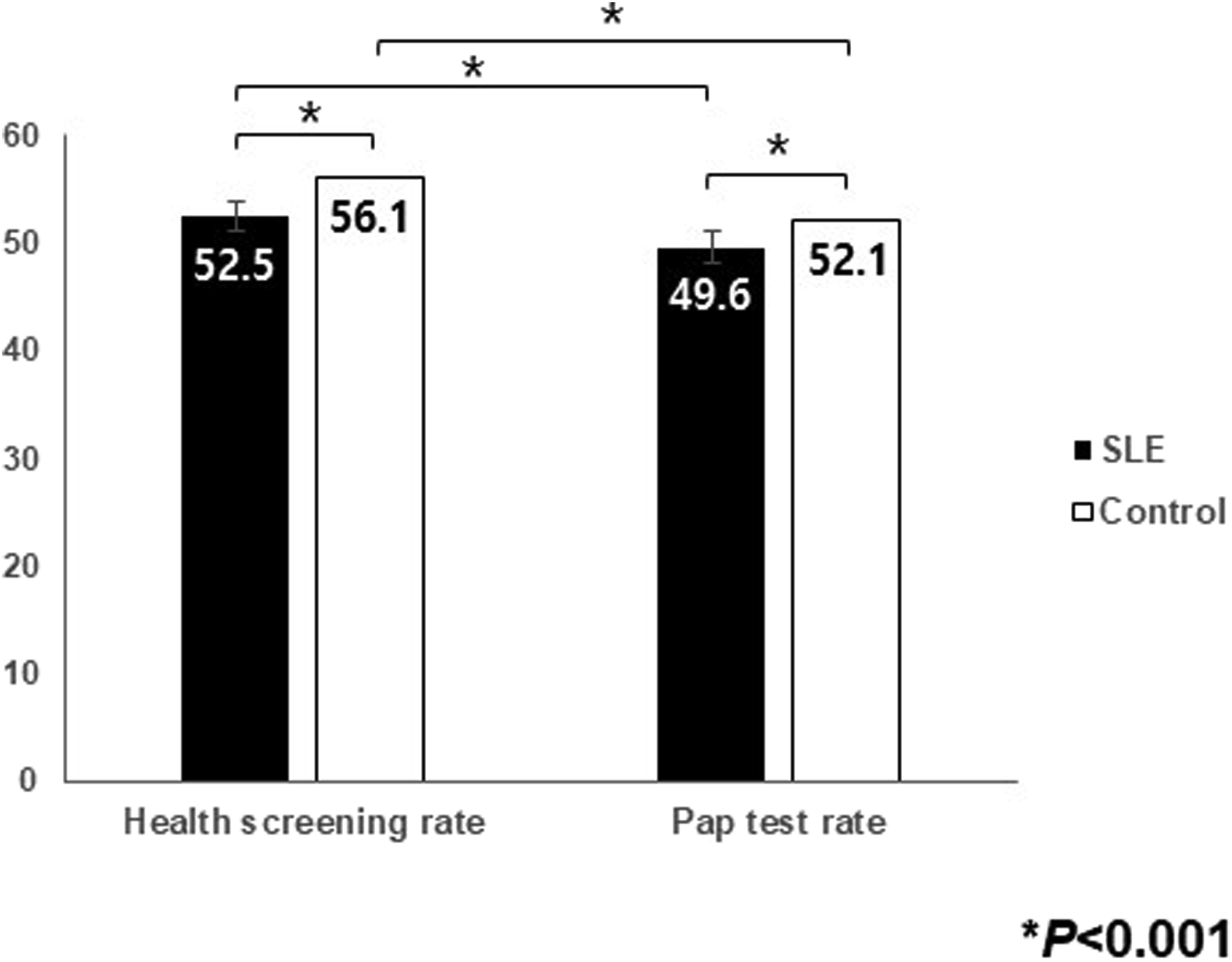
Factors associated with cervical cancer screening uptake
Differences in baseline characteristics based on cervical cancer screening uptake.
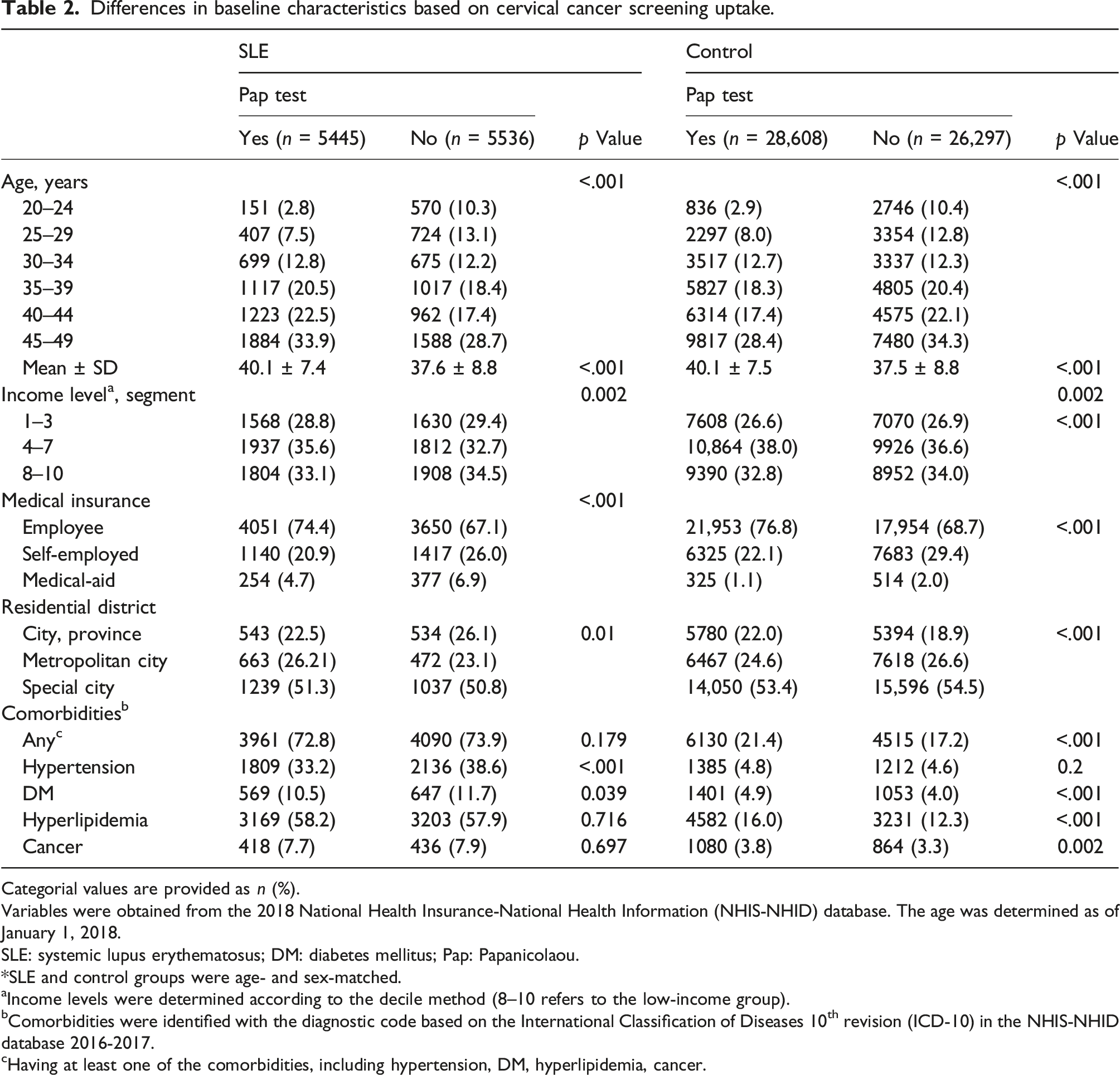
Categorial values are provided as n (%).
Variables were obtained from the 2018 National Health Insurance-National Health Information (NHIS-NHID) database. The age was determined as of January 1, 2018.
SLE: systemic lupus erythematosus; DM: diabetes mellitus; Pap: Papanicolaou.
*SLE and control groups were age- and sex-matched.
aIncome levels were determined according to the decile method (8–10 refers to the low-income group).
bComorbidities were identified with the diagnostic code based on the International Classification of Diseases 10th revision (ICD-10) in the NHIS-NHID database 2016-2017.
cHaving at least one of the comorbidities, including hypertension, DM, hyperlipidemia, cancer.
Logistic regression analysis revealed that younger age, lower income, self-employment or medical-aid insurance, and rural residence were linked to a reduced likelihood of CCS uptake in both the SLE and control groups. The highest OR for CCS uptake was observed in the 40-44 age group for women with SLE (OR 5.09, 95% CI 4.17-6.22) and the controls (OR 4.65, 95% CI 4.26-5.07). In the control group, comorbidities increased the likelihood of CCS uptake (OR 1.18, 95% CI 1.13-1.23). Conversely, in the SLE group, comorbidities were associated with a decreased likelihood of Pap test participation, though the result was not statistically significant (OR 0.96, 95% CI 0.87-1.04) (Figure 2). Factors associated with National Health Insurance (NHIS) cervical cancer screening uptake (2018–2019) among women of childbearing age with SLE compared to controls. OR: odds ratio; CI: confidence interval.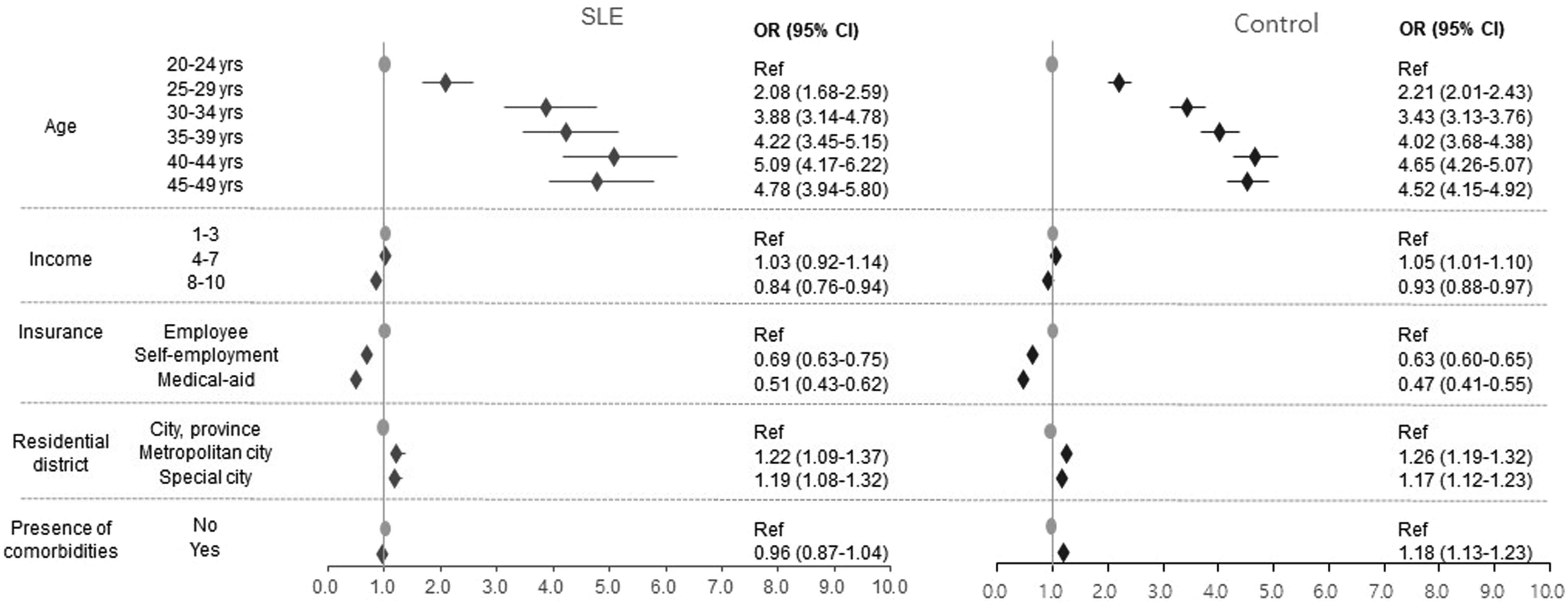
Discussion
This study is first to evaluate CCS rates and factors influencing CCS uptake in Korean women of childbearing age with SLE compared to age-matched controls based on the Korean NCSP protocol for the general population. Our findings revealed that CCS rates were significantly lower in women with SLE than in their age-matched controls, especially in those with lower income and those residing in rural areas. While the presence of comorbidities was associated with increased screening uptake in the control group, it did not affect participation in the SLE group, despite their higher burden ofcomorbidities.
In Korea, the NCSP offers free Pap tests every 2 years for women aged 20 and older as a part of NHSP. However, despite this universal program, the CCS rate among eligible women was only 56.0% in 2020. 23 This study found that the screening rate for women of childbearing age without RD was 52.1%, lower than the overall rate for women aged 20 and older. Among women with SLE, the screening rate was even lower at 49.6%, significantly below that of age-matched women without RD. Low screening rates may lead to missed opportunities for early detection and increased cervical cancer mortality. These findings align with previous studies from other countries, which consistently indicate suboptimal CCS participation rates among women with SLE.14,15,19 Research from the United States reported that CCS rates among women with SLE were comparable to or higher than the general population.18,24 However, despite the higher prevalence of abnormal cervical pathology in women with SLE, approximately one-quarter had not undergone CCS within 3 years of diagnosis. 18 Adherence to CCS was reported at 61.5%, 25 and only 38% followed SLE-specific guidelines established by the American Society for Colposcopy and Cervical Pathology guidelines. 17 Similarly, a survey in Japan found that while CCS rates were slightly higher than the general population, 23% of patients had been screened. 16 Single-center studies from Canada, France, and Brazil also reported lower screening rates and reduced adherence to CCS guidelines among women with SLE.14,15,19
Demographic factors such as low socioeconomic status, rural residence, limited education, unmarried status, and ethnic minority background are associated with reduced CCS uptake in the general population.12,23,26,27 Health-related behavioral factors, including obesity, smoking, inadequate sleep, alcohol use, and low physical activity, have also been linked to lower participation in CCS.28,29 This study identified similar demographic factors associated with lower CCS uptake in women of childbearing age with SLE, consistent with patterns observed in the general population. These factors included younger age, lower income, self-employment or medical-aid insurance types, and rural residence. Notably, a greater proportion of women of childbearing age with SLE were represented in the lower-income, self-employment or medical-aid insurance coverage, and rural residence groups, indicating that these factors may exert a greater influence on reduced CCS uptake in this population. Previous studies examining factors affecting CCS uptake among socioeconomically vulnerable populations in Korea have found that individulas with low income often demonstrate a lower intention to participate in screening, primarily due to limited awareness of the importance of health checkups. Additionally, their socioeconomic circumstances may lead them to place less priority on personal health management.30,31 Although Pap tests are provided free of charge under the NCSP, they are only available at NHIC-designated facilities equipped to perform the test, requiring patients to visit these specific sites. In rural areas, limited access to such facilities may partially explain the lower screening rates observed in this group. In this study, comorbidities such as HT, HLD, DM, and cancer were associated with higher CCS rates in the general population; however, they did not impact screening uptake among women with SLE, despite the greater burden of comorbidities in this group. 32 This aligns with previous studies indicating that women with SLE, especially those with comorbidities or high disease activity, are less likely to undergo cancer screening.14,18,25 This may reflect a tendency to prioritize the management of their disease over engagement in preventive healthcare services.
The main strength of this study is that it is the first nationwide study to assess CCS rates among women of childbearing age with SLE. By using a nationally representative dataset, this study addresses the limitations of prior research, which relied on small sample sizes. The NHIS-NHID includes health information for most of the Korean population, enabling a comprehensive analysis of factors influencing cervical cancer screening uptake. However, this study has limitations. As a cross-sectional study, it does not provide data on long-term adherence to CCS guidelines. Moreover, certain health-related behaviors and disease-specific factors, such as SLE disease activity, disease-related damage, and immunosuppressive drug use, could not be evaluated as these variables are not included in the NHIS-NHID dataset.
Women with SLE face a higher risk of human papillomavirus (HPV)-associated high-grade cervical cytology, as well as cervical, vaginal, and vulvar cancers compared to the general population.10,33–35 According to recent expert recommendations on CCS for immunosuppressed women without human immunodeficiency virus (HIV) suggest that all women with SLE—regardless of immunosuppressive use—should follow screening recommendations for HIV-infected women. 36 According to the US Centers for Disease Control and Prevention, women with HIV should undergo 2 Pap tests during the first year after diagnosis, followed by annual screenings throughout their lifetime. 37 In Korea, CCS using cytology is recommended every 3 years for women aged 20 to 74. 38 However, there are no specific national guidelines addressing CCS in immunocompromised women. Even in countries with national guidelines for CCS in immunosuppressed women, adherence remains lower than expected. 25 Although Korea’s National Immunization Program provides HPV vaccination free of charge to 12 year old girls, there is currently no public reimbursement for adult women or immunocompromised patients, including those receiving immunosuppressive therapy. 39 This policy gap may further increase cervical cancer risk in this vulnerable population. Given that cervical cancer is highly preventable through regular screening and timely vaccination, targeted strategies are in need to improve CCS and prevention efforts in this high-risk population.
In conclusion, Korean women of childbearing age with SLE face a higher risk of cervical pre-cancer and cancer but remain underscreened for cancer prevention, particular among those with lower income and those of rural residency. Despite their significant burden of comorbidities, these factors did not influence CCS uptake among women of childbearing with SLE. To address this disparity, efforts should be made to enhance awarebess of CCS, particularly among socioeconomically disadvantaged populations, and to improve acess to healthcare services in rural areas. Furthermore, there is an urgent need to develop national cervical cancer screening guidelines for immunosuppressed patients, including those with SLE in order to ensure standardized preventive care. These findings highlight the need for targeted screening programs to improve cervical cancer prevention in women with SLE. Such initiatives could enhance understanding of cancer prevention disparities and improve care for this vulnerable population.
Footnotes
Author contributions
Conceptualization: Lee J. Data curation: Lim H. Formal analysis: Lim H. Investigation: Park JS & Lee J. Methodology: Park JS & Lee J. Writing - original draft: Lee J. Writing - review & editing: Baek IW & Chung MK & Park PG & Lee CH & Park JS.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Health Insurance Ilsan Hospital, South Korea (NHIMC-2023-PR-002). This study used data from the Korean NHIS-NHID database, created by the NHIS (NHIS-2024-11-1-030).