
Abstract
Objectives
The main challenge in the care of patients with primary antiphospholipid syndrome (APS) or associated to systemic lupus erythematosus (SLE) is to determine whether patients will experience new events that may impair their clinical outcome. Triggering receptor expressed on myeloid cells-1 (TREM-1) is an amplifier of the Toll like receptor (TLR4) pathway, which is involved in APS. Plasma soluble TREM-1 (sTREM-1) levels indicate increased receptor activation and were significantly greater in thrombotic primary APS patients compared to controls. This prospective cohort study investigated the predictive value of plasma sTREM-1 levels at inclusion for the occurrence of thrombotic events or death in patients with APS, antiphospholipid antibodies (aPLs) and/or SLE.
Methods
Serum sTREM-1 levels were measured at inclusion in 108 patients with APS, isolated aPL or SLE followed during 46 months. The primary outcomes included thrombosis, death and obstetrical morbidity. The occurrence of the first event of interest and predictors were modeled in a multivariable Cox model.
Results
During follow-up, 15 of the 108 patients presented with thromboses (14%), 5 patients died (5%), and 3 women experienced obstetrical morbidities (3%). Elevated serum sTREM-1 levels were an independent predictor for the occurrence of the composite outcome (HR 7.54 [95% CI; 2.44-23.31] p < .001). In addition, sTREM-1 levels were greater in patients with APS than patients with isolated aPL (p < .01).
Conclusion
High levels of sTREM-1 at inclusion predicted the occurrence of a thrombotic and obstetric event or death in patients with aPL and/or SLE. Therefore, sTREM-1 represents a potential new prognostic biomarker in these patients.
Keywords
Introduction
Antiphospholipid syndrome (APS) is an autoimmune disease that is characterized by recurrent thrombosis events (arterial, venous and/or small vessels) and/or obstetrical morbidity (early or late fetal losses, premature births) and persistent positivity of at least one antiphospholipid (aPL) test: the lupus anticoagulant (LA), and/or IgG/IgM anticardiolipin (aCL), and/or IgG/IgM anti-β2-glycoprotein-I (aβ2GPI). 1 APS can be primary or associated with an autoimmune disease like systemic lupus erythematosus (SLE). In this study, we aimed to evaluate whether baseline plasma sTREM-1 levels could predict the occurrence of thrombotic events, obstetric complications, or death as outcomes observed in the context of aPL positivity. Therefore, a prognostic biomarker may be useful. Innate immunity plays a key role in APS thrombosis via leukocytes and myeloid or Toll-like receptors (TLRs).2–4 β2-Glycoprotein-I (β2GPI) is involved in lipopolysaccharide (LPS) neutralization by monocytes due to its scavenger function. Binding of LPS to β2GPI via domain V induces a conformational change that exposes a cryptic epitope in domain I that is recognized by aPL. 5 β2GPI interacts with TLR4 via LPS and contributes to aPL-mediated endothelial cell activation. 4 These results support the role of β2GPI as a component of innate immunity, and TLR4 activation may play a role as a “second hit” mechanism.
Triggering receptor expressed on myeloid cells 1 (TREM-1) is a cell surface receptor that belongs to an immunoglobulin variable domain superfamily of proteins. This receptor has been identified on human neutrophils, mature monocytes, platelets and endothelial cells. 6 TREM-1 activates neutrophils and monocytes to favor neutrophil extracellular trap (NET) release and thrombin generation.7–9 It also activates endothelial cells and amplifies the production of proinflammatory cytokines via the TLR4 pathway. TREM-1 is involved in acute inflammation, such as sepsis, aseptic inflammation, such as rheumatoid arthritis and atherosclerosis, and coagulation via monocyte activation.7,10–13 Activation of the TREM-1 pathway cleaves the extracellular domain to create a soluble form (sTREM-1). STREM-1 levels correlate with innate immune activation and TREM-1 upregulation. 14 Plasma sTREM-1 levels are significantly greater in primary APS patients and thrombotic APS patients compared to controls. However, the clinical relevance of this finding is not known. 3 Moreover, sTREM-1 has been shown to predict short-term mortality in hospitalized patients with severe conditions, highlighting its prognostic relevance in immune-mediated diseases. 15
Therefore, the aim of study was to determine the predictive value of plasma sTREM-1 levels at inclusion for the occurrence of thrombotic events or death in patients with APS, antiphospholipid antibodies (aPLs) and/or SLE.
Materials and methods
Design and study population
The APLART (Anti-PhosphoLipides-rigidité ARTerielle) study is a prospective cohort study that included consecutive patients (prevalent cases at various stages of their disease) from the National Referral/Reference Center for Rare Vascular and Systemic Autoimmune Diseases at the Nancy University Hospital, France, which is a tertiary care referral center for the region “Grand Est”. All patients were routinely clinically followed from 2011 to 2019. The inclusion criteria were patients older than 18 years old with aPL in plasma on two or more occasions at least 12 weeks apart according to Sydney criteria or with another AID. 16 aPL patients with clinical criteria for APS, according to the Sapporo-Sydney criteria, were considered primary or secondary APS based on the presence of a SLE according to the EULAR classification. 17 The others were considered asymptomatic aPL patients.
The exclusion criteria were age <18 years, pregnancy, absence of written consent or inability to follow-up. The APLART study protocol was reviewed and approved by the IRB (Comite de Protection des Personnes – Est III - registration number 10.06.03), and patients provided written informed consent.
Definition of outcomes
The main outcome was a composite criterion of the occurrence of vascular thrombosis (arterial and/or venous and/or small vessels), an obstetrical event or death. The endpoint was the time to the event. Only the first event was analyzed. The definitions of thrombosis were previously reported. 18 We used the Sapporo criteria for the definition of obstetrical events. 16
Assays for sTREM-1
Peripheral blood samples were obtained at inclusion via venipuncture using a 21-gauge needle and collected in S-monovette tubes containing sodium citrate (3.2%) (Sarstedt). The plasma was centrifuged for 10 min at 2000×g and 20°C then stored at −80°C until use.
The plasma concentration of sTREM-1 at inclusion was determined using a commercial ELISA kit (Human TREM-1 Quantikine kit assay®, DTRM10 C, R&D System, MN, USA) following the manufacturer’s recommendations. Briefly, this assay used a 96-well plate coated with a specific human TREM-1 antibody. The absorbance was measured at 450 nm, and the sTREM-1 concentration was quantified using a standard calibration curve. All plasma samples and standards were assayed in duplicate, and the mean of both measurements was used. The results are expressed in pg/ml.
Clinical and immunological data
Baseline characteristics
At the inclusion visit, full medical history and physical examination data were recorded.
Baseline characteristics included demographics, past APS-related thrombosis and/or obstetrical morbidity according to the Sydney criteria and the presence of non-criteria APS manifestations, such as livedo, cardiac valve disease, APS- or SLE -related nephropathy, and thrombocytopenia. We also recorded the following routine biological signs of lupus activity: cytopenia, antinuclear antibodies, double-stranded DNA, and complement activity. The inclusion criteria included anthropomorphic measurements (height, weight) and data on classical cardiovascular risk factors (age, sex, smoking habits, diabetes, dyslipidemia, and hypertension). We recorded treatments at inclusion, including anticoagulant therapy, steroids or other immunosuppressive agents.
We determined arterial stiffness using pulse wave velocity (PWV) measured with a Pulse Pen® system at inclusion. 19 The cut-off values in the literature recommend 12 m.s−1 followed by 10 m.s-1.20,21 An equation that accounts for blood pressure and age was also proposed but did not lead to changes in the recommendations. Therefore, we used the same analysis used for sTREM-1 (see below) with a sensitivity analysis. 22
Follow-up data
Patients were followed every 6 months and at the time of any new event. We recorded all medical events during the follow-up, including thrombotic or obstetrical events, death, treatment and cardiovascular risk factors. When an event occurred, the presence of thrombotic risk factors (venous and arterial) was recorded.
Antiphospholipid positivity
The presence of aPL was defined as positivity for LA and/or aCL IgG/IgM and/or aβ2GPI IgG/IgM on a minimum of two consecutive occasions at least 12 weeks apart. ACL and aβ2GPI were identified using ELISA and considered positive at titers > the 99th percentile, as previously described. 23 LA was assessed according to the three-step guidelines of the Subcommittee on LA of the International Society on Thrombosis and Haemostasis (ISTH) using Partial Thromboplastin Time–Lupus Anticoagulant (PTT-LA) and diluted Russel’s Viper VenomTime (dRVVT) reagents. 24 For patients treated with VKA, procedures from international guidelines were followed according to the index normalized ratio value. 25
Statistical methods
Baseline characteristics, plasma s-TREM1 level and events during follow-up were described by percentages for categorical variables and means +/− standard deviation for continuous variables.
Comparisons were used Pearson’s chi-squared test (or Fisher’s exact test, as appropriate) and Student's t test, depending on the nature of the variables.
Predictors with the occurrence of an event were investigated using bivariable and multivariable Cox regression models where appropriate.
Variables whose p-value in bivariable analysis was <0.2 were candidates for multivariate analysis. Given the limited number of events (n = 23), the number of covariates included in the multivariate Cox models was restricted according to the events-per-variable (EPV) rule of thumb (approximately 10 events per variable). Variables were selected based on their significance in bivariable analysis and on clinical relevance. This strategy was used to reduce the risk of overfitting and model instability; however, results should be interpreted with caution and confirmed in larger cohorts.
We chose to evaluate predefined percentiles (50th, 75th, 90th, 95th) using bivariate Cox models because our primary aim was to identify thresholds with prognostic value in a time-to-event framework, which is not directly addressed by ROC curves. ROC analysis is more appropriate for binary outcomes at fixed time points, whereas our data involved varying follow-up durations. The use of Cox models preserved the temporal dimension of the data and accounted for censoring. The statistical significance threshold was set at 5%. Statistical analysis was performed using SAS® software version 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
A total of 108 patients were included between 2011 and 2014 and followed until 1st January 2019, with a median follow-up time of 54 months.
Baseline characteristics
Characteristics of patients at inclusion.
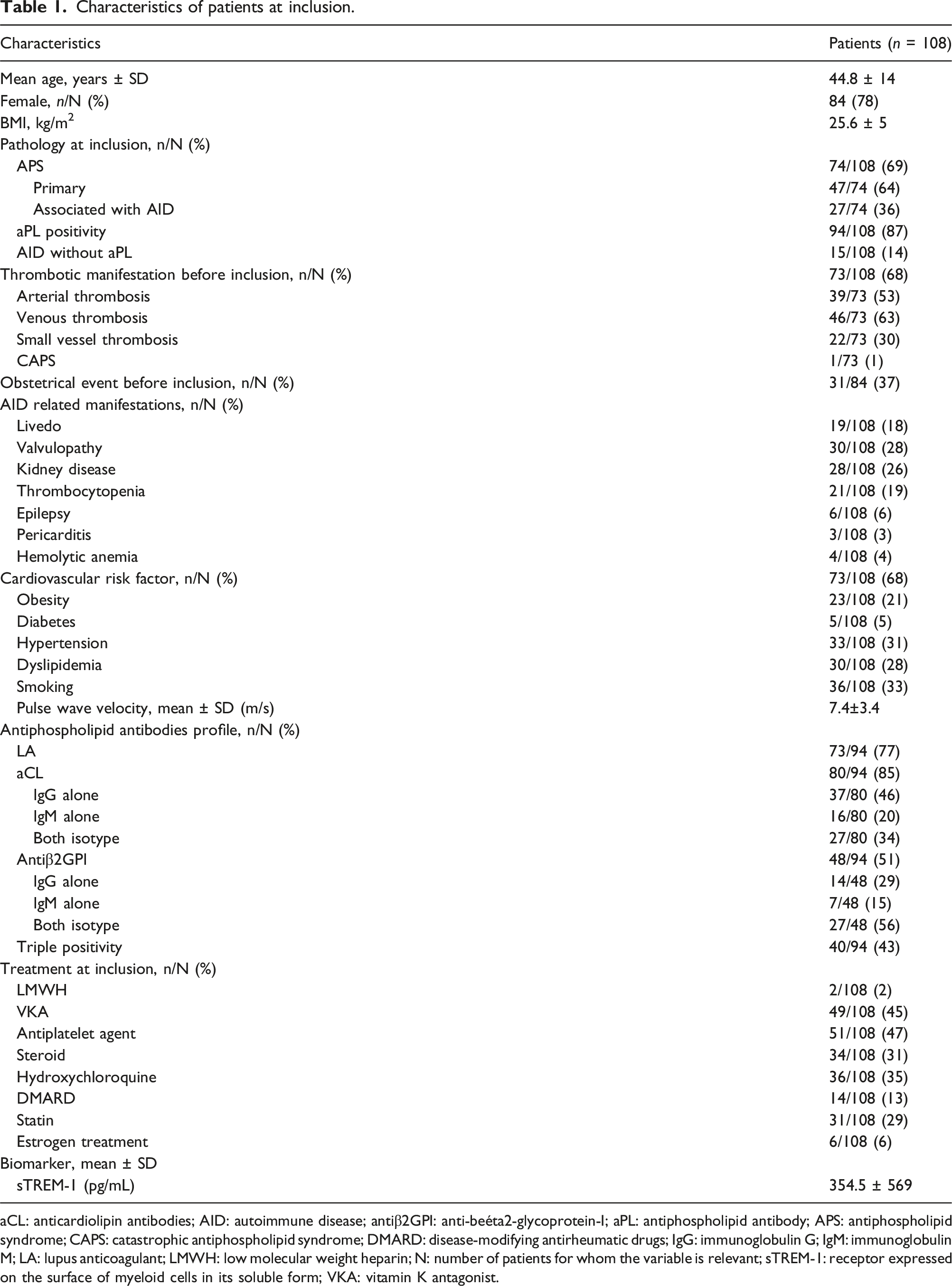
aCL: anticardiolipin antibodies; AID: autoimmune disease; antiβ2GPI: anti-beéta2-glycoprotein-I; aPL: antiphospholipid antibody; APS: antiphospholipid syndrome; CAPS: catastrophic antiphospholipid syndrome; DMARD: disease-modifying antirheumatic drugs; IgG: immunoglobulin G; IgM: immunoglobulin M; LA: lupus anticoagulant; LMWH: low molecular weight heparin; N: number of patients for whom the variable is relevant; sTREM-1: receptor expressed on the surface of myeloid cells in its soluble form; VKA: vitamin K antagonist.
Seventy-three (68%) patients had a history of previous thrombosis. One patient had a history of catastrophic APS (CAPS). Among patients with aPL positivity, 77% had LA, 85% had aCL, and 51% had anti-β2GPI. Triple positivity was found in 43% of patients.
Plasma sTREM-1 levels
Patients with primary APS had a higher sTREM-1 mean concentration than patients with isolated aPL positivity (363.7 ± 530 pg/mL vs. 149.4 ± 55, p = .02) [insert Figure 1]. Higher-s-TERM1 levels in patients with primary APS than with isolated aPL. sTREM-1 levels was higher in APS than in patients with isolated aPL.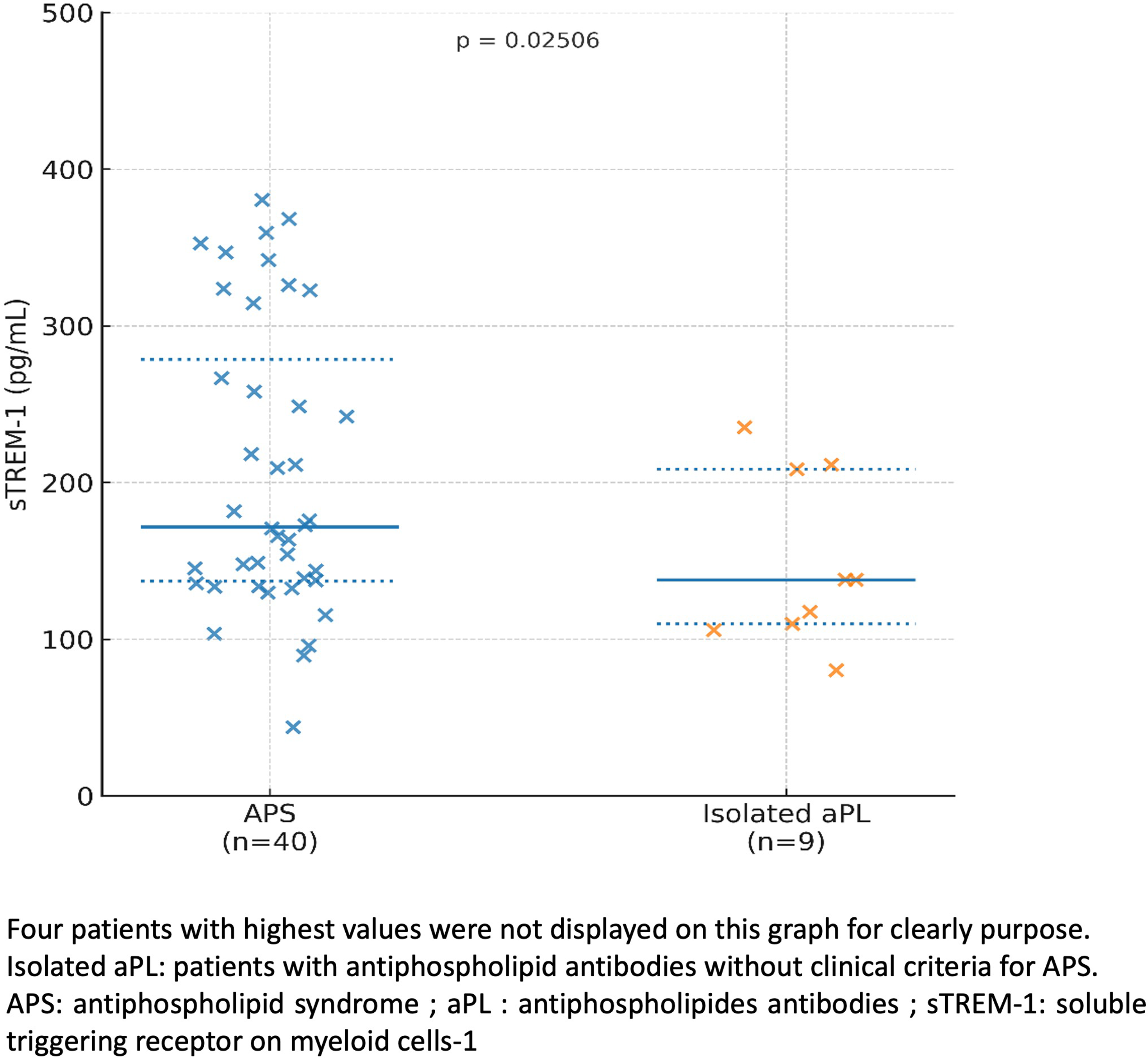
Events during follow-up
Twenty-three (21%) patients presented with an event during the follow-up, with a median time to onset of 28 months. Events were primarily thromboses, 6 arterial, 4 venous and 5 small vessels thromboses. Five patients died from APS complications during the follow-up. Three women presented with obstetrical events. Most of these patients (74%) had APS, three (13%) had previously had aPL without clinical criteria for APS, and three (13%) had isolated SLE.
Characteristics of events during the follow-up.
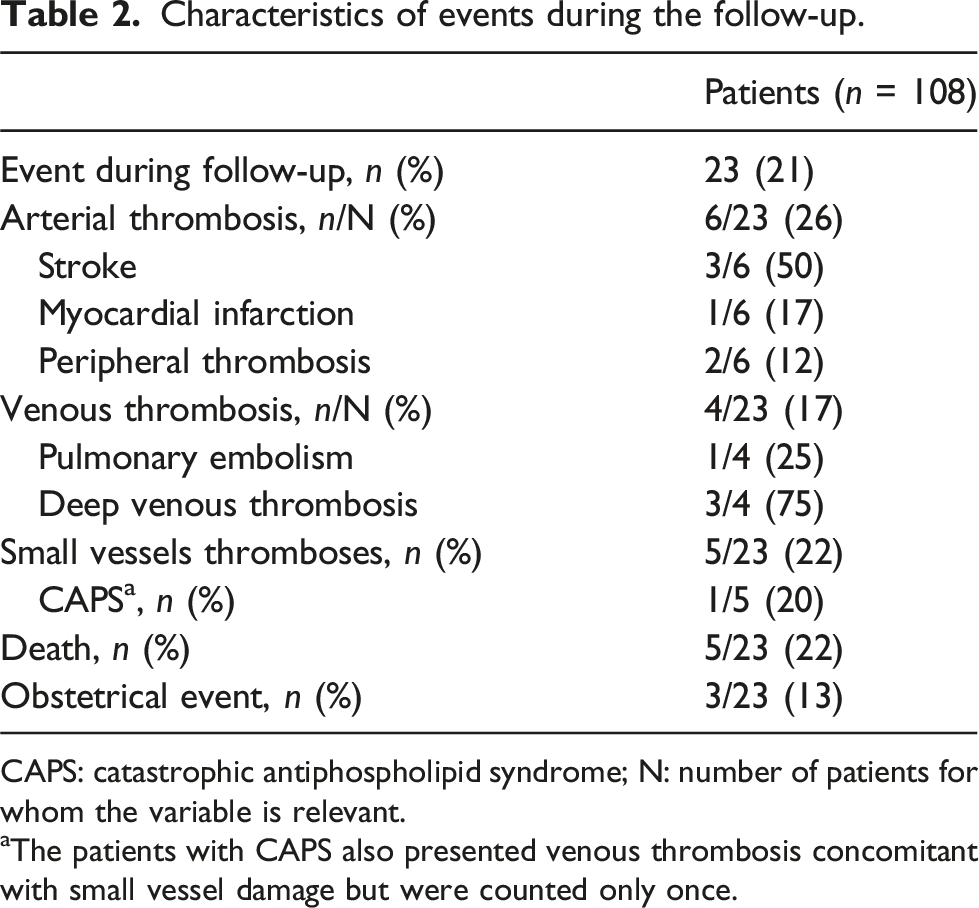
CAPS: catastrophic antiphospholipid syndrome; N: number of patients for whom the variable is relevant.
aThe patients with CAPS also presented venous thrombosis concomitant with small vessel damage but were counted only once.
Predictors of the occurrence of an event during follow-up
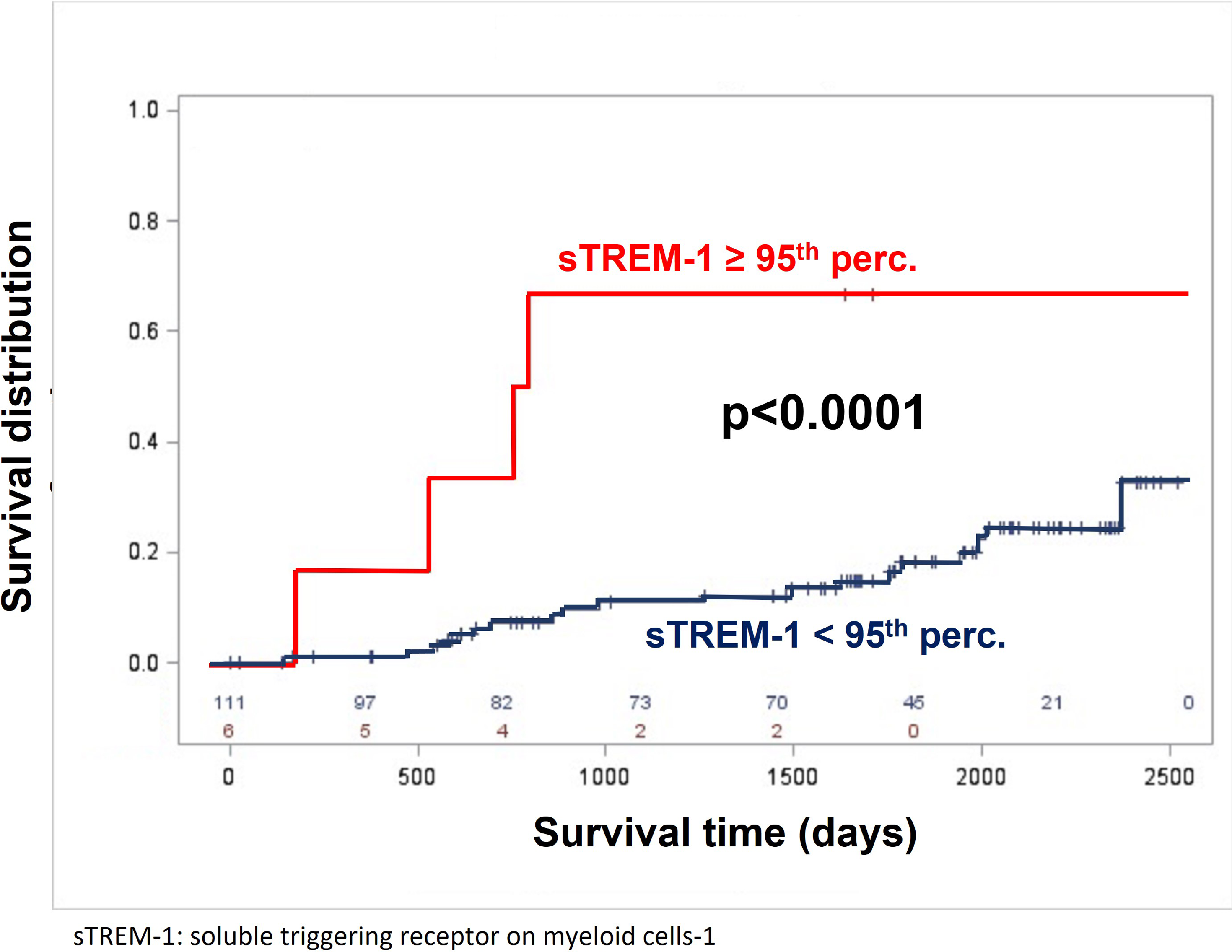
As shown in Figure 2 [insert Figure 2], the probability of occurrence of the composite criterion over time increased according to the sTREM-1 concentration. In bivariable regression, sTREM-1 ≥ 95th percentile (=1578 pg/mL) was the factor most strongly associated with the onset of an event (HR 7.54 [95% CI; 2.44-23.31]). The probability of an event occurring over time depending on the plasma level of sTREM-1 is shown in Figure 3 (levels over 95th percentile compared to lower values) [insert Figure 3]. Risk of compensate criterion (vascular thrombosis, obstetrical event or death) occurrence over time according to sTREM-1 values. Increased event risk with increasing sTREM-1 values. Probability of an event occurring over time according to the plasma level of sTREM-1. High level of sTREM-1 predicts the occurrence of a thrombotic and obstetric event or death in patients with aPL and/or SLE.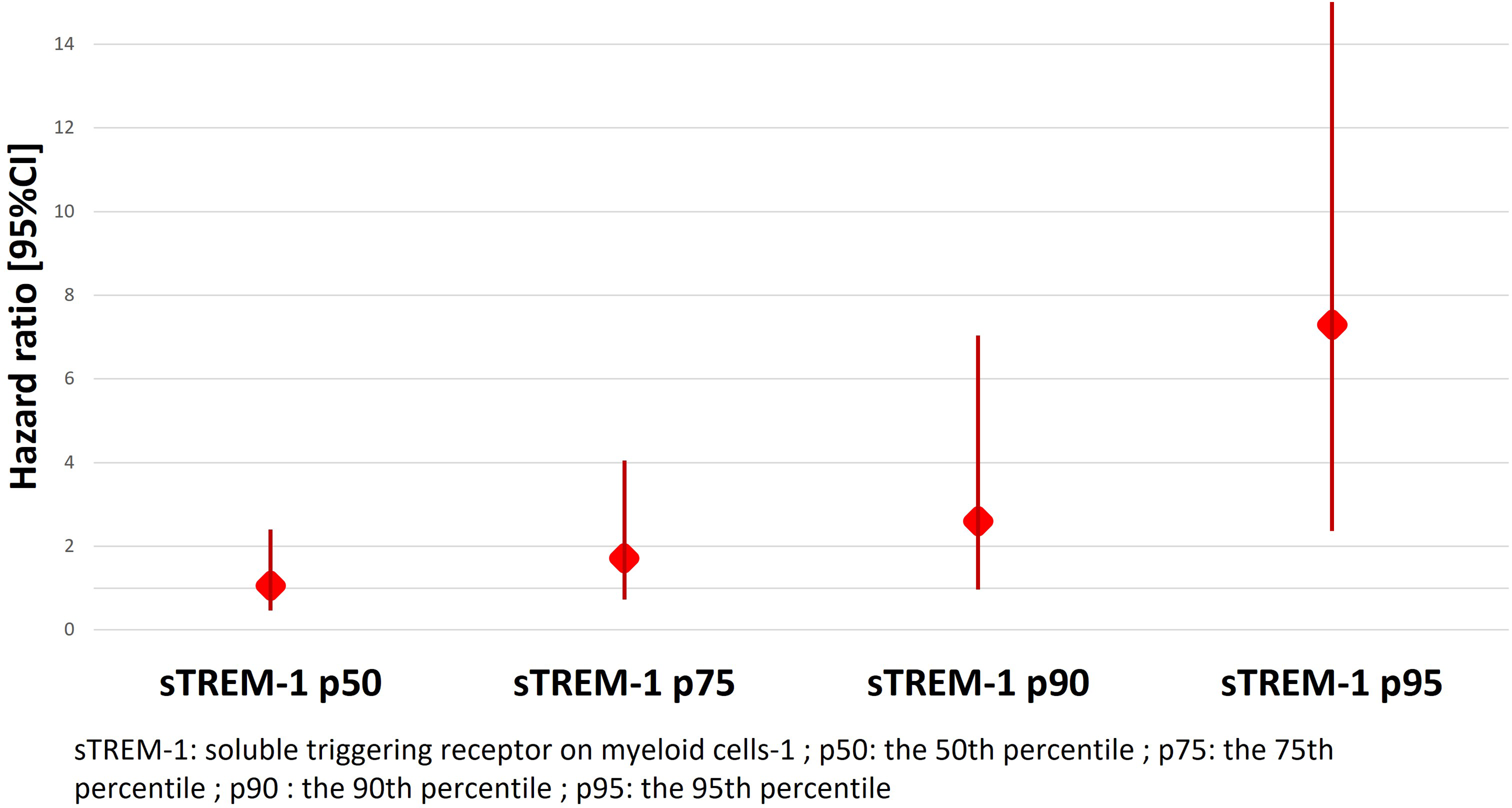
Bivariate regression for the global population.
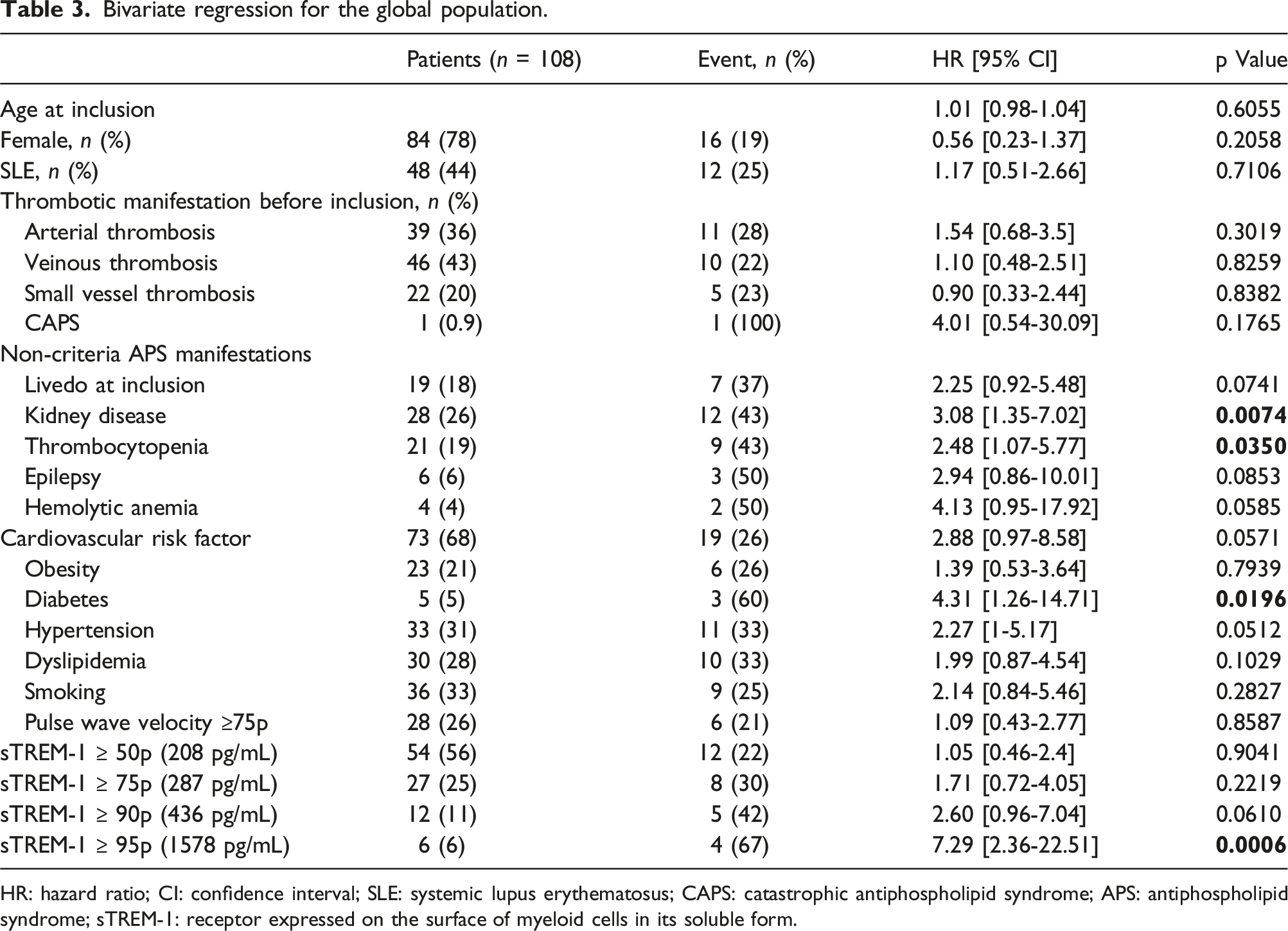
HR: hazard ratio; CI: confidence interval; SLE: systemic lupus erythematosus; CAPS: catastrophic antiphospholipid syndrome; APS: antiphospholipid syndrome; sTREM-1: receptor expressed on the surface of myeloid cells in its soluble form.
There was no correlation between biological signs of lupus activity (anti-double stranded (ds)DNA positivity, complement or leukocyte levels) and the occurrence of the composite criterion. The patients ranged in age from 23 to 70 years, with a median age of 44.8 years. Age at inclusion was not associated with the occurrence of the composite criterion. The mean age of patients who experienced an event during follow-up was 45 years, and the mean age of patients with sTREM-1 > 95th percentile was also 45 years.
In multivariate analysis, independent predictors for the occurrence of an event during follow-up were sTREM-1 ≥ 95th percentile (HR 3.79 [95% CI 1.06-13.58], p = .041) and the presence of kidney disease (HR 2.47 [95% CI 1.03-5.95], p = .043).
Discussion
Our study is the first longitudinal prospective study to examine the prognostic value of the sTREM-1 plasma concentration for the occurrence of events in patients with aPL and/or SLE. We showed that higher plasma concentrations of sTREM-1 increased the risk of an event occurring.
APS is a complex autoimmune disease associated with various organ involvement, various thrombotic risks and sometimes other autoimmune diseases. The risk of the occurrence of an event is often difficult to determine because so-called unprovoked thrombotic events are frequent in APS patients. Their potential degree of seriousness is variable, ranging from benign manifestations to catastrophic APS, due to specificities in APS physiopathology. The role of TREM-1 as an amplifier of the inflammatory response was established in septic shock. Inhibition of TREM-1 in a mouse model of sepsis partially protected against death. 27 In addition, the role of TREM-1 was demonstrated in chronic non-septic inflammatory states, particularly in AIDs, such as SLE 28 and rheumatoid arthritis. 29 Recent evidence suggests that sTREM-1 can be a new biomarker of disease activity and a potential predictor of the chronic course of Still’s disease. 13 However, data on TREM-1 involvement in APS are lacking. We confirmed the results of Edel et al., and showed, for the first time, the prognostic value of sTREM-1 concentration for thrombotic and obstetrical morbidity risk and death (composite criterion) in a cohort of patients composed primarily of aPL-positive patients.
This effect may be explained by the ability of TREM-1 to amplify TLR4 signaling and the pivotal role of TLR4 in APS. 4 Activation of the TLR4 pathway is involved in thrombosis in APS patients. The binding of aPL to β2GPI triggers the TLR4 pathway, which promotes NF-κB activation and the release of proinflammatory cytokines and procoagulant molecules by endothelial cells and monocytes.4,30 aPLs activate monocytes, which are the main blood cells that produce tissue factor, the initiator of coagulation. Activation of TLR4/NF-kB signaling in monocytes is involved in the expression of tissue factors. 31 TREM-1 inhibition decreases thrombin generation supported by monocytes via a reduction in tissue factor activity. 7
To use the sTREM-1 concentration as a biomarker of thrombotic risk, further investigations are needed to determine threshold values in different populations. If the role of the TREM-1 pathway in the pathogenesis of APS is confirmed, it may represent a new therapeutic target since TREM inhibitors are currently available for use in sepsis. 32
Our study has several limitations. Our study population was heterogeneous and included several patient groups. However, it allowed comparisons of patients with and without aPL and the same underlying disease, and this population reflects the real complex and heterogeneous population of patients with aPL in everyday practice. Moreover, the most of patient (86.1%) had aPL positivity. In our cohort, we registered biological variables related to lupus activity, such as anti-dsDNA positivity, complement activity, and leukocyte count. There were no predictors of the occurrence of the composite criterion, and there were no correlations between these biomarkers and sTREM-1 values. The main limitation is the number of patients, particularly patients with high TREM values, so the statistical power may have been insufficient to identify other predictive factors or potential confounding factors. However, we showed that higher sTREM-1 values predicted the occurrence of the composite criterion. Our results should be confirmed in larger multicenter prospective studies. Because the number of events was low, we used a composite endpoint clustering of thrombotic events, obstetrical events and death. Our study has also strength: it is a prospective study with a significant follow-up for a rare disease. Also, among patients with APS according to Sapporo-Sidney criteria, 86.1% fulfilled the ACR/EULAR APS 2023 criteria.
Conclusion
This preliminary study tends to confirm the hypothesis that patients with a high concentration of sTREM-1 were most at risk of thrombotic events, death or obstetric morbidity. Consequently, sTREM-1 represents a potential new prognostic biomarker in these patients. Taken together, these results suggest that targeting the TREM-1 pathway could represent a new approach to the treatment of APS.
Footnotes
Author contributions
V.D., S.Z., T.F., J.L., T.M., V.E. and D.W. conceived and designed the study, performed the quantification of sTREM-1 and aPL, collected and interpreted the data and wrote the first draft of the report. V.D., C.B., I.CU. S.Z. and D.W. performed the statistical analyses. J.L., D.W., S.Z., V.D. wrote and review the original draft.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Centre Hospitalier Regional de Nancy (Nancy Academic Hospital), Institut National de la Sante et de la Recherche Medicale and Association des chefs de service du CHRU de Nancy.