
Abstract
Objectives
In systemic lupus erythematosus (SLE), a serologically active clinically quiescent (SACQ) state is defined as one in which high anti-DNA antibody levels or low complement levels persist, however, disease activity remains stable. Although treatment intensification is not recommended for the SACQ state under the Treat to Target strategy, SACQ has been reported to be a risk factor for flares. The present study aimed to evaluate the efficacy of adding belimumab (BLM) to hydroxychloroquine (HCQ), the standard treatment for SLE, for patients in the SACQ state.
Methods
Patients treated with BLM were defined as the exposure group and those who did not were defined as the control group. Propensity score analysis with inverse probability of treatment weighting was used to analyze outcomes. The primary outcome was analyzed using the Kaplan–Meier method to determine time-to-event achievement to reduce prednisolone (PSL) dose to 7.5 mg/day or 5 mg/day. Secondary outcomes were as follows: (1) time to flares, analyzed using the Kaplan–Meier method, and (2) difference in median PSL dose at the last observation, analyzed using the Mann–Whitney U-test.
Results
Of the 146 patients in the SACQ state who received HCQ, 27 were included in the exposure group and 107 in the control group. The primary outcome, time-to-event achievement to reduce PSL dose to 7.5 mg/day and 5 mg/day had an HR value of 1.21 (95% confidence interval (CI) 0.78–1.89, p = 0.396) and 1.19 (95% CI 0.74–1.89, p = 0.471) in the two groups, respectively, with no significant difference between the two groups. No significant differences were observed in other outcomes.
Conclusions
Adding BLM to HCQ in patients in the SACQ state did not demonstrate effects in preventing flares or reducing glucocorticoids (GC) dose.
Keywords
Introduction
Systemic lupus erythematosus (SLE) is a disease characterized by recurring episodes of flares and remission, leading to damage across multiple organ systems due to chronic inflammation. The primary goal of SLE treatment is to achieve and maintain remission; however, maintaining low disease activity remains challenging. Historically, glucocorticoids (GC) have been the cornerstone of SLE treatment; however, GC-induced organ damage has posed clinical issues comparable to those caused by the disease activity itself. Organ damage due to GC use is dose-dependent but can also arise from long-term use, even at low doses.1,2 For instance, significant organ damage was observed when the time-adjusted mean dose of prednisolone (PSL) exceeded 4.42 mg/day. 3 Therefore, SLE treatment strategies aim to control disease activity while minimizing cumulative damage from disease activity and treatment-related side effects. In recent years, the effective use of biologics has garnered attention. Belimumab (BLM) and anifrolumab (ANF) have shown benefits in suppressing disease activity, reducing GC dose, and preventing flares in patients with active disease.4,5 The latest European Alliance of Associations for Rheumatology (EULAR) recommendations endorse these agents with a Grade A recommendation for patients with disease activity ranging from low to high. 6 However, the efficacy of BLM in serologically active clinically quiescent (SACQ) patients remains unclear.
SACQ is a state in which high anti-DNA antibody levels or low complement levels persist, however, the disease activity remains stable. The precise definition of SACQ varies across different studies.7–9 SACQ is an independent risk factor for flares.7,8 Additionally, it may be difficult for clinicians to reduce GC dose for patients with SACQ. In a survey of 130 clinicians from 30 countries, the rates of GC dose reduction and discontinuation in serologically abnormal patients compared with serologically normal patients were 58% (n = 59) versus 92% (n = 94) (p < 0.001) and 22% (n = 22) versus 52% (n = 53) (p < 0.001), respectively. 10 The clinical issues in the SACQ state are flare risk and cumulative GC exposure.
The treat-to-target (T2T) strategy for SLE states that “it is not recommended that the treatment in clinically asymptomatic patients be escalated based solely on stable or persistent serological activity.” 11 However, this recommendation was based on treatment escalation with GC, which increased cumulative GC exposure. A recent study reported that treatment escalation with hydroxychloroquine (HCQ), BLM, or immunosuppressants in the SACQ state does not effectively prevent flares or achieve remission. 12 However, subgroup analyses have indicated that BLM may improve remission rates. The limitations of this previous study included the low proportion of patients receiving HCQ as standard treatment (18 out of 109) and the small sample size for BLM (6 out of 24). The efficacy of BLM in the SACQ state during standard HCQ treatment is unclear.
We hypothesized that adding BLM to HCQ for patients in the SACQ state may reduce cumulative GC exposure and improve survival and functional outcomes. The present study aimed to clarify the efficacy of BLM for patients in the SACQ state receiving HCQ.
Methods
Population
The study was a retrospective analysis of patients with SLE who had a history of outpatient or hospitalization at the Department of Rheumatology at Juntendo University Hospital in Japan between January 1, 2012, and June 30, 2024. The patients with SLE were 18 years old or older and satisfied the following criteria: the 1997 American College of Rheumatology (ACR) revised criteria for SLE, 13 the 2012 Systemic Lupus International Collaborating Clinics classification criteria, 14 or the 2019 EULAR/ACR classification criteria. 15 In addition, the patients with SLE met the following SACQ definitions for ≧6 months: serological activity was defined as the presence of high levels of anti-DNA antibodies (>6 IU/mL, radioimmunoassay) or low levels of serum complement (C3 < 86 mg/dL and/or C4 < 17 mg/dL and/or CH50 < 25.0 CH50/mL). Disease activity was assessed using the SLE Disease Activity Index 2000 (SLEDAI). 16 The patients in the SACQ state met serological activity criteria, a clinical SLEDAI score of 0, and a PSL dose of ≦ 10 mg/day. The following patients were excluded: patients with less than 1 year of HCQ treatment history, patients undergoing treatment for malignancy, patients with other active autoimmune diseases, patients who have participated in clinical trials, and patients with unknown treatment histories.
Data collection
Data were collected from the medical records of Juntendo University Hospital, including age, sex, clinical history, medications, disease activity (SLEDAI), physician global assessment (PGA), and blood test results (C3, C4, CH50, anti-DNA antibody, anti-SS-A (Ro) antibody (double immunodiffusion method), anti-SS-B (La) antibody (double immunodiffusion method), anti-U1-RNP antibody (double immunodiffusion method), and anti-Sm antibody (double immunodiffusion method)). C3, C4, CH50, and anti-DNA antibodies were routinely measured for patients with SLE at our department, and we monitored serological levels and GC dose of PSL equivalent at each visit.
Study design
For eligible patients in the SACQ state who received HCQ, those who received BLM for at least 6 months were defined as the exposure group, and those who did not were defined as the control group. The observation period commenced after patients had received HCQ for more than 1 year and had maintained SACQ status for at least 6 months. It was terminated upon discontinuation of HCQ or BLM, the occurrence of flares, or at the time of the last observation. For the assessment of flares, we categorized them into mild/moderate and severe flares based on the SLENA-SLEDAI flare index (SFI). 17 HCQ was approved in Japan in September 2015, and BLM in May 2017. The exposure and the control groups were constituted in this study after these approval dates.
Outcomes
The primary outcome was defined as time-to-event achievement to reduce PSL dose to 7.5 mg/day or 5 mg/day. The number of cases for PSL 2.5 mg/day and 0 mg/day was extremely small to study. The secondary outcomes were the time to flares and the median difference in PSL dose at the last observation. The dose of PSL 7.5 mg/day and 5 mg/day referred to lupus low disease activity state (LLDAS) and definition of Remission in SLE (DORIS) 2021.18,19 LLDAS definition was the following: SLEDAI ≦ 4, with no activity in major organ systems and no hemolytic anemia or gastrointestinal activity, no new lupus disease activity compared with the previous assessment, PGA ≦ 1 (scale 0–3), a current PSL (or equivalent) dose ≦ 7.5 mg/day, and well tolerated standard maintenance doses of immunosuppressants and approved biological agents. 18 DORIS 2021 definition was the following: a clinical SLEDAI score = 0, PGA <0.5, PSL dose ≦5 mg/day, and stable HCQ, immunosuppressants, and biologics. 19
Statistical analysis
Patient characteristics were expressed as median (interquartile range (IQR)) or number of patients (percentage) and were compared between the exposure and control groups using the Mann–Whitney U test for continuous variables and the chi-squared test for categorical variables.
As the exposure group was expected to have a much smaller sample size than the control group, propensity score analysis with Inverse Probability Treatment Weighting (IPTW) was performed to minimize selection bias. The propensity score (PS) was calculated using logistic regression analysis, considering age, sex, disease duration, PSL dose at the time of inclusion, and lupus nephritis (LN) comorbidity as variables. Hajek scaling was used for the calculation of weights. For the exposure group, the weights were calculated as “(patients treated with BLM/sum of weights of patients treated with BLM)/(PS of patients treated with BLM)”; for the control group, the weights were calculated as “(patients not treated with BLM/sum of weights of patients not treated with BLM)/(1-PS of patients not treated with BLM). To evaluate differences in GC reduction time between the exposure and control groups, the event was defined as the point at which PSL was reduced to 7.5 mg/day or 5 mg/day, and the Kaplan–Meier method was used to analyze the time-to-event achievement. Cases that did not reach the target PSL dose during the observation were censored at the last observation. Similarly, flares were defined as the event, and the time to flares was analyzed using the Kaplan–Meier method as the flare-free survival probability. Cases that did not experience flares during the observation were censored at the last observation. Differences between groups were assessed using the log-rank test. The Mann–Whitney U test was used to analyze the median difference in PSL dose at the last observation. All reported P-values are two-sided. Statistical significance was set at p < 0.05. All analyses were conducted using R software version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Ethical considerations
This study was approved by the Institutional Review Board of Juntendo University, Japan (Approval No. E24-0234-H01). The present study was conducted in accordance with the principles of the Declaration of Helsinki. Owing to the anonymous nature of the patient data, the requirement for informed consent was waived.
Results
Patient characteristics
Approximately 1000 patients with SLE continuously visit the Department of Rheumatology at Juntendo University Hospital, Japan. SACQ is a state that can change transiently and the present study represented an observation at a single time point from a long-term perspective. Therefore, we selected patients who presented with SACQ for 6 months between January 2012 and June 2024. A total of 151 patients receiving HCQ who met the criteria for the SACQ state were identified. Five patients who had less than 1 year of HCQ treatment history, two patients undergoing treatment for malignancy, two with other active autoimmune diseases, two with unclear treatment histories, and six participating in clinical trials were excluded. Finally, 27 patients were included in the exposure group and 107 in the control group. BLM was administered intravenously in four patients (two of the four patients were subsequently switched to subcutaneous injections) and subcutaneously in the other patients.
Baseline clinical characteristics of the patients in the BLM + HCQ and HCQ groups.
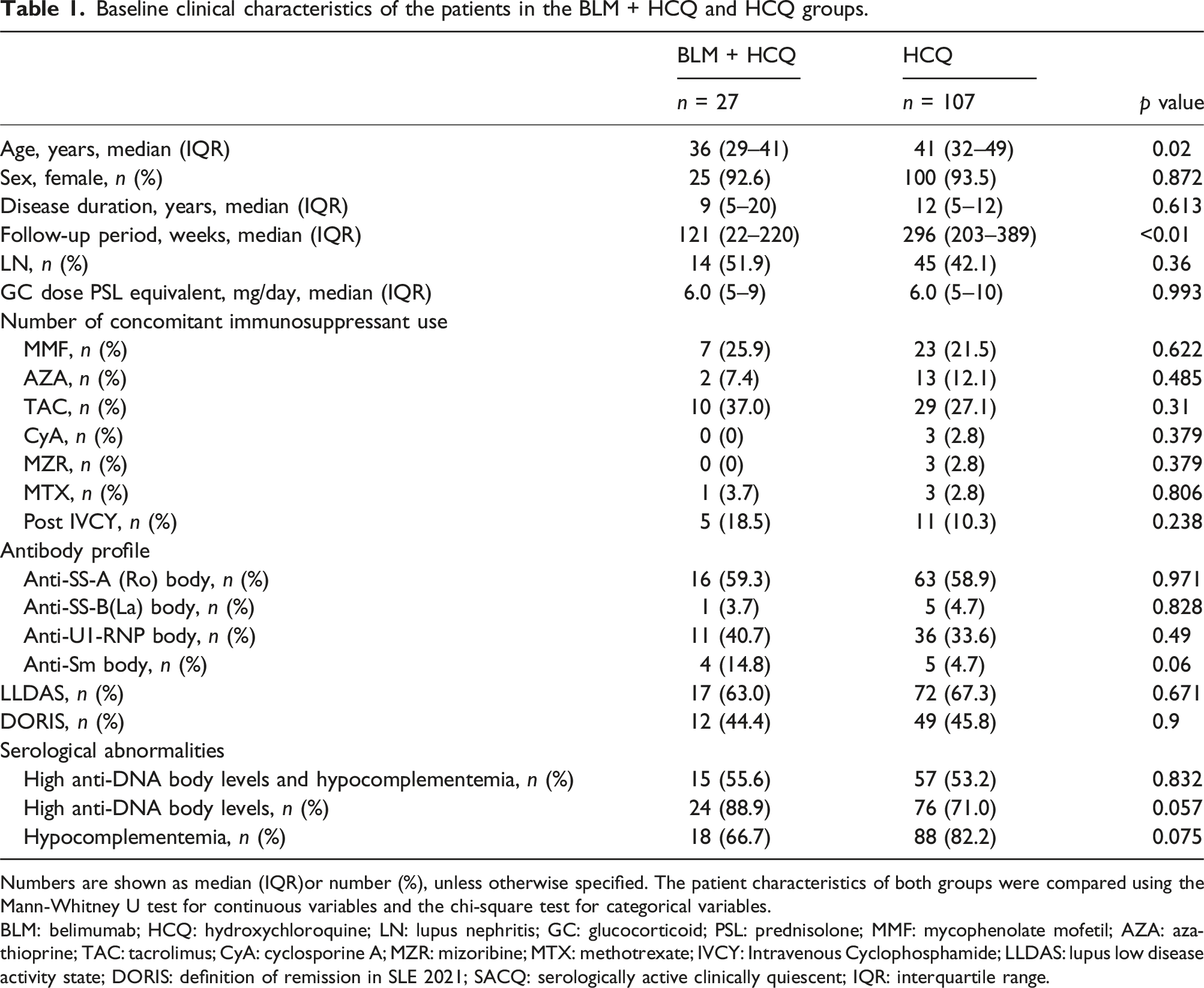
Numbers are shown as median (IQR)or number (%), unless otherwise specified. The patient characteristics of both groups were compared using the Mann-Whitney U test for continuous variables and the chi-square test for categorical variables.
BLM: belimumab; HCQ: hydroxychloroquine; LN: lupus nephritis; GC: glucocorticoid; PSL: prednisolone; MMF: mycophenolate mofetil; AZA: azathioprine; TAC: tacrolimus; CyA: cyclosporine A; MZR: mizoribine; MTX: methotrexate; IVCY: Intravenous Cyclophosphamide; LLDAS: lupus low disease activity state; DORIS: definition of remission in SLE 2021; SACQ: serologically active clinically quiescent; IQR: interquartile range.
We attempted to match patients in both groups using IPTW: the age category was stratified and used to age-match patients in the control and exposure groups. The analysis of the flare-free survival probability was performed using a dataset that included flare cases (Supplement 1). The analysis of the primary outcome and the difference in the median PSL dose at the last observation was performed using a dataset that excluded flare cases (Supplement 2). The standardized mean difference (SMD) for each dataset is shown in Supplement 1 and Supplement 2. However, when sex was included (male vs female), the SMD was not less than 0.1. When restricted to female participants, the SMD was <0.1, indicating balanced variables between the two matched groups (Supplement 1, 2). SLE has a female-to-male ratio of 9:1. Additionally, male cases tend to be more severe and adjusting for background factors is difficult. For these reasons, limiting the analysis to female participants was clinically appropriate.
Outcomes
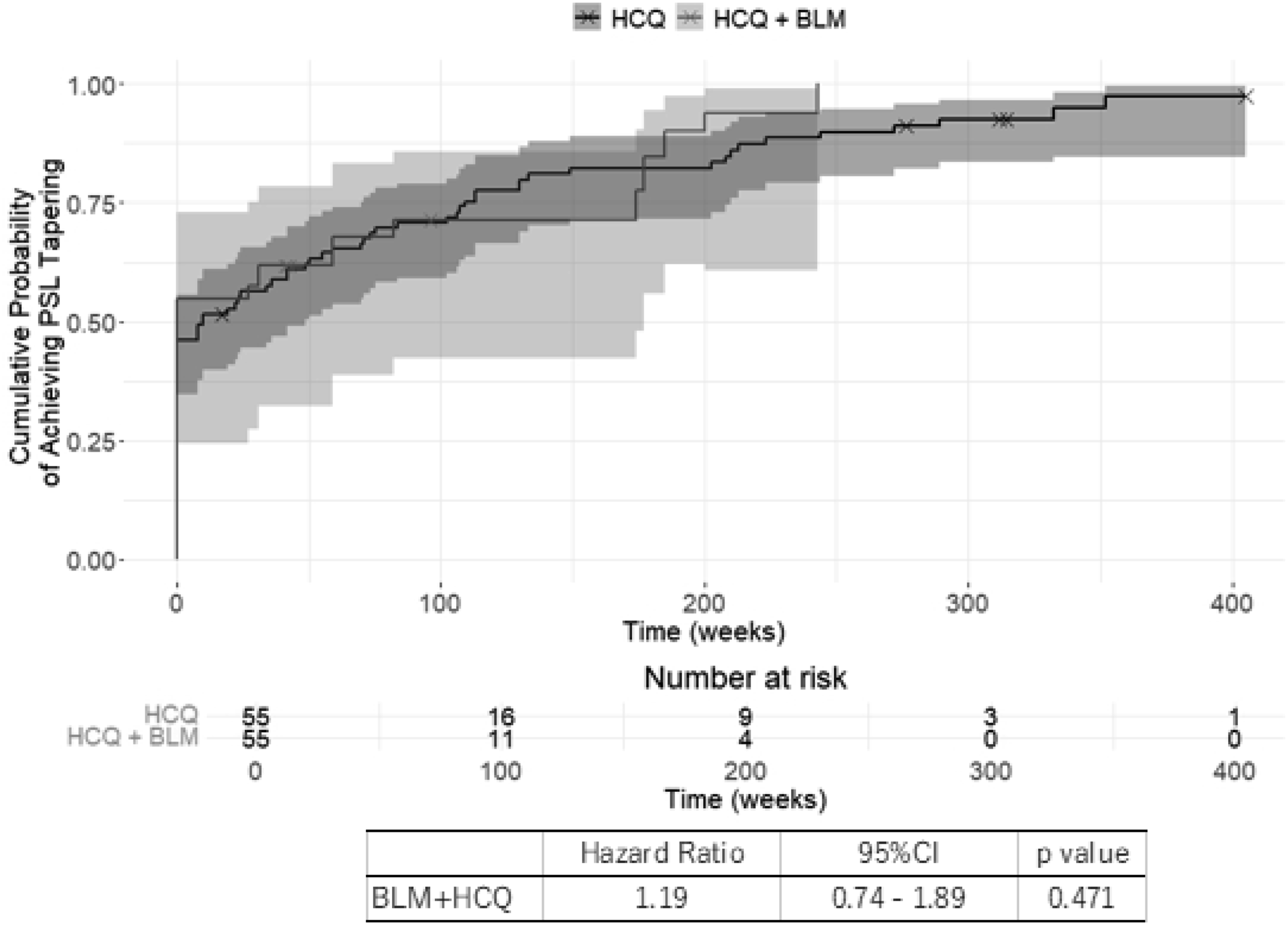
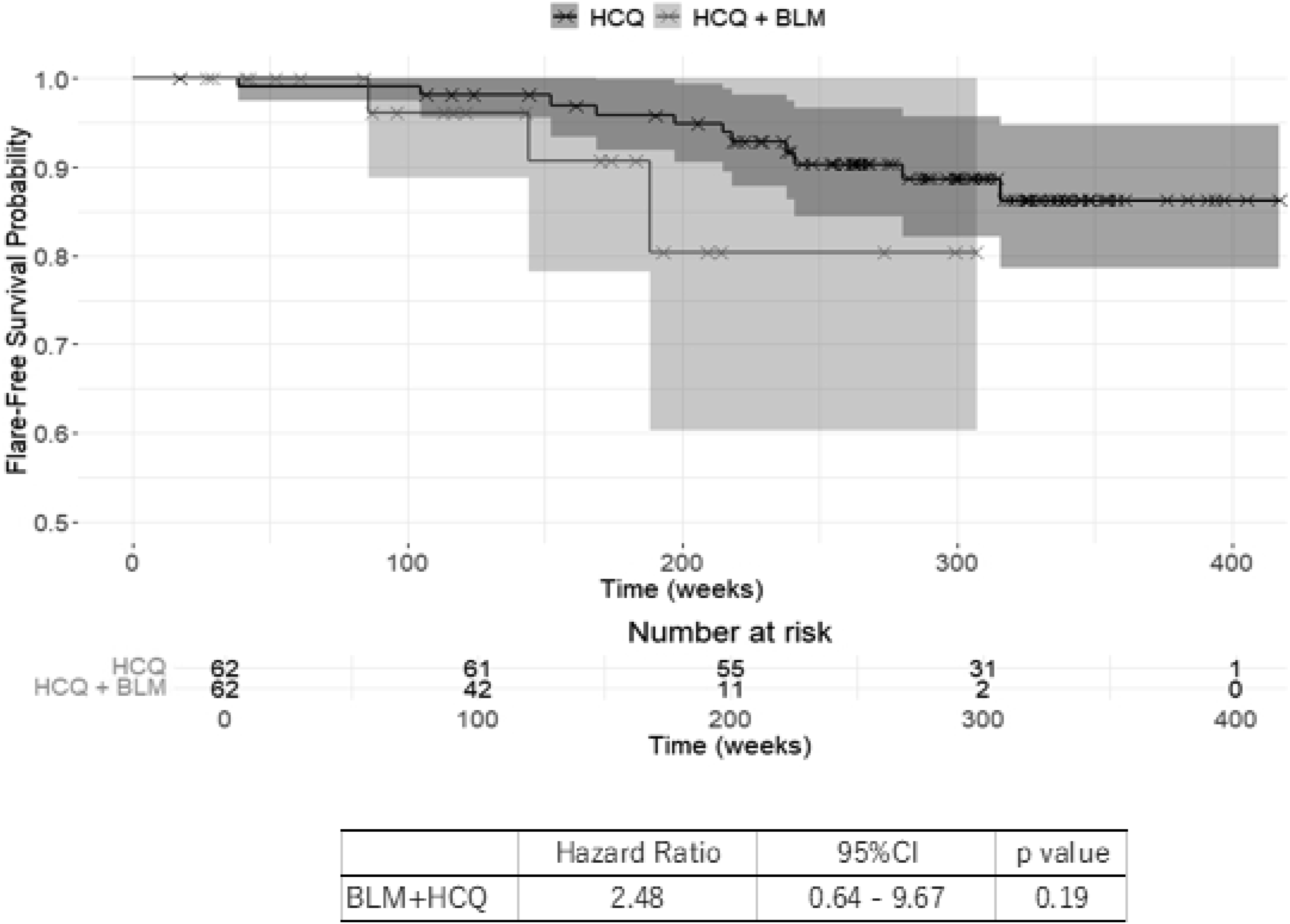
During the observation period of the study, flares occurred in three patients (3/27, 11.1%) in the exposure group and 12 patients (12/107, 11.2%) in the control group. In the exposure group, there were two severe flares (one neuropsychiatric SLE (NPSLE), one LN) and one mild/moderate flare. Conversely, the control group had two severe flares (one NPSLE, one LN) and 10 mild/moderate flares. The primary outcome, time-to-event achievement to reduce PSL dose to 7.5 mg/day and 5 mg/day showed no significant difference between the two groups, and showed a Hazard Ratio (HR) of 1.21 (Figure 1, 95%CI: 0.78–1.89, p = 0.396) and 2.48 (Figure 2, 95%CI: 0.74–1.89, p = 0.471), respectively. The flare-free survival probability showed no significant difference between the two groups based on HR values of 2.48 (Figure 3, 95%CI 0.64–9.67, p = 0.19). In the present study, the median PSL dose at the last observation was 5 mg/day (Inter-quartile Range [IQR]: 2.2–7.8 mg/day) in the exposure group and 4 mg/day (IQR: 1–7 mg/day) in the control group. The difference in median PSL dose at the last observation was 0.073 (p = 0.297), indicating no significant difference. The time-to-event achievement to reduce PSL dose to 7.5 mg/day. The time-to-event achievement to reduce PSL dose to 5 mg/day. The flare-free survival probability.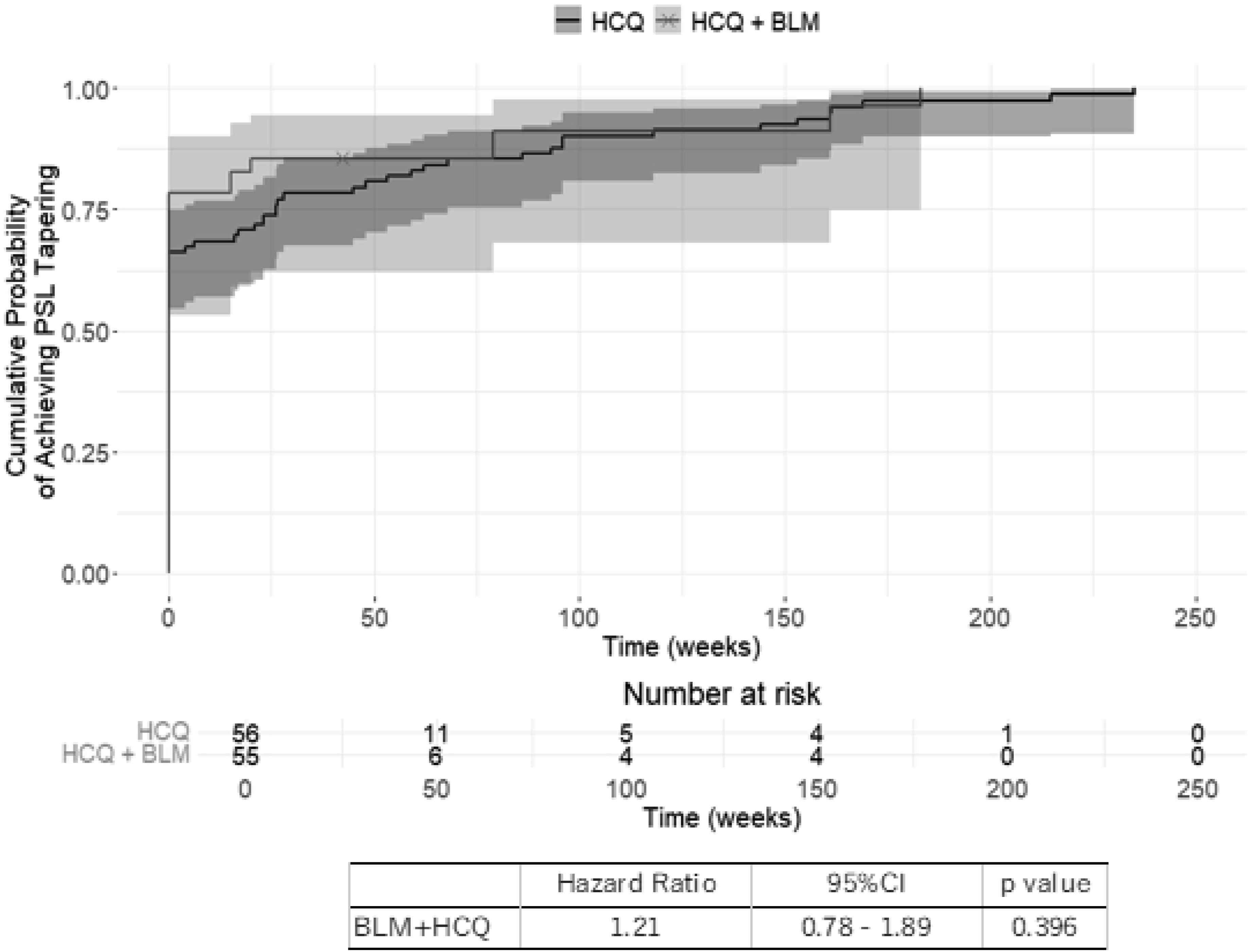
Safety analysis
In the present study, five patients met the SACQ criteria, however, had been treated with HCQ for less than 1 year as they had side effects. Three patients experienced skin rashes, and two patients experienced gastrointestinal symptoms.
After inclusion, no withdrawals due to adverse events or infections caused by HCQ or BLM were observed in either group.
Discussion
The present study found no advantage of adding BLM to the treatment regimen of patients in the SACQ state being treated with HCQ in terms of the reduction of GC and the time to flares.
The 2014 T2T recommendations stated that “in the absence of clinical symptoms, treatment intensification based solely on serological abnormalities (elevated anti-DNA antibodies and hypocomplementemia) is not recommended.” 11 This recommendation was based on treatment escalation with GC. In current SLE management guidelines, treatment escalation with HCQ, immunosuppressants, and biologics, such as BLM and ANF can be considered. Whether intensifying treatment with these therapeutic agents for the SACQ state can prevent flares or improve remission rate has remained a clinical question. A previous study investigated the efficacy of treatment escalation with HCQ, BLM, and immunosuppressants in terms of flare and remission rates in patients in the SACQ state. 12 HCQ therapy was found to be effective in preventing flares; however, no significant differences were observed in flare or remission rates. However, in subgroup analysis, a significant improvement in remission rates was observed with BLM treatment. The low rate of HCQ use in this study may have contributed to the significant increase in remission rates upon BLM administration. The efficacy of HCQ treatment has been demonstrated in various studies. HCQ has been shown to reduce disease activity, prevent flares, and reduce long-term GC dose. 20 Moreover, even after adjusting for disease activity and GC dose, HCQ has been shown to reduce damage accumulation in patients with SLE. 21 The clinical guidelines for SLE have recommended the introduction of HCQ as standard therapy for all patients with SLE. 6
The present study focused on patients in the SACQ state receiving HCQ and was able to eliminate the limitations of the previous study. This enabled us to evaluate the efficacy of BLM treatment on patients in the SACQ state under standard treatment with HCQ. BLM treatment has been found to significantly reduce flare rate, with a meta-analysis reporting a 66% reduction in flares. 22 Adding BLM to HCQ treatment was expected to lead to better outcomes in terms of flare prevention. However, no significant difference was observed in the time to flares among the two groups. The reasons for the discrepancies with the previous study include insufficient statistical power due to the small sample size and differences in patient characteristics. In the patient characteristics of the previous study, the mean GC dose equivalent PSL was 12.1 mg/day (range: 8.8–30.0 mg/day), and the mean SLEDAI score was 10.1 (range: 8.0–12.7), which differed from the patient characteristics in the present study. Considering the present and previous studies, it could be concluded that treatment intensification for patients in the SACQ state who are already receiving HCQ is not recommended, aligning with the T2T recommendations. A previous study showed that HCQ therapy for patients in the SACQ state was associated with a reduced risk of flares. 9 Currently, for the treatment of patients in the SACQ state, it is important to first start HCQ therapy if it is not already being administered, as recommended by the guidelines.
Although the SACQ state has been reported to not influence overall survival, 23 it is an independent risk factor for flares.7,8 In clinical practice, GC dose reduction in the SACQ state is often difficult due to concerns regarding organ damage from flares. However, GC treatment itself is associated with organ damage.1–3 In the SACQ state, the hesitation to reduce GC dosage due to the fear of flares leads to long-term GC exposure, which is a clinical concern. BLM is also recognized for its GC dose reduction effect. 24 Therefore, the present study aimed to evaluate the efficacy of adding BLM on GC dose reduction for patients in the SACQ state who had been receiving HCQ. The present study showed no significant difference between the two groups in the median PSL dose at the last observation and the time to achieve a reduction to PSL 7.5 mg/day or 5 mg/day. These results suggest that adding BLM therapy to patients in the SACQ state who had been receiving HCQ may not facilitate GC dose reduction. However, even with a gradual reduction of the PSL dose by 1 mg/day, no significant increase was observed in the risk of general flares (HR 1.02, 95%CI: 0.99–1.05) or severe flares (HR 0.98, 95%CI: 0.96–1.004). 9 Moreover, tapering the GC dose was associated with a reduced risk of damage accumulation (HR 0.96, 95%CI: 0.93–0.99) in patients who had an initial PSL dose exceeding 5 mg/day. 9 It is important to consider tapering GC in SACQ patients to reduce cumulative GC exposure based on their clinical course.
The present study has several limitations. First, the initiation of BLM therapy and the schedules for GC dosage tapering were left to the discretion of the attending physician, making it difficult to adjust for patient backgrounds. Particularly regarding the initiation of BLM in patients in the SACQ state, there is no established recommendation, and the decision is made by individual clinicians. Although we used IPTW analysis to adjust for patient backgrounds and account for the small sample size, unmeasured confounders may still not have been controlled. Furthermore, since the GC tapering was slow in the present study, the flare rate may vary depending on the GC tapering. As this was a retrospective study, future prospective studies using randomized controlled trials are needed. Second, the maximum follow-up period of the present study was about 9 years, and longer follow-ups may alter the results. While the present study evaluated GC dose reductions to 7.5 mg/day and 5 mg/day of PSL, further investigation into reductions at lower doses, such as 2.5 mg/day and 0 mg/day through longer-term follow-up, would be beneficial. In addition, the timing of the pharmaceutical approval of HCQ and BLM in Japan differed, and the observation periods for the two groups were different, which may have led to differences in the analysis results and clinical background. Third, the small sample size likely led to reduced statistical power. Fourth, it was difficult to confirm medication compliance, using tests, such as BLM and HCQ serum concentrations. Finally, the present study was conducted solely in Japan, which introduces the possibility of selection bias due to racial factors.
The present study examined the efficacy of BLM therapy for patients in the SACQ state receiving HCQ. However, no significant effect was found in preventing flares or reducing the GC dose. In patients with the SACQ state receiving HCQ, it is recommended to reduce GC dose and minimize the risk of long-term GC-related damage.
Supplemental Material
Suppplemental Material - Efficacy of adding belimumab to hydroxychloroquine for patients with serologically active clinically quiescent in systemic lupus erythematosus: A retrospective study
Suppplemental Material for Efficacy of adding belimumab to hydroxychloroquine for patients with serologically active clinically quiescent in systemic lupus erythematosus: A retrospective study by Yusuke Yanagimoto, Kentaro Minowa, Eitaro Yoshida, Emi Nakanishi, Ayako Makiyama, Hirofumi Amano, Ken Yamaji and Naoto Tamura in Lupus
Footnotes
Acknowledgments
We thank all the participants of this study for their cooperation. We thank 4DIN Ltd for commissioning the statistical analysis.
Author contributions
All authors were involved in drafting the article or revising it critically for important intellectual content and approved the final version to be submitted for publication. Y. Y. had full access to all the data of this study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study design and coordination: K M, NT.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NT has received research grants from Asahi Kasei Pharma, Asahi Kasei Medical, Ayumi, AbbVie, Eisai, Nippon Boehringer Ingelheim, Taisho, Tanabe Mitsubishi, Chugai, and speaker’s fee and/or consulting fee from Asahi Kasei Pharma, AstraZeneca, AbbVie, Eli Lilly Japan, GlaxoSmithKline, Chugai, Novartis, Bristol Myers Squibb, Janssen. The other authors declare that they do not have any conflicts of interest concerning the research, authorship, and/or publication of this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
We obtained approval for this study from the Institutional Review Board of Juntendo University, Japan (Approval No. E24-0234-H01). This study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent to participate
Owing to the anonymous nature of the data, the requirement for informed consent was waived.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.