
Abstract
Background
LupusPRO is a disease-targeted, patient-reported outcome measure developed for assessing the quality of life in patients with systemic lupus erythematosus. Initially, the questionnaire was validated among U.S. patients of varied ethnic backgrounds and genders. This study aims to carry out a cross-cultural adaptation and validation of the Polish-translated version of LupusPRO.
Method
We administered the Polish version of LupusPRO along with the 36-Item Short Form Health Survey (SF-36) and EQ-5D-5L questionnaire, and the Polish modification of the Hospital Anxiety and Depression Scale (HADS-M). At the same time, we collected demographics and clinical characteristics. Disease activity, damage, and exacerbation were assessed using SELENA-SLEDAI, SLICC/ACR DI and LFA. Furthermore, we tested internal consistency reliability (measured with Cronbach’s alpha), test-retest reliability (using r-Pearson correlation coefficient), convergent validity (against corresponding domains of SF-36) and criterion validity (against disease activity, damage and EQ-VAS), and known group validity.
Results
A total of 199 (91% females) patients with SLE with a mean age of 42.6 ± 12.62 years participated in the study. We observed that the mean SELENA-SLEDAI reached 5.3 (±5.9) points, while SLICC/ACR DI was at 1.3 (±2.0) points. The internal consistency reliability of LupusPRO domains ranged between 0.737 and 0.925 (except for Lupus Symptoms, Social Support, Coping, and Satisfaction with care). For all domains except Social Support, test-retest reliability exceeded 0.7. Convergent validity with corresponding domains of the SF-36 was good (r > 0.5). All health-related quality of life domains performed well against disease activity and damage measures, establishing its criterion validity. Confirmatory factor analysis showed a satisfactory fit. (± expression of range).
Conclusion
The Polish version of LupusPRO has proved to have fair psychometric properties among Polish patients with SLE.
Introduction
Systemic lupus erythematosus is a chronic inflammatory connective tissue disease of autoimmune origin. The disease significantly affects various spheres of human life: physical, mental, and social. As a result, the quality of life in patients with SLE is substantially decreased compared to the general population, as numerous scientific publications proved.1–3 Initially, the quality of life in SLE patients was assessed using general questionnaires: SF-36, 4 WHO-BREF, 5 and EQ-5D-5L. 6 However, they all proved imperfect, as these questionnaires did not include many important aspects for lupus patients. Furthermore, the general questionnaires were not sensitive enough to register changes in disease activity.7,8 In response to their imperfections, researchers have begun to develop new, specific quality-of life questionnaires designed exclusively for patients with lupus: SSC, 9 SLEQOL, 10 LQOL, 11 LupusQOL 12 and LupusPRO. 13 They all have obtained satisfactory psychometric properties assessment and can be used among SLE patients. The LupusQoL and SLEQOL are disease-specific questionnaires developed to assess health-related quality of life (HRQoL) in patients with systemic lupus erythematosus (SLE), with the LupusQoL being the most frequently used instrument in this context. Of the SLE-specific questionnaires, LupusPRO stands out in particular because of its comprehensive evaluation of the quality of life - taking into account its two dimensions: healthrelated (HRQOL) and non-health-related (non-HRQOOL). It has the advantage of being validated among a U.S. population of SLE patients of both genders with diverse ethnic backgrounds. The original and other validations14–24 versions have obtained satisfactory assessments of psychometric properties: reliability and validity. So far, no questionnaire specific to SLE has been available in Poland. In this study, we report the results of cross-cultural validation of the Polish version of LupusPRO in patients with SLE.
Methods
LupusPRO has two constructs: health-related (HRQOL) and non-health-related (non-HRQOL) quality of life. The HRQOL domains are Lupus symptoms, Cognition, Lupus medications, Procreation, Physical health, Pain/Vitality, Emotional Problems, and Body image. The non-HRQOL domains are Desires/Goals, Coping, Social support, Satisfaction with medical care, and General health. Individual domains score, total HRQOL, and total non-HRQOL scores range from 0 to 100, where a higher score signifies a better QOL. This study was conducted in four reference Rheumatology Departments in Poland. It was approved by the Institutional Ethics Committee of the Rheumatology Institute in Warsaw. The translation of the US LupusPRO was undertaken using standard guidelines25,26 to develop the Polish LupusPRO. During the linguistic and socio-cultural adaptation of the LupusPRO questionnaire, no significant difficulties were noted in translating it into Polish and adapting it to Polish conditions. Before inclusion into the study, we obtained informed consent from all patients. The study involved adult patients above 18 years of age with SLE diagnosed based on the SLICC criteria 27 from 2012. Data on the following variables were collected during a baseline visit: demographic information, clinical examination, disease activity, and damage assessment. Patients filled out the quality of life questionnaires: the Polish version of LupusPRO, SF-36, and EQ-5D-5L. Higher scores on SF-36 indicate better health. Disease activity was assessed by SELENA-SLEDAI 28 scale, and damage was assessed by SLICC/ACR DI. 29 In addition, depression and anxiety were evaluated using a Polish modification of the Hospital Anxiety and Depression scale (HADS-M). 30 HADS-M assesses the level of the severity of depression and anxiety. Furthermore, patients were handed another LupusPRO to be completed within 2–3 days and returned to the study site or sent by mail. Psychometric properties studied reliability and validity. Under reliability, internal consistency (ICR) was examined, and a test-retest was conducted. The ICR was evaluated using Cronbach’s alpha, where an alpha> 0.7 is considered acceptable. 31 TRT was tested by assessing agreement between the patient responses to each domain at two-time points. It was evaluated using r-Pearson correlation coefficient. The evaluation of the validity of the Polish version of the LupusPRO questionnaire consisted of examining construct and criterion validity. Convergent validity, the method of validating known groups, and confirmatory factor analysis were analyzed as part of the construct validity assessment. Convergent validity was examined using Spearman’s correlation coefficient by evaluating the correlation strength with related domains on the SF-36v2 and HADS-M. The criterion validity of the polish version of LupusPRO questionnaire was determined by correlation with SELENA-SLEDAI, SLICC/ACR DI and EQ-VAS. Correlations were classified as strong (r > 0.5), moderate (0.3 > r < 0.5), weak (0.1 > r < 0.3), or absent (<0.1). Floor and ceiling effects were analyzed. Known group validity was judged against disease activity (SELENA-SLEDAI) and patient-reported health status (item 1 from SF-36). The conceptual framework (hypothesized item-to-scale relationships) of the LupusPRO was evaluated using confirmatory factor analysis (CFA) appropriate for categorical data. The goodness of fit of the hypothesized item-to-scale relationships (multi-factor) was evaluated with the Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), and Root Mean Square Error of Approximation (RMSEA). It is recommended that CFI and TLI should be 0.9 or greater as evidence of acceptable model fit, 32 and RMSEA should be ≤0.08. 33 All reported p values are two-tailed.
Results
Description of the study cohort (n = 199).
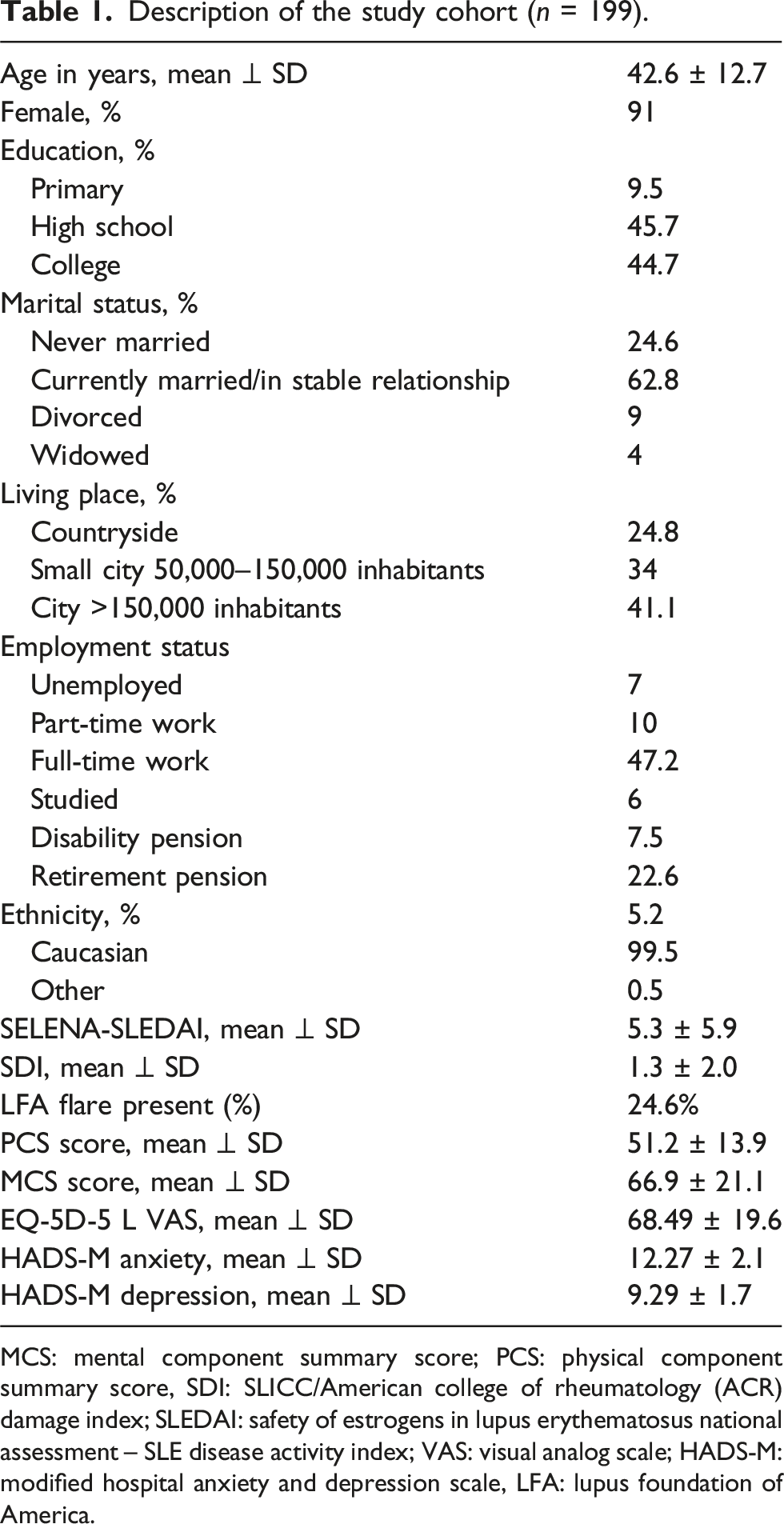
MCS: mental component summary score; PCS: physical component summary score, SDI: SLICC/American college of rheumatology (ACR) damage index; SLEDAI: safety of estrogens in lupus erythematosus national assessment – SLE disease activity index; VAS: visual analog scale; HADS-M: modified hospital anxiety and depression scale, LFA: lupus foundation of America.
Descriptive scores of the LupusPRO domains in polish patients with SLE.
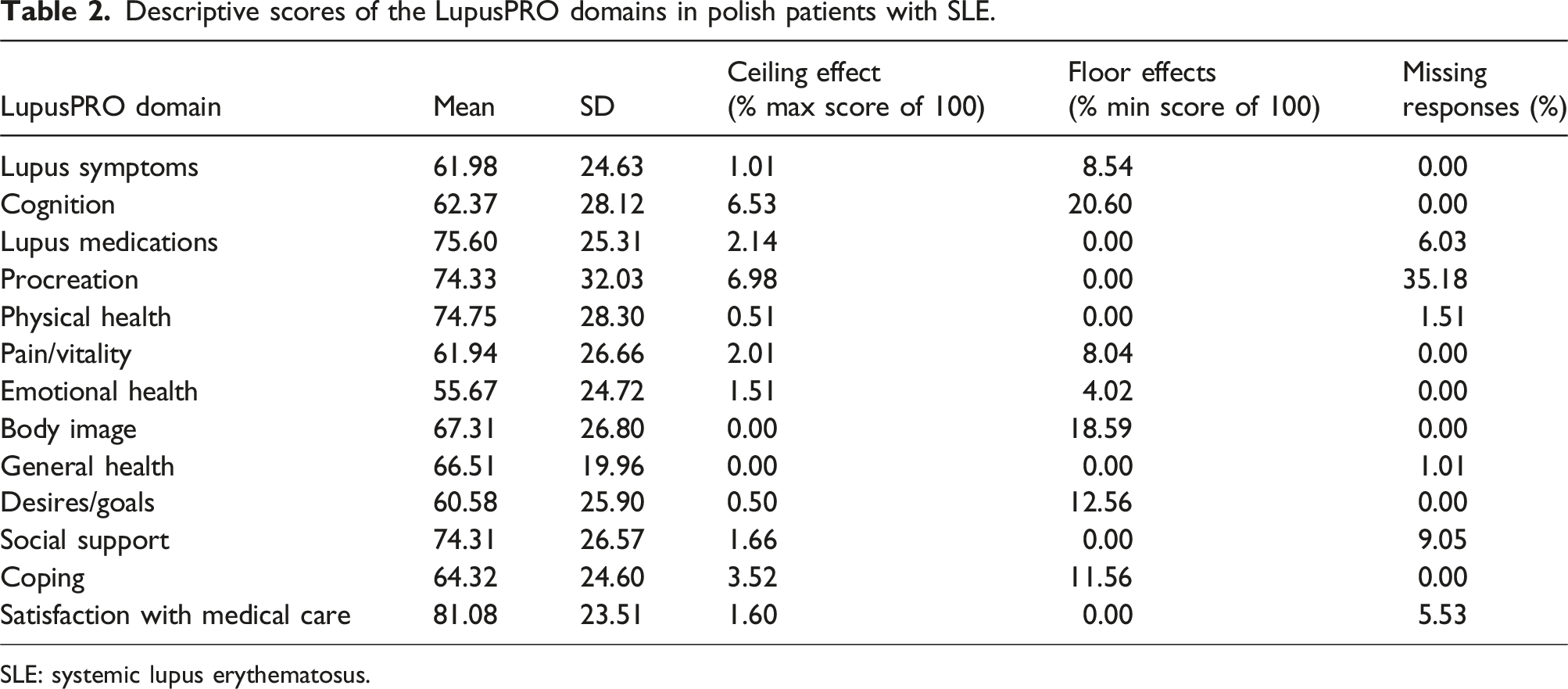
SLE: systemic lupus erythematosus.
Psychometric properties of LupusPRO.
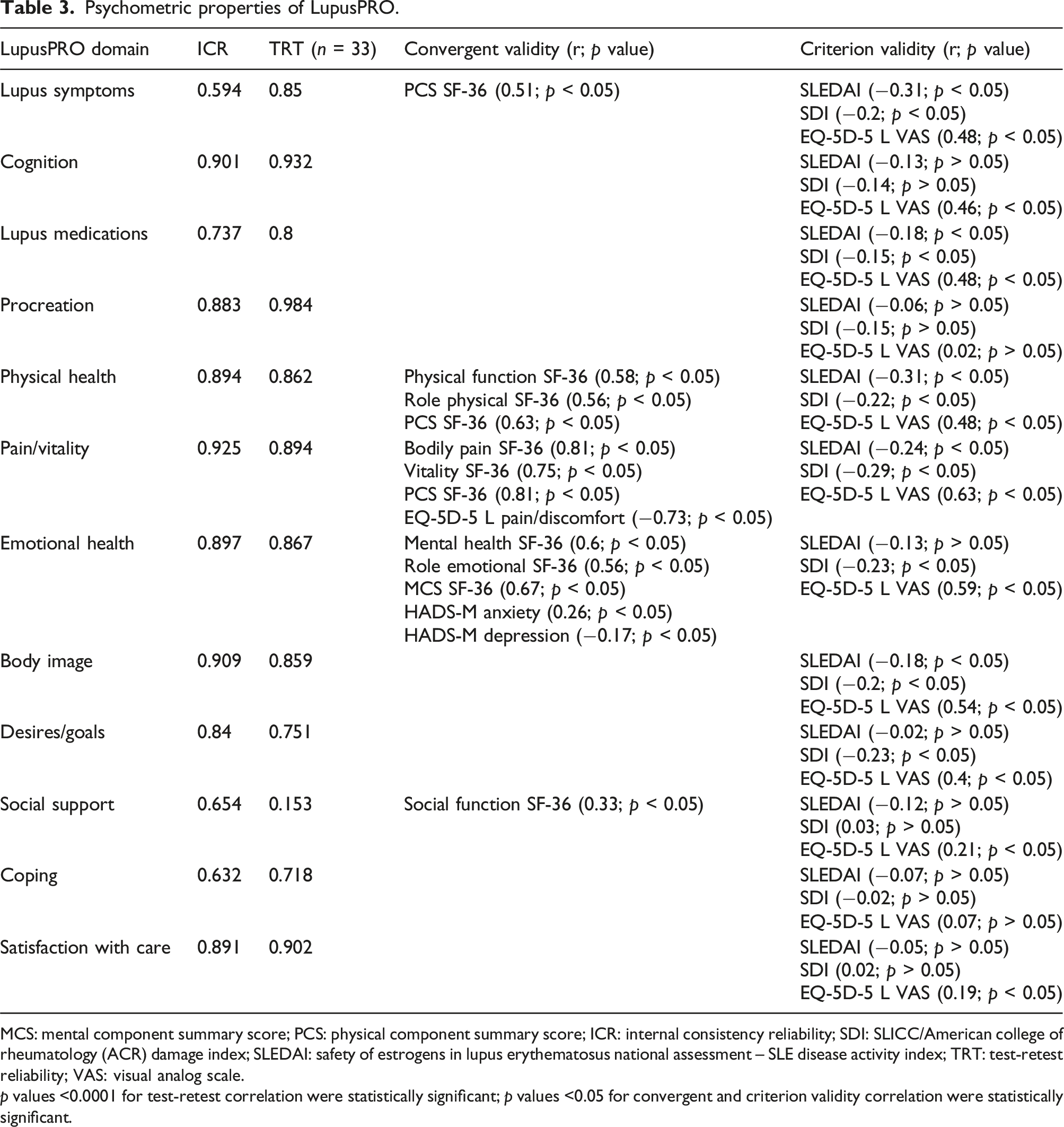
MCS: mental component summary score; PCS: physical component summary score; ICR: internal consistency reliability; SDI: SLICC/American college of rheumatology (ACR) damage index; SLEDAI: safety of estrogens in lupus erythematosus national assessment – SLE disease activity index; TRT: test-retest reliability; VAS: visual analog scale.
p values <0.0001 for test-retest correlation were statistically significant; p values <0.05 for convergent and criterion validity correlation were statistically significant.
Confirmatory factor analysis of LupusPRO.
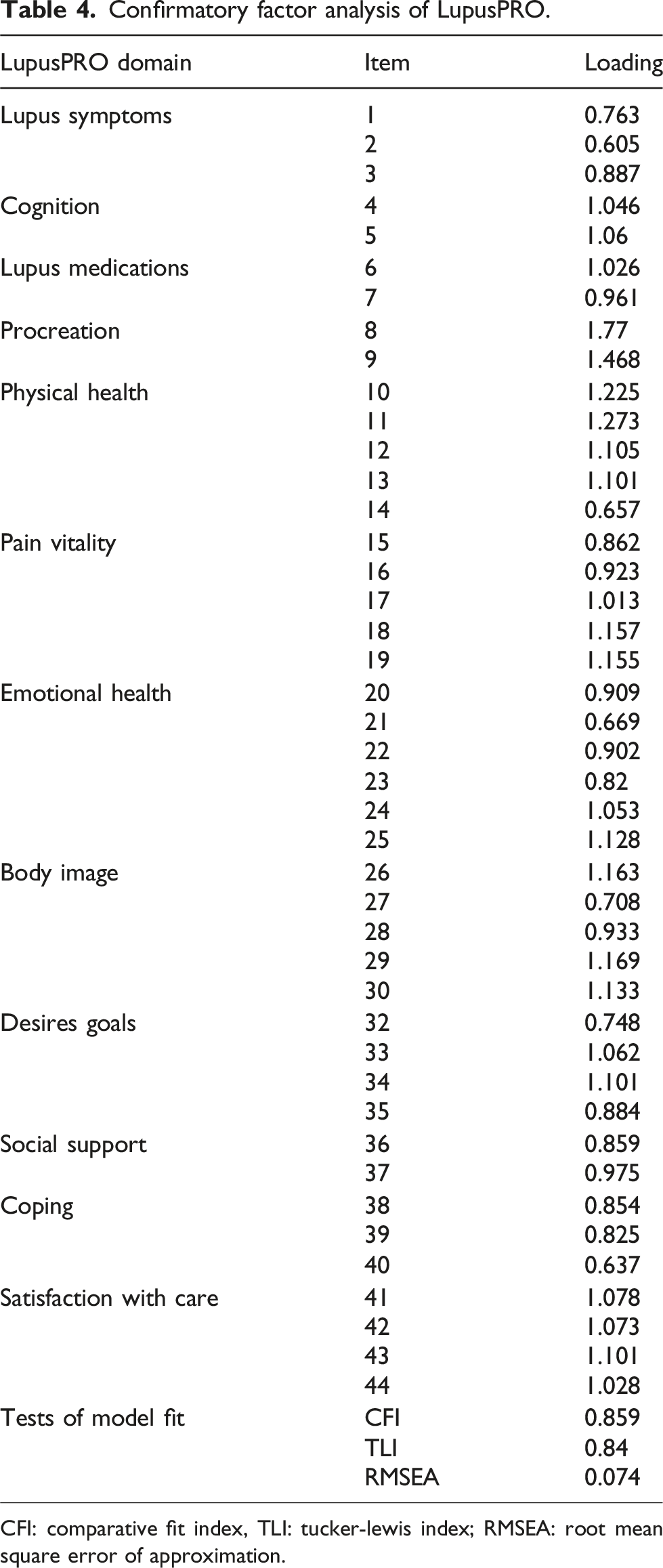
CFI: comparative fit index, TLI: tucker-lewis index; RMSEA: root mean square error of approximation.
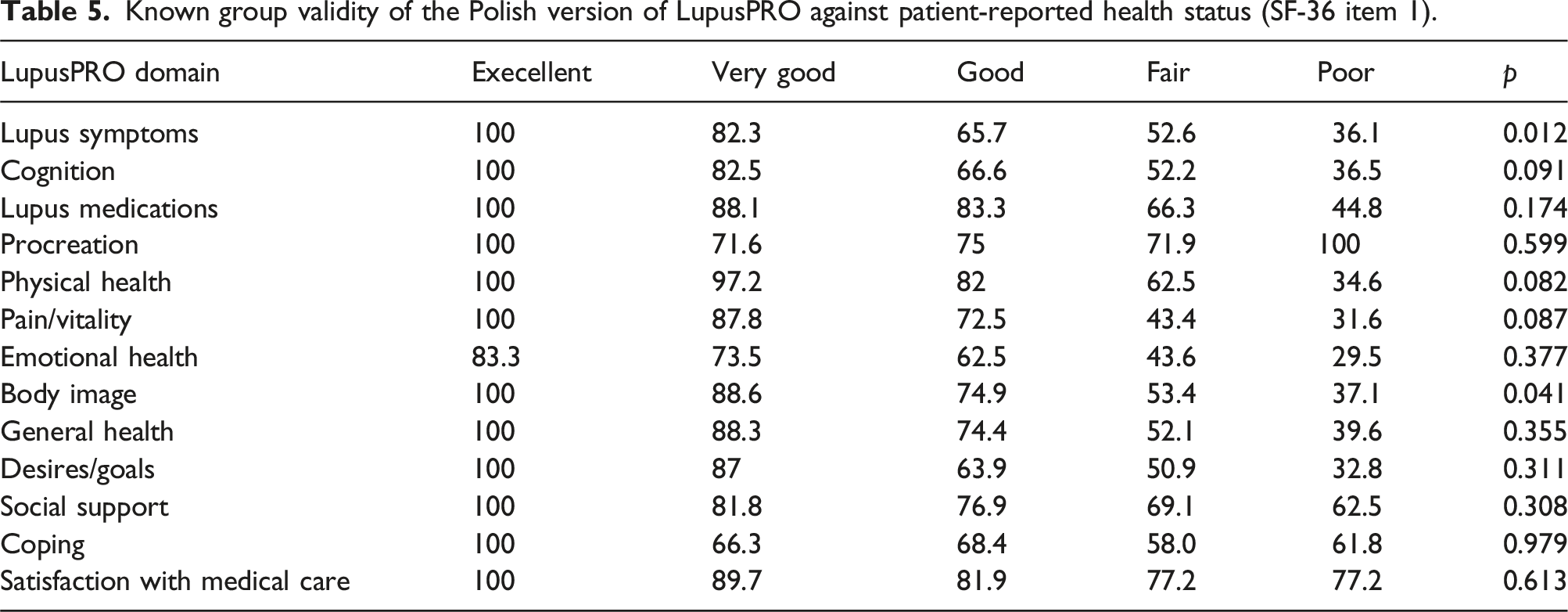
Known group validity of the Polish version of LupusPRO against patient-reported health status (SF-36 item 1).
Known group validity of the polish version of LupusPRO against disease activity by high (≥4) and low (<4) SLEDAI level.
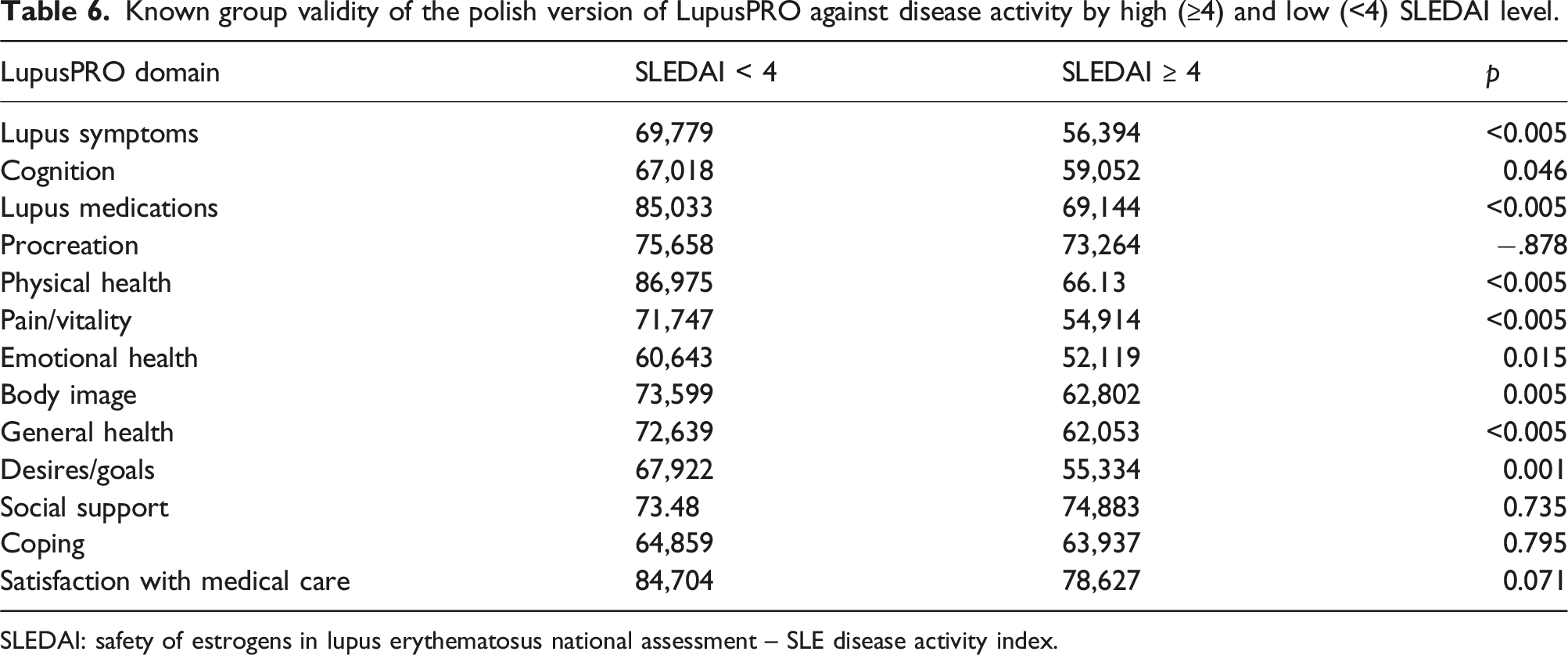
SLEDAI: safety of estrogens in lupus erythematosus national assessment – SLE disease activity index.
Discussion
The complexity of the clinical picture of SLE means that the disease affects various aspects of a patient’s life. Even reasonable control of the disease process is not always reflected in a high quality of life for patients. For this reason, it is vital that the medical care of patients with SLE - in addition to monitoring indicators of clinical disease activity - should also include an assessment of the quality of life, which is a subjective perception of one’s situation in the face of life conditions, including the disease. Failure to take this parameter into account may result in an inadequate grasp of the essence of the patient’s problem and, consequently, result in a lower effectiveness of the overall therapeutic process. In Poland, so far, there have been no linguistically and culturally adapted specific questionnaires available, which has made it difficult for physicians caring for SLE patients to obtain information about their quality of life in accordance with international standards. The Polish version of LupusPRO was cross-culturally adapted and validated. The scores of the individual domains of the Polish version of LupusPRO oscillated between 55.67 and 81.08, which allows us to conclude that the quality of life of the particular dimensions is reduced but is above the average index of possible scores in the questionnaire. The lowest scores were recorded in the Emotional Problems domain, followed by Desires/Goals and Pain/Vitality. The Emotional Problems domain was among the lowest-scoring domains in the other six published LupusPRO validations.13,15,17,18,20,23 Emotional disturbances are a leading cause of life impairment in SLE patients. 34 They occur twice as often as in the general population. 35 At the same time, the literature on the subject indicates frequent omission by attending physicians of the diagnosis of psychiatric disorders of patients.36,37 This problem requires greater attention and implementation of appropriate procedures into everyday clinical practice. The Polish versions of LupusPRO includes proper results of ceiling and floor effects. Only one borderline results concerning ceiling effects was found in the domain of Cognition. In the study, the Polish version of LupusPRO demonstrated good reliability. The ICR was reliable for most domains. Unsatisfactory ICR results were registered in three domains: Lupus symptoms, Social support, and Coping skills. This may be a result of some limitations of using alpha-Cronbach’s alpha - the small number of items in the test may underestimate its value. 38 A lower ICR was observed in original LupusPRO and its language versions and it was associated with the exact domains: Lupus Symptoms15–17,19–21 Lupus Treatment,13,16,17 Social Support17,23,26 and Coping Skills.16,19 Each of these contains a small number of items - two or three. In contrast, there was no low ICR in the domains consisting of more issues (four, five, and six issues), which supports the idea that ICR is influenced by the limitations of the alpha-Cronbach’s rule. On the other hand, a lower ICR score indicates a weak correlation between issues, which consequently supports the measurement of different constructs. The Social Support domain assesses whether the patient received sufficient help from family and friends. Poles may treat these social groups differently, 39 suggesting some dissociation between the expectation of receiving support from family and friends. A similar pattern was observed in the Coping Skills and Lupus Symptoms domains, where issues included in the domains assessed different constructs. The results of the TRT was satisfactory. One of the main limitations of using TRT is the lack of specification proper, optimal time interval. 40 Several publications have narrowed the reassessment time for a period from 2 days to 4 weeks41–43 although there are no clear guidelines indicating the optimal time interval. The results of convergent validity of the corresponding domains of the Polish version of LupusPRO and SF-36 showed a strong correlation, as in other studies.13,14,18–21,23 The correlation between the corresponding domains of the Polish version of LupusPRO questionnaire and the HADS-M scale was weak. The reason could be that both subscales of the HADS-M only address selected issues of the analyzed domain of the Polish version of LupusPRO questionnaire. Moreover, the HADS-M scale is not a questionnaire for assessing the quality of life but a method for identifying selected psychiatric disorders. The poor correlation may be related to the fact that the two tools measure different constructs. We also noted weak but statistically significant correlations between domains of Polish LupusPRO and measures of disease activity and damage (except for domains Lupus symptoms and Physical Health) which demonstrates criterion validity. A certain limitation of the study is that the impact of fibromalgia was not examined although previous studies reported its influence on HRQoL. 44 In conclusion, the assessment of psychometric properties of the Polish LupusPRO showed satisfactory reliability and validity among polish patients with SLE. Evaluation of the quality of life in the Polish population of patients with SLE revealed deficits in the mental sphere.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of the article.