
Abstract
Background and Objectives
Pulmonary diseases (PD) are common in Systemic Lupus Erythematosus (SLE) and associated with increased mortality and decreased health-related quality of life, but no study has so far addressed PD in newly diagnosed patients with SLE. Our objectives were among newly diagnosed patients with SLE to investigate: Primarily, if PD and subtypes of PD are present, and secondarily characterise the patients by means of (i) lung physiology, (ii) radiology, (iii) thoracic ultrasound (TUS) and diaphragmatic ultrasound (DUS).
Methods
Patients newly diagnosed with SLE from 1st July 2023 to 31st July 2024 at Odense University Hospital, Odense, Denmark, underwent a dedicated clinical evaluation for PD, including pulmonary function tests (PFT), chest high-resolution computed tomography or computed tomography scan alongside with TUS and DUS. Subsequently, PD were diagnosed, and subtype was categorised on a multidisciplinary discussion.
Results
Ten participants were included in average 3 months after SLE diagnosis, and six out of ten had PD. PD included one case of shrinking lung syndrome (SLS) and two cases of interstitial lung disease. All participants exhibited at least one abnormal PFT measure, with some showing severely reduced pulmonary function. TUS was associated with diseases of the lung parenchyma and pleura and DUS with SLS.
Conclusion
We found PD among newly diagnosed patients with SLE and in some cases associated with severely affected pulmonary function. TUS and DUS may contribute with information in diagnosing SLE related PD, but further studies are needed.
Background
Systemic lupus erythematosus (SLE) is an autoimmune disease defined by the presence of specific autoantibodies and characteristic involvement of multiple organs. 1 Typical non-infectious and non-malignant pulmonary diseases (PD) in SLE are interstitial lung diseases (ILD), pleural diseases, airway diseases, pulmonary hypertension (PH), thromboembolism, and shrinking lung syndrome (SLS). 2 PD in SLE are associated with mortality 3 and lower health-related quality of life 4 and, importantly, the clinical manifestations of several PD measured as decreased pulmonary function may improve among patients with SLE with suitable treatment.5,6
Pulmonary diseases (PD) are common in SLE and estimated to be present in approximately half of the patients with SLE. 2 PD in SLE have been studied predominantly in patients with longstanding disease with duration means/medians ranging from few years to more than ten years.7–10 However, Habib et al have investigated PD among patients with SLE with a mean of 20 months disease duration and found that PD were prevalent in 45% in whom 9.5% had ILD. 11 No clinical observational studies have investigated PD in patients newly diagnosed with SLE, to our knowledge.
The diagnosis of PD can be cumbersome because symptoms may be absent or range from vague to severe, 2 therefore, systematic examination using diagnostic tools with high accuracy seems important. Thoracic ultrasound (TUS), with focus on B-lines and abnormal pleural line, shows promise in identifying ILD among patients with rheumatic diseases,12–14 still, there are only few reports on TUS in SLE. 12 Diaphragmatic ultrasound (DUS) abnormalities, such as decreased diaphragmatic excursion (DE) and decreased diaphragmatic thickness, have been associated with decreased pulmonary function in SLE, 15 but to our knowledge, it has not been studied among patients newly diagnosed with SLE. In the present study the term PD covers non-malignant diseases of the parenchyma, pleura, airways, diaphragm, and pulmonary vasculature.
The primary objective of this cross-sectional study was to describe if PD and subtypes of PD are present among newly diagnosed patients with SLE. The secondary objectives were among patients newly diagnosed with SLE to characterise them by means of: (i) lung physiology, (ii) chest high resolution computed tomography scan (HRCT), (iii) TUS and DUS.
Methods
Summary of the project methods
Participants newly diagnosed with SLE underwent a one-day visit where the investigations described below were performed. These investigations were done within 3 months on average from SLE diagnosis. Before the visit the participants’ medical records were reviewed to register prespecified disease manifestations focusing on SLE, PD, cardiac diseases, anti-phospholipid syndrome (APS), and biomarkers. On the visit day participants underwent: Clinical examination, blood and urine sampling, TUS, DUS, PFT, and HRCT. Afterwards HRCT were described, and finally, PD were diagnosed at a multidisciplinary discussion (MDD) involving experienced pulmonologists, a thoracic radiologist, and a rheumatologists. The study is reported according to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline 16 (Checklist Supplemental Material A).
Study population and inclusion
We invited all newly diagnosed patients with SLE at a tertiary rheumatological referral centre at the Department of Rheumatology, Odense University Hospital, Denmark, between 1st July 2023 and 31st July 2024. We included all who accepted invitation after informed consent. SLE was diagnosed according to Fries and Holman’s diagnostic principle 17 and classified using the EULAR/ACR 2019 classification criteria for SLE. 18
Data handling
All data were pseudonymised and stored in a Research Electronic Data Capture (REDCap) database.
Data collection
Outpatient clinic visit
At the visit the participants’ medical history of SLE was revised, routine blood samples including, presence of anti-double stranded DNA and levels of complement C3 and C4 were analysed. The SLE disease activity was evaluated according to the disease activity score Systemic Lupus Erythematosus Disease Activity index 2000 (SLEDAI-2K). 19 The scores of SLEDAI-2K are presented both with and without contributions from PD. SLE related damage was registered corresponding to Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index for systemic lupus erythematosus (SDI) 20 definition of damage, if it would be sustained for 6 months. We noted if participants had following signs and symptoms: Rales, effusion, friction rubs, dullness of lower zones, cyanosis, clubbing, dry cough, frequent respiratory tract infections (RIT), prior hospitalisation due to RIT, and a sensation of tightness in the chest. We reviewed medical records regarding findings of the latest chest X-ray (CXR), and noted description and time between examination and visit day.
Pulmonary function tests (PFT)
Participants performed PFT according to current guidelines guided by a nurse experienced in respiratory medicine.21–24 The nurse was blinded to other clinical data, including diagnose of PD, HRCT, TUS, DUS, information from clinical visit ect. Before PFT, participants were asked about their feeling of breathlessness according to the Medical Research Council breathlessness scale (MRC). 25 From the PFT we report Forced Expiratory Volume in one second (FEV1), Forced Vital Capacity (FVC), The FEV1/FVC ratio, Total Lung Capacity (TLC), Diffusing Capacity for the Lung for Carbon Monoxide (DLCO), and Carbon Monoxide Transfer Coefficient (KCO). Six-minute walk test (6MWT) was performed according to guidelines 21 and oxygen saturation and distance walk were noted. Results were compared to reference values according to age, height, ethnicity, and sex. Results below 80% were regarded as abnormal, except for FEV1/FVC ratio where the threshold was below 70%.
Chest computed tomography scans
HRCT were performed on the visit day on a Revolution CT; General Electric Company; Boston, Massachusetts, USA. Acquisition parameters of the diagnostic end-inspiratory scanning are collimation 8 cm, kV 120, SmartmA (140–900 mA), Noise Index 25, Pitch 0.5, Rotation time 0.35 s, Asir-V 40%. Images were reconstructed using a 1024 × 1024 matrix and chest algorithm. Axial slice thickness is 0.625 mm. Image overlap 20%. Almost identical acquisition parameters were used for the low-dose end-expiratory scanning. However, noise index was raised to 30. End-expiratory images were reconstructed using a standard algorithm. A single axial series was reconstructed. Slice thickness was 2.5 mm. All examinations were assessed on Vue PACS; Koninklijke Philips N.V., Amsterdam, The Netherlands. If a Chest Computed Tomography (CT) or a HRCT, of a sufficient quality, were performed after SLE diagnosis and within 6 months of the visit day it was used, and no new scan was performed. The scans were described after the visit day by an experienced thoracic radiologist, blinded to other results, and registering results in a predefined REDCap database.
Diagnoses of pulmonary diseases
At MDD involving experienced pulmonologists, a thoracic radiologist, and a rheumatologist the presence of PD was evaluated and subsequently subcategorised according to PD subtype. All were blinded to TUS and DUS.
Thoracic and diaphragmic ultrasound (TUS and DUS)
All scans were performed by HL with a Hitachi Arietta v70 machine, software version 3.0.2., using a convex transducer (C251) 1-5 mHz or a linear transducer (L64) 5-18 mHZ. The US machine was programmed with pulmonary settings: Dept 10 cm, focus 2 cm, compound settings and Harmonics were deactivated, then each clip was optimised by HL. Participants were scanned in a sitting position according to a 14-zone protocol recommended by the European Respiratory Society
26
saving 8 seconds video clips from each zone in B-mode. The clips were later evaluated for B-lines, abnormalities of the visceral pleura, and thickening parietal pleura by HL. B-lines were defined as vertical lines from the pleura and to the bottom of the picture, moving synchronously with the pleural movement; abnormalities of the visceral pleura was defined as irregularities in the otherwise smooth hyperechoic pleura line; thickened parietal pleura was defined as a hypoechoic line superficial from the visceral pleura, examples are shown in Figure 1. We chose a threshold of ≥10 B-lines to indicate abnormal lung interstitium, which has proven to detect ILD in a similar approach among participants with Rheumatoid Arthritis (RA).
13
TUS clips showing normal pleura, B-lines, and pleural abnormalities of 10 newly diagnosed patients with SLE. Arrow indicates pathology. (a) – normal pleura and lung parenchyma presentation; (b) - multiple B-lines; (c) – abnormality in visceral pleura; (d) –thickening of parietal pleura.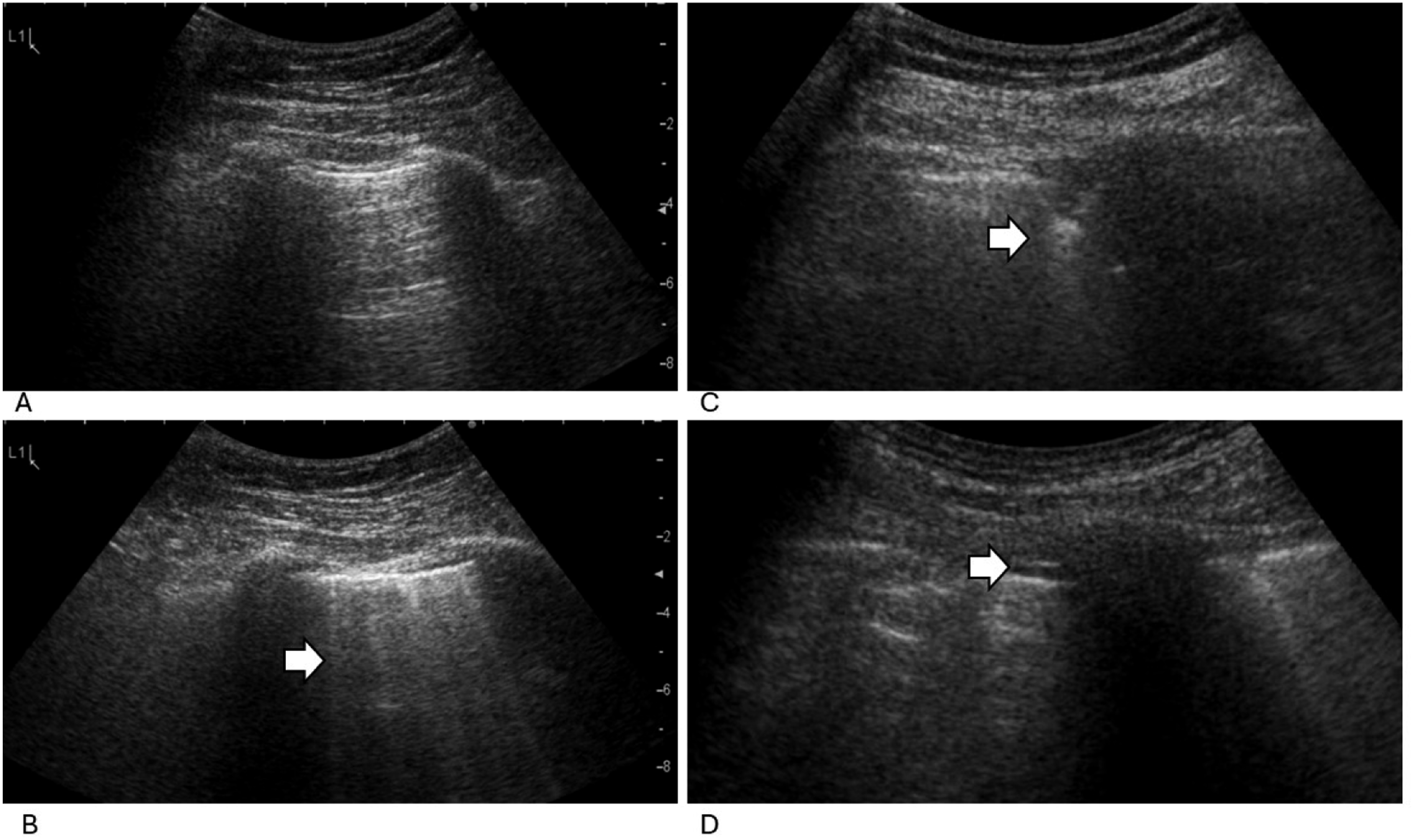
Additionally, the DE was assessed with the convex transducer at right side in a subcostal midclavicular view at quiet (DEq) and deep (DEd) inspiration. DE was done in M-mode while the participants were sitting in an approximately 45° angle as previously described.26,27 If the window was not optimal HL moved the transducer cranially using intercostal spaces as acoustic windows. We chose the normal value minus standard deviation proposed by Boussuges et al. as threshold to discriminate between normal and abnormal,
28
therefore, the threshold for DEq was 1.4 cm for females and 1.5 cm for males and the threshold for DEd was 5.9 for females and 6.6 for males. The thickness of the diaphragm was measured with the linear transducer at right side in the midaxillary line above costa 8 to 10 and afterwards moved cranial or caudal to find the optimal location with participants sitting upright in M-mode as previously described.26,29 We report the diaphragmatic thickness at inspiration (DTinsp) and the diaphragmatic thickness fraction (DTF) (DTF = (DTinsp – DTekspiration)/DTekspiration), examples are shown in Figure 2. We chose a thickness 1.6 mm as lower limit for normal inspiration thickness based on the mean minus standard deviation among Turkish patients with SLE,
15
and we chose 30% as threshold for abnormal DTF as proposed.
29
TUS and DUS were performed prior to the other investigations but after HL had read the participants’ medical record, why HL was only partly blinded to the participants status of PD. DUS clips in M-mode showing movement and thickness of the diaphragm among 10 newly diagnosed patients with SLE. Black lines indicates where distances were measured. (a) – Normal movement of diaphragm at quiet breathing (Diaphragmatic excursion (DE)); (b) – Abnormal movement of diaphragm at quiet breathing (DE); (c) – Normal movement of diaphragm at deep breathing (DE); (d) – Abnormal movement of diaphragm at deep breathing (DE); (e) − Diaphragmatic thickness (DTinsp) with normal thickness fraction (DTF); (f) – Diaphragmatic thickness (DTinsp) with abnormal thickness fraction (DTF).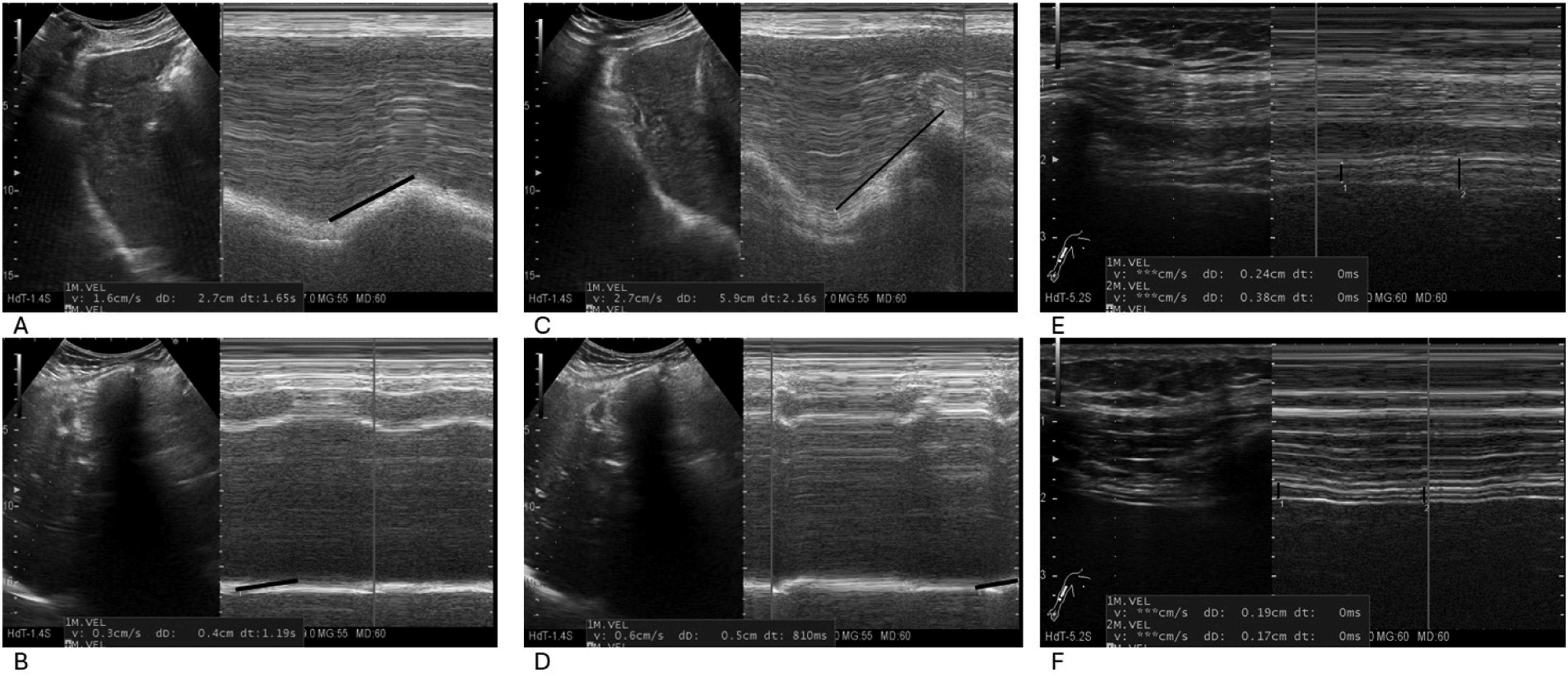
Ethics and registration
The study was approved by the local ethics committee (project ID S20210164) and by the local data protection authority (23/22,079). Before the study two patient partners have read the protocol, commented it, and participated in a project day. One patient partner has reviewed the final manuscript.
Data analysis
As the present exploratory study included a sample of 10 participants, we chose to perform only descriptive statistics. We summarise categorical outcomes and present numbers and percentages. Continuous variables are presented as a mean and standard deviation (SD) if normally distributed otherwise with median and interquartile range (IQR). Normal distribution was evaluated with Shapiro-Wilk test (p-value >.05 was regarded as a sign of normal distribution) and subsequently we evaluated the data’s distribution visually with histograms.
Results
Characteristics of participants and PD
Overview of prevalent PD and clinical characteristics among 10 patients newly diagnosed with SLE. Baseline characteristics, treatment, and SLE related outcomes are reported.
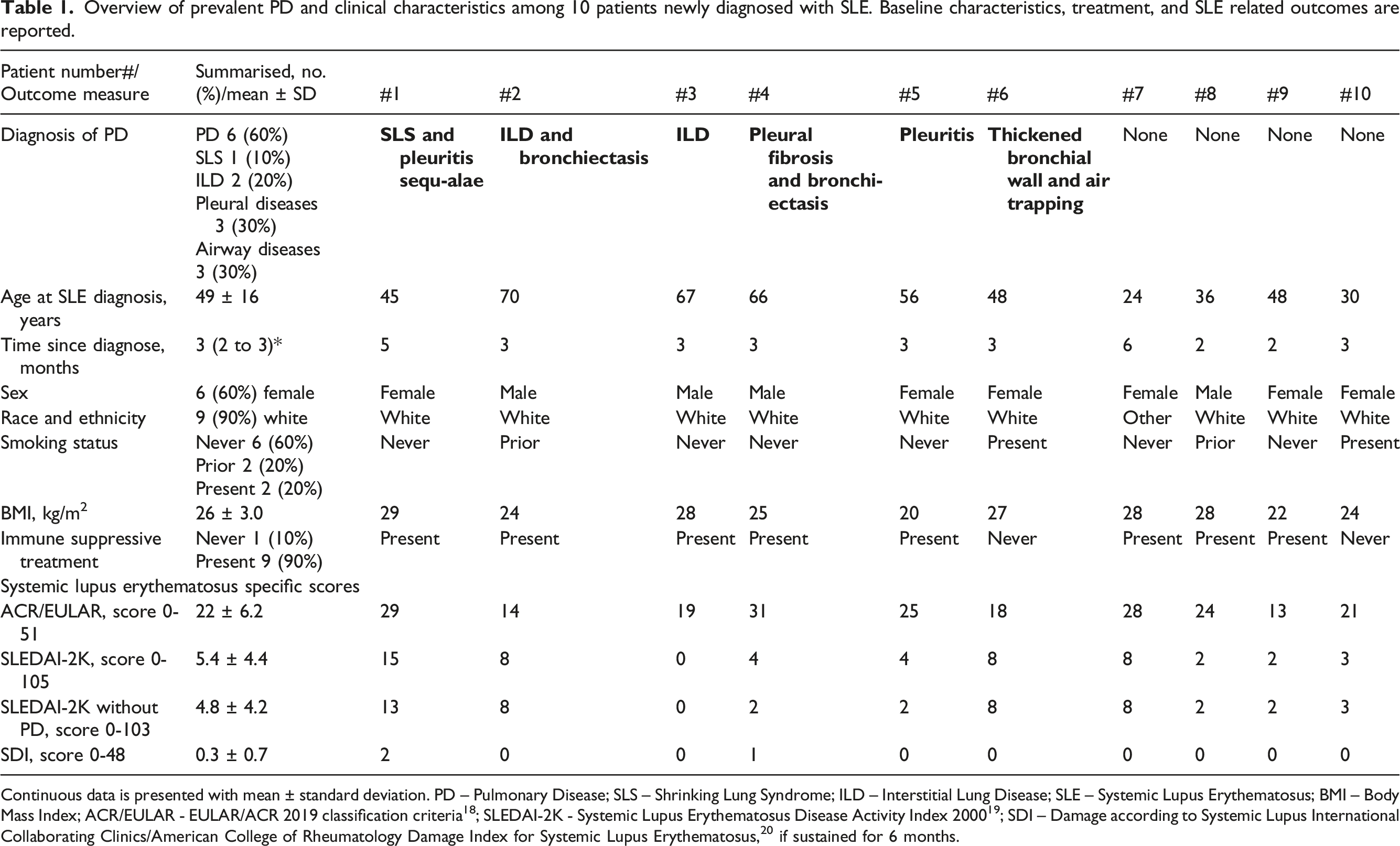
Continuous data is presented with mean ± standard deviation. PD – Pulmonary Disease; SLS – Shrinking Lung Syndrome; ILD – Interstitial Lung Disease; SLE – Systemic Lupus Erythematosus; BMI – Body Mass Index; ACR/EULAR - EULAR/ACR 2019 classification criteria 18 ; SLEDAI-2K - Systemic Lupus Erythematosus Disease Activity Index 2000 19 ; SDI – Damage according to Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index for Systemic Lupus Erythematosus, 20 if sustained for 6 months.
Clinical manifestations and chest X-ray (CXR)
Participants had few clinical symptoms related to their PD (Appendix 1). All participants with effusions had PD, and most commonly pleural diseases. Three had dullness of lower zones at auscultation and had prior been hospitalised for RIT, all had pleural diseases. CXR were described abnormal in four participants and without abnormalities in five, and one had never had an CXR. All abnormal CXR were among participants with PD, however, two participants with a without abnormalities CXR had PD, and CXR overlooked diagnoses of PD compared to HRCT.
Pulmonary function tests (PFT)
Diagnosis of PD and results of PFT among 10 patients newly diagnosed with SLE.
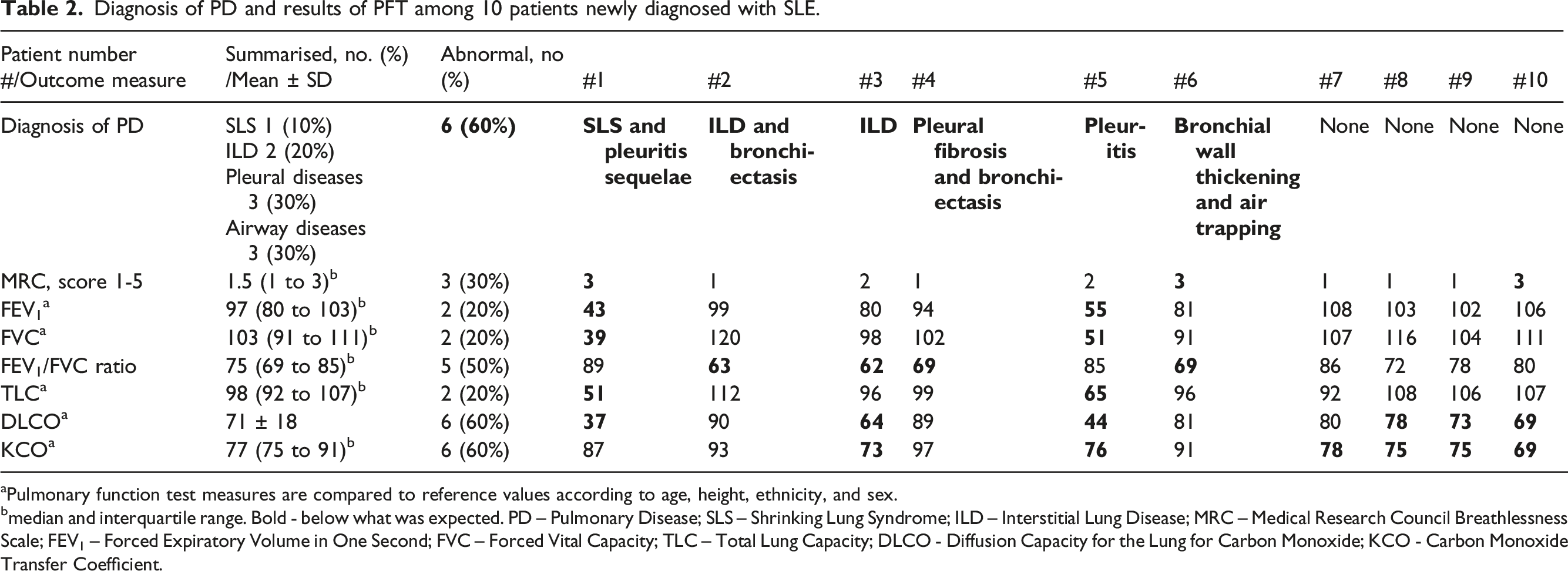
aPulmonary function test measures are compared to reference values according to age, height, ethnicity, and sex.
bmedian and interquartile range. Bold - below what was expected. PD – Pulmonary Disease; SLS – Shrinking Lung Syndrome; ILD – Interstitial Lung Disease; MRC – Medical Research Council Breathlessness Scale; FEV1 – Forced Expiratory Volume in One Second; FVC – Forced Vital Capacity; TLC – Total Lung Capacity; DLCO - Diffusion Capacity for the Lung for Carbon Monoxide; KCO - Carbon Monoxide Transfer Coefficient.
Chest computed tomography (CT) scans
PD according to CT scans of the thorax of among 10 patients newly diagnosed with SLE.
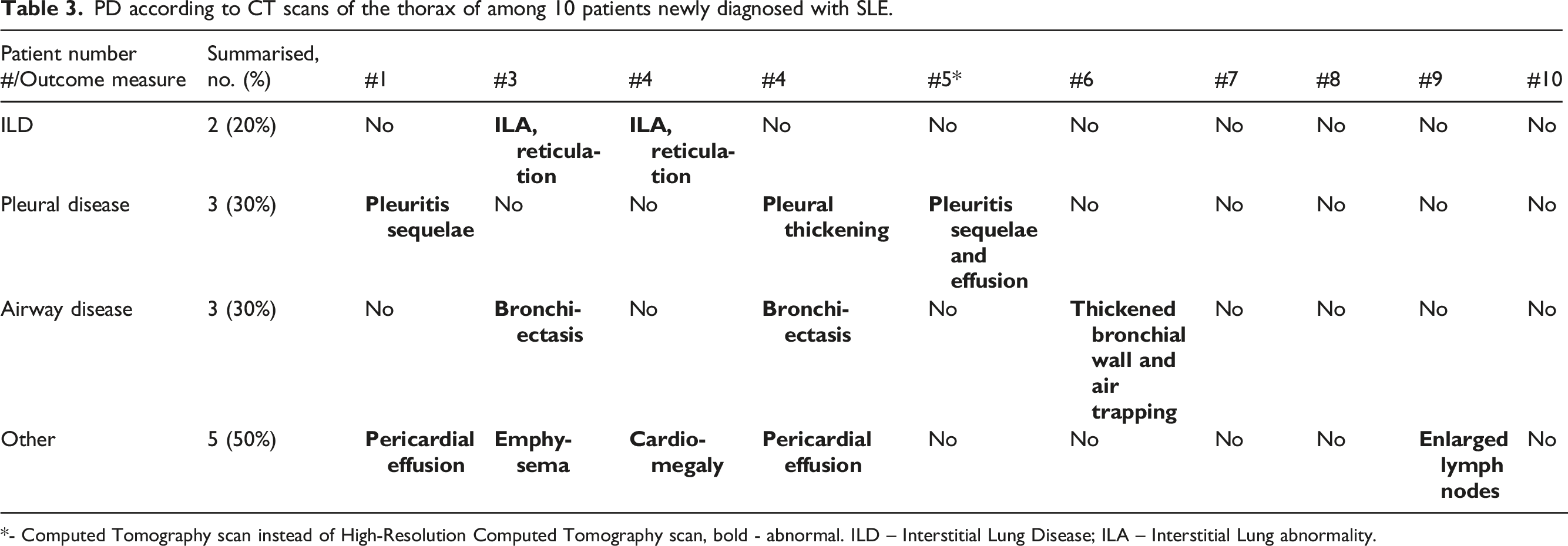
*- Computed Tomography scan instead of High-Resolution Computed Tomography scan, bold - abnormal. ILD – Interstitial Lung Disease; ILA – Interstitial Lung abnormality.
Thoracic- and diaphragmic ultrasound (TUS and DUS)
Presence of PD and findings on TUS and DUS among 10 patients newly diagnosed with SLE.
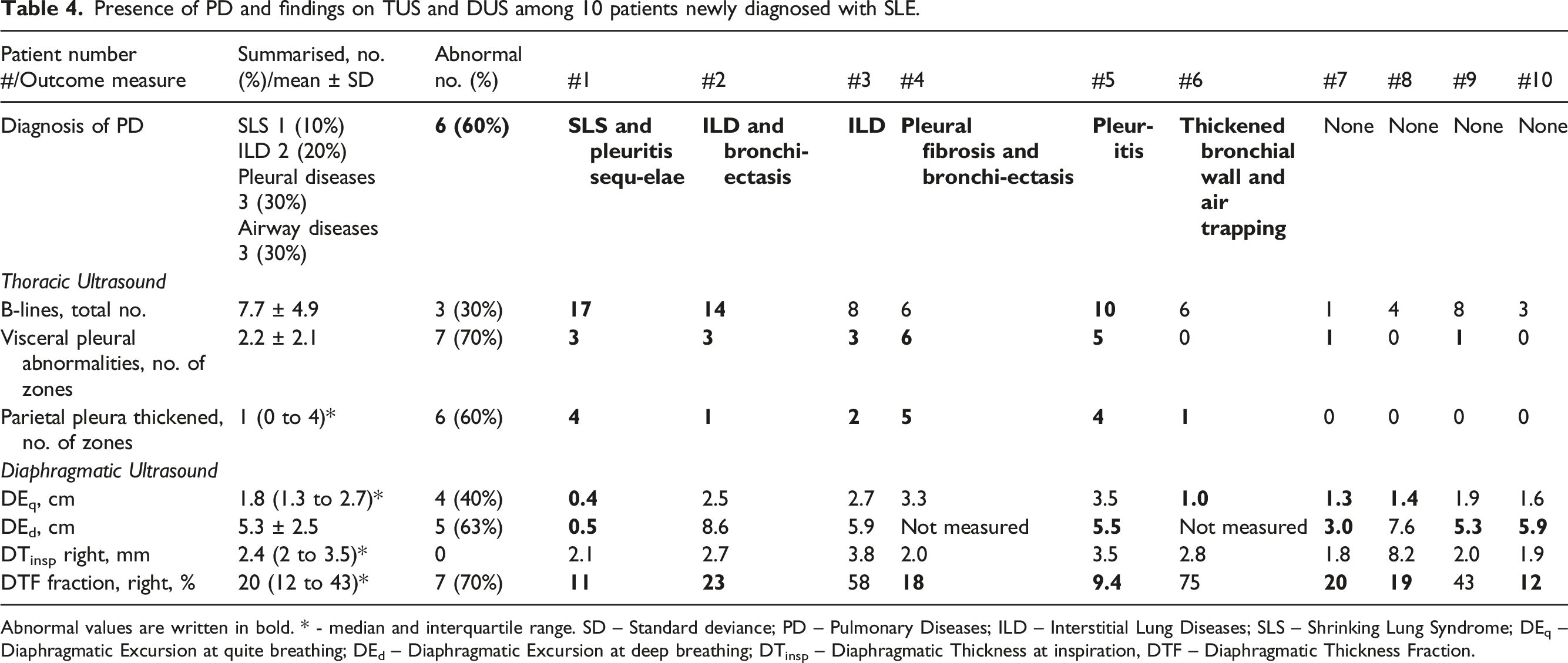
Abnormal values are written in bold. * - median and interquartile range. SD – Standard deviance; PD – Pulmonary Diseases; ILD – Interstitial Lung Diseases; SLS – Shrinking Lung Syndrome; DEq – Diaphragmatic Excursion at quite breathing; DEd – Diaphragmatic Excursion at deep breathing; DTinsp – Diaphragmatic Thickness at inspiration, DTF – Diaphragmatic Thickness Fraction.
DUS demonstrated severely decreased DE in one participant who was later diagnosed with SLS, and where a reduced DEd was most evident. Several participants had an abnormally low DE, no participants had an abnormal DTinsp, and 70% had an abnormal DTF. The two participants with the most abnormal DTF were later diagnosed with a PD (SLS with sequelae of pleuritis and pleuritis) and had the most decreased FVC. Results of DUS are shown in Table 4 and examples of different DUS measures are shown in Figure 2.
Discussion
Main findings
To our knowledge, this is the first clinical observational study that describes PD among newly diagnosed patients with SLE. We included 10 participants and six had PD with different combinations of parenchymal, pleural, and airway affection, including ILD and SLS, Table 1. All participants had at least one decreased pulmonary function measure, and, in some cases, pulmonary function was severely decreased, Table 2. Descriptions of chest CT and HRCT scans were closely associated with the diagnosis of PD, Table 3. Abnormal TUS were seen in patients with PD with primarily parenchymal and pleural disease and abnormal DUS was most prominent in a patient with SLS, Table 4. However, we included only 10 participants, why our results must be interpreted with this limitation in mind.
Few studies have evaluated the prevalence of all PD in SLE, but according to expert opinion approximately half of all patients with SLE have PD.2,31 Interestingly, the prevalence of PD applied to newly diagnosed patients with SLE in the present study. Our results indicate that SLE possibly manifests with PD early in the disease course. Our findings are supported by results by Habib et al.’s, who reported PD in 45% of patients with SLE and less than 2 years of disease duration. 11 However, our results are based on 10 participants, why the prevalence needs investigation in larger study populations, and our results are hypothesis-generating.
SLS is considered to affect 2% to 10% of patients with SLE,2,10,32 and even more patients with dyspnoea. 8 In the present study we identified one patient with SLS, characterised by a reduced and restrictive ventilation capacity, but with unaffected diffusion indicated by normal KCO. We show that SLS can develop among newly diagnosed patients with SLE, despite SLS mostly develops in patients with SLE after several years of disease duration. 6
We identified two participants with ILD. One systematic review claims the prevalence of SLE related ILD is 6%. 33 However, the systematic review did not include several relevant studies, that report a higher prevalence of SLE related ILD.9,34 We show that ILD can occur among patients newly diagnosed with SLE, corresponding to with findings of Habib et al. who found ILD among 9.5% of patients with SLE and short disease duration. 11
Three participants had pleural diseases, Table 1. If these pleural abnormalities are still evident after 6 months two will be classified as damage according to SDI. 20 Furthermore, the pleural diseases were associated with decreased pulmonary function, Table 2. Pleuritis is thought to be prevalent in 30-50% of patients with SLE. 2 We show that pleuritis may occur among patients newly diagnosed with SLE, and in some might lead to reduced pulmonary function and damage according to SDI.
Airway diseases are estimated to affect 20% of patients with SLE, 2 but apparently airway diseases draw little attention, illustrated by the absence of literature reviews addressing lower airway diseases among patients with SLE and/or CTD. We found airway diseases among newly diagnosed patients with SLE, Table 1, which indicates that airway diseases might be present at the debut of SLE.
We found it difficult to diagnose PD based on information obtained in the outpatient clinic visit. It seems that prior effusions, dullness of lower lobes at auscultation, and a prior abnormal CXR should increase awareness of PD, especially pleural diseases. Our results indicate that patients with one or more of the above-mentioned findings may benefit from a HRCT.
PFT were abnormal in all participants, Table 2. The participants who had tests indicating a restrictive pattern had pleural diseases, and obstruction was often related to airway diseases. However, decreased diffusion was the most common PFT abnormality even in the absence of PD. Prior studies have shown, that abnormally decreased spirometry and diffusion measures are common in SLE, also in the absence of PD.7,35–37 This suggests that SLE may affect the lungs even without structural changes are visible on HRCT. DLCO can be decreased for several reasons including ILD, PH, and pulmonary embolies (PE). 38 We find it unlikely that three out of four with a decreased DLCO or KCO and without PD had PE or PH, because the prevalence of PH and PE are reported to be less than 10% in SLE, 2 and the HRCT showed no evidence of PH in these participants. We speculate if endothelial dysfunction contributes to the decreased DLCO, as higher levels of cytokines associated with endothelial dysfunction are prevalent in both patients with SLE 39 and in some patients with decreased DLCO. 40 6MWT were mostly normal regarding saturation, while distance was reduced in several cases without being associated with PD, Appendix 1. This indicates that 6MWT might not identify PD among newly diagnosed patients with SLE, however, this needs to be confirmed in larger studies.
CT and HRCT descriptions related closely to the final diagnosis of PD in this study. We believe that this indicates that evaluation involving CT or HRCT are necessary for a thorough evaluation of PD in SLE. We acknowledge that CT and HRCT may be inaccessible 41 and exposes patients to unwanted radiation. 42 Therefore, diagnostic tools that are reliable, accessible, radiation free, and of low cost are warranted as upfront identification or screening for SLE-related PD.
TUS is increasingly being investigated as a tool to identify ILD among patients with CTD 12 and RA, 13 however, no internationally accepted protocol including firm definitions of ILD affections within CTD-ILD exists. We defined an abnormal TUS as the presence of ≥10 B-lines, indicating involvement of the lung interstitium. In our study 30% of the participants exhibited an abnormal number of B-lines and all had PD, Table 4. In patients with other CTDs pleural abnormalities are associated with ILD.13,14 Among the present patients the majority had abnormalities in at least one zone of the visceral pleura regardless of PD or not. When applying a threshold of 2 ≥ zones with abnormalities in the visceral pleura we identified all participants with parenchymal or pleural disease and excluded those without. The parietal pleura can be evaluated with TUS, 26 but has not been evaluated among patients with CTD, to our knowledge. Evaluation of the parietal pleura performed surprisingly well, as all participants without PD did not have any thickening of their parietal pleura and all participants with thickened parietal pleura in at least one zone had a PD. Furthermore, all three participants with thickening of parietal pleura in ≥2 zones had pleural disease, Table 4. Even though the results seem promising in this pilot study among 10 SLE patients, the clinical utility of TUS needs to be confirmed in larger studies.
To our knowledge, there is limited research on DUS in patients with CTD, and there are no widely accepted criteria for differentiating normal from abnormal DUS findings. However, DUS abnormalities have been linked to dyspnea and SLS in a study of patients with SLE and in a case report.15,43 We found DUS identified one participant with a clearly abnormal DUS, especially regarding DE, and the participant had SLS. Other participants had an abnormally DE without an obvious association with PD or abnormal PFT measures. Several participants had decreased DTF but the findings did not seem associated to PD or decreased pulmonary function. Our results indicate that DUS might be used for diagnosing SLS, but this finding needs to be confirmed in other studies. 44
Strength and limitations
The study had several strengths. The participants were consecutive patients with SLE from an out-patient clinic, diagnosed with SLE according to current classification criteria. 18 Two patients declined the invitation but did not differ from the study population regarding sex and age. The participants underwent a thorough and dedicated diagnostic work-up PD including a MDD with participation of experienced personal, which is considered gold standard for diagnosis of ILD. 45 However, the study only included 10 participants, which makes it possible, that findings were due to chance, and makes it difficult drawing conclusions. 40% of the study participants were men, which is a larger proportion than in other SLE populations, 46 and because PD is more common among males than females with SLE 47 it could make PD more prevalent in this study. This must be kept in mind before applying our results to other newly diagnosed patients with SLE. The association between TUS and DUS and PD was investigated in 10 participants, why we regard the results as hypothesis-generating.
Perspective
PD can occur among newly diagnosed patients with SLE, and PD may affect most structures of the lung including the parenchyma, pleura, and airways. We believe, that it is important to subdivide PD into different categories, as different treatment approaches are necessary in different subtypes of PD in SLE.6,30,31,48,49 We found it difficult to diagnose and categorise PD without chest CT or HRCT, however TUS and DUS seem promising in this pilot study.
Conclusion
This is the first dedicated clinical observational study to investigate PD among patients with SLE and few months of disease duration. We observed that PD can appear and might be severe already at diagnosis of SLE. We found an association between PD and decreased pulmonary function, and that PD might lead to damage according to SDI early in the SLE disease course. It was difficult to diagnose PD based on findings from the out-patient visit including PFT and CXR, whereas HRCT descriptions strongly pointed towards the final diagnosis of PD, indicating that HRCT at present is necessary for a thorough evaluation of PD in SLE. An abnormal TUS was associated with diseases of pleura and pulmonary parenchyma and abnormal DUS with SLS. Our results are based on 10 participants, why we cannot draw any conclusion but regard our results as hypothesis-generating. The potential of TUS and DUS for identification of PD in SLE should be investigated in dedicated studies including more participants making to draw conclusions.
Patient’s perspective
The patient partner states: It is surprising how common pulmonary diseases are among newly diagnosed patients with SLE, but it is encouraging that there are relevant treatment options. Most SLE patients should probably be investigated for PD, and new diagnostic tools are appreciated if they are safe, comfortable, and easily accessible. The study might lead to many questions from the patients including: - What can patients do to prevent pulmonary diseases? - Are pulmonary diseases dangerous? - Are pulmonary diseases treatable? - What is the downside of possible treatment of pulmonary diseases? - Is it possible that the patient’s symptoms can improve? - Is TUS and DUS reliable tools or is chest CT necessary?
Supplemental Material
Supplemental Material - Prevalence of pulmonary diseases among patients newly diagnosed with systemic lupus erythematosus: A cross-sectional case-series introducing thoracic ultrasound and diaphragmatic ultrasound
Supplemental Material for Prevalence of pulmonary diseases among patients newly diagnosed with systemic lupus erythematosus: A cross-sectional case-series introducing thoracic ultrasound and diaphragmatic ultrasound by Henrik Zachar Langkilde, Jesper Rømhild Davidsen, Stefan Markus Walbom Harders, Stefan Møller Luef, Susan Due Kay, Sille Fløjborg, and Anne Voss in Lupus.
Footnotes
Acknowledgments
Primarily Le Chat by Mistral AI but also ChatGPT were used to improve the readability of the manuscript and in the process of finding references. All performed under the supervision of the first author, who has edited any suggestions and are accountable for full the manuscript. We also like to acknowledge the patient partner, who is not a co-author, for helping to develop the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: HL received funding from The Danish Rheumatism Association, University of Southern Denmark, Region of Southern Denmark, Odense University Hospital, and Fonden til Lægevidenskabens Fremme – The A.P. Moller Foundation. The funders did not have any role in the study.
ORCID iDs
Supplemental Material
Supplemental Material for this article is available online.
Appendix
Clinical characteristics, 6MWT measures, and CXR descriptions of 10 participants newly diagnosed SLE. Continuous data are presented with median and interquartile range, as non were normally distributed. * -defined as more than once pr. Year. ** defined as sensation of tightness in the chest. RTI – respiratory tract infections. NA – Not abnormal. 6MWT – six-minute walk test. CXR – chest X-ray.
Patient number/Outcome
Summarized
#1
#2
#3
#4
#5
#6
#7
#8
#9
#10
Diagnosis of pulmonary diseases
SLS and pleuritis sequalae
ILD and bronchi-ectasis
ILD
Pleural fibrosis and bronchi-ectasis
Pleuritis
Thickened bronchial wall and air trapping
None
None
None
None
Prior medical history
Dry cough
Never 8
Newer
Never
Prior
Prior
Never
Never
Never
Never
Never
Never
Prior 2
Recurrent RTI*
No 9
No
No
No
Yes
No
No
No
No
No
No
Yes 1
Prior hospitalisation for RTI
No 7
Yes
No
No
Yes
Yes
No
No
No
No
No
Yes 3
Chest pain**
Never 4
Present
Never
Prior
Present
Prior
Never
Prior
Never
Never
Present
Prior 3
Present 3
Effusions
Never 6
Present
Never
Prior
Present
Present
Never
Never
Never
Never
Never
Prior 1
Present 3
Clinical investigation
Rales
10 NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
Friction rubs
10 NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
Cyanosis
10 NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
Clubbing
10 NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
Lower zone dullness at auscultation
7 NA
Yes
NA
NA
Yes
Yes
NA
NA
NA
NA
NA
3 Yes
Tests
Saturation, %
99 (99 - 100)
99
98
100
100
100
99
94
Low quality
99
100
Any desaturation, at 6MWT, %
1 (0 - 2)
Yes, 5
No
Yes, 2
No
Yes, 3
No
Yes, 1
Low quality
No
Yes, 1
Distance 6MWT, %
80 (72-102)
78
108
102
82
71
101
72
64
106
72
Time since latest CXR, months
3 (2-4)
9
2
2
0.5
3
Not perfor-med
6
4
3
3
Description of most recent CXR
NA 5
NA
Emphysema and fibrosis, otherwise NA
Pleural effusion, otherwise NA
Bilateral effusion otherwise NA
Pleural effusion, otherwise NA
Not perfor-med
NA
NA
NA
NA
Abnormal 4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.