
Abstract
Introduction
Cutaneous lupus can manifest with acute, subacute, and chronic eruptions triggered and exacerbated by ultraviolet exposure, making photoprotection an evidence-based aspect of disease management. This study aims to assess skincare and photoprotection knowledge and habits, medical information sources, and accessibility barriers among patients with lupus to identify knowledge gaps and inform educational initiatives.
Methods
A cross-sectional 41-question survey was distributed via REDCap to adult participants with self-reported lupus identified through Research Match, the Northwestern Medicine Enterprise Data Warehouse, and lupus community organizations from August 2022 to March 2023. Data analysis was conducted in R version 4.3.1, and descriptive and linear regression model tests were performed.
Results
Of 129 initiated questionnaires, 115 were completed and met eligibility criteria. Only 43% correctly identified UVA protection on sunscreen labels, and 49% reported daily sunscreen use. Most participants reported receiving skincare information from dermatologists (49%) or rheumatologists (40%), with no statistically significant differences in knowledge level between groups (p = 0.38). Participants with Fitzpatrick skin tones III-IV and V-VI had significantly lower photoprotection knowledge scores compared to Fitzpatrick skin tones I-II (p = 0.002 and p = 0.0006, respectively). Participants with lower incomes (≤$75,000) scored lower than those with higher incomes (>$75,000; p = 0.003). One-third (33%) endorsed difficulty affording the management of their lupus and 15% reported that the cost of sunscreen influenced sunscreen use.
Conclusions
These exploratory findings highlight a need for targeted educational efforts to improve lupus management and outcomes, particularly in low-income groups and communities of color. Dermatologists and rheumatologists care for a substantial portion of patients with lupus and share a responsibility to educate and address these gaps.
Introduction
Systemic lupus erythematosus (SLE) and cutaneous lupus erythematosus (CLE) manifestations can be triggered and exacerbated by ultraviolet (UV) exposure. 1 Adherence to UV-protective behaviors, such as sunscreen use and sun avoidance, in conjunction with topical and systemic therapies, plays a vital role in preventing and managing flares. Prior research studies have demonstrated that the majority of patients with lupus (92.3%–98%) are aware of the relationship between UV exposure and lupus exacerbations.2,3 However, usage of sunscreen has been found to vary greatly in different geographic cohorts, from 23% in Ireland to 93.7% in Thailand.4,5 In a previous cohort study in the United States, CLE patients with Fitzpatrick skin types III–VI were significantly less likely to use sunscreen than those with lighter complexions. 6 This trend has also been found among non-lupus populations. 7 Furthermore, prior literature has found discrepancies in photoprotection knowledge by race in patients with lupus. 8
In this cross-sectional exploratory study, we investigated photoprotective practices, skincare knowledge, and accessibility barriers faced by patients with lupus. We further examined sources of medical information, including healthcare providers and online sources.
Methods
An online 41-question survey was developed to assess demographics, lupus-related medical history, current medications, skincare knowledge, photoprotective behaviors, educational sources, and access barriers (See Supplement 1). The survey was not tested with samples, however, content validity of the survey was determined by two academic dermatologists on the study team with expertise in survey creation and clinical subspecialty care of patients with lupus. Previously published photoprotection knowledge surveys were utilized as a basis to validate internal consistency. After obtaining Institutional Review Board (IRB) approval through Northwestern University, the survey was anonymously distributed via REDCap from August 2022 to March 2023. Recruitment occurred through Research Match (a national patient registry supported by the National Institutes of Health), lupus community groups and organizations, and the Northwestern Medicine Enterprise Data Warehouse (EDW). Inclusion criteria included having a self-reported lupus diagnosis and being 18 years or older.
Data were stratified into two income brackets, using an annual household income threshold of $75,000 to differentiate low- and high-income groups. The composite photoprotection knowledge score was measured as the share of correct responses (0-100%) to three survey questions: understanding of UV exposure from artificial light indoors, identification of broad-spectrum UVA protection, and the recognition of SPF value as an indicator of UVB protection. Participants self-reported their Fitzpatrick skin tone using a descriptive scale. Data analysis was conducted in R version 4.3.1, and descriptive and multivariable linear regression models adjusted for education, race, region, and disease duration were performed to interpret the data, with p < 0.05 considered statistically significant.
Results
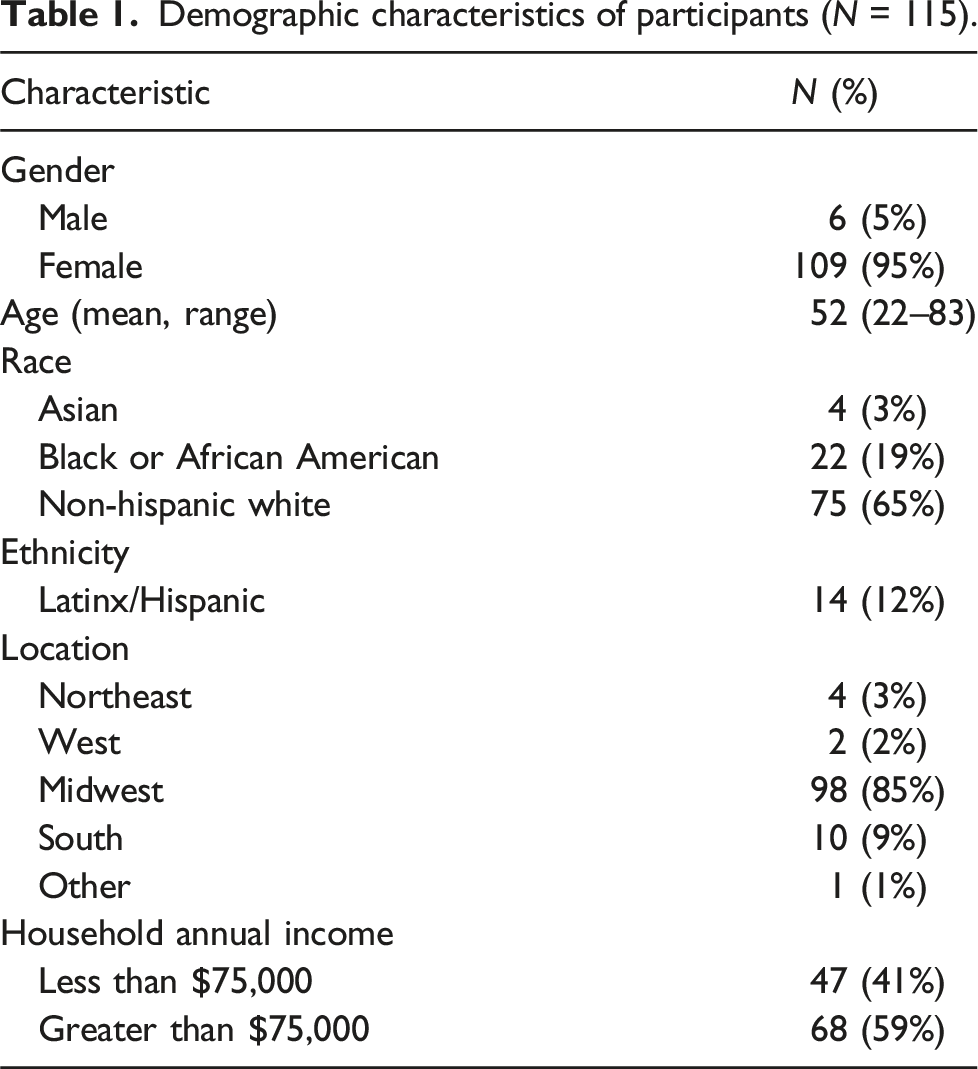
Participant characteristics
Demographic characteristics of participants (N = 115).
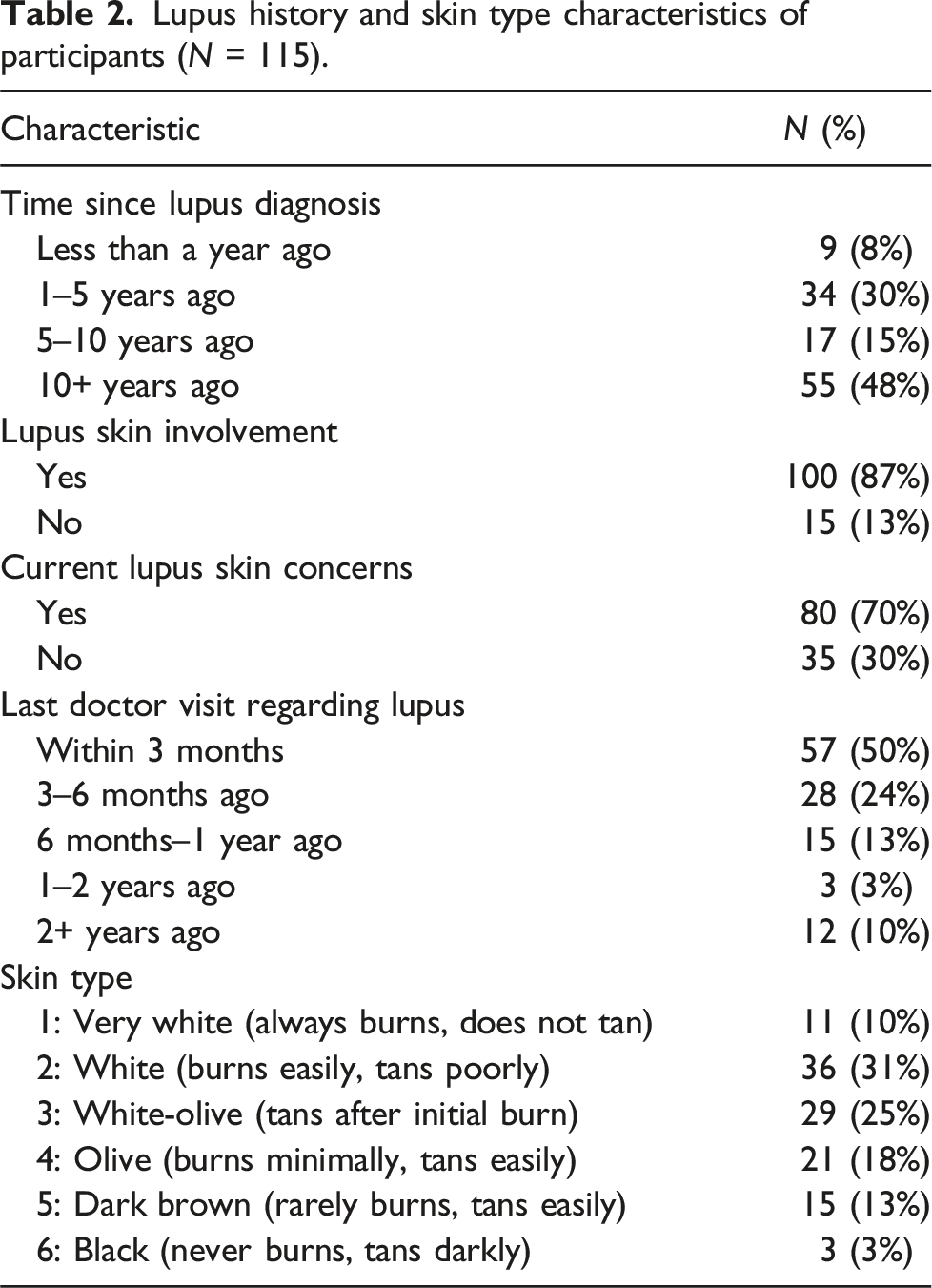
Lupus history and skin type characteristics of participants (N = 115).
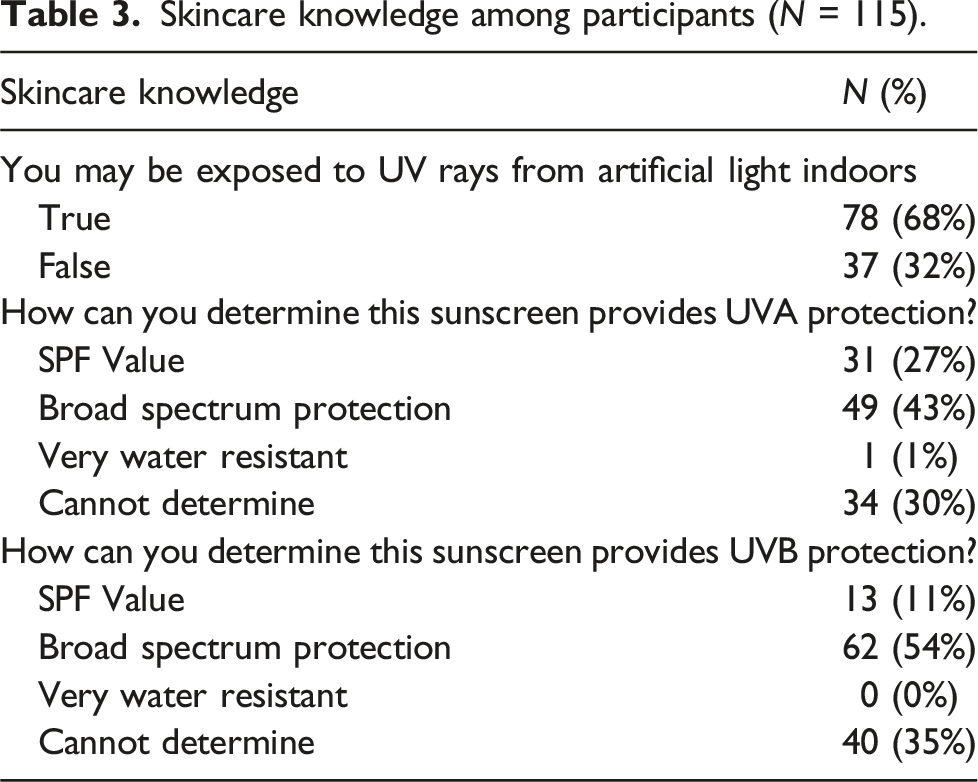
Photoprotective behavior and photoprotection knowledge
Skincare knowledge among participants (N = 115).
Skincare and sunscreen habits among participants (N = 115).
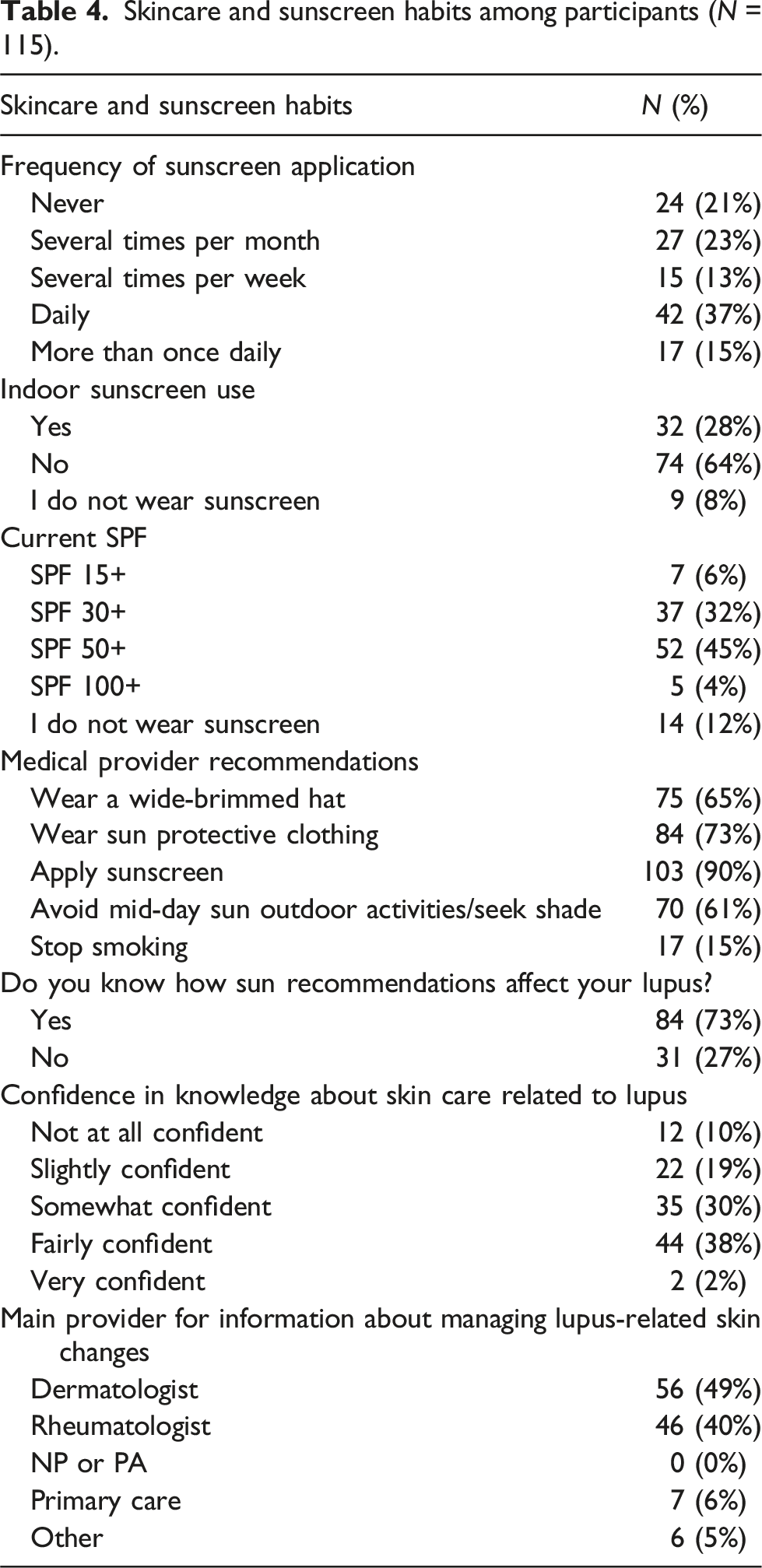
Self-reported confidence in skincare knowledge was also limited. Only two participants (2%) reported feeling ‘very confident’ when asked to rate their confidence in their knowledge about how to care for their skin in relation to lupus. The majority reported being either ‘fairly confident’ (n = 44, 38%) or ‘somewhat confident’ (n = 35, 30%), while 22 (19%) felt ‘slightly confident,’ and 12 (10%) ‘not at all confident.’
Effects of income and skin tone
Knowledge and sunscreen use were limited across income groups. However, participants with lower household incomes demonstrated lower knowledge about photoprotection. Among those with an annual household income ≤$75,000 (n = 47), 11 (23%) correctly identified UVA protection of sunscreen, 19 (40%) did not know one could be exposed to UV rays from artificial light indoors, and 10 (21%) wore sunscreen indoors. In comparison, participants with annual household income >$75,000 (n = 68) showed higher knowledge and sunscreen usage. Over half (n = 38, 56%) correctly identified UVA protection on sunscreen labels, yet 18 (26%) were unaware of UV exposure from artificial light, and only 22 (32%) wore sunscreen indoors. Daily sunscreen use was higher in the higher-income group (n = 35, 51%) compared to the lower-income group (n = 14, 30%) (p = 0.03).
Unadjusted regression analysis of composite photoprotection knowledge scores demonstrated that participants with lower incomes (≤$75,000) scored 13 percentage points lower than those with higher incomes (>$75,000; 95% CI: −22.4 to −4.6; p = 0.003). This difference remained significant when controlling for region, race, and disease duration, with an effect of −10 percentage points (95% CI: −19.6 to −0.7; p = 0.04).
Non-Hispanic white respondents scored 16 percentage points higher than respondents of color (95% CI: 7.2 to 25.3; p = 0.0006). This difference remained significant when controlling for region, income, and disease duration with an effect of 14 percentage points (95% CI: 3.9 to 23.2; p = 0.006).
Participants with darker self-identified Fitzpatrick skin tones demonstrated significantly lower knowledge scores. Compared to participants with Fitzpatrick I-II, participants with Fitzpatrick III-IV scored 14 percentage points lower (95% CI −23.7 to −5.04; p = 0.003), and participants with Fitzpatrick V-VI scored 23 percentage points lower (95% CI −35.3 to −9.9; p = 0.0006). Adjusted regression analysis controlling for income, geographic region, and disease duration showed that, compared to participants with Fitzpatrick I-II, Fitzpatrick III–IV skin types had 15 percentage points lower knowledge scores (95% CI −25.0 to −5.56; p = 0.002), and Fitzpatrick V–VI skin tones had scores 22 percentage points lower (95% CI −35.2 to −8.6; p = 0.001).
Affordability and accessibility
Among all participants, 38 (33%) reported that skincare products recommended for lupus were unaffordable. This included 17 lower-income and 21 higher-income participants. Medication for lupus was the most frequently reported expense that participants found unaffordable. Notably, 17 (15%) noted that the cost of sunscreen affected application frequency, highlighting financial barriers to consistent photoprotection. Despite these challenges, only 11 participants discussed affordability issues with their medical providers, revealing a communication gap related to access.
While no statistically significant differences in affordability perceptions were observed based on race or skin tone, a significant relationship was identified between affordability concerns and the reduction of sunscreen application due to cost (p = 0.0002), underscoring the impact of financial barriers across all patients.
Medical source of information
Most participants reported receiving most of their skincare information from dermatologists (n = 56, 49%) or rheumatologists (n = 46, 40%). No statistically significant difference in skincare knowledge (p = 0.38) or confidence in knowledge (p = 1) was observed between groups. Participants who received information from dermatologists used sunscreen slightly more (86% vs 74%); however, this difference was not statistically significant (p = 0.14).
Discussion
Our results reinforce the suboptimal use of sunscreen in patients with lupus in the United States, as shown in other studies based on US cohorts.4,6 Overall, less than half of our cohort (37%) of used daily sunscreen despite high awareness of its importance in disease management, active cutaneous concerns, and acknowledgement of provider recommendations. Notably, 93% reported that their provider had recommended using sunscreen to manage their lupus, yet 21% stated that they never applied sunscreen. This highlights a persistent challenge in translating knowledge into sustainable photoprotective habits and behaviors, even among patients with recent healthcare contact.
Deficiencies in skincare knowledge and adherence to photoprotective behaviors were more pronounced among vulnerable subgroups in our cohort. We found the association that participants from lower-income backgrounds had statistically significantly lower knowledge of photoprotection and rates of photoprotective behaviors. We found similar associations when analyzing by Fitzpatrick skin type and race, with non-Hispanic whites and Fitzpatrick I-II scoring higher in photoprotection knowledge. These results highlight multifactorial influences rather than causal relationships for our small cohort. Our findings in photoprotection knowledge variance by race and Fitzpatrick skin type align with previous trends found in research in this population.6,8 Further research in larger cohort studies with diverse populations is warranted.
Our findings have two key implications. First, they illustrate the complexity of implementing evidence-based guidelines and behavioral change despite awareness of the importance of photoprotection and provider recommendations. Second, they demonstrate persistent educational knowledge gaps despite endorsement of awareness, suggesting that building knowledge and habits in photoprotection is a multi-layered process. A previous study by Kaushik et al. found that their educational intervention for CLE patients did not show long-term retention. 8
We also examined how certain structural barriers may hinder the implementation of photoprotective behaviors and disease management. A previous study estimated that the financial burden of CLE in 2018 exceeded $10,000 per year. 9 In our cohort, we found that most participants believed skincare products to manage their lupus were affordable. However, a third (33%) of all participants felt that products were not affordable, with 55% (n = 21) of these respondents earning a household income greater than $75,000. This underscores that affordability concerns span income groups. However, a minimal number of participants (n = 11, 10%) had shared these concerns with their medical provider. The financial burden associated with lupus can be further compounded by other stressors that have been studied among patients with lupus, including mental health, stress, and Ref. 10.
Fostering discussion during medical appointments with patients about the structural, accessible, and financial barriers is an actionable step that can help begin to address these challenges. There has been some research on digital intelligence initiatives, including teledermatology for other dermatologic conditions such as acne vulgaris with promising results in patient satisfaction and greater accessibility, particularly for patients in rural areas.11,12 Teledermatology may offer an additional avenue to address structural barriers to photoprotective behaviors, including building knowledge and access to care.
One limitation of our study is that the survey instrument was not formally psychometrically validated, which may limit interpretability, generalizability, and reproducibility. Other limitations of our study include the potential for recall bias and the sample population not accurately reflecting the general population. Our recruitment relied on online registries and one large tertiary medical network in an urban setting. Therefore, our participants may have greater internet access and health literacy than the general population of lupus patients.. Another limitation is that most participants were from the Midwest. Additionally, lupus is a condition that predominantly affects darker-skinned individuals, which in our study participant population are not the majority; therefore, further analysis focusing on skin of color is warranted. It is also worth noting that most of our participants earned over $75,000 a year, which can influence our results on affordability and structural and accessibility barriers.
Gaps in knowledge and sunscreen use highlight a need for greater education and interventions targeting these areas, particularly in low-income groups and patients of color. Dermatologists and rheumatologists care for a substantial portion of patients with lupus and share a responsibility to educate on the role of photoprotection in their lupus management. Further studies are needed to evaluate current educational resources available for lupus, particularly in under-resourced populations to identify better methods to improve access and adherence to photoprotection.
Conclusion
Barriers in skincare knowledge and photoprotection habits persist among patients with lupus. Dermatologists and rheumatologists are critical sources of skincare information for this population. Photoprotection management of lupus is unaffordable for some patients and may impact sunscreen application frequency. Improving knowledge and photoprotective habits among lupus patients remains a significant challenge.
Supplemental material
Supplemental Material - Survey-based assessment of skin care knowledge and accessibility barriers in lupus
Supplemental Material for Survey-based assessment of skin care knowledge and accessibility barriers in lupus by Claudia Roldan Rivera, Riddhi D. Patel, Roopal V. Kundu, Jennifer L. Shastry in Lupus.
Footnotes
Acknowledgments
We thank the patients who generously contributed their time and perspectives to this study.
Author Contributions
C.R.R. contributed to the study’s conceptualization, design, data collection, analysis, interpretation of findings, and manuscript writing. R.D.P. assisted with data analysis and manuscript writing. R.V.K. contributed to study conceptualization, survey design, interpretation of findings, manuscript review, and senior supervision. J.L.S. contributed to study conceptualization, survey design, interpretation of findings, manuscript review, and senior supervision. All authors reviewed and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This study was reviewed and approved by the Northwestern University Institutional Review Board (IRB), under protocol number STU00217181. All participants provided informed consent electronically prior to participation in the survey. Data were collected anonymously, and no identifiable personal information was retained.
Consent to participate
All participants provided informed consent electronically prior to participation in the survey.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.