
Abstract
Objectives
Anti-dense fine speckled 70 (anti-DFS70) antibodies have been reported to be more prevalent in healthy individuals (HI) than in patients with autoimmune diseases including systemic lupus erythematosus (SLE). However, subsequent studies have yielded inconsistent findings. The reliability of anti-DFS70 antibodies as exclusionary markers for SLE remains uncertain and warrants further investigation.
Methods
Sixteen studies investigating 6092 subjects (2427 SLE patients and 3665 healthy individuals) were included in the analysis. A meta-analysis was conducted to evaluate and compare the sensitivity, specificity, and diagnostic odds ratio (DOR) of anti-DFS70 antibodies for determining their utility in excluding SLE in the general population.
Results
In SLE patients, the prevalence of anti-DFS70 antibodies was 10.1% (244/2427; 95% CI: 5.7–14.5%), which was not significantly higher than that of HI, at 5.8% (212/3665; 95% CI: 2.9–8.7%). The pooled sensitivities, specificities, and DOR of anti-DFS70 antibodies for the exclusion of SLE were 0.10 (95% CI: 0.09–0.11), 0.94 (95% CI: 0.93–0.95), 1.04 (95% CI: 0.59–1.85), respectively. The area under the summary receiver operating characteristic (SROC) curve was 0.58 (95% CI: 0.28–0.90), indicating that the test results of anti-DFS70 antibodies have similar distributions in SLE patients and HI. Regarding monospecific anti-DFS70 antibodies in SLE, three studies involving 385 patients with SLE and 648 healthy individuals found these antibodies in 0.8% (3 out of 385) of SLE patients, compared to 6.6% (43 out of 648) of healthy individuals. The corresponding DOR for excluding an SLE diagnosis was 4.00 (95% CI: 1.39–11.46).
Conclusions
While the present study corroborates findings that the frequency of anti-DFS70 antibodies is slightly higher in SLE patients (10.1%, 244 out of 2427), the lack of statistical significance underscores the need for more comprehensive studies to draw definitive conclusions for the exclusion of SLE.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease which disproportionately affects women, and people of Asian, Black, Hispanic and Indigenous descent. 1 Patients with SLE may suffer from a wide range of symptoms, which may compromise health-related quality of life, develop comorbidities, and finally death.2–4 Earlier diagnosis and treatment advances are crucial, and have resulted in improved outcomes over the past decades.5,6 According to the 2019 European League Against Rheumatism (EULAR)/ACR classification criteria, the presence of antinuclear autoantibodies (ANA) is the obligatory entry criterion of SLE. 7 Since patients with SLE may present with only a few clinical features, clinicians may request ANA detection when evaluating a patient with a suspected autoimmune disease. Detection of ANAs by indirect immunofluorescence (IIF) using HEp-2 cells is considered the gold standard for the detection of ANAs, 8 which is a highly sensitive, widely utilized test for detection and distinguishing different antibodies targeting nuclear, mitotic and cytoplasmic antigens. However, ANAs are also observed in up to 54% of healthy individuals.9,10 The high prevalence of ANA reactivity in otherwise healthy individuals complicates the diagnostic assessment of autoimmune diseases, leading to undue anxiety in patients who lack clinical symptoms and placing additional strain on health care resources.11–15
According to the international consensus on ANA patterns (ICAP), ANA positivity with the pattern dense fine speckled (DFS) or AC-2, defined by a dense and heterogeneous speckled staining in the nucleoplasm throughout the interphase (sparing the nucleoli) and the metaphase chromosomal plate, might be associated with the anti-dense fine speckled 70 (anti-DFS70) autoantibodies. It is the target antibody of DFS70 protein, also known as lens epithelium-derived growth factor p75 (LEDGF/p75). First described in the serum of patients with interstitial cystitis, these antibodies were named anti-DFS70 antibodies owing to its staining pattern of Hep-2 cells by IIF and its target antigen was a 70-kDa protein16,17. This protein has a number of physiological and pathological functions, including promoting cell survival when facing environmental stressors such as alcohol, UVB irradiation, and starvation.18–20 It also participates in the process of human immunodeficiency virus replication through an interaction with viral integrase, 21 as well as being considered a stress oncoprotein for its overexpression in malignant tissues.18,22,23 The anti-DFS70 autoantibodies have subsequently been identified in a variety of diseases, including inflammatory diseases, cancers, and healthy individuals (HI).17,24,25 Whether these autoantibodies have protective or pathogenic roles remains elusive.
Systemic autoimmune rheumatic diseases (SARD) comprise a group of diseases which include SLE, Sjögren’s syndrome, systemic sclerosis, dermatomyositis/polymyositis (DM/PM), mixed connective tissue diseases (MCTD), and others.26,27 Healthy individuals with anti-DFS70 autoantibodies rarely develop SARD, especially in the absence of clinical evidence or additional anti-extractable nuclear antigen (ENA) antibodies, as confirmed during an average follow-up period of 4 years.12,28–30 In SLE, the prevalence of anti-DFS70 antibodies ranged from 0% to 22.1%.14,31–35 Despite wide variation reported, the prevalence of anti-DFS70 antibodies was relatively rarer than the positive rates of healthy individuals in most studies.24,33,34,36–39 Over the past decade, there has been ongoing debate and research regarding the diagnostic significance of anti-DFS70 autoantibodies in patients with SLE.9,12,29,40,41 Early studies demonstrated that the prevalence of anti-DFS70 autoantibodies was relatively lower in patients with SLE compared to healthy individuals,12,17,24,25,33 leading to the proposal of their potential utility as an exclusion marker in the diagnosis of SLE. However, as more recent research has emerged, the situation has become more complex. For instance, Nilsson et al. found that the prevalence of DFS70 autoantibodies was 2.3% (3/131) in Danish SLE patients, which was not significantly different from the prevalence observed in blood donors (2.0%; 5/249; P = 1.0). 40 Hayashi et al. reported the prevalence of anti-DFS70 antibodies was 16.4% (41/250) in HI and 22.1% (15/68) in patients with SLE. 32 These newer studies have shown an increasing trend in the positive rate of anti-DFS70 antibodies among SLE patients,29,32,35,40,42–46 which points to the need for further investigation into whether the presence of these antibodies can serve as a reliable exclusion marker for SLE. Therefore, we conducted this systematic review and meta-analysis to evaluate the prevalence and the diagnostic indicators of anti-DFS70 antibodies for the exclusion of SLE. Additionally, since the prevalence of anti-DFS70 antibodies varies among ethnic groups31,32 and shows an increasing trend over time, 47 we also determine whether ethnicity and temporal factors influence the diagnostic value of anti-DFS70 antibodies.
Materials and methods
A comprehensive search of peer-reviewed articles indexed in the electronic databases of PubMed, EMBASE, Google scholar, and Ovid Medline was performed, and the reference lists of the retrieved articles were also reviewed to identify additional studies for inclusion. The electronic search covered the period from January 2000 to July 2024, with no language restrictions. Search terms included: “anti-DFS70 antibodies,” “lupus,” “SLE,” “health individuals,” “general population,” and “prevalence.” Studies were included if they provided a clear definition of healthy individuals and reported the positivity rate of anti-DFS70 antibodies among SLE patients and healthy individuals using specific detection methods such as enzyme immunoassay (EIA), chemiluminescence immunoassay (CIA), or immunoblot (IB). Studies were excluded if they involved fewer than five patients or healthy individuals.
Two review authors (YH and PH) conducted the electronic search independently and in duplicate. Any disagreement was resolved by consensus, and if consensus could not be reached, the issue was referred to a third author (KY) for final adjudication. When multiple articles for a single study had been published by the same teams or authors, we used the most relevant publication and supplemented it with data from the authors’ other publications. Authors of studies were contacted when pertinent information was not available in the published version.
The following data of eligible articles was extracted, including author’s name, year of publication, total number of patients, method of detecting anti-DFS70 antibodies, number of SLE patients with anti-DFS70 antibodies, and number of healthy individuals with anti-DFS70 antibodies. Data extraction was conducted independently by two reviewers (YH and PH) to minimize errors and enhance the reliability of the results. The quality of each included study was evaluated according to the Quality Assessment of Studies of Diagnostic Accuracy-2 (QUADAS-2). 48 Data were pooled by means of a random-effects model, and then the sensitivity, specificity, positive and negative likelihood ratios (LR+ and LR–, respectively), diagnostic odds ratios (DOR), summary receiver operating characteristic (SROC) curve, and 95% confidence intervals (CI) were calculated. We also constructed forest plots for DOR along with the corresponding 95% CI, and calculated the area under the curve (AUC) to assess the diagnostic accuracy of the examination. All statistical analyses were performed in Meta-DiSc 2.0 (Universidad Complutense, Barcelona, Spain). 49
Results
Characteristics of the study populations
In the present study, we identified 122 articles from online database, of which 94 irrelevant articles were excluded. The remaining 28 articles were further assessed for eligibility. Nine of the articles were excluded due to results not including both SLE patients and HI, whereas three of the articles were excluded due to overlapping patient populations. The definition for healthy individuals in each study was carefully reviewed. We had excluded articles that involved individuals without clear definition of “health”. For example, first degree relatives of SLE patients, people who followed up at Rheumatologist’s office but without definite diagnosis for SARD, and others. Eventually, 16 articles12,17,24,25,29,31,32,36,38–45 were included in the meta-analysis consisting of a total of 2427 SLE cases and 3665 HI. Figure 1 shows the PRISMA flow diagram for studies retrieved through the electronic search and the selection processes for study inclusion. The quality of the included studies as assessed by the QUADAS-2 tool was generally high, with all studies meeting eight or more of the criteria. The detailed characteristics of each study are presented in Table 1. Among the included studies, five were conducted in Asian populations, including three studies in Japan,17,24,40 one study in China,
44
and one study in Indonesia.
31
An additional eight studies examined individuals from Caucasian populations in the United States25,32,42 Canada,
41
Italy,
29
Denmark,
38
Bulgaria,
45
and Russia
39
(Table 1). The remaining studies were conducted in Brazil,
12
Turkey,
43
and Israel.
36
Methods for detecting anti-DFS70 antibodies included immunofluorescence (IIF) assay, EIA, CIA, line immunoassay (LIA), and IB. Six of the studies used CIA, eight of the studies used EIA, two used IB, and one used an indirect fluorescent antibody assay (IFA). All of the above were suitable methods for detection of anti-DFS70 antibodies (Table 1). PRISMA flow diagram for studies retrieved through the electronic search and the selection processes. Characteristics of the studies included in the meta-analysis. SLE: Systemic lupus erythematosus; HI: Health individuals; IIF: indirect immunofluorescence; IB: immunoblot; EIA: enzyme immunoassay; CIA: chemiluminescence immunoassay; IFA: indirect fluorescent antibody assay. aNumber of cases with anti-DFS70 antibody/total number of cases.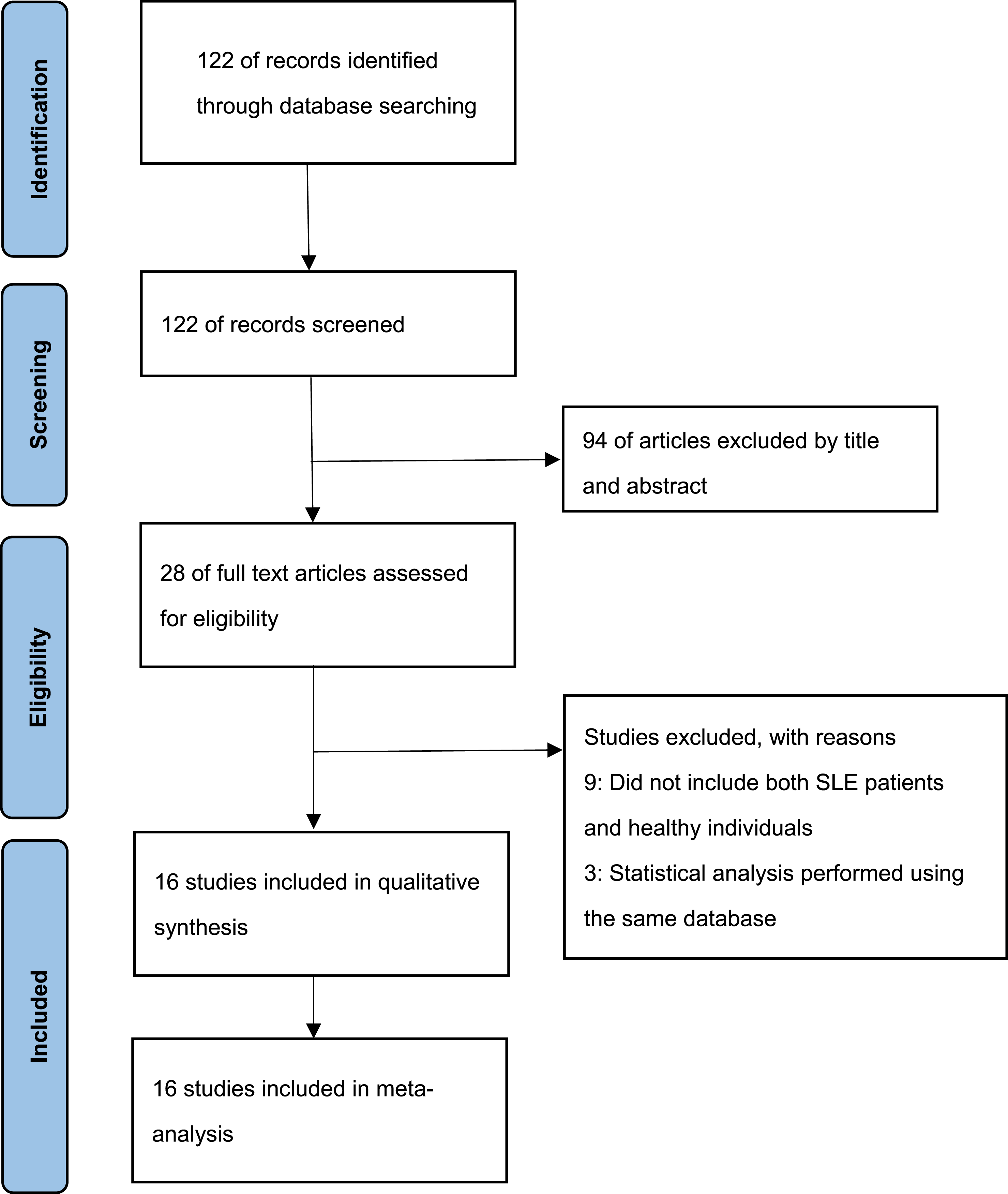
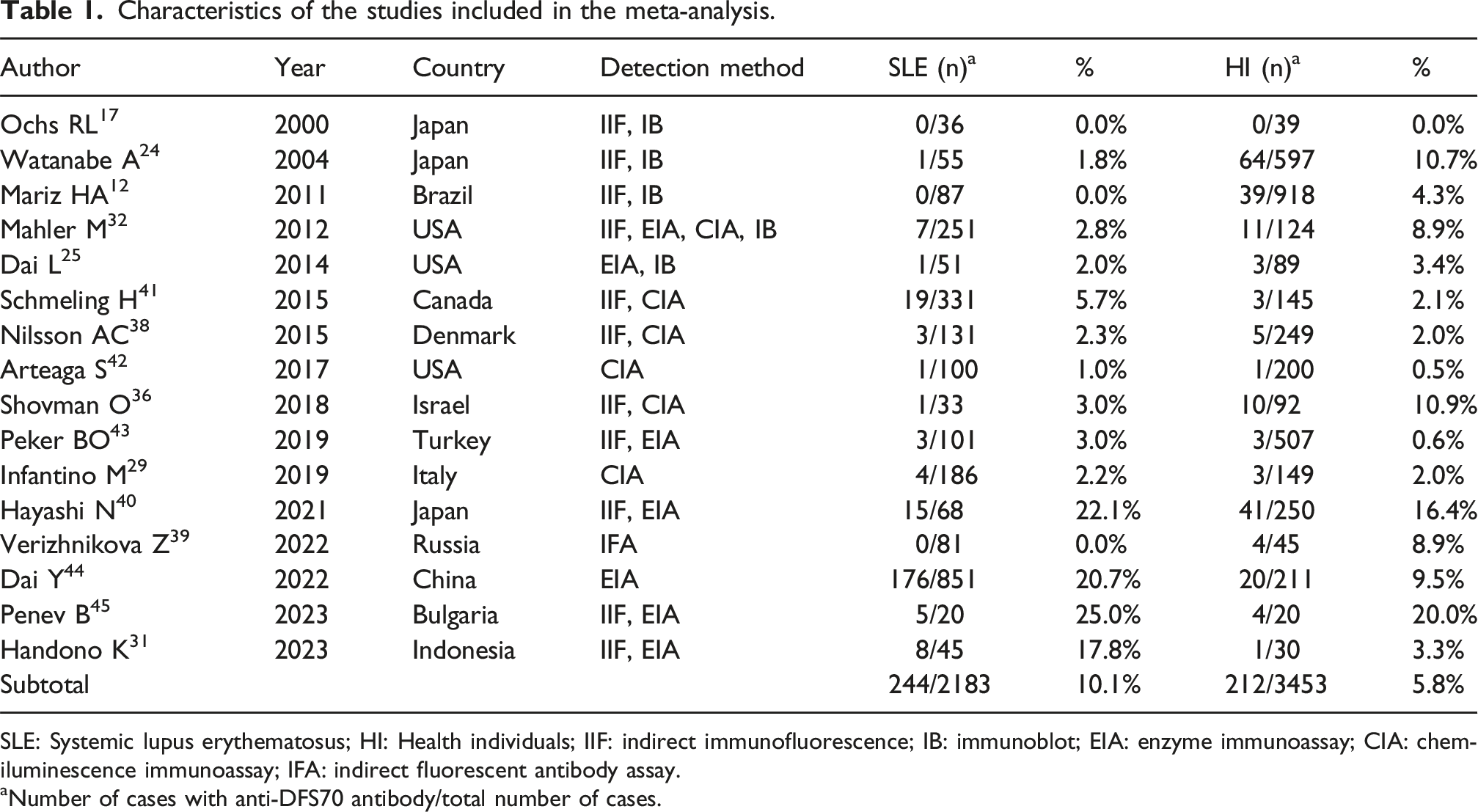
The reported prevalence of anti-DFS70 antibodies among patients with SLE ranges between 0% and 25% (Table 1). The overall prevalence of anti-DFS70 antibodies in patients with SLE was 10.1% (244/2427; 95% CI: 5.7–14.5%). The sample sizes of SLE cases in each study ranged from 20 to 851 (mean 152, median 84). The overall prevalence of anti-DFS70 antibodies in HI was 5.8% (212/3665; 95% CI: 2.9–8.7%). The sample sizes of healthy individuals in each study ranged from 20 to 918 (mean 229, median 147). The prevalence of anti-DFS70 antibodies between SLE patients and healthy individuals had no statistical difference (10.1% vs 5.8%, p = 0.821).
Diagnostic performance of anti-DFS70 antibodies in the exclusion of SLE
Diagnostic indicators of the included studies for the exclusion of SLE through anti-DFS70 antibody.
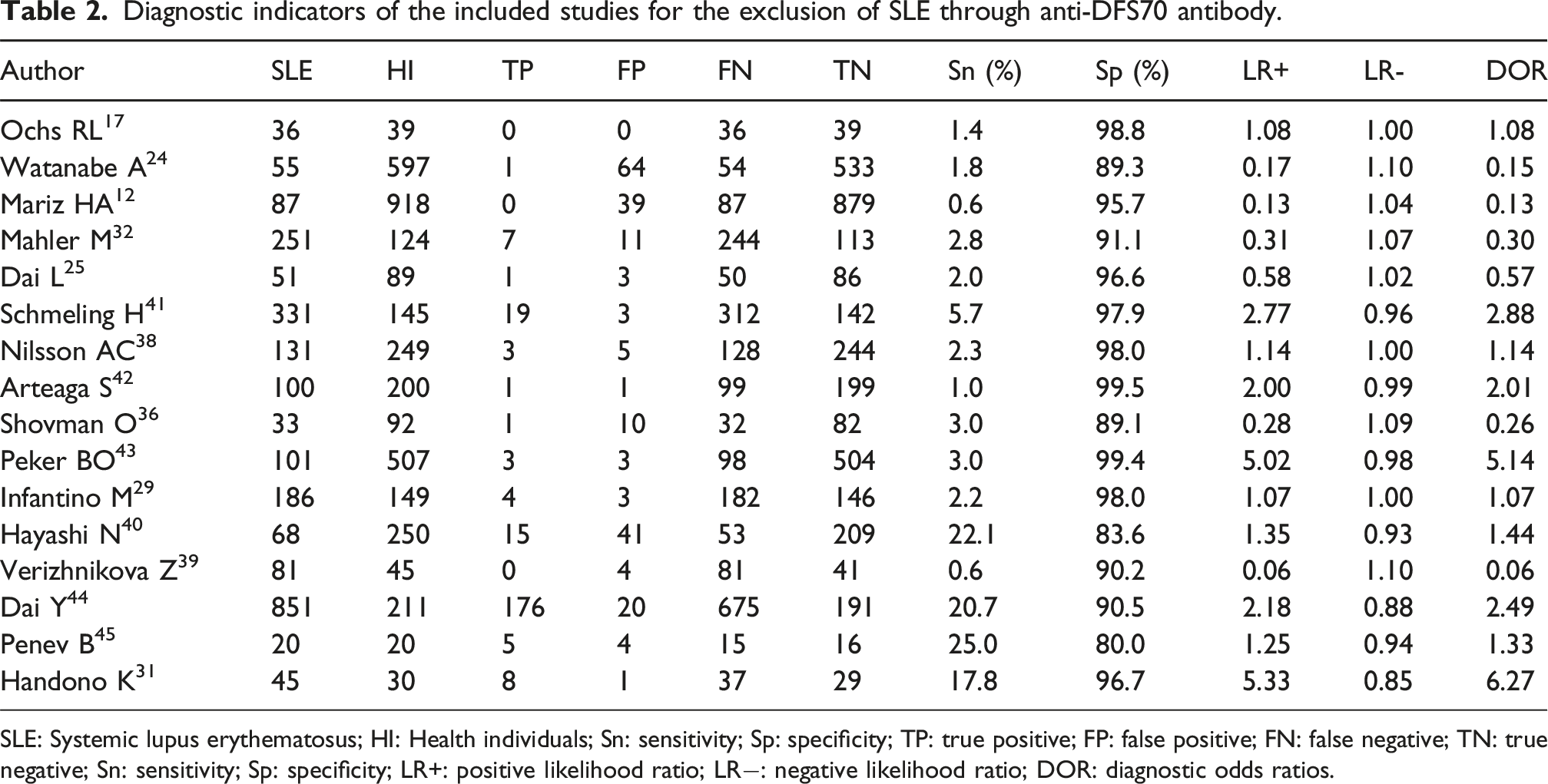
SLE: Systemic lupus erythematosus; HI: Health individuals; Sn: sensitivity; Sp: specificity; TP: true positive; FP: false positive; FN: false negative; TN: true negative; Sn: sensitivity; Sp: specificity; LR+: positive likelihood ratio; LR−: negative likelihood ratio; DOR: diagnostic odds ratios.
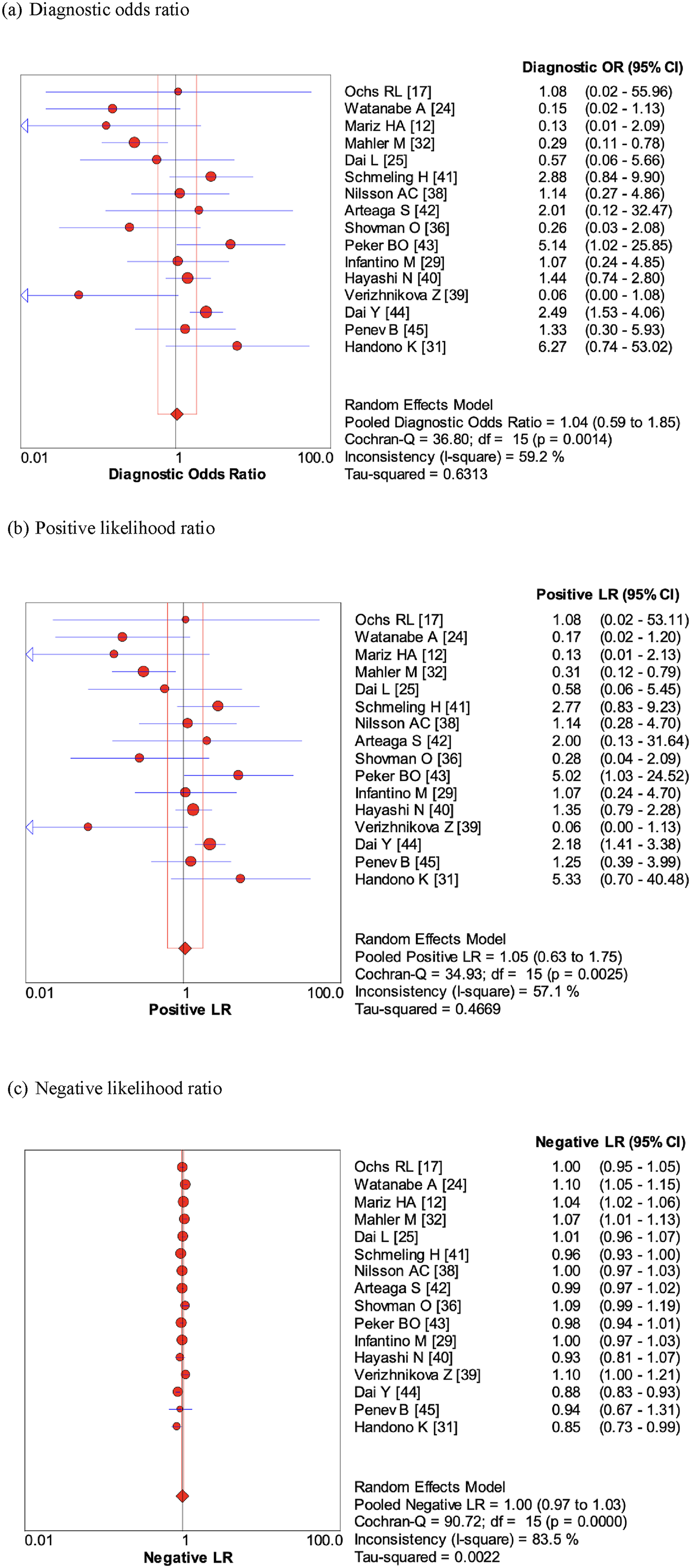
The diagnostic indicators of anti-DFS70 antibodies for the exclusion of SLE: (a) diagnostic odds ratio, (b) positive likelihood ratio, (c) negative likelihood ratio. LR: likelihood ratio.
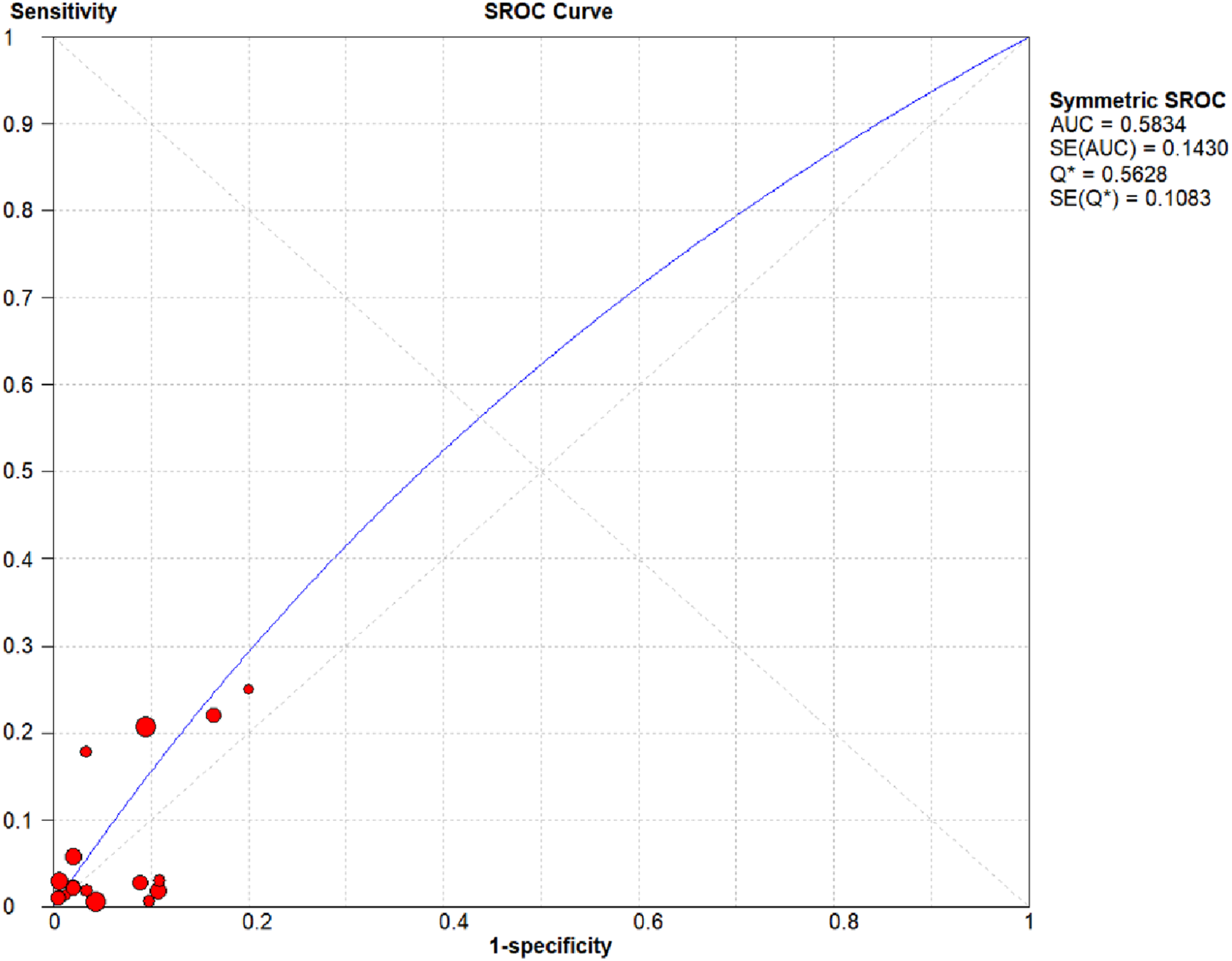
SROC curve of anti-DFS70 antibodies for the exclusion of SLE.
Subgroup analysis
Ethnicity may contribute to the observed variation in the positive rate of anti-DFS70 antibodies; therefore, a further subgroup analysis based on ethnicity was conducted. The included studies were classified into Asian and non-Asian groups according to the countries of origin. The DOR of each group was analyzed. In the Asian group, the DOR was 1.58 (95% CI: 0.71–3.54), while in the non-Asian group, the DOR was 0.84 (95% CI: 0.40–1.77). Overall, anti-DFS70 antibodies demonstrated no clinical utility in excluding SLE in either Asian or non-Asian populations.
We also found an increasing temporal trend in the prevalence of anti-DFS70 antibodies from 2015 to 2023 (Table 1). A comparable increasing temporal trend was observed in an American cohort analyzing the prevalence of anti-DFS70 antibodies in 1988-2012. 47 We investigated whether the increased positivity rate may impact the diagnostic performance of anti-DFS70 antibodies over time. We stratified the studies into two groups based on their publication year: those published before 2015 and those published after 2015, the year in which the prevalence rate among SLE patients exceeded that of HI in the majority of studies (Table 1). Subgroup analyses based on year (before vs after 2015) revealed the following DORs for the presence of anti-DFS70 antibody in excluding an SLE diagnosis: before 2015, 0.57 (95% CI: 0.20–1.58); and after 2015, 1.60 (95% CI: 0.88–2.90). These results suggest that the exclusion of SLE based on anti-DFS70 antibodies was not significantly influenced by the temporal trend.
Discussion
SLE is an autoimmune disorder that may involve multiple organs with a variety degree of severity. The early and definite diagnosis of SLE was challenging either because the patient may not have common SLE features or because the initial presentation may mimic other diseases.43,50,51 Of particular concern, the criteria for diagnosing SLE have lower sensitivity for classifying early lupus, probable lupus, incomplete lupus or other lupus endotypes.52,53 Delayed diagnosis and misdiagnosis are common problems, which may cause devastating long-term consequences for SLE patients.54,55
The anti-DFS70 antibodies play an increasing role in the exclusion of SLE.14,24,29,33,38,41,45,56,57 Anti-DFS70 antibodies have been detected at elevated frequency in apparently healthy individuals compared to patients with SLE, which was usually accompanied by additional antibodies. This negative association between antibodies to DFS70 and SLE led to its use as a possible biomarker for the exclusion of SLE. On the contrary, Mockenhaupt et al. found a specificity of 86.6%, a sensitivity of 26.9%, and a positive predictive value (PPV) of 68.2% for anti-DFS70 antibodies with regard to the exclusion of CTD, including SLE. 9 The author concluded that the presence of anti-DFS70 antibody has limited value for the exclusion of CTD in the presence of a positive ANA result. 9 The prevalence of anti-DFS70 antibodies in SLE patients and HI varies significantly across studies, even within the same country. Watanabe et al. reported a lower prevalence in SLE (2%) than HI (10.7%) 24 whereas Hayashi et al. observed a higher prevalence in SLE (22.1%) than in HI (16.4%). 40 This inconsistency highlights the need for further research before using anti-DFS70 antibodies as a reliable biomarker to exclude ANA-related diseases. The present study found that the overall prevalence of anti-DFS70 antibodies in patients with SLE and HI was 10.1% (244/2427; 95% CI: 5.7–14.5%) and 5.8% (212/3665; 95% CI: 2.9–8.7%), respectively. The overall prevalence of anti-DFS70 antibodies in our meta-analysis of SLE patients was similar with that observed in a large international study conducted in 2017, which reported a frequency of 7.1% (95% CI: 5.7–8.8%) among 1137 SLE patients. 46 In the present study, the pooled DOR was 1.04 (95% CI: 0.59–1.85), which indicated that the odds of detecting anti-DFS70 antibodies are comparable in both diseased and non-diseased individuals, suggesting that anti-DFS70 antibodies have limited utility for excluding the diagnosis of SLE. The AUC for the diagnosis of SLE in the presence of anti-DFS70 antibodies was 0.58 (95% CI: 0.28–0.90). The AUC value was below 0.8, and therefore was of limited clinical utility. 58
According to previous studies included in this meta-analysis, the prevalence of anti-DFS70 antibodies among SLE patients was ranged from 0% to 25% (Table 1). The variation in the prevalence of anti-DFS70 antibodies may be multi-factorial, such as inherent variations between ethnic groups, environmental factors, and detection methods.31,44 With respect to ethnicity, previous studies have found that the prevalence of anti-DFS70 antibodies is higher in Asian populations than in non-Asian populations. For example, Hayashi et al. reported a higher prevalence of anti-DFS70 antibodies in Japanese healthy individuals (16.4%) than in American healthy individuals (8.5%). 40 Choi et al. revealed that Canadian and European patients were less likely to have anti-DFS70 antibodies than patients residing in the USA and Asia. 46 In the present study, we found that despite adjusting for ethnicity, the diagnostic performance of anti-DFS70 antibodies in excluding SLE was not statistically significant in Asian, non-Asian, or overall populations. The DOR of anti-DFS70 antibodies for the exclusion of SLE in the overall population was 1.04 (95% CI: 0.59–1.85), whereas the DOR of anti-DFS70 antibodies was 1.58 (95% CI: 0.71–3.54) in the Asian group and 0.84 (95% CI: 0.40–1.77) in the non-Asian group. The reason for this result is unclear at present. Further studies investigating anti-DFS70 antibodies across different populations and geographic regions are needed. Notably, the prevalence of anti-DFS70 antibodies in patients with SLE appears to have more frequently surpassed that observed in HI since 2015 (Table 1). This increasing trend may be attributed to factors including advancements in diagnostic methods, increased clinician awareness of autoimmune diseases leading to more frequent testing, and potential effects related to COVID-19 vaccination. 59 The clinical significance and implications of this rising prevalence remain an area of ongoing research. Subgroup analysis of the DORs by year (before vs after 2015) demonstrated a DOR of 0.57 (95% CI: 0.20–1.58) prior to 2015 and 1.60 (95% CI: 0.88–2.90) thereafter. The present study suggests that the observed temporal increase did not significantly influence the diagnostic performance of anti-DFS70 antibodies.
Several limitations were identified in the present study. Firstly, the number of studies included in this systematic review was limited, which may have resulted in reduced statistical power. Secondly, although numerous studies assessed the positive rate of anti-DFS70 antibodies in patients with SLE, some were excluded due to the absence of data regarding the positive rate of these autoantibodies in healthy individuals. As a result, the pooled findings should be interpreted with caution. Thirdly, the detection method may influence the positive rate of anti-DFS70 antibodies. Cheng et al. reported that the detection of anti-DFS70 antibodies using the CIA method had a higher specificity than other methods,
11
which could potentially influence the final results. However, due to the limited number of studies and the wide variety of detection methods employed, we were unable to perform subgroup analyses. Finally, Infantino et al. found that while the overall prevalence of anti-DFS70 antibodies was similar among ANA associated rheumatic diseases (AARD), non-AARD, and undifferentiated connective tissue disease (UCTD) patients (2.1% [7/333] vs 2.3% [9/384] vs 5.9% [3/51], respectively; p-value = 0.188), monospecific anti-DFS70 antibodies showed a significant distribution difference.
29
The result emphasizes that monospecific anti-DFS70 antibodies may serve as a useful marker for excluding AARD in ANA-positive patients.29,32,38 We further analyzed the role of isolated anti-DFS70 antibodies in the exclusion of SLE and found that the diagnostic odds ratio for excluding an SLE diagnosis was 4.00 (95% CI: 1.39–11.46). When interpreted as a marker of disease exclusion rather than disease presence, the discriminative performance corresponds to an AUC of 0.68, suggesting that isolated anti-DFS70 antibodies may serve as a potential biomarker for excluding SLE. Taken together, these findings suggest that the presence of anti-DFS70 autoantibodies cannot directly exclude SLE in patients with suspected disease. We incorporated anti-DFS70 autoantibody testing and propose an interpretative algorithm for positive ANA findings (Figure 4). In patients with suspected SLE who tested ANA positive, further testing for other SLE-associated antibodies was recommended. Anti-DFS70 antibody testing algorithm in ANA interpretation. This flowchart shows how to approach a positive ANA with a dense fine speckled (DFS) nuclear pattern. The steps include: recognizing the DFS pattern on HEp two cells, checking for clinical suspicion of autoimmune rheumatic disease, testing for disease specific autoantibodies, and confirming anti DFS70. Isolated anti DFS70 (without other autoantibodies) usually indicates low likelihood of systemic autoimmune disease.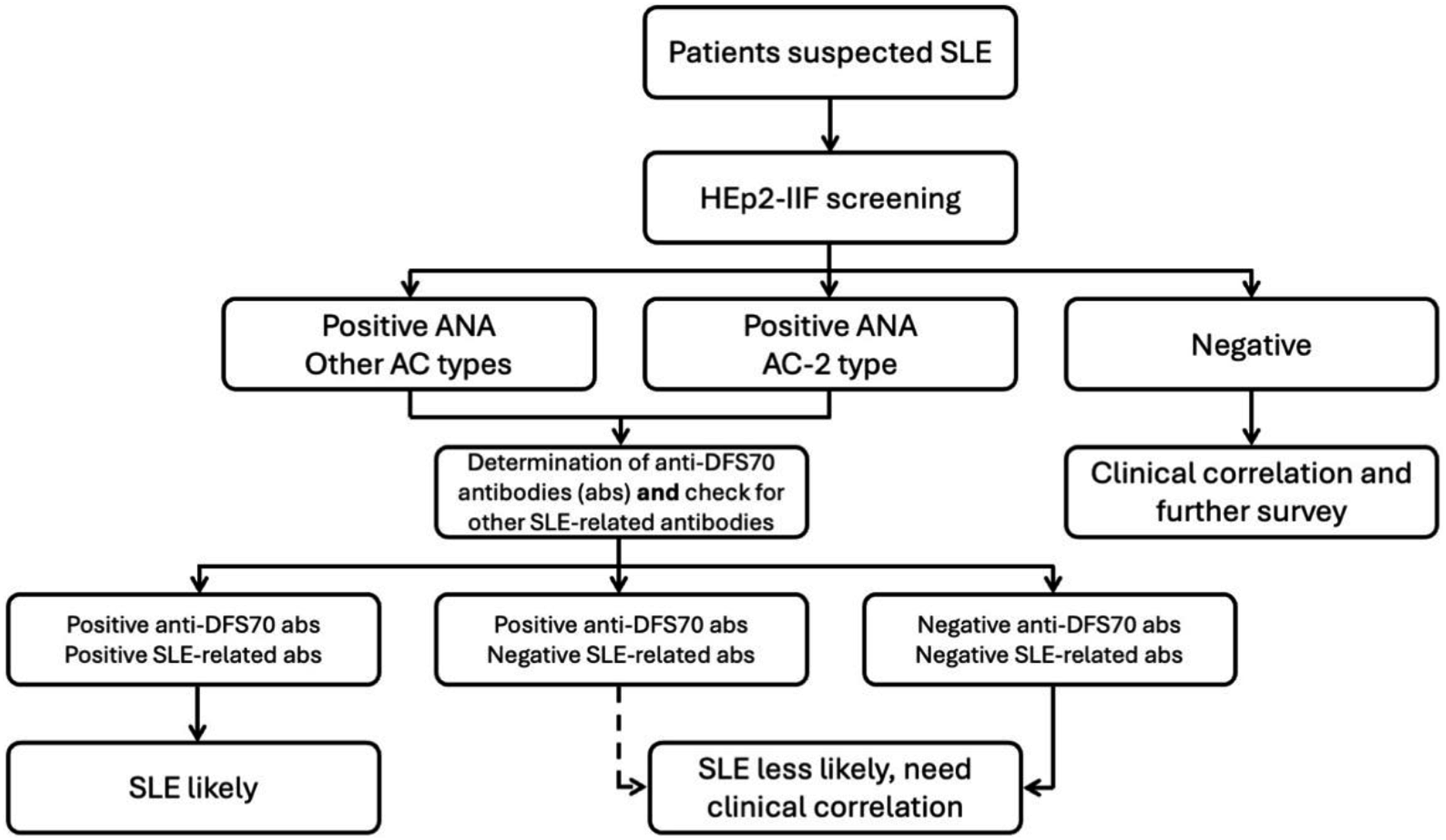
In conclusion, in this systematic review we found that anti-DFS70 antibodies are detected in individuals with SLE at frequencies greater than, or at least comparable to, those observed in healthy individuals. This observation challenges the previously held assumption that anti-DFS70 antibodies are exclusive markers of SARD and highlights the need for comprehensive studies to reach more definite conclusions in the context of SLE diagnosis. Further research is warranted to clarify the diagnostic performance of anti-DFS70 antibodies and to identify more reliable biomarkers for distinguishing SLE from other conditions.
Supplemental material
Supplemental material - Diagnostic performance of anti-DFS70 antibodies in excluding systemic lupus erythematosus diagnosis: An updated systematic review and meta-analysis
Supplemental material for Diagnostic performance of anti-DFS70 antibodies in excluding systemic lupus erythematosus diagnosis: An updated systematic review and meta-analysis by Yu-Chi Hung, Pao-Feng Hsieh, Kuang-Hui Yu in Lupus
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosures
The authors declare no conflicts of interest. All authors contributed to each of the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be submitted.
Data Availability Statement
No new data were created or analysed in this study. Data sharing is not applicable to this article.
Supplemental material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.