
Abstract
Objective
We evaluated the reading & comprehension levels of Systemic Lupus Erythematosus (SLE) Patient educational materials (PEMs) available online, from both nonprofit and for-profit organizations.
Methods
We analyzed PEMs from four nonprofit organizations (American College of Rheumatology [ACR], Lupus Foundation of America [LFA], Lupus Research Alliance [LRA], Lupus Society of Illinois [LSI]) & three for-profit company’s platforms (Aurinia, AstraZeneca, GlaxoSmithKline [GSK]). Reading & comprehension scores were calculated using six standard tools, and comparisons were performed using one-way ANOVA & Tukey’s post-hoc analysis. A p-value ≤0.05 was considered statistically significant.
Results
The average Flesch–Kincaid Grade Level (FKGL) and Flesch Reading Ease Score (FRES) across all PEMs were 10.05 ± 0.70 and 52.68 ± 4.10, respectively. Materials from nonprofit organizations had a FKGL of 10.35 ± 0.88 and a FRES of 51.19 ± 4.91, indicating a reading level requiring 10th- to 12th-grade proficiency. For-profit organizations had a slightly lower FKGL of 9.98 ± 0.42 and a higher FRES of 54.35 ± 2.65. These differences were not statistically significant (p = 0.53 and 0.16). However, significant within-group differences were observed. Among nonprofits, PEMs from LFA had the most favorable readability metrics (FKGL 9.19 ± 0.44, FRES 58.34 ± 3.11), compared to ACR (10.64 ± 0.56, 49.81 ± 2.24), LRA (10.53 ± 0.61, 50.54 ± 2.69), and LSI (11.28 ± 0.45, 45.64 ± 2.03) (p < 0.01). Among for-profits, PEMs from Aurinia had significantly better readability scores (FKGL 9.59 ± 0.46, FRES 55.77 ± 3.05) than those from AstraZeneca (9.93 ± 0.38, 53.13 ± 2.48) and GSK (9.86 ± 0.25, 54.28 ± 2.16) (p < 0.001).
Conclusion
Most SLE patient education materials available online are written at or above a 10th-grade level. These findings highlight the urgent need to improve PEM readability to support patients with lower health literacy.
Keywords
Key points
(1) Online educational resources for patients with SLE exceed the reading levels recommended by health literacy guidelines, which can create difficulties for patients with low health literacy. (2) Nonprofit organizations’ patient educational materials show high variability in complexity, while for-profit organizations’ online patient educational materials are more uniformly complex. (3) Improving readability and incorporating health literacy principles may enhance patient comprehension and engagement in SLE care.
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune, multisystemic disease characterized by periods of disease activity, remission, and unpredictable flares.1,2 The disease also has multidimensional impacts on patients’ lives. In addition to physical symptoms, individuals with SLE often face emotional, psychological, and social challenges, making disease management particularly complex. 3 Disease manifestations may vary depending on the organs involved and the severity of disease, adding to diagnostic challenges for patients and healthcare providers. Post-diagnosis, disease management includes continued surveillance for disease activity and the use of medications that may have significant side effects, necessitating ongoing monitoring for potential adverse effects. 2
A thorough understanding of the disease, available treatments, and self-management strategies is essential for patients with SLE. This knowledge can empower them to participate actively in their care, engage in shared decision-making, adhere to treatment plans, and improve their overall health outcomes.4,5 Patient education materials (PEMs) play a critical role in supporting disease self-management by providing essential guidance on symptom control, treatment options, and lifestyle adjustments that can significantly enhance quality of life.4,5
Despite their importance, many PEMs developed for individuals with SLE are written at a literacy level that exceeds the reading and comprehension skills of the average adult in the United States, particularly those with limited health literacy. Health literacy (HL) refers to an individual’s ability to access, interpret, and use essential health information to make informed medical decisions. HL is a key determinant of health outcomes in chronic conditions such as SLE. 6 Studies show that individuals with limited HL often struggle with effective disease management, leading to increased hospitalizations and greater healthcare costs.7–9
SLE disproportionately affects people of color, 10 a population that also faces challenges related to health literacy, health equity and healthcare disparities, factors that may further compromise disease outcomes.7,11 As such, improving HL is critical to helping patients manage their illness and actively engage in their care.11,12
Both nonprofit (NP) and for-profit (FP) organizations play a vital role in promoting health literacy. Organizational Health Literacy (OHL) refers to the extent to which institutions, such as healthcare organizations, implement strategies to simplify health information, facilitate navigation of the healthcare system, and support patient engagement and self-management. These organizations often serve as key disseminators of educational materials on diseases, medications, and treatment strategies, reaching patients and their families either directly or through healthcare professionals.
The National Institutes of Health (NIH) and the American Medical Association (AMA) recommend that health materials be written at or below a 6th-grade reading level to promote optimal comprehension.13,14 However, there is limited data on the readability of PEMs available for SLE. In 1997, Hearth-Holmes et al. evaluated several printed SLE materials and found that they were written at a high school or college reading level. 15 This complexity may hinder patients’ reading and comprehension of essential educational resources aligned with their health literacy levels.16,17 Research suggests that simplifying language, avoiding medical jargon, and incorporating visual aids can significantly enhance patient understanding and engagement with PEMs.13,18 These strategies have been shown to improve information retention and promote better disease self-management.4,7
Online health resources have proliferated over the last two decades, with more than 45% of SLE patients reporting the Internet as their primary source of health information. 19 During July–December 2022, 58.5% of U.S. adults used the internet to look for health or medical information, with women (63.3%) more likely than men (53.5%); usage peaked among adults aged 30–44 before declining in older age groups. 20 Another survey found that roughly half of the adult population consults the internet for health-related information. 21 These statistics underscore the importance of ensuring that online PEMs are written at a reading level accessible to the general public.
Greater disease knowledge plays a central role in improving patient engagement and clinical outcomes in chronic conditions such as systemic lupus erythematosus (SLE). This includes understanding of disease causes, underlying pathophysiology, treatment rationale, and preventive strategies, which together enhance adherence to therapy and improve clinical outcomes. Patients with a better understanding of their disease are more likely to actively participate in their care, adhere to treatment regimens, and engage in shared decision-making with healthcare providers. Evidence suggests that increased disease knowledge is associated with higher levels of self-efficacy, improved medication adherence, and better overall disease management. 22 In SLE specifically, improved health literacy has been linked to reduced disease activity, enhanced patient–physician communication, and improved quality of life.23–25 Conversely, limited understanding of the disease may contribute to poor adherence, delayed recognition of disease flares, and suboptimal clinical outcomes. These findings underscore the importance of developing patient education materials that are not only accessible but also effective in enhancing patient comprehension and supporting long-term disease management. Despite the ubiquity of online platforms, the quality of freely available health information varies. Evaluations of YouTube videos on stroke rehabilitation and percutaneous tracheostomy found that most videos were of poor quality and contained insufficient information, with only 13 of 100 stroke rehabilitation videos rated high quality 21 and 72 of 100 percutaneous tracheostomy videos judged insufficient. 26 High-quality videos were typically uploaded by academic or physician sources.21,26 These findings highlight the need for reliable, easy-to-understand textual materials produced by trusted organizations to support patient education.
The readability of currently available online PEMs for SLE remains largely unexamined. Regular readability evaluations are necessary to ensure that educational content supports appropriate reading and comprehension and meets the evolving needs of the SLE patient population. 27
Methodology
This study was designed as a cross-sectional quantitative analysis of online patient education materials for SLE to determine whether currently available resources are consistent with recommended reading and comprehension guidelines for patient education.
Between January and April 2025, texts of patient education materials for SLE were systematically collected from both non-profit (NP) organizations and for-profit (FP) pharmaceutical companies. Both entities have differences in mission and resources available to them. Food and Drug Administration approvals for medications for SLE or lupus nephritis are relatively recent (Belimumab 2011–2020; voclosporin 2021, Anifrolumab 2021), hence their online patient centered resources platforms are also relatively recent allowing for comparison between long-established nonprofit advocacy resources and relatively recent industry-sponsored educational platforms that may potentially include recommended approaches to patient education.
The NP organizations included the American College of Rheumatology (ACR), Lupus Foundation of America (LFA), Lupus Research Alliance (LRA), and Lupus Society of Illinois (LSI). These organizations were selected because they are nationally and regionally recognized advocacy and educational bodies that are frequently recommended by healthcare providers and widely accessed by patients and caregivers. The FP organizations, Aurinia (voclosporin), AstraZeneca (Anifrolumab), and GlaxoSmithKline (GSK) (Benlysta), were included.
Only English-language materials intended for patients or caregivers were included. Content designed primarily for healthcare professionals or purely promotional materials were excluded. The materials reviewed covered a range of topics, including disease overviews (pathophysiology, signs and symptoms, diagnosis, and prognosis), medication information (mechanisms of action, benefits, and potential side effects), and lifestyle or self-management recommendations (diet, exercise, pregnancy, sun protection, and mental health). Because available materials differed in focus across organizations and the number of accessible documents was limited, strict topic standardization was not feasible. Instead, all general educational pages available on each website were included to reflect the information realistically accessible to patients. Two representative examples of the materials analyzed, along with their readability scores and suggested simplifications, are provided in the supplemental material.
We analyzed the readability of the collected materials using six established readability and comprehension metrics.
The Flesch–Kincaid Grade Level (FKGL) estimates the educational grade level required to comprehend a text based on sentence length and word difficulty, with higher scores indicating greater reading complexity.
The Flesch Reading Ease Score (FRES) evaluates readability on a scale from 0 to 100, with higher values indicating easier text.
The Gunning Fog Index estimates the years of formal education required to understand a passage by accounting for sentence length and the percentage of complex words.
The Simple Measure of Gobbledygook (SMOG) calculates the grade level based on polysyllabic word counts and is particularly suited for healthcare materials.
The Coleman–Liau Index (CLI) and Automated Readability Index (ARI) estimate grade level using characters per word and words per sentence.
According to recommendations from the National Institutes of Health and the American Medical Association, patient education materials should ideally be written at or below a 6th-grade reading level.13,14 However, because different readability formulas assess text complexity in slightly different ways, indices such as Gunning Fog, SMOG, CLI, and ARI may classify texts as more complex; therefore, scores up to the 8th-grade level are often considered acceptable. The interpretation of numeric readability scores for all metrics used in this study is provided in Supplemental Table S1 to assist readers in understanding what the values represent in terms of reading difficulty. The strengths and limitations of these readability tools in patient education research have been systematically reviewed by Friedman and Hoffman-Goetz. 28
Text from each material was extracted and analyzed using the ReadabilityFormulas.com calculator. For each metric, mean and standard deviation values were calculated across all materials and separately for NP and FP groups. One-way analysis of variance (ANOVA) was performed to compare readability scores between NP and FP organizations. Additional ANOVAs were conducted within each group to identify differences among individual organizations. Post-hoc pairwise comparisons were carried out using Tukey’s Honestly Significant Difference (HSD) test. Effect sizes were calculated using eta squared (η2) for ANOVA and Cohen’s d for pairwise comparisons. The complete scoring process, raw readability outputs, and ANOVA results are provided in the supplemental files for transparency.
NOTE: Readability scores were obtained using a single online calculator. Although this platform provides widely accepted readability indices, prior research has noted that readability values may vary slightly across different calculators due to differences in algorithm implementation. This is discussed further in the limitations section of this study.
Ethical considerations
As this study did not involve human subjects or patient-specific data, ethical approval was not required. All materials analyzed were publicly available on organizational websites, and no personal patient information was involved.
Results
We analyzed a total of 40 patient education materials (PEMs) related to systemic lupus erythematosus (SLE), including 22 documents from nonprofit organizations (American College of Rheumatology [ACR], n = 6; Lupus Foundation of America [LFA], n = 6; Lupus Research Alliance [LRA], n = 5; and Lupus Society of Illinois [LSI], n = 5) and 18 documents from for-profit pharmaceutical companies (Aurinia, n = 6; AstraZeneca, n = 6; and GlaxoSmithKline [GSK], n = 6). Across all sources combined, the average Flesch–Kincaid Grade Level (FKGL) was 10.05 ± 0.70, and the average Flesch Reading Ease Score (FRES) was 52.68 ± 4.10, corresponding to a reading level at or above the 10th grade.
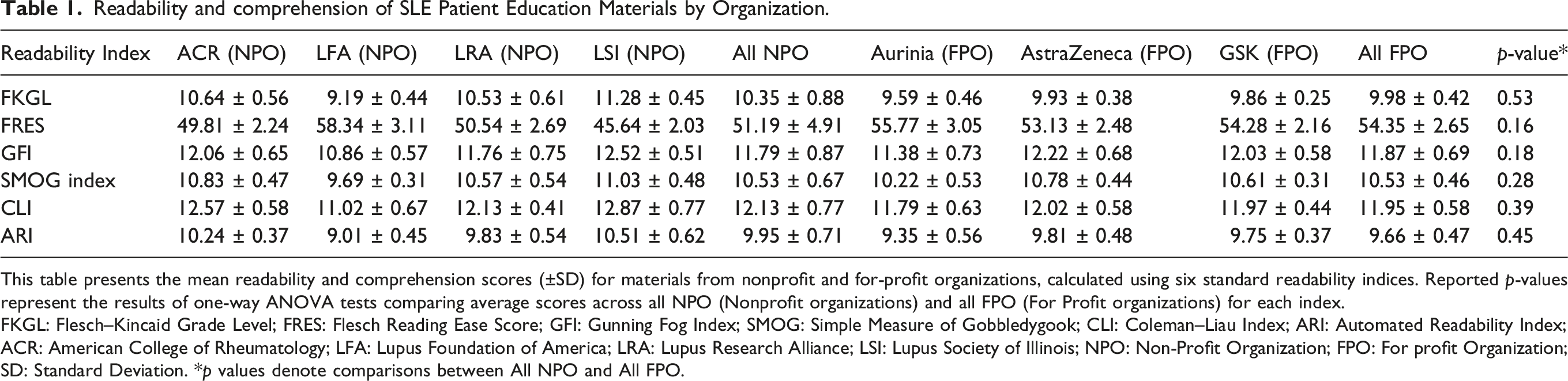
All patient education materials for SLE across the seven organizations were written above the NIH-recommended 6th-grade reading level (Figure 1). All online PEM sources were at or above the 9th-grade level. Table 1 presents the mean readability scores (± standard deviation) for each readability index, organized by source. These findings informed subsequent statistical comparisons by organization type (nonprofit vs for-profit) and by individual source. Average readability scores for nonprofit and for-profit SLE patient education materials across six indices, compared to the NIH-recommended readability level (≤6th grade, dashed line). All materials exceeded this recommended threshold. Differences between nonprofit and for-profit groups were not statistically significant across any index (all p > 0.05). Abbreviations: SLE: Systemic Lupus Erythematosus; NIH: National Institutes of Health; FKGL: Flesch-Kincaid Grade Level; FRES: Flesch Reading Ease Score; GFI: Gunning Fog Index; SMOG: Simple Measure of Gobbledygook; CLI: Coleman–Liau Index; ARI: Automated Readability Index. Readability and comprehension of SLE Patient Education Materials by Organization. This table presents the mean readability and comprehension scores (±SD) for materials from nonprofit and for-profit organizations, calculated using six standard readability indices. Reported p-values represent the results of one-way ANOVA tests comparing average scores across all NPO (Nonprofit organizations) and all FPO (For Profit organizations) for each index. FKGL: Flesch–Kincaid Grade Level; FRES: Flesch Reading Ease Score; GFI: Gunning Fog Index; SMOG: Simple Measure of Gobbledygook; CLI: Coleman–Liau Index; ARI: Automated Readability Index; ACR: American College of Rheumatology; LFA: Lupus Foundation of America; LRA: Lupus Research Alliance; LSI: Lupus Society of Illinois; NPO: Non-Profit Organization; FPO: For profit Organization; SD: Standard Deviation. *p values denote comparisons between All NPO and All FPO.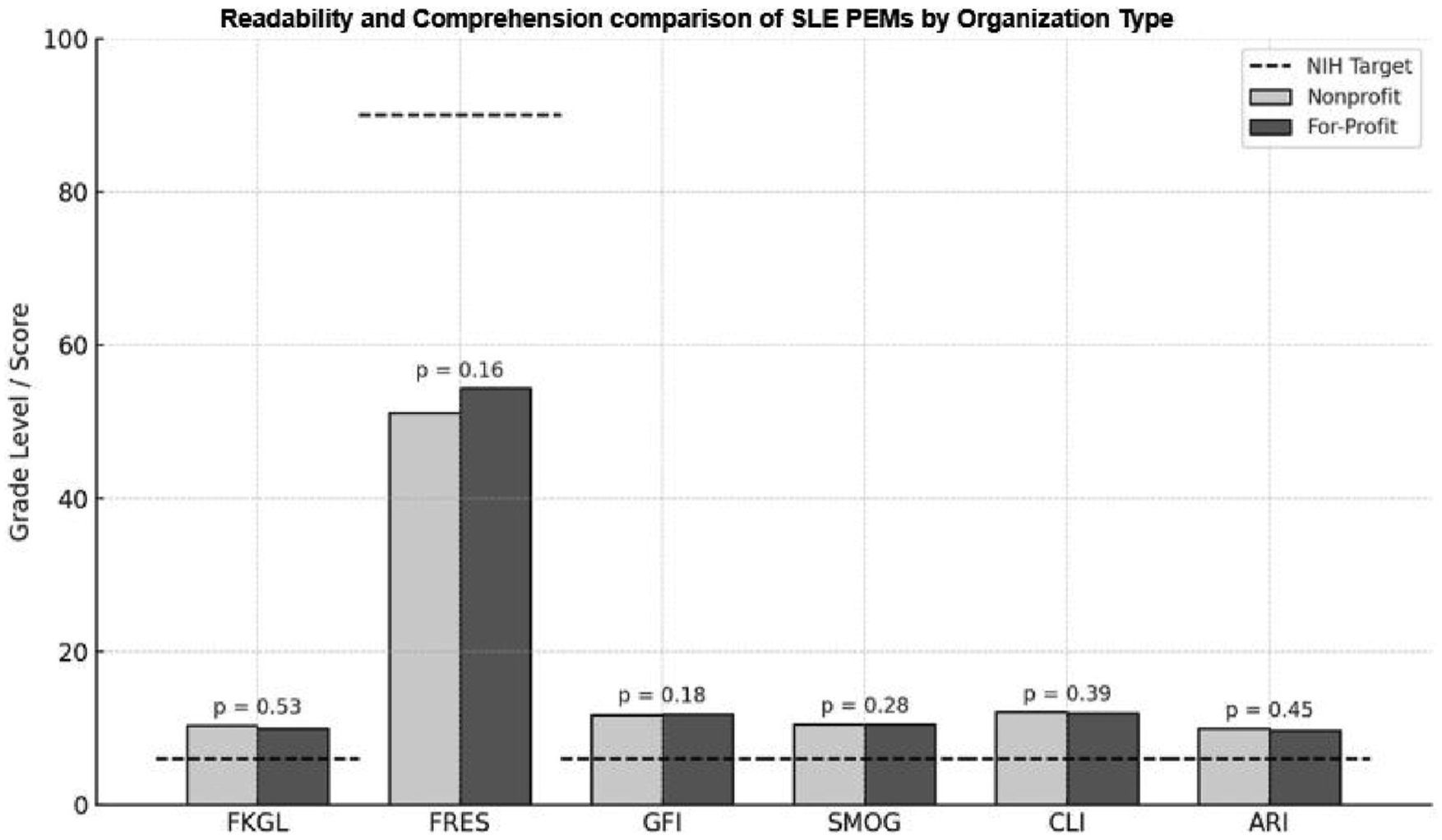
Readability metrics by organization type (nonprofit vs for-profit)
The average FKGL was 10.35 ± 0.88 for nonprofit organizations and 9.98 ± 0.42 for for-profit organizations (p = 0.53). When aggregated, PEMs from nonprofit organizations had slightly higher reading and comprehension levels, with an FKGL of 10.35 ± 0.88 and a FRES of 51.19 ± 4.91, compared to PEMs from for-profit organizations, which had an FKGL of 9.98 ± 0.42 and a FRES of 54.35 ± 2.65. However, these differences were not statistically significant (p = 0.53 for grade level; p = 0.16 for reading ease). For reference, a FRES between 50 and 60 corresponds to a 10th- to 12th- grade reading level. Table 1 summarizes the readability scores across all organizations.
Among nonprofit organizations, the Lupus Society of Illinois (LSI) had the most difficult materials to read, with the highest average FKGL (11.28 ± 0.45) and the lowest average FRES (45.64 ± 2.03), indicating more complex content that may be challenging to comprehend. A FRES between 30 and 50 corresponds to a college-level reading difficulty. In contrast, the Lupus Foundation of America (LFA) provided PEMs that were comparatively easier to read and understand, with an average FKGL of 9.19 ± 0.44 and an average FRES of 58.34 ± 3.11. PEMs from for-profit sources, the reading and comprehension demands were more consistent across the three pharmaceutical companies, Aurinia, AstraZeneca, and GSK, which collectively averaged a mean FKGL of 9.98 ± 0.42 and a FRES of 54.35 ± 2.65. This suggests materials that are moderately challenging but more uniform in their demands.
To evaluate differences in the readability of patient education materials for SLE across individual organizations, one-way ANOVA tests were conducted using both FKGL and FRES as dependent variables. Among nonprofit organizations, statistically significant differences were found in both FKGL (F (3, 18) = 117.88, p < 0.001) and FRES (F (3, 18) = 144.60, p < 0.001), with large effect sizes (η2 = 0.95 and η2 = 0.79, respectively), indicating that differences among nonprofits accounted for 95% of the variability in FKGL and 79% in FRES. For example, materials from LFA had the lowest average FKGL (9.19 ± 0.44) and highest average FRES (58.34 ± 3.11), while those from LSI had the highest average FKGL (11.28 ± 0.45) and lowest average FRES (45.64 ± 2.03), reflecting significantly more complex material.
Among for-profit organizations, ANOVA also revealed significant differences in FKGL (F (2, 15) = 21.73, p < 0.001) and FRES (F (2, 15) = 3.23, p = 0.045), though the effect sizes were smaller (η2 = 0.74 and η2 = 0.07, respectively). Aurinia’s materials were the most readable, with an average FKGL of 9.59 ± 0.46 and an average FRES of 55.77 ± 3.05, compared to AstraZeneca (FKGL = 9.93 ± 0.38; FRES = 53.13 ± 2.48) and GSK (FKGL = 9.86 ± 0.25; FRES = 54.28 ± 2.16). While the variation in FRES was more limited, the FKGL differences were more pronounced. Importantly, across all organizations, the average reading and comprehension demands still exceed the NIH and AMA recommendation that PEMs be written at or below a 6th-grade reading level, corresponding to a FRES of 90 or higher. Figure 1 illustrates the average readability and comprehension scores for nonprofit and for-profit patient education materials for SLE across all indices.
Because ANOVA tests only indicate overall differences, Tukey’s Honestly Significant Difference (HSD) test was conducted to identify specific pairs with significant variation. All results below are based on FKGL. As shown in Figure 2, LFA’s materials were significantly easier to read than those from LRA (mean difference = −1.40, p = 0.009) and LSI (mean difference = −2.10, p = 0.002). ACR PEMs were significantly more difficult than LFA’s (mean difference = 1.50, p = 0.001). Additional comparisons such as ACR versus LSI and LRA versus LSI also reached significance (p < 0.001), confirming substantial variability in FKGL among nonprofit PEMs. Tukey’s HSD test comparing Flesch–Kincaid Grade Level scores across organizations. (ns) indicates non-significant comparisons (p > 0.05). Negative values indicate the first group’s materials are easier to read; positive values favor the second group. Note. Exact p-values are reported in the Results section. Values shown as “p < 0.001” in the figure represent comparisons below the reporting threshold.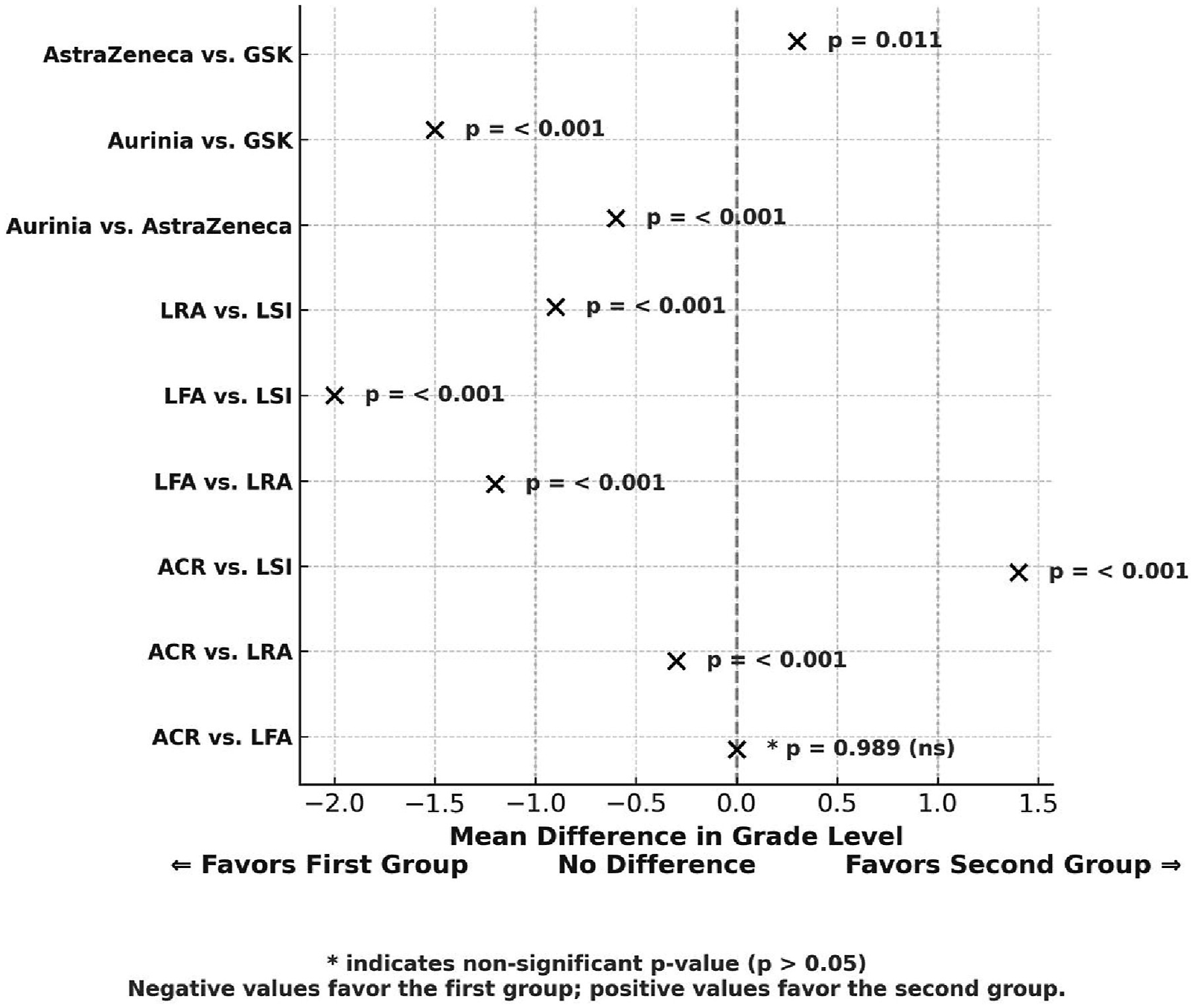
Among for-profit organization PEMs, several pairwise comparisons reached statistical significance based on FKGL. Specifically, Aurinia’s materials were significantly easier to read than those from AstraZeneca (p < 0.001) and GSK (p < 0.001). Although the FKGL difference between AstraZeneca and GSK was also statistically significant (p = 0.011), the effect size was small to moderate (Cohen’s d = 0.39), suggesting a limited practical difference in readability.
Discussion
Patients with SLE have expressed a significant need for education, particularly in areas related to self-care, understanding the disease process, and receiving emotional support. 29 In a qualitative study, newly diagnosed SLE patients described the available information as limited and difficult to understand, leaving them with feelings of fear and confusion. For most patients, there was a clear gap between the information they sought and what was provided at diagnosis. Participants reported that the information and support offered at the time of diagnosis were inadequate to meet their needs. 30
To help guide organizational health literacy, we evaluated the reading, and comprehension demands of the currently available online PEMs for lupus. In our study, we found that existing online patient education materials for SLE, whether produced by nonprofit or for-profit organizations, consistently exceeded the recommended 6th-grade reading and comprehension levels. While nonprofit materials exhibited greater variability, for-profit materials were more uniform but still written above the recommended thresholds. These findings underscore a critical gap between the reading and comprehension levels of available online educational content and the literacy skills of the target patient population. Enhancing the clarity of patient education materials for SLE is essential to improve patient reading and comprehension, support self-management, and advance health equity in lupus care.
The patient education materials reviewed in this study were, on average, written at or above the 10th-grade reading and comprehension level. Materials written at high school or college reading levels are likely to be challenging for a large segment of the patient population.6,9 Many adults, including those with SLE, read at or below a middle school level; thus, a pamphlet or webpage requiring an 11th- or 12th-grade reading ability may exceed the comprehension skills of many readers.13,31 Consequently, patients may struggle to understand crucial information about disease symptoms, treatment options, or self-care strategies.12,31 This mismatch between material complexity and patients’ reading skills can undermine effective disease self-management, 11 especially with those with limited health literacy.
The findings of this study have important implications for patient health literacy, and the reading and comprehension demands in SLE care. Prior research has shown that low health literacy is associated with poorer health outcomes, including higher hospitalization rates and lower use of preventive services. 32 In the context of lupus, if patients cannot fully understand their condition or treatment plans due to overly complex language, they may be less likely to adhere to medications, recognize warning signs of flares, or communicate effectively with healthcare providers, ultimately having a negative impact on their health outcomes. Maheswaranathan et al. reported lower patient activation, reduced self-efficacy, higher disease damage, increased disease activity, and worse patient–physician communication among SLE patients with limited health literacy compared to those with adequate health literacy. 23 Moreover, patients with limited health literacy experienced a lower quality of life, greater levels of stress, and were nearly 2.5 times more likely to suffer from depression and anxiety disorders compared to those with adequate health literacy. Similarly, in childhood-onset SLE, 67% of youth demonstrated inadequate functional health literacy, as measured by the Brief Health Literacy Screen (BHLS). Higher BHLS scores were associated with improved medication adherence and better quality of life. 24
The high reading and comprehension demand of current patient education materials for SLE pose a significant barrier, particularly for vulnerable groups such as those with limited formal education or for whom English is not a first language. 33 Notably, even nonprofit organizations, many of which have an educational mission, often produce materials at reading levels beyond the average patient’s capacity. Simply being a nonprofit or patient-focused entity does not guarantee content aligned with recommended reading and comprehension guidelines. Both nonprofit and for-profit providers appear to face similar challenges in simplifying medical information, indicating a systemic issue in health communication.
There is a paucity of studies evaluating health literacy in SLE. Hearth-Holmes et al. (1997) reported that SLE patients had an average reading ability at the 7th–8th grade level, yet many PEMs available at the time from organizations such as the Arthritis Foundation, U.S. Department of Health and Human Services, Louisiana Lupus Foundation, and others were written at high school or college reading levels. 15 Specifically, materials from the Lupus Foundation of America (LFA), Dubois’ Lupus Erythematosus textbook, and the Arthritis Foundation ranged from a 7th- to 15th-grade reading level. 15 Similarly, a recent review reported limited health literacy in four of six studies of SLE patients, with 8% to 48% of patients across those studies classified as having low health literacy. 34 More than one-third (38%) of participants in the California Lupus Epidemiology Study were found to have low health literacy. 25
Some experts have cautioned against oversimplifying lupus PEMs, arguing that materials should cater to patients across a range of literacy levels. 35 These differing viewpoints suggest the need for balance, PEMs must be improved to support better reading and comprehension without omitting necessary medical details, ensuring that they meet the needs of patients with varied literacy skills.
Strengths and limitations of this study
A key strength of this study is the direct comparison of readability across multiple widely accessed non-profit and for-profit organizations that serve as primary sources of SLE information for patients and caregivers. The use of six validated readability metrics provides a comprehensive evaluation of textual complexity from multiple perspectives. By analyzing materials that patients realistically encounter online rather than selectively sampling only high-quality examples, this study offers practical insight into how current educational resources align with health literacy recommendations. The inclusion of both advocacy-based and industry-sponsored educational platforms enhances the generalizability of these findings and highlights sector-wide challenges in producing accessible patient education.
Despite the strengths of this study in highlighting readability concerns, several limitations should be acknowledged. First, the sample PEMs analyzed may not represent the full spectrum of SLE-related resources currently in circulation. This study focused on online PEMs from well-established nonprofit and for-profit organizations based in the United States, as these are widely available and have broad reach. Materials in other languages or from international sources were excluded; therefore, these findings primarily apply to English-language PEMs and may not generalize to multilingual materials or alternative content formats, such as videos or audio resources. Additionally, we did not evaluate any PEMs that did not require access to a computer or the internet. Accessing online PEMs assumes a certain level of dexterity, vision, and coordination, in addition to indicating the availability of resources. We focused on online PEMs because prior research shows that over 45% of SLE patients use the internet as their primary source of health information. 19
Our broad classification of materials into “nonprofit” and “for-profit” categories may also overlook important differences within each group. For example, content from a government health agency and a national lupus organization, both nonprofits, may vary significantly in tone, style, and reading demands. Similarly, commercial health websites may present information differently from pharmaceutical companies. These distinctions were not explored in this study and may warrant further research.
Another limitation is the reliance on standard readability formulas as proxies for reading and comprehension, and not a direct assessment from patients themselves. In addition, readability scores were generated using a single online readability calculator. Tools such as the Flesch–Kincaid Grade Level primarily assess sentence length and word complexity but do not account for conceptual density, document layout, or the presence of unfamiliar medical terminology. 3 Materials may technically meet lower grade-level standards yet remain difficult to understand due to specialized language or assumptions about prior knowledge. This is particularly relevant in SLE-related content, where the use of medical terms such as systemic lupus erythematosus, anti-nuclear antibody, or medications like azathioprine and rituximab are often unavoidable. These terms inherently raise readability scores despite being medically necessary.
Conversely, materials that exceed recommended reading levels may still be user-friendly if they include explanatory tools such as glossaries, analogies, or visual aids, elements not captured by standard readability formulas. Additionally, this study did not assess the usability or design features of PEMs (e.g., font size, visual layout, or cultural sensitivity), all of which play significant roles in comprehension. Finally, this study was cross-sectional, evaluating materials at a single point in time. As PEMs are periodically revised and updated, ongoing monitoring will be necessary to assess trends in reading and comprehension demands over time.
Beyond patient education, digital and social media platforms also play an increasingly important role in the dissemination and visibility of scientific research.
AI-based tools have shown variable readability and inconsistency in adherence to evidence-based guidance, with concerns regarding accuracy and transparency of information. 26 Video-based platforms such as YouTube are widely used but have been shown to contain a substantial proportion of incomplete or low-quality medical content. 22 In contrast, institutional PEMs are generally more reliable and evidence-based but often exceed recommended reading levels, limiting accessibility for patients with lower health literacy. These differences highlight a trade-off between accessibility, readability, and reliability across commonly used health information sources. In comparison, the PEMs analyzed in this study represent structured, institutionally developed educational resources that generally prioritize accuracy and evidence-based content; however, similar to findings reported across other studies of online patient education materials, they remain written above recommended readability levels. Therefore, while platforms such as AI tools and YouTube may offer greater perceived accessibility and rapid information delivery, they demonstrate greater variability and reduced reliability, whereas PEMs provide higher informational validity but at the cost of accessibility for patients with limited health literacy. Similar concerns have been reported across multiple specialties, including rheumatology, cardiology, orthopedics, anesthesiology, intensive care, and spine surgery.36–40
We recommend integrating key health literacy principles into PEM development. These include the use of plain language and avoidance of unnecessary jargon. For example, “inflammation in the kidney from lupus” is preferred over “lupus nephritis.” When technical terms are necessary, brief explanations or analogies should be included. Simplifying sentence structures by breaking long, complex sentences into shorter, single-idea statements improves comprehension. 13 These recommendations are supported by consistent findings across multiple specialties, where PEMs frequently exceed national readability benchmarks and may hinder patient understanding.36–40
The use of diagrams, illustrations, or infographics can reduce cognitive load, while careful attention to layout and visual cues may enhance navigation. Involving patients in content development, pre-testing materials with focus groups, and assessing comprehension with standardized tools like the Patient Education Materials Assessment Tool (PEMAT) 10 can guide meaningful revisions. Including readability scores directly on PEMs and offering more advanced versions for patients with higher literacy levels may further personalize and improve the patient’s experience.
Conclusion
Currently available online patient education materials (PEMs) for individuals with systemic lupus erythematosus are written at or above a 10th-grade reading and comprehension level. These materials are not appropriate for patients with limited health literacy and do not align with nationally recommended guidelines, which advise that PEMs be written at or below a 6th-grade level to support adequate reading and comprehension. Addressing these gaps is essential to improve understanding of patients, promote effective disease self-management, and enhance health outcomes for individuals living with SLE, especially among those with limited health literacy.
Supplemental material
Supplemental Material - Evaluating the readability and comprehension of patient education materials for Systemic Lupus Erythematosus (SLE) available online
Supplemental Material for Evaluating the readability and comprehension of patient education materials for Systemic Lupus Erythematosus (SLE) available online by Nagoor Shaik, Ugochukwu C Nweke, and Meenakshi Jolly in Lupus
Supplemental material
Supplemental Material - Evaluating the readability and comprehension of patient education materials for Systemic Lupus Erythematosus (SLE) available online
Supplemental Material for Evaluating the readability and comprehension of patient education materials for Systemic Lupus Erythematosus (SLE) available online by Nagoor Shaik, Ugochukwu C Nweke, and Meenakshi Jolly in Lupus
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a philanthropic grant from the Brewer Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.