
Abstract
Background/Purpose
Mycophenolate compound (MMF, to represent both mycophenolate mofetil and mycophenolic acid) is an immunosuppressant used to treat Systemic Lupus Erythematosus (SLE). Due to its teratogenicity, the FDA recommends universal mycophenolate Risk Evaluation and Mitigations Strategies (MREMS) to prevent unplanned pregnancies and minimize fetal exposure. This quality improvement initiative aimed to improve documentation of the MREMS protocol in the encounter clinic note from 0% to 75% within 14 months.
Methods
The project was conducted in an academic lupus clinic from February 2023 to May 2024, with the intervention beginning in March 2023. MREMS was recommended for adult female SLE patients aged 18–50 on MMF, excluding those with hysterectomy. Interventions included provider and nurse education, nursing algorithms for identifying eligible patients and ordering pregnancy tests, electronic health record template updates, and regular feedback. Required documentation included counseling on MMF teratogenicity and contraception, with pregnancy testing at each visit. Control charts monitored documentation of MREMS counseling and pregnancy testing, and a one-year post-implementation follow-up was completed.
Results
Among eligible encounters (n = 89), MREMS documentation increased from 0% to an average of 24% during the first 8 months of PDSA cycles, then shifted to an average of 67% of encounters. We reached and sustained our documentation goal of 75% for the last three consecutive months. Pregnancy-test ordering rose from 0% to 63%, and contraception was documented at 98% of visits. Over the course of the intervention, no pregnancies were exposed to MMF. MREMS documentation and pregnancy screening remained above 75% of encounters 1 year after intervention.
Conclusion
Using quality improvement cycles, we incorporated a two-part MREMS protocol into a busy academic lupus clinic, with improved documentation and pregnancy screening.
Problem
Adherence to MREMS documentation was low in an academic lupus clinic leaving patients at risk for teratogenic exposure of MMF during pregnancy. In this quality improvement project, the aim was to identify, study, and implement iterative changes to clinic procedures to increase adherence to MREMS documentation and pregnancy screening in provider clinic notes from 0% to 75% in 14 months.
Background
Mycophenolate compound (MMF, to include mycophenolate mofetil (Cellcept) and mycophenolic acid (Myfortic), is an immunosuppressant medication that is commonly used in Systemic Lupus Erythematosus (SLE) for induction and maintenance therapy of lupus nephritis, as well as many other manifestations of SLE. 1 Post marketing surveillance studies of MMF revealed increased first trimester pregnancy loss (>40%) and congenital malformations (20%) of live born infants in women exposed to MMF. 2 Due to these safety concerns, the FDA agreed on a universal Risk Evaluation and Mitigation Strategies for all MMF (MREMS) with an aim to prevent unplanned pregnancies in patients treated with mycophenolate products, minimize fetal exposure, and collect information on pregnancy outcomes. 3
Current MREMS recommendations consist of four main steps. The first step is education to providers on the embryo-fetal toxicity associated with MMF. Second, during encounters with females of reproductive age, providers should counsel on risks of MMF during pregnancy (miscarriage, birth defects) and adequate birth control options. Third, pregnancy screening is recommended prior to start of treatment, 8-10 days later and reassessed on every encounter thereafter. Fourth, in the event of a positive pregnancy, the provider should report the pregnancy to the Mycophenolate Pregnancy Registry.
Despite its presence for over a decade, the impact of the MREMS on clinical practice is not clear. 4 A recent study, reported only 37% of rheumatologist correctly identified MMF as a teratogenic medication. 5 This is of concern, as MMF remains one of the most commonly used immunosuppressants used for SLE treatment in the United States 6 and SLE patients are often of reproductive age and on a teratogenic medication. 7 Moreover, unplanned pregnancies in the SLE population can be as high as 40%. 8 An evaluation of private insurance claim databases demonstrated that since MREMS establishment, although MMF initiation has decreased during pregnancy (i.e., prescribers evaluating pregnancy status prior), conception rates while on the medication has not changed. 9
There are limited studies evaluating strategies to improve adherence and incorporation of MREMS into rheumatology clinical practice. 10 Given these gaps, we developed a quality improvement initiative to increase MREMS adherence within a rheumatology lupus dedicated clinic.
Methods
Clinic
The quality initiative took place at the Duke Lupus Clinic (DLC). This is a weekly clinic dedicated to patients with SLE, with a range of 30-50 patients seen daily. The clinic is staffed by seven rheumatologists with rotating rheumatology fellows, residents and advanced practice providers. It has a standardized note template used for all DLC patient encounters. Patients complete standardized patient-reported outcome measures at each visit that include questions about contraception and pregnancy planning. All patients are also invited to participate in the Duke Lupus Registry (DLR) (IRBPro00008875), sub-studies (IRB Pro00094645), with over 80% of lupus patients seen in the DLC also enrolled in the DLR.
All patients meeting 1997 American College of Rheumatology (ACR) criteria 11 for SLE seen in the DLC, are invited to enroll in the DLR. Once they accept, they sign a consent form that allows collection and storage of medical information, blood and urine samples throughout their following visits or until withdrawal. At each clinic visit, patients within the DLC complete an intake form either on paper or within medical record that includes questions about their current quality of life, lupus activity, and several preventive health measures.
The clinic has a high contraception documentation rate, 12 but had not included MREMS adherence or performing pregnancy screening. Therefore, implementing MREMS documentation was deemed feasible within this clinical setting.
Population
Eligible participants included females age 18-50 in the DLR, with an active prescription for MMF, and seen within an in-person visit. Participants with tubal ligation were included given potential for reversibility. We excluded patients who were post-menopausal or had total hysterectomy. We also excluded telemedicine encounters.
Design
The project was conceived in February 2023 with interventions implemented from March 2023 to May 2024. We performed an initial retrospective chart review and confirmed no MREMS documentation was taking place prior to intervention. We then proceeded to develop feasible and practical approaches for MREMS counseling, documentation and pregnancy screening within the DLC clinic. While clinical practice was implemented across DLC patients, the quality improvement chart review and data analysis only included consented DLR participants. The team identified several primary drivers essential to reaching these goals: (1) provider participation, (2) nurse education, (3) integration of the intervention into the clinical workflow, (4) standardization of clinical documentation, and (5) streamlined recognition of eligible patients. The key driver diagram served as a visual framework to align the multidisciplinary team, prioritize interventions, and monitor progress toward the project aim (Figure 1). A QI team consisting of lupus clinic director, reproductive rheumatologist and fellow was formed and developed a two-step MREMS protocol. We educated providers and nurses on the protocol which included: (1) Required encounter note documentation of counseling of teratogenic nature of MMF and need for contraception and (2) Ordering of pregnancy screening test at each visit. Driver diagram illustrating the drivers and interventions contributing to the aim of increasing the percentage of encounters with MREMS counseling, documentation and pregnancy test screening. MREMS, Mycophenolate Risk Evaluation and Mitigation Strategies.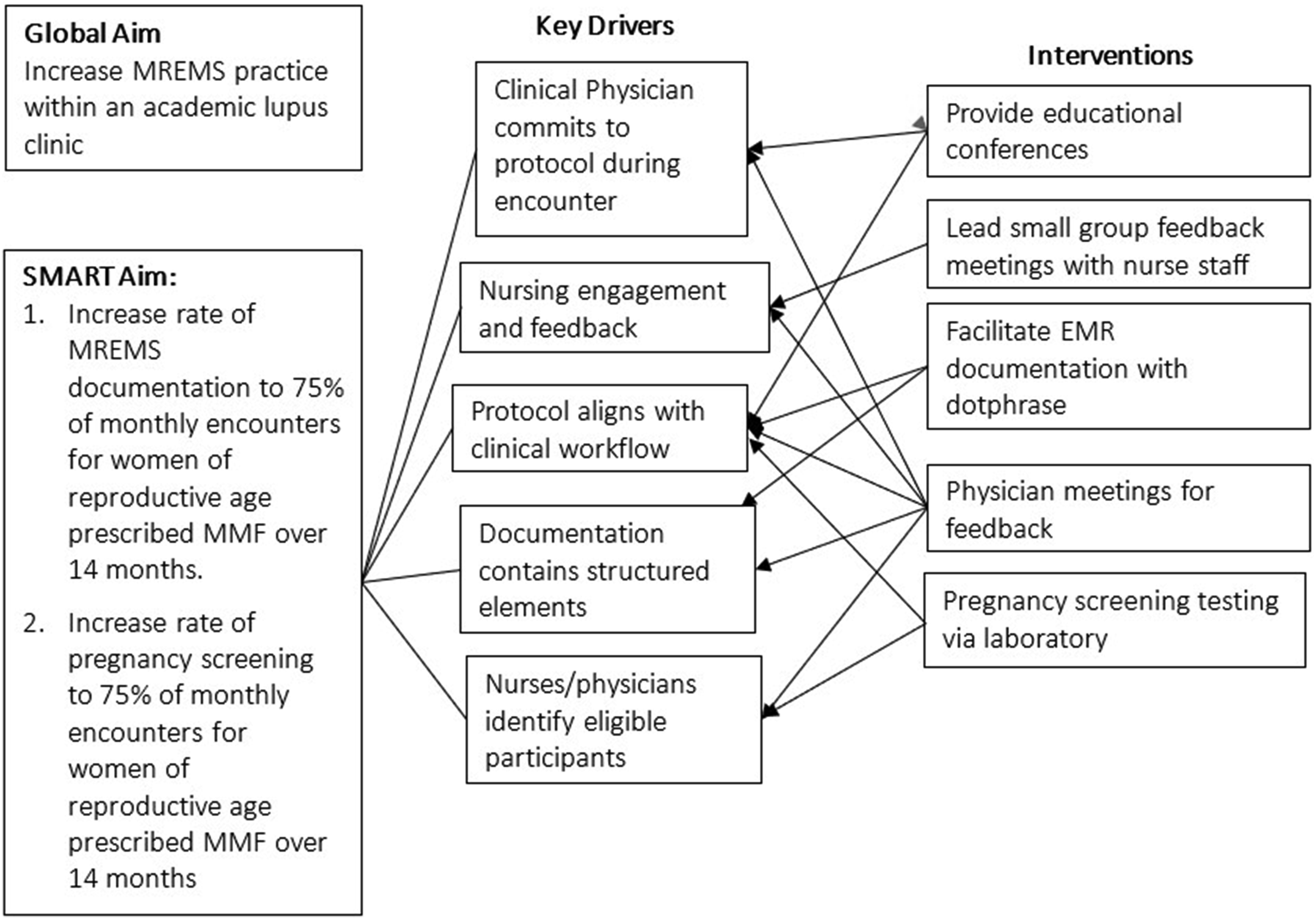
Strategy
Detail of challenges, changes and lessons learned at each PDSA cycle during the intervention.
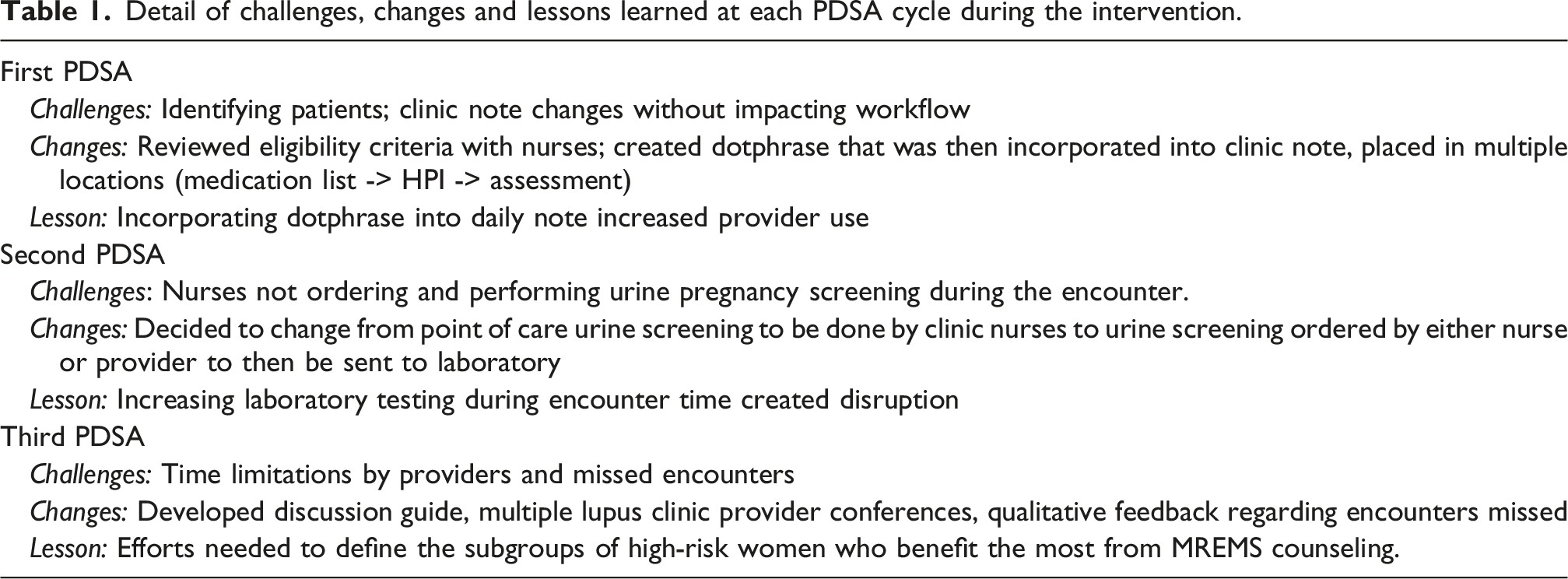
In our second PDSA cycle, we developed multiple sessions for provider and nurse feedback. The primary challenge was the variability in pregnancy screening completion, with samples not being completed prior to the end of the clinic encounter. Nurses found point-of-care testing difficult due to their clinic responsibilities and demands during the day. Given challenges with timing and workflow, we changed the initial goal of point-of-care urine pregnancy testing during the clinic encounter to sending urine samples to the laboratory for urine pregnancy testing with results released after the visit.
Finally, we had quarterly QI team feedback sessions focusing on missed encounters. We gave a case-based conference to DLC providers highlighting missed encounters and detailing visit characteristics and patient demographics. This helped clarify participant eligibility and protocol completion requirements. Provider notes on limitations and barriers implementing MREMS during the encounter were also collected. Finally, we developed an MREMS discussion guide to facilitate discussion during the encounter. (Supplemental 1).
Electronic health records (EHR)
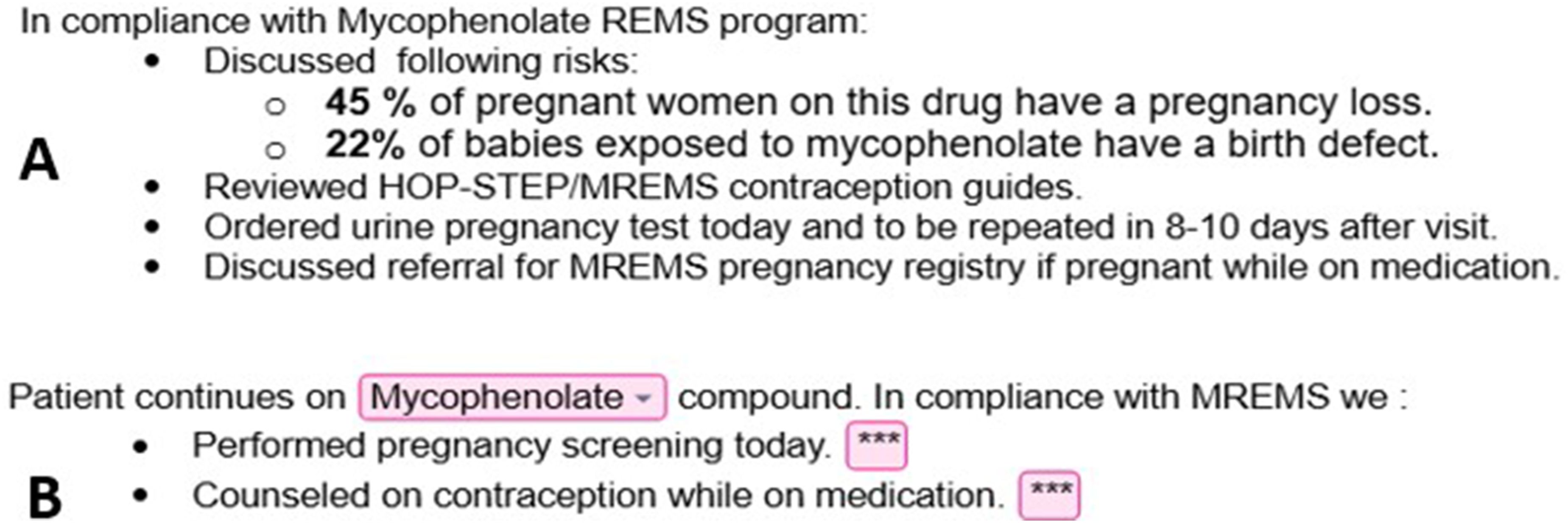
The Duke Health System uses Epic (Verona, Wisconsin, USA). Which allows clinical notes to be embedded with Epic Smartphrases (also known as a dot phrases). We developed an MREMS dotphrase within the standardized clinic note template (Figure 1).
Primary outcome
The primary outcome of interest was completion of MREMS documentation per encounter. MREMS protocol two essential components (1) documentation discussion of teratogenic risk and (2) documentation of contraception (Figure 2). As secondary outcomes we collected Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) mean and clinical scores, measured the frequency of laboratory pregnancy screening at each encounter and the type of contraception chosen by our participants. We assessed the success rate by which providers followed the MREMS protocol during encounters by weekly chart review. We could then follow the trend of our post intervention measurements through the end of each PDSA cycle. We continued cycles until we reached our goal of 75% of eligible encounters meeting protocol.
As process measures we included number of reproductive age women seen during that clinic day to see if this impacted rate of documentation, as well as assessing provider acceptability and limitations through feedback sessions with the project team.
Analysis
This was a QI study using the Method for Improvement framework. Baseline data collection occurred in March 2023 as we looked retrospectively at February 2023. New data were gathered monthly following implementation. Analysis of the primary outcome measure of MREMS completion rate was performed via a p chart, a statistical process control chart, in Microsoft Excel (Redmond, Washington, USA). Upper and lower control limits were defined by ± 3 standard deviations. Special cause was determined by a shift with ≥8 consecutive data points above the centerline. The centerline, or mean, was adjusted for a shift in the data. 13 Descriptive statistics were used to describe outcome measures regarding contraception use among participants. Disease activity measures were summarized as mean (standard deviation) and compared between encounters with and without MREMS documentation using independent-samples t tests.
Results
Among eligible encounters (n = 89), MREMS documentation increased from 0% (no prior MREMS documentation) to an average of 24% following process improvements generated through PDSA cycles in the first 8 months. This then shifted to an average of 67% of encounters as we continued the intervention for a total of 14 months. We reached and sustained our documentation goal of 75% for the last three consecutive months (Figure 3). No significant association was observed between SLE disease activity at time of visit (based on SLEDAI score) and adherence to MREMS documentation. Control Chart of percent of eligible encounters with MREMS documentation including prior to intervention on February 2023 and then throughout intervention from March 2023 to May 2024. Interventions throughout PDSA cycles described per month in text boxes. Target goal of 75% green line. n= number of eligible visits per month. Upper and lower control limits were defined by ± 3 standard deviations. Special cause was determined by a shift with ≥ 8 consecutive data points above the centerline. The centerline, or mean, was adjusted for a shift in the data. Abbreviations: DLC, duke lupus clinic, QI, quality initiative.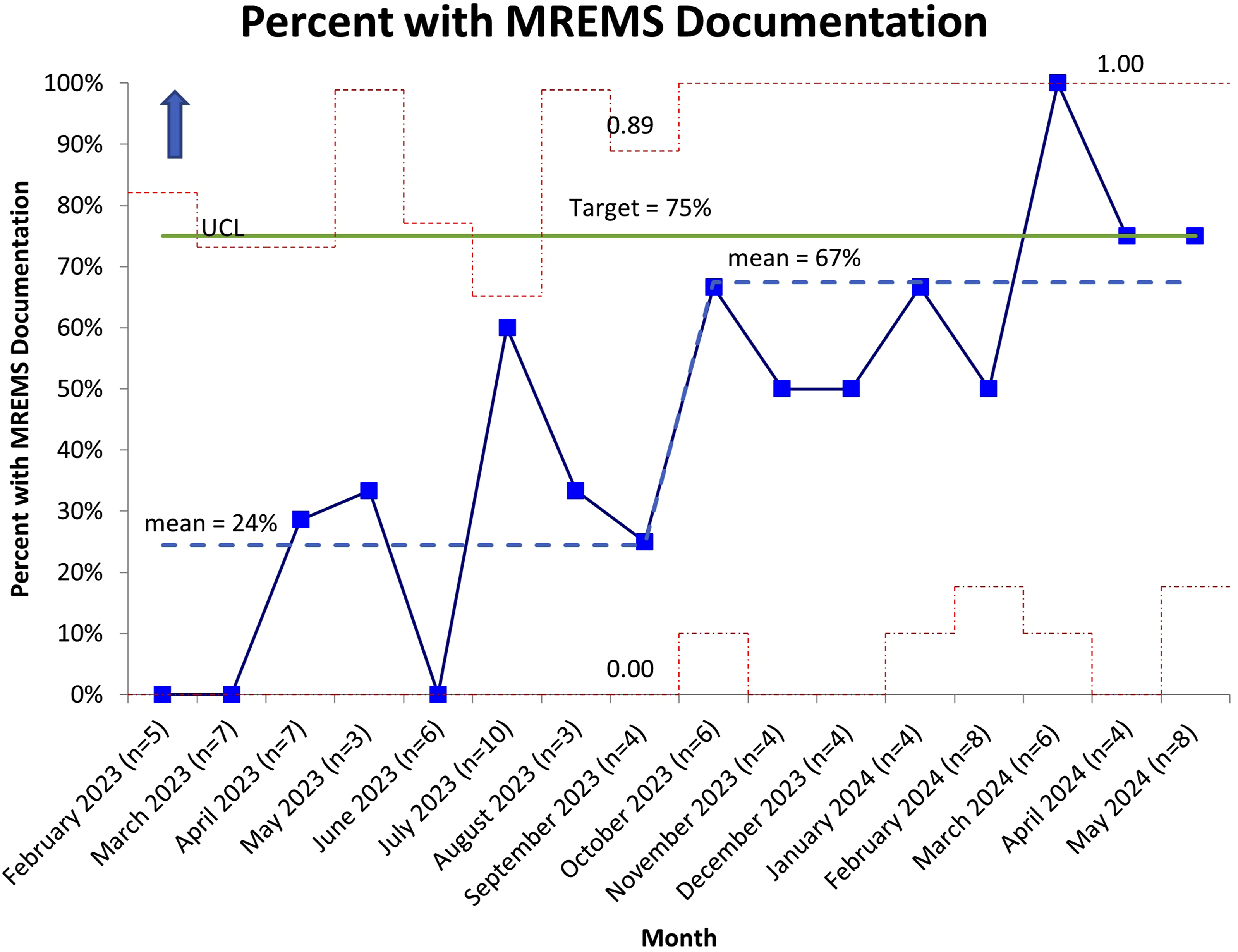
In parallel, pregnancy screening ordered by nursing staff and physicians also increased from 0% to a median of 63% of encounters. (Figure 4) Although we did confirm improvement, this was more erratic over time and did not reach the sustained change in performance metric that we observed with documentation. Over the course of the intervention, we did not have any pregnancies while on MMF. Control Chart of percent of eligible encounters having pregnancy test screening at baseline February 2023 and then throughout intervention from March 2023 to May 2024. Interventions throughout PDSA cycles described per month in text boxes. Target goal of 75% green line. N= number of eligible encounters per month. Upper and lower control limits were defined by ± 3 standard deviations.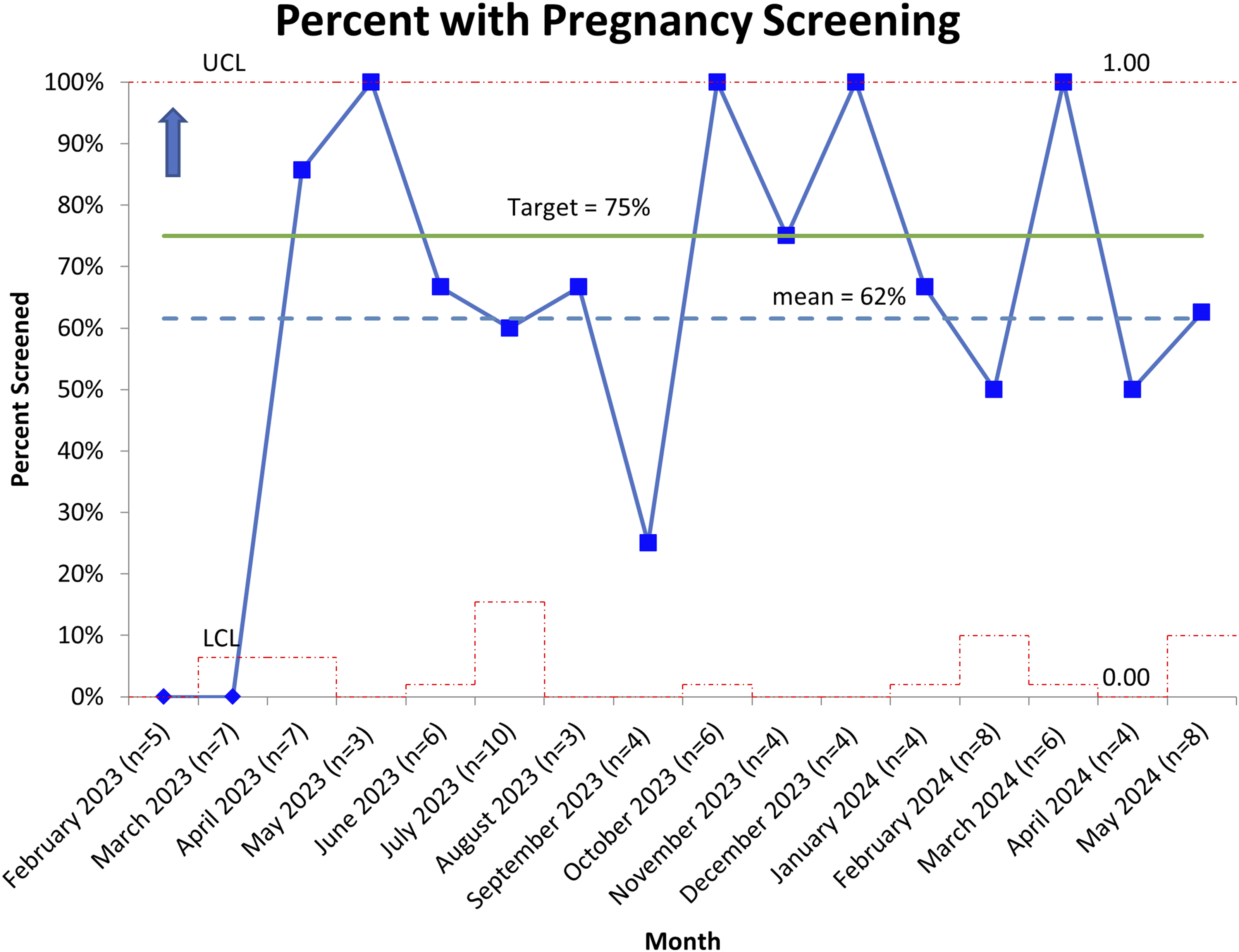
There were no significant differences in disease activity measures between encounters with and without MREMS documentation. Mean clinical SLEDAI scores were 0.7 (2.0) for encounters without MREMS documentation versus 0.5 (1.0) for those with MREMS documentation (p = 0.5). Mean total SLEDAI scores were similarly comparable between groups at 4.5 (4.1) versus 4.2 (3.3), respectively (p = 0.7). The proportion of encounters with active lupus nephritis was also similar, occurring in 17 (37%) encounters without MREMS documentation and 16 (38%) encounters with MREMS documentation.
Demographic characteristics and contraception type of women who had completion of MREMS during encounter in comparison to those who did not over the course of 14 months.
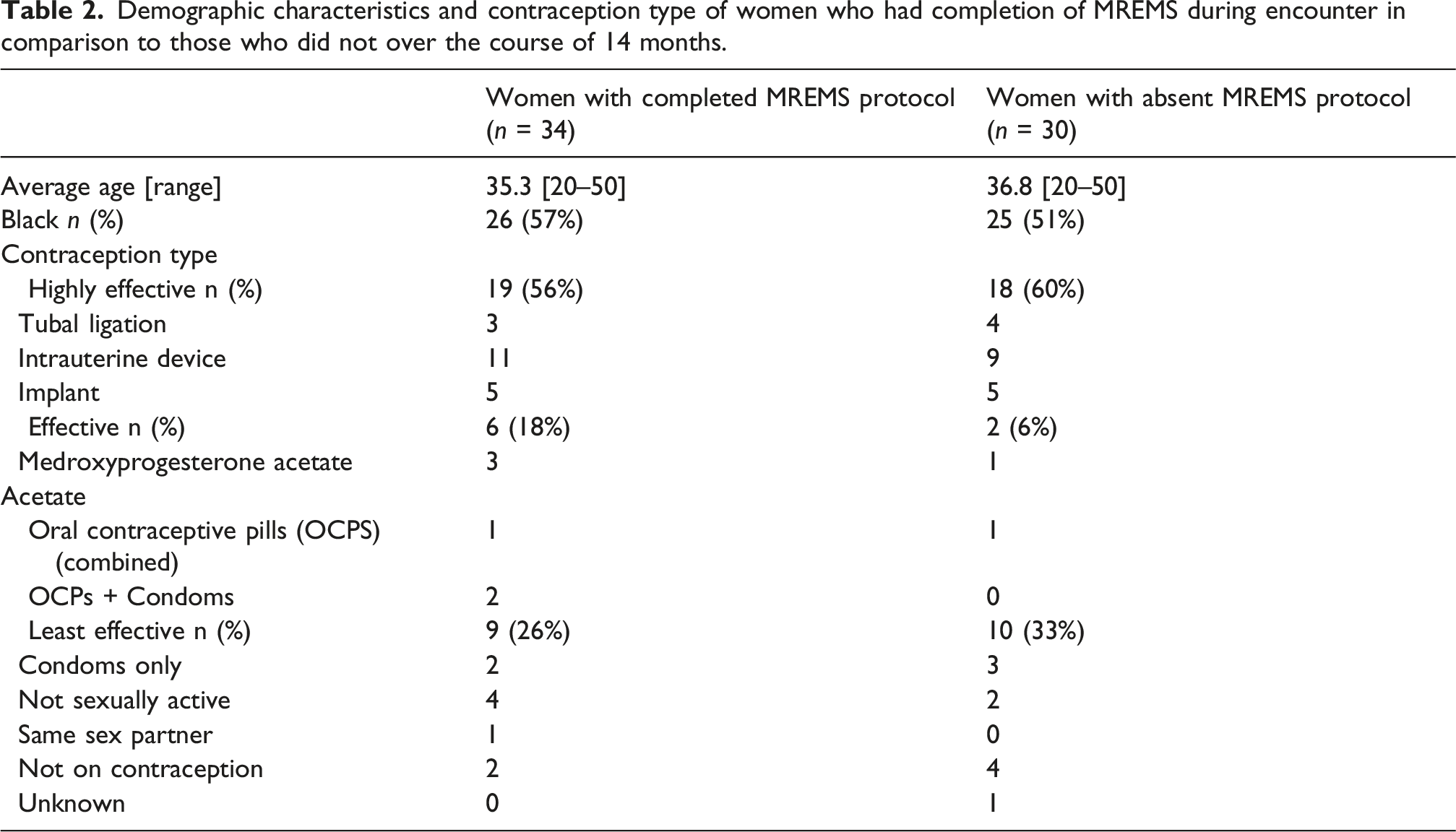
Across the 14 months of the intervention, ten participants had absent MREMS documentation and were not on effective contraception (Table 2). When further characterizing these participants,who could be considered at high risk of pregnancy while on teratogenic medication, we found that half of them did have pregnancy screening completed during the visit. In addition, two of the encounter participants had male partners with vasectomies, while another was not on contraception due to prior side effects. Emergency contraception was only prescribed once.
At one-year follow-up, over 3 months compliance with MREMS documentation was sustained at 80%. In parallel, pregnancy screening also remained sustained with 75% of encounters having urine screening.
Discussion
In this QI project, we developed an intervention that resulted in meaningful improvements in both MREMS counseling documentation and pregnancy screening. These findings align with the emphasis placed by professional societies on the need for structured pregnancy counseling in rheumatology. The ACR, for example, recommends that women receive risk counseling when contemplating pregnancy, maintain disease control for at least 3–6 months prior to conception, and discuss any medication changes in advance with their rheumatologist. 14
Despite clear guidelines, gaps in implementation persist. Although the MREMS program has been associated with fewer pregnancies at the time of treatment initiation, it has not consistently prevented pregnancies occurring during therapy. 9 This gap may reflect ongoing challenges in translating recommendations into routine clinical practice. Recent evaluations of community rheumatology practices suggest that contraception documentation is more common among younger white women, those with more frequent clinic visits, within larger health systems, and those treated by female providers. 15 Our study was limited to a single academic center, but we did not observe differences by age or race. Notably, most providers in our clinic are female, which may have contributed to the success of our intervention. Additionally, contraception documentation rates were already high prior to implementing MREMS.
Unlike our findings, other rheumatology quality-improvement initiatives have reported only modest increases in documented pregnancy screening after intervention. 16 Similar challenges have been observed in pediatric settings caring for adolescents with lupus who are prescribed MMF. 17 Together, these observations highlight the difficulty of sustaining consistent reproductive health practices in busy outpatient environments—particularly among patients with SLE, who often rely on their rheumatologist as their primary source of reproductive health counseling. 18
Disease activity at time of visit was not associated with change in documentation adherence. These findings suggest that gaps in MREMS documentation are not driven by clinical complexity. Providers do not appear to omit documentation during visits with higher disease activity or when clinical management demands are greater. Instead, the lack of association indicates that missed documentation is unlikely to be patient-driven and is more plausibly attributable to workflow- or system-level factors.
Women of reproductive age receiving mycophenolate mofetil (MMF) require careful risk stratification as part of routine clinical care. In our study, nearly 2% of encounters without documented MREMS counseling involved women who were either not using or on low effective contraception. This subgroup represents a particularly high-risk population due to the significant teratogenic potential of MMF. Therefore, ensuring thorough MREMS counseling and documentation is especially critical in these patients, as it supports informed decision-making and helps mitigate the risk of adverse fetal outcomes.
This study highlights various important ethical considerations. Female patients should be clearly informed of the teratogenic risks associated with mycophenolate to ensure that any decision to initiate or continue therapy is fully informed and voluntary. Providers must respect patient autonomy while ensuring that the patient understands the seriousness of potential fetal risks. This requires careful navigation of the ethical balance between protecting maternal health and minimizing fetal harm. Additionally, thorough documentation of counseling regarding teratogenic risks, as well as the patient’s understanding and decisions, is essential, as it provides legal evidence of adherence to FDA recommendations.
Future directions include developing targeted clinical flags to identify women of reproductive age on mycophenolate mofetil (MMF) who are not using contraception, thereby prioritizing this high-risk group for timely counseling and intervention. In addition, conducting qualitative assessments of providers regarding the use of structured discussion guides may help evaluate their effectiveness in facilitating MREMS-related conversations while minimizing additional clinical burden.
Lessons and limitations
A strength is the meaningful and sustained improvement in MREMS counseling documentation and pregnancy screening achieved through a clinic-embedded intervention that aligns with national recommendations. A second strength, was the use of a standardized, non-cloned templated note applied at every encounter and used consistently across providers, which supported reliable and reproducible documentation.
Implementation challenges included justifying pregnancy test costs and lower relevance of MREMS protocol in patients on effective long-term contraception, same sex partners or tubal ligation. The current FDA MREMS recommendations do not go into detail regarding these specific subgroups.
Conclusion
This quality improvement project confirmed that it is feasible to implement MREMS within a busy academic lupus clinic. We were able to increase documentation of MREMS counseling within our notes, as well as implement pregnancy testing during every visit. This remained sustained at 1 year follow up. We used practical interventions in a busy academic clinic, that we believe make this project reproducible in other clinical sites to provide higher quality and safer care to women on MMF.
Supplemental material
Suppplemental Material - A quality improvement project to incorporate the mycophenolate Risk Evaluation and Mitigation Strategies in an academic lupus clinic
Suppplemental Material for A quality improvement project to incorporate the mycophenolate Risk Evaluation and Mitigation Strategies in an academic lupus clinic by Dahima Cintron, Caitlan Pinotti, Jennifer L Rogers, Kai Sun, Rebecca Sadun, Mithu Maheswaranathan, Jayanth Doss, Lisa Criscione-Schreiber, Megan E.B. Clowse in Lupus
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
Clowse: GSK, UCB consultant. Criscione-Schriber: GSK grant. Doss: Aurina share holder. Rogers, Eudy, Clowse: Exagen, Immunovant, DoD grants. Eudyand Sun: NIH NCATS 1KL2TR002554. Rogers: Eli Lilly, Immunovant, Janssen, Aurina consultant.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.