
Abstract
Current B-cell depletion strategies in lupus nephritis (LN) may encounter a mechanistic “glass ceiling.” While rituximab remains an important therapeutic option, its activity can be constrained by CD20 internalization, antigenic modulation, and greater reliance on complement-dependent mechanisms, which may be less efficient in complement-consuming inflammatory states. Type II anti-CD20 antibodies, particularly obinutuzumab, offer a biologically distinct approach by favoring stronger effector-cell recruitment and direct cell-death programs while reducing target internalization. In this perspective, we examine whether these properties may support deeper B-cell depletion in proliferative LN. Drawing conceptually from hematologic oncology, we propose that minimal residual disease (MRD) may serve as a useful analogue for thinking about depletion depth in nephrology; however, MRD-like peripheral depletion should not be interpreted as a validated renal endpoint or as direct proof of intrarenal immune quiescence. High-sensitivity flow cytometry may refine quantification of residual circulating B cells, whereas biomarkers such as uCD163 may provide complementary information on ongoing intrarenal inflammatory activity rather than tissue B-cell depletion per se. At present, surveillance-based retreatment and fixed peripheral thresholds remain investigational. Overall, obinutuzumab expands the mechanistic and clinical horizon of LN therapy, while underscoring the need for studies linking depletion depth, tissue biology, safety, and durability of response.
Introduction
Rituximab has established itself as a cornerstone of B-cell depletion strategies in lupus nephritis (LN), particularly in refractory scenarios.1,2 However, despite its biological rationale, clinical trials reveal a “glass ceiling”. 1 In the pivotal LUNAR trial, rituximab failed to meet the primary endpoint and results from subsequent randomized controlled trials (RCTs) have been inconsistent.1,3 Nevertheless, it remains widely utilized as acknowledged in the most recent EULAR recommendations. 2
Peripheral blood B-cell depletion may not fully capture the fate of tissue-resident or rapidly reconstituting autoreactive populations, but this should be framed as a biologically plausible explanation rather than a proven determinant of clinical non-response in LN. 4 Mechanistically, trogocytosis—namely, Fc receptor–dependent transfer or “shaving” of antibody–antigen complexes and adjacent membrane from the target-cell surface—and FcγRIIB-mediated internalization can reduce surface CD20 density and shorten the exposure window for complement recruitment and other effector mechanisms.5,6 These escape pathways may help explain why type I anti-CD20 strategies can lose efficiency in complement-consuming inflammatory states, although they do not fully account for all rituximab failures in LN.5–7 Thus, the “glass ceiling” is better framed as a limitation of the conventional anti-CD20 depletion axis rather than as proof that tissue persistence is the dominant mechanism in every patient.3,5–7 Experimental data support FcγRIIB-mediated internalization with downstream lysosomal handling of the CD20–antibody complex, but the extent to which this reflects durable antigen loss versus transient surface removal in LN remains incompletely defined, and current evidence does not justify selecting one rituximab schedule over another on this basis alone.3,5
Type II antibodies: Overcoming the mechanistic barrier
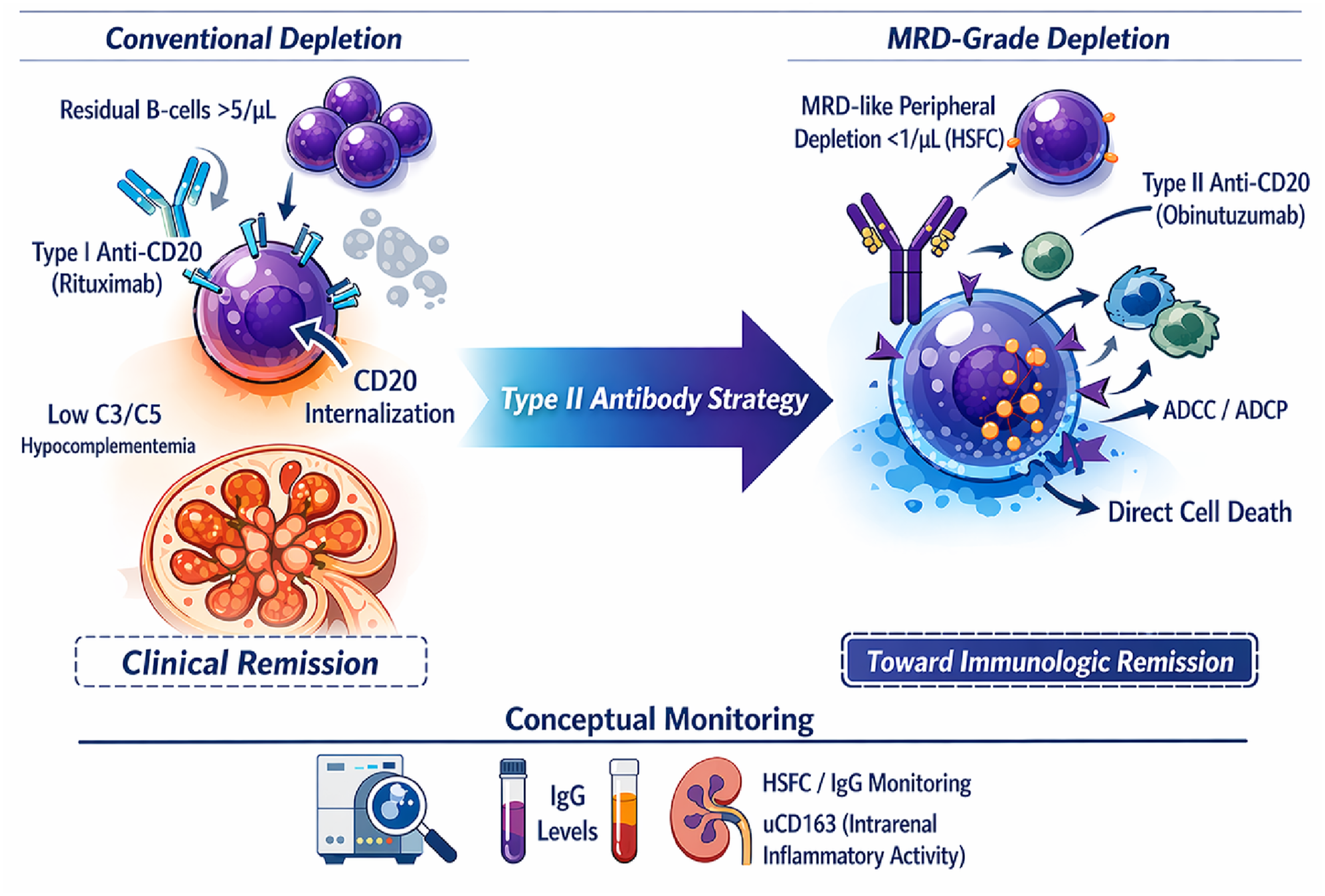
In proliferative LN, the distinction between type I and type II anti-CD20 antibodies may influence depletion depth because anti-CD20 efficacy depends on both intrinsic and extrinsic mechanisms.3,4,7 Rituximab relies more heavily on complement-dependent cytotoxicity (CDC), although antibody-dependent cellular cytotoxicity (ADCC) and antibody-dependent cellular phagocytosis (ADCP) also contribute in vivo.3,7 It is additionally subject to a critical escape axis: type I antibody-induced CD20 clustering favors FcγRIIB-mediated internalization of the complex, removing the target from the cell surface and shortening the window for effector recruitment. 5 In contrast, obinutuzumab (OBI) is a glycoengineered type II antibody designed to enhance FcγRIII engagement, thereby shifting depletion toward stronger ADCC and ADCP while also promoting direct cell death.3,8 Importantly, the effectiveness of any anti-CD20 monoclonal antibody still depends on extrinsic host factors such as complement availability, Fcγ receptor-bearing macrophages and NK cells, and recirculation of opsonized B cells through the reticuloendothelial system.3,4 Intravital imaging suggests that hepatic Kupffer-cell phagocytosis is a major in vivo route for depletion of circulating B cells, which may partly explain why tissue-resident B-cell populations are not necessarily depleted to the same extent as circulating cells. 4 This is also why newer depletion platforms merit attention: whereas monoclonal antibodies remain partly constrained by complement biology and reticuloendothelial trafficking, T-cell engagers and cell-based approaches may circumvent some of these extrinsic barriers by redirecting cytotoxic effector function more directly, although kidney-specific comparative data remain limited. 3
For type I antibodies, FcγRIIB-mediated internalization appears biologically relevant because it can promote loss of surface CD20 and downstream lysosomal handling of the complex, but current evidence does not support choosing one rituximab schedule over another in LN solely on the basis of this mechanism.3,5 By contrast, type II antibodies favor homotypic adhesion, actin remodeling, lysosomal membrane permeabilization, and non-apoptotic direct cell death; however, these mechanistic data arise largely from B-cell malignancy models and should not be over-extrapolated to all autoimmune B-cell subsets or tissue niches.3,8,9
The hypocomplementemia paradox
The Type II advantage becomes even more compelling in the immune ecology of the inflamed kidney, where complement consumption often renders CDC-dependent strategies inefficient.3,7,10 In the OBI trial population, hypocomplementemia was highly prevalent at baseline. 10 In this environment, OBI offers a biologically coherent rationale: reduced target internalization may preserve effector engagement even when the complement pathway is unstable, and type II antibodies can additionally trigger direct lysosomal cell-death programs that are less dependent on classical complement sufficiency.3,5,8 By combining greater effector recruitment with direct cell death, OBI targets deep depletion as a novel therapeutic goal beyond proteinuria (Figure 1).8,10,11
Translating “MRD” to nephrology
We propose translating the hematologic concept of minimal residual disease (MRD) to LN. 12 The persistence of small populations of CD19+ B cells, even after peripheral depletion deemed “adequate” by conventional methods (<5–10 cells/µL), may represent the substrate for early relapse.12,13 Traditional lymphocyte counting underestimates residual B cells, whereas MRD-dedicated platforms can identify levels below 1 cell/µL. 12 Accordingly, HSFC can be viewed as a more granular pharmacodynamic tool for quantifying residual circulating B cells below conventional thresholds. 12 In this Editorial, “MRD” is used as a conceptual analogue rather than as a validated renal endpoint or a proven treatment target in LN.12,14 The current clinical data support the biological relevance of deeper depletion, but they do not yet establish that an MRD-like peripheral threshold is itself sufficient to define remission or superiority over rituximab in routine practice.10–12 Peripheral depletion therefore should be interpreted as a refined systemic readout, not as direct proof of intrarenal immune quiescence.12,15
In LN, HSFC can operationalize “MRD-like” depth by quantifying residual circulating B cells with far greater granularity than conventional flow thresholds. 12 However, paired validation of HSFC-defined peripheral thresholds against repeat renal tissue immunophenotyping remains limited.12,15 Early exploratory repeat-biopsy data from the REGENCY program presented at ACR Convergence 2025 suggest that obinutuzumab can markedly reduce kidney parenchymal B-cell infiltrates, but these findings should not yet be equated with validated “tissue MRD-negativity”. 15 Paired blood–kidney studies should therefore be prioritized to determine whether any peripheral threshold is biologically and clinically informative enough to serve as a robust surrogate.12,15
Clinical evidence and the price of potency
Recent evidence suggests OBI “raises the ceiling” of response.10,11 In the NOBILITY trial, OBI added to standard care increased complete renal response rates at week 52 and maintained separation through week 104, accompanied by improvements in serological measures. 10
The “price” of greater depletion should be stated more precisely.10,11,16 Infusion-related reactions were more frequent with OBI, but severe reactions including clinically significant hypersensitivity appear uncommon in the available trial datasets and were largely concentrated in the early infusions; current reports do not suggest an infusion-related or overall mortality signal exceeding comparator therapy, although available follow-up remains limited for rare but consequential infectious outcomes.10,11,16 Serious infections, cytopenias, and longer-term hypogammaglobulinemia remain the more clinically consequential safety concerns, particularly when deep depletion is repeated on top of background immunosuppression.11,16,17 This creates a real trade-off between efficacy and immunologic fragility, requiring close monitoring during the front-loaded phase and continued vigilance thereafter.11,14,16,17 A further practical niche worth acknowledging is the patient with prior rituximab intolerance, hypersensitivity, or secondary non-response.18,19 In such cases, obinutuzumab may be mechanistically attractive and has emerging supportive experience in SLE/LN, including patients with prior rituximab intolerance, hypersensitivity, or secondary non-response, but the evidence remains limited and should be presented as evolving rather than established.18,19
Pre-infusion IgG levels and lymphocyte subsets may help contextualize safety when further B-cell–depleting therapy is being considered, but current evidence is insufficient to endorse a validated HSFC/IgG-triggered re-dosing algorithm in LN.12,14,17 At present, any surveillance-based retreatment strategy should be framed as a clinically interesting but unproven approach rather than as an evidence-based standard.12,14 Conceptually, an MRD-informed model may be useful as a research framework for time-limited induction followed by careful observation of repopulation kinetics, immunoglobulin recovery, infections, and renal response, rather than as a directive to retreat whenever low-level repopulation is detected.12,13,17 Claims of benefit should therefore remain anchored in randomized trial evidence, while acknowledging that current guideline-based maintenance frameworks still organize therapy over a longer multiyear horizon.10,11,14
Plasma-cell escape and repopulation kinetics
A central limitation remains: anti-CD20 therapies do not eliminate long-lived, CD20-negative plasma cells. 3 The objective is not to “kill plasma cells,” but to cut the supply line: by depleting upstream precursors, OBI reduces the replenishment of pathogenic niches. 3 The pivotal nuance is not merely how low B cells go during induction, but how they reconstitute thereafter.3,13 Durable responders are more often associated with an immature/naïve reconstitution pattern, whereas relapse may be preceded by memory-enriched repopulation. 13 This is one reason deeper depletion may plausibly matter not only for induction of remission but also for the durability of response.3,12,13 Even so, whether obinutuzumab produces a clinically meaningful relapse-prevention advantage over rituximab in LN remains to be proven in prospective studies specifically designed for that question.3,10,11 Because plasmablasts and long-lived plasma cells are CD20-negative, neither type I nor type II anti-CD20 therapy should be expected to deplete these compartments directly to the same extent as mature CD20-positive B cells. 3
Operationalizing immunologic remission
A practical caveat is implementation in low-resource settings.20,21 Type II anti-CD20 antibodies, HSFC platforms, repeat-biopsy programs, and expanded urinary biomarker panels are not uniformly available across LN care pathways, particularly in middle-income countries.20,21 In Brazil, access to innovative lupus therapies has historically been uneven across public and private systems, although obinutuzumab received ANVISA approval in January 2026 for adults with active class III or IV LN, with or without concomitant class V.14,20,21 Even so, regulatory approval does not ensure rapid or equitable access, and formal health-economic analyses specifically addressing HSFC- or obinutuzumab-based monitoring strategies in LN remain scarce.20,21 For such settings, the most transferable message may be strategic rather than technological: deeper biologic monitoring can refine care where available, but high-quality standard therapy, infection prevention, careful renal follow-up, and timely referral remain the foundation while access expands.2,14,20,21 The Brazilian experience also suggests that regulatory approval alone is insufficient: scalable gains are more likely when approval is paired with referral concentration, risk-based prioritization, and stepwise expansion of access to advanced diagnostics and biologics.20,21
Any pragmatic implementation of this framework should couple HSFC-guided monitoring with practical “depth-without-fragility” safeguards—periodic IgG surveillance, vaccination planning, and individualized prophylaxis.2,12,14,17 Clinically, OBI may be particularly attractive for patients with high-risk biology where conventional strategies underperform—e.g., aggressive phenotypes with marked hypocomplementemia, suggesting complement-dependent immune activation as a vulnerability.10,11 Whether monitoring should evolve from fixed-interval dosing to phenotype-informed re-infusion remains uncertain. 14 HSFC-guided retreatment is a reasonable research hypothesis and may inform individualized practice in selected centers, but it is not yet a guideline-endorsed, evidence-based standard in LN.12,14
To translate MRD-like thinking into practice, a composite monitoring strategy is more defensible than reliance on any single marker.12,14,22 HSFC provides a systemic pharmacodynamic readout of circulating B-cell depletion, whereas urinary biomarkers such as uCD163 should be interpreted differently: they reflect ongoing intrarenal inflammatory activity and macrophage activation rather than direct evidence of tissue B-cell depletion or repopulation.12,22 In concept, uCD163 may therefore complement HSFC by flagging discordance between peripheral depletion and persistent renal inflammatory activity, but it should not be used as a stand-alone surrogate for intrarenal B-cell kinetics.12,22 Thus, in concept, uCD163 should be viewed as a parallel marker of residual intrarenal inflammatory activity rather than as a biomarker of tissue B-cell depletion or repopulation per se.12,22 The therapeutic target is better framed as sustained immunologic and renal quieting during the consolidation phase, not as a validated mandate to keep circulating B cells below an MRD-like threshold for a fixed 12–18 months.12,14 Any duration hypothesis should be tested against contemporary guideline-based treatment frameworks rather than treated as established standard of care.2,14 Current ACR and EULAR frameworks position obinutuzumab within longer combination-treatment strategies in responders, rather than as evidence supporting a validated mandate for 12–18 months of MRD-like peripheral suppression alone.2,14
In summary, obinutuzumab strengthens the case for deeper B-cell depletion as a potentially important therapeutic dimension in LN, but the field has not yet established that MRD-like peripheral depletion is itself a validated treatment target or that it should replace guideline-based clinical end points.10–12,14 At present, the most defensible position is that obinutuzumab expands the mechanistic and clinical horizon of LN therapy while motivating prospective studies that link depletion depth, tissue biology, safety, and relapse prevention.10–12,14,15