
Abstract
Objective
Systemic lupus erythematosus (SLE) is a chronic autoimmune disorder associated with considerable morbidity and mortality, particularly due to frequent hospitalisations. This study aimed to describe the causes, clinical course, and outcomes of hospitalisations among patients with SLE in a multinational cohort.
Methods
This retrospective cohort included adults (aged ≥18 years) with SLE hospitalised at Hamad General Hospital, Qatar, between June 2016 and August 2020. Each admission was considered separately. Data included demographics, clinical features, SLE Disease Activity Index (SLEDAI), serological markers, complications, treatments, and prognoses. Predictors of intensive care unit (ICU) admission were evaluated using univariable and multivariable logistic regression.
Results
There were 281 admissions among 153 patients. Most patients (87%) were female, with a median age of 34 years (IQR: 26–44). The principal causes of admission were lupus flares, haematologic (38%), renal (28%), and articular (20%), followed by infection (20%). The median hospital stay was 7 days (IQR: 4–12). Re-admission occurred in 51% of the patients, and 17% of the admissions required ICU care. ICU admission was associated with a longer hospital stay (median 16 vs 6 days, p < 0.001) and higher mortality (11% vs 0%, p < 0.001). Factors predicting ICU admission were a higher SLEDAI score (odds ratio (OR) 1.14, 95% confidence interval (CI)1.07–1.21, p < 0.001), sepsis (OR 4.91, 95% CI 2.02–11.89, p < 0.001), and cardiac involvement (OR 7.57, 95% CI 1.74–32.93, p = 0.007).
Conclusions
In this multinational cohort, SLE flares and infections were the leading causes of hospitalisation. Sepsis, comorbid conditions, and high disease activity are associated with adverse outcomes. Optimising disease control, preventing infection, and managing comorbidities are essential to improve hospitalisation outcomes and reduce mortality.
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disorder with an unpredictable course, multisystem involvement, and a high burden of comorbidities. Despite therapeutic advances, patients frequently develop severe complications necessitating hospitalisation. Hospital admissions contribute considerably to morbidity, healthcare utilisation, and financial burden.1,2
Global studies indicate that patients with SLE are hospitalised at higher rates than the general population, with causes including disease flares, infections, and treatment-related complications.3–6 In-hospital mortality remains a major concern, particularly among patients requiring intensive care unit (ICU) management.7–9 Predictors of poor outcomes include disease activity, multi-organ involvement, infection, and comorbidities such as cardiovascular disease.10–12
Although several large cohort studies from North America, Europe, and Asia have examined these outcomes, data from the Middle East and Gulf region remain scarce.13,14 Given the region’s multiethnic populations, varied healthcare systems, and differences in access to care, local studies are necessary to identify patterns of disease, hospitalisation burden, and outcomes.
Healthcare delivery across the Middle East and Gulf region varies considerably with respect to access to specialist rheumatology and critical care services. In Qatar, healthcare is publicly funded with universal access to tertiary rheumatology and intensive care services through a centralised national healthcare system. This contrasts with other regional settings where access to specialised care may vary according to geographical location or insurance coverage. Studies from Saudi Arabia have reported lupus flares as the predominant cause of hospitalisation, with higher ICU mortality rates compared with Western cohorts, highlighting potential differences in disease severity, access to care, and critical care delivery across the region. 15
This study aimed to address this gap by characterising hospitalisations of patients with SLE at a tertiary centre in Qatar. We assessed the causes of admission, complications, ICU utilisation, mortality, and predictors of poor outcomes in a multinational cohort of adult patients with SLE.
Methods
This retrospective cohort study was conducted at Hamad General Hospital, a tertiary academic referral centre in Doha, Qatar. The study adhered to the Declaration of Helsinki, Good Clinical Practice guidelines, and regulations of the Ministry of Public Health, Qatar. Approval was obtained from the Institutional Review Board of the Medical Research Centre at Hamad General Hospital (Approval No. MRC-01-20-056).
The study population comprised all adult patients (aged ≥18 years) with established SLE, diagnosed according to the 1997 American College of Rheumatology (ACR) classification criteria, who were admitted between June 2016 and August 2020. Patients aged <18 years or with missing hospitalisation data were excluded. Each admission was analysed separately.
Collected data included demographics (age, sex, ethnicity), clinical features (comorbidities, baseline manifestations, medications), and Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) scores for each admission. Serological data were reviewed retrospectively, including antinuclear antibodies (ANA), anti-double-stranded DNA (anti-dsDNA), extractable nuclear antigen (ENA) panel, and antiphospholipid antibodies (aPL). Reasons for hospital admissions were classified into lupus flares and non-flare SLE-related complications. Lupus flares were further categorised by organ system involvement, including haematological, renal, serositis, articular, neuropsychiatric, and mucocutaneous manifestations. Non-flare SLE-related admissions included infections, thromboembolic events, cardiovascular events, adverse drug reactions, pregnancy-related complications, malignancy, and other SLE-associated conditions, in-hospital complications (e.g., renal impairment, sepsis, pulmonary haemorrhage). Sepsis was defined based on clinical diagnosis documented in the medical records by the treating physicians, supported by laboratory and microbiological data where available. Renal impairment was defined as deterioration in renal function during hospitalisation, including acute kidney injury based on changes in serum creatinine and/or reduced estimated glomerular filtration rate (eGFR), as documented in the medical records. Interventions included (pulse corticosteroids, intravenous immunoglobulin [IVIG], plasmapheresis, renal replacement therapy). Outcomes included ICU admission, length of hospital and ICU stay, and in-hospital mortality.
Analyses were performed using Stata version 17.0 (StataCorp LLC, College Station, TX). Continuous variables were tested for normality and reported as medians with interquartile ranges (IQR); categorical variables were expressed as frequencies and percentages. Comparisons between ICU-admitted and non-ICU patients were performed using Wilcoxon rank-sum tests for continuous variables and chi-square tests for categorical variables. Predictors of ICU admission were identified using univariable logistic regression; variables with p < 0.05 were entered into a multivariable logistic regression model. Odds ratios (ORs) with 95% confidence intervals (CI) were adjusted and reported. Statistical significance was defined as p < 0.05 (two-tailed). Missing data were handled using pairwise deletions without imputation. This study followed the STROBE checklist for observational cohort studies to ensure methodological consistency and reproducibility.
Results
Demographics and comorbidities of hospitalised patients with SLE stratified by ICU admission status.
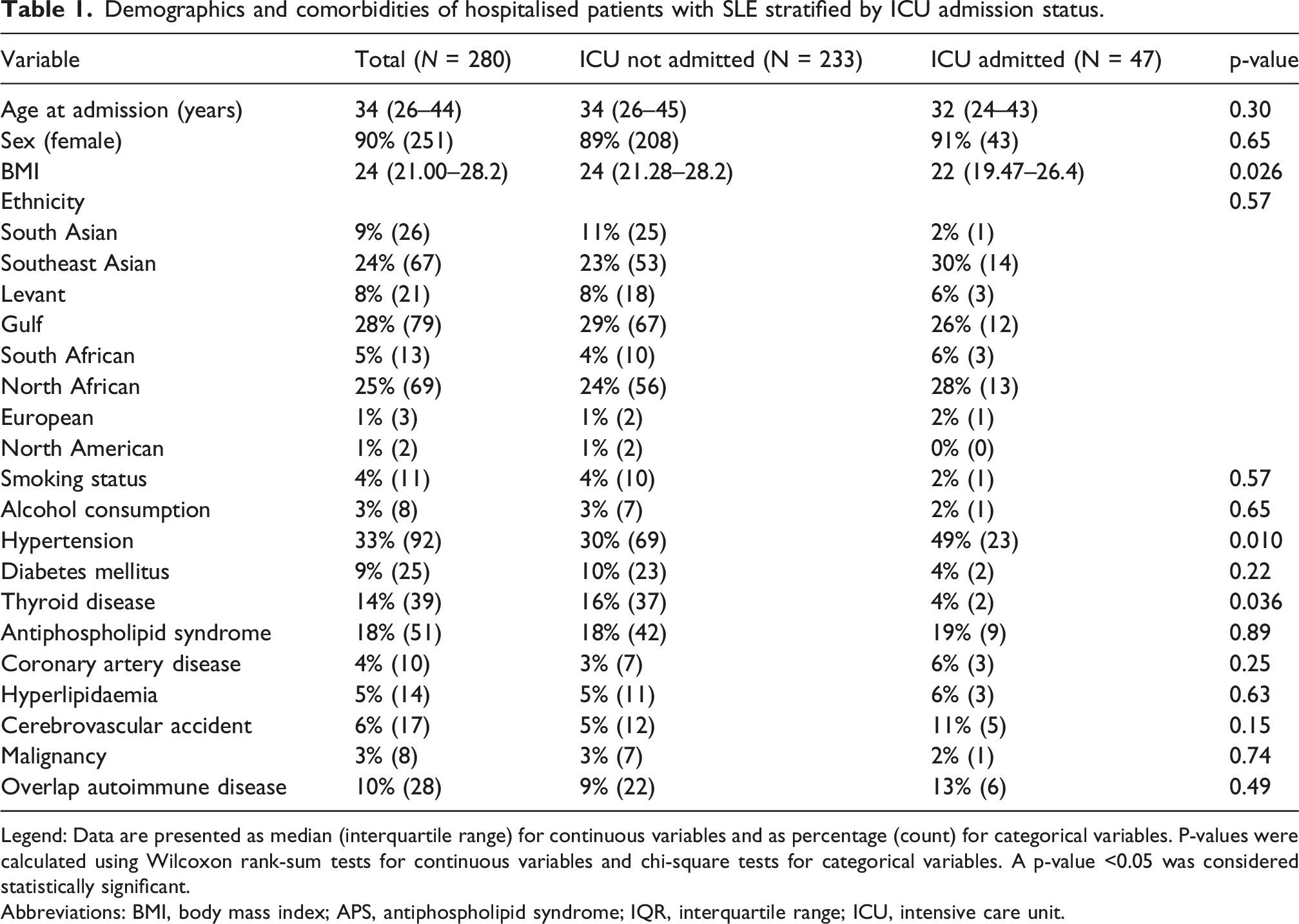
Legend: Data are presented as median (interquartile range) for continuous variables and as percentage (count) for categorical variables. P-values were calculated using Wilcoxon rank-sum tests for continuous variables and chi-square tests for categorical variables. A p-value <0.05 was considered statistically significant.
Abbreviations: BMI, body mass index; APS, antiphospholipid syndrome; IQR, interquartile range; ICU, intensive care unit.
Baseline manifestations, serological markers, disease activity, and medications of patients with SLE by ICU admission status.
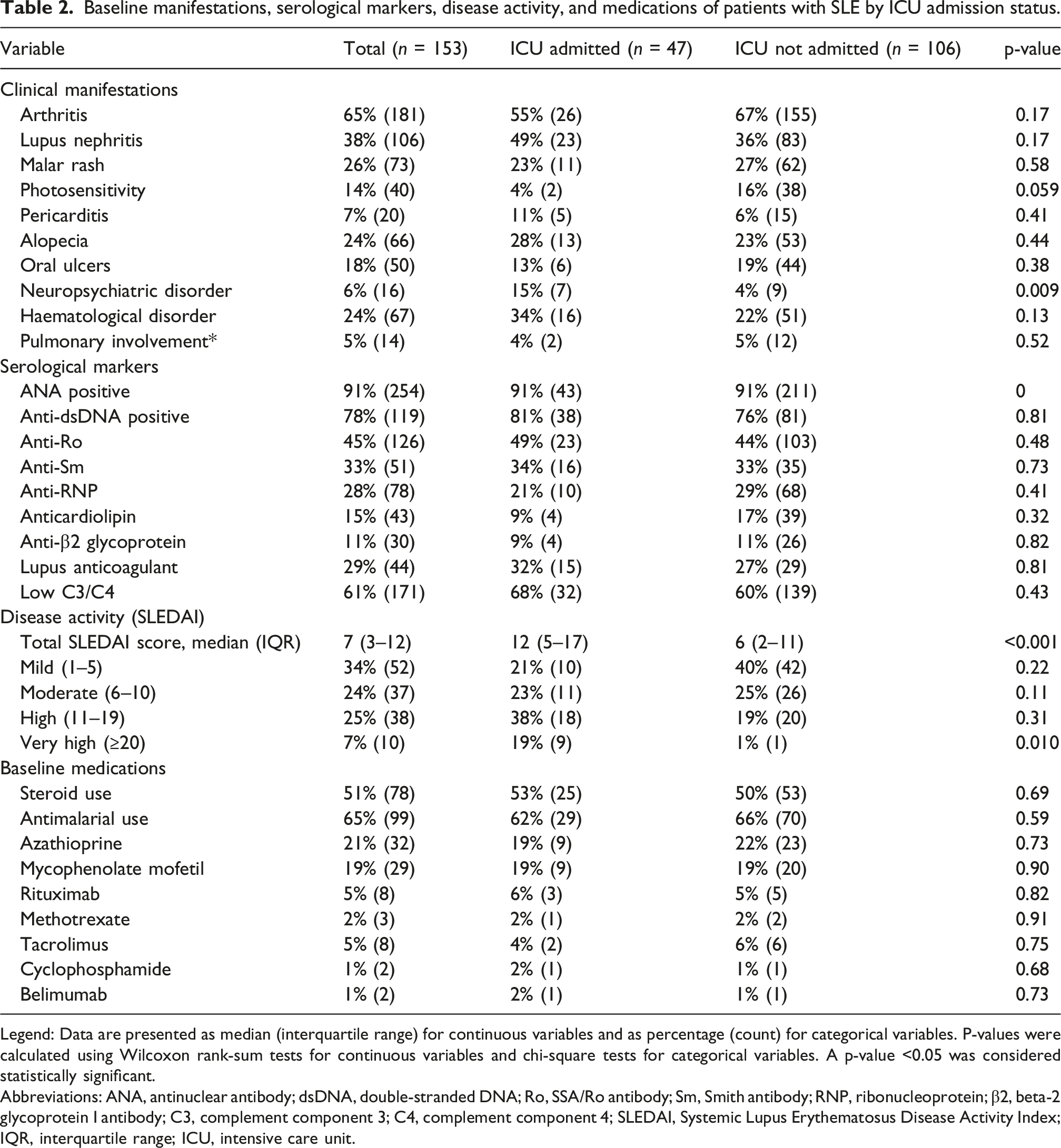
Legend: Data are presented as median (interquartile range) for continuous variables and as percentage (count) for categorical variables. P-values were calculated using Wilcoxon rank-sum tests for continuous variables and chi-square tests for categorical variables. A p-value <0.05 was considered statistically significant.
Abbreviations: ANA, antinuclear antibody; dsDNA, double-stranded DNA; Ro, SSA/Ro antibody; Sm, Smith antibody; RNP, ribonucleoprotein; β2, beta-2 glycoprotein I antibody; C3, complement component 3; C4, complement component 4; SLEDAI, Systemic Lupus Erythematosus Disease Activity Index; IQR, interquartile range; ICU, intensive care unit.
Reasons for hospitalisation
The leading reasons for hospitalisation were lupus flares and infections (Figure 1). Among the flares, haematological manifestations were most common (38%) and primarily included immune thrombocytopenia, autoimmune haemolytic anaemia, pancytopenia, and severe leukopenia, followed by renal (28%) and articular (20%) involvement. Given that all arthritis flares required hospitalisation, they likely represent moderate to severe disease; however, formal severity grading was not available. Infections primarily affecting the respiratory tract (predominantly pneumonia and viral lower respiratory tract infections) and urinary tracts accounted for 20% of the admissions. Additional causes included thromboembolic events (3%), cardiovascular complications (9%), and adverse drug reactions (3%). Reasons for hospitalisation among patients with systemic lupus erythematosus (SLE).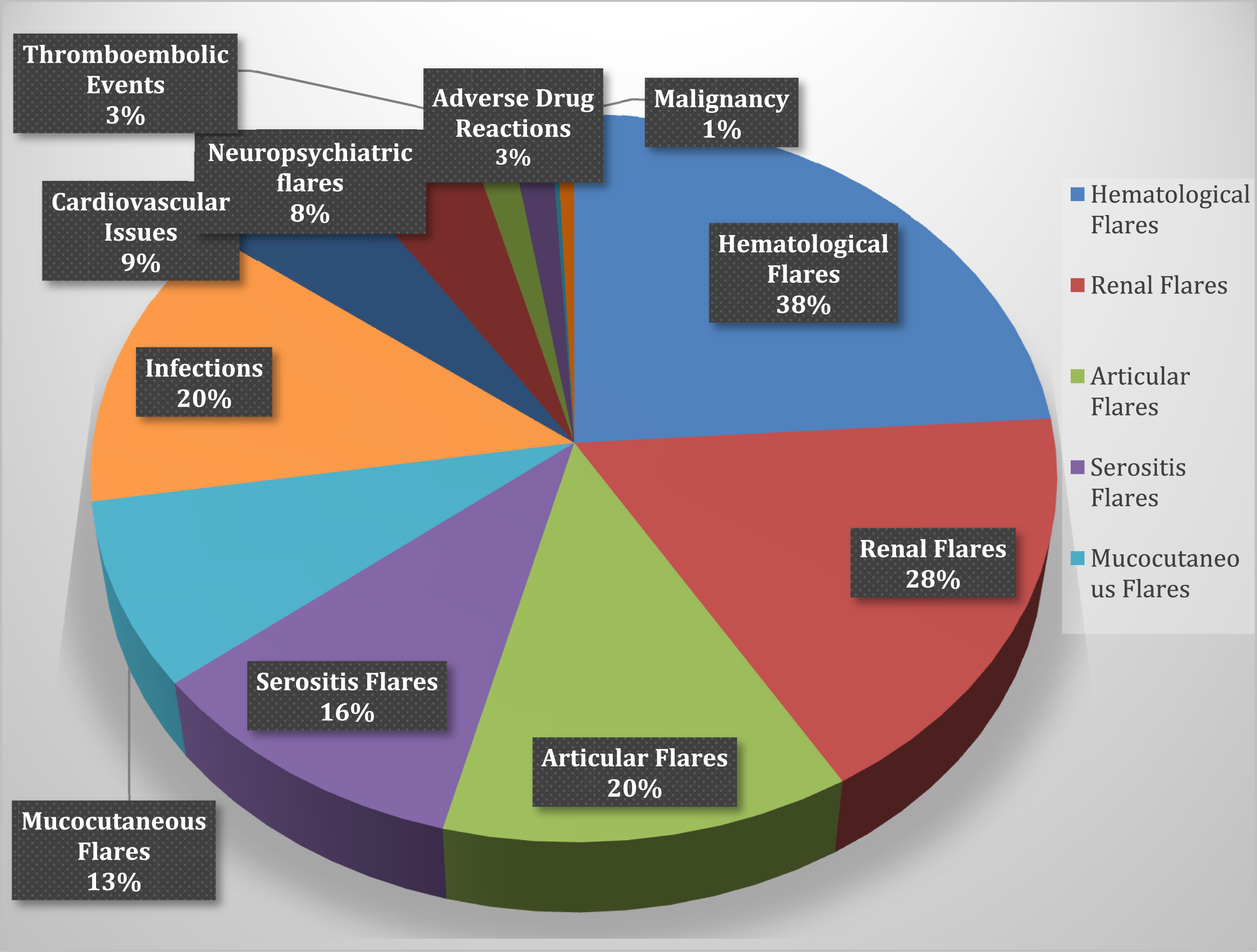
Interpretation of laboratory parameters
Laboratory findings indicated active systemic inflammation at baseline. Median C-reactive protein (CRP) was 24.5 mg/L (IQR 9.0–74.7) and erythrocyte sedimentation rate (ESR) 33 mm/hr (IQR 18–49), consistent with moderate to high inflammatory load. ESR may be elevated in SLE disease activity, whereas elevated CRP levels are more commonly associated with infection rather than lupus flare. The elevation of both markers in our cohort likely reflects a combination of disease activity and concurrent infections, particularly in patients requiring ICU admission. Median ferritin levels were also elevated (561 ng/mL, IQR 179–1,238), likely due to chronic inflammation. Procalcitonin, a more specific marker of bacterial infection, had a median value of 0.4 ng/mL (IQR 0.11–1.22). Elevated levels in several admissions support infection as a common cause of hospitalisation and a major complication, especially among ICU patients.
Medications on admission
At the time of admission, the patients were receiving a range of immunomodulatory therapies (Table 2). Oral corticosteroids were the most common (51%). Use was slightly higher among ICU patients (53%) than among non-ICU patients (50%), although the difference was not significant (p = 0.69). Antimalarial agents, primarily hydroxychloroquine, were prescribed in 65% of the cohort, with similar use in the ICU and non-ICU groups (62% vs 66%, p = 0.59). Other immunosuppressants included azathioprine and mycophenolate mofetil (19–21%), while fewer than 5% received cyclophosphamide, tacrolimus, methotrexate, or belimumab. Rituximab was prescribed in 5% of admissions, with a slightly higher frequency in ICU patients (6% vs 5%, p = 0.82). No statistically significant differences were observed in baseline immunosuppressive regimens between the groups (Table 2). However, ICU patients required a numerically greater frequency of intensive therapies (pulse steroids, IVIG, and plasmapheresis) during hospitalisation (Supplementary Table S1).
Complications and interventions
Among 281 hospitalised encounters of patients with SLE, renal impairment was the most frequent complication, affecting 40% (n = 111) of patients overall. The prevalence of renal impairment was significantly higher among those admitted to the intensive care unit (ICU) compared with non-admitted patients (57% vs 36%; p = 0.023). Sepsis represented another major complication, occurring in 23% (n = 63) of all patients, and was markedly more frequent among admitted patients (43%) than those not admitted (18%; p < 0.001). Heart failure was observed in 7% (n = 20) overall and was also significantly more common in admitted cases (21%) than in non-admitted ones (4%; p < 0.001). Pulmonary haemorrhage was an uncommon but serious event, recorded in 2% (n = 6) of the total cohort; it occurred exclusively among admitted patients (13% vs 0%; p < 0.001). Additional complications, such as pericardial tamponade (1%), interstitial lung disease (1%), haematological malignancies (1%), and ischaemic stroke (3%), were rare and exhibited no statistically significant differences between the admitted and non-admitted groups (p > 0.05 for all). These patients required more aggressive interventions, including pulse steroids (51% vs 30%, p = 0.023), other immunosuppressants (62% vs 40%, p = 0.022), renal replacement therapy (38% vs 8%, p < 0.001), IVIG (19% vs 5%, p = 0.004), plasmapheresis (9% vs 0%, p < 0.001), anticoagulation (23% vs 6%, p = 0.001), and broad-spectrum antibiotics (74% vs 48%, p = 0.004) (see Figure 2 and Supplementary Table S1). Complications during hospitalisation in patients with SLE.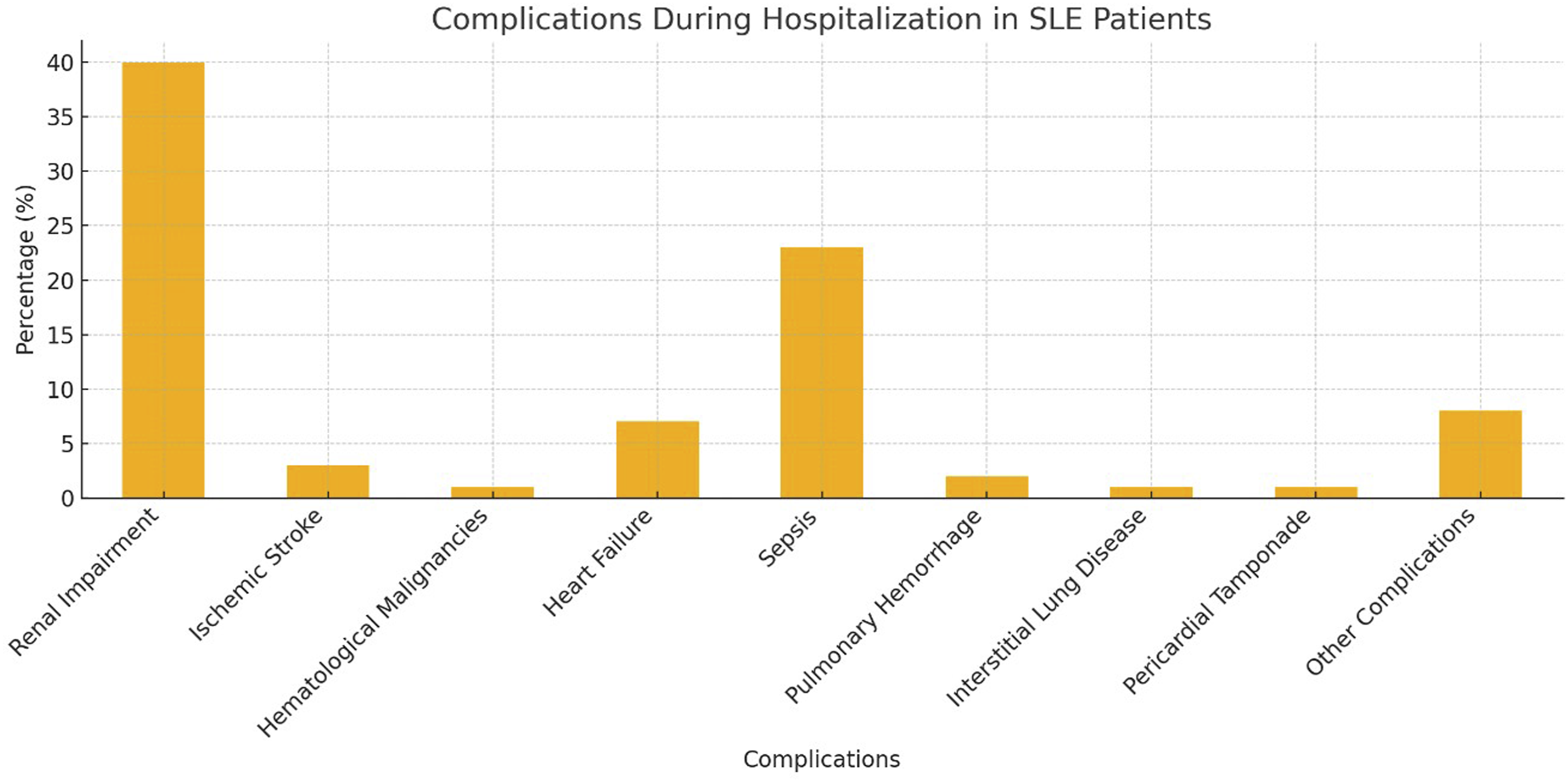
Outcomes of hospitalisations
During the study period, 153 patients with SLE accounted for 281 hospitalisations. Re-admission was frequent, with 51% of patients experiencing ≥2 admissions. The number of admissions ranged from one to nine per patient, with a mean of 1.83 re-admissions. Overall, 47 admissions (17%) required ICU care. The median hospital stay was significantly longer for ICU patients (16 days, IQR 11–40) compared to non-ICU patients (6 days, IQR 4–10; p < 0.001). The median ICU stay was 7 days (IQR 3–15). Among the 47 patients admitted to the ICU, 68% (n = 32) required invasive mechanical ventilation, 4% (n = 2) required non-invasive ventilation (BiPAP), and 28% (n = 13) did not require ventilatory support. The overall in-hospital mortality rate was 1.8% (n = 5), all of which occurred in ICU patients, resulting in an ICU mortality rate of 11%. Causes of death were septic shock (n = 4) and intracerebral haemorrhage (n = 1). ICU patients also had higher rates of re-admission (68% vs 47%, p = 0.02) and were more likely to require intensified immunosuppression. They experienced significantly more complications, including renal failure, sepsis, and pulmonary haemorrhage.
Predictors of ICU admission
Predictors of ICU admissions in hospitalised patients with SLE.
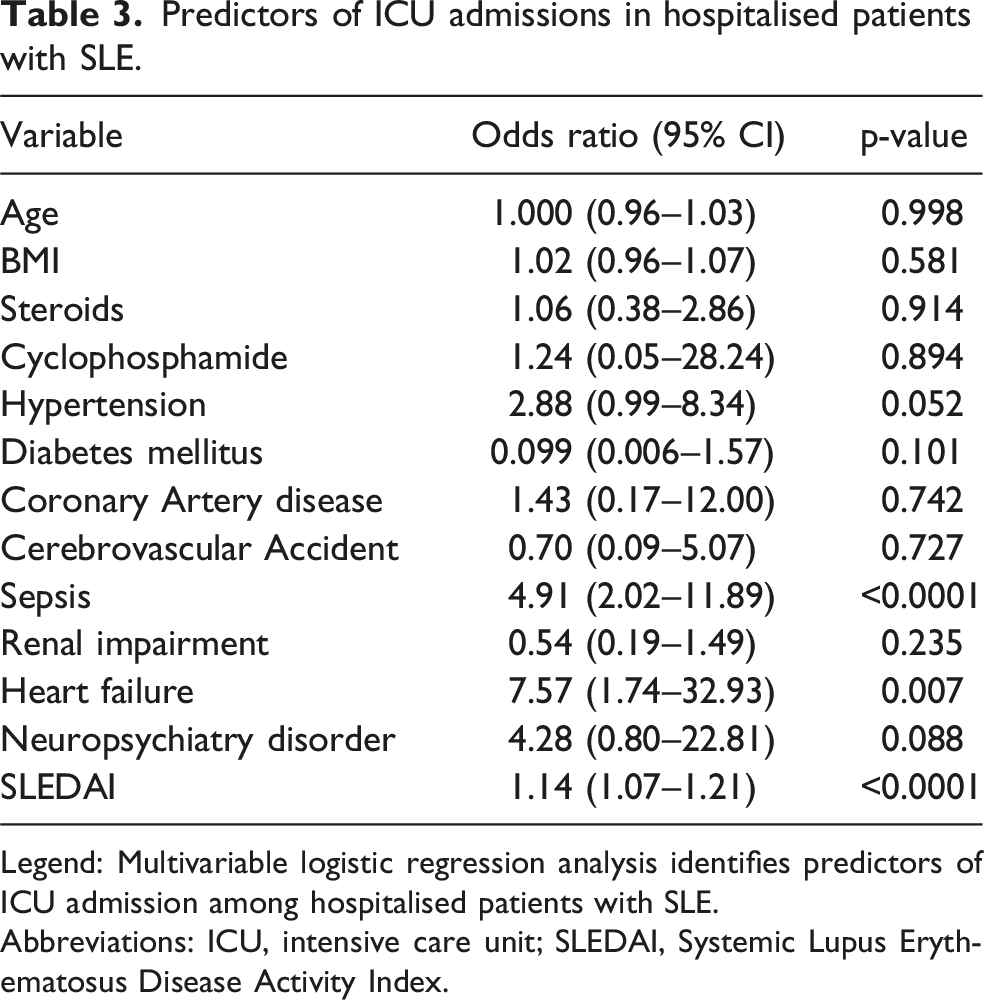
Legend: Multivariable logistic regression analysis identifies predictors of ICU admission among hospitalised patients with SLE.
Abbreviations: ICU, intensive care unit; SLEDAI, Systemic Lupus Erythematosus Disease Activity Index.
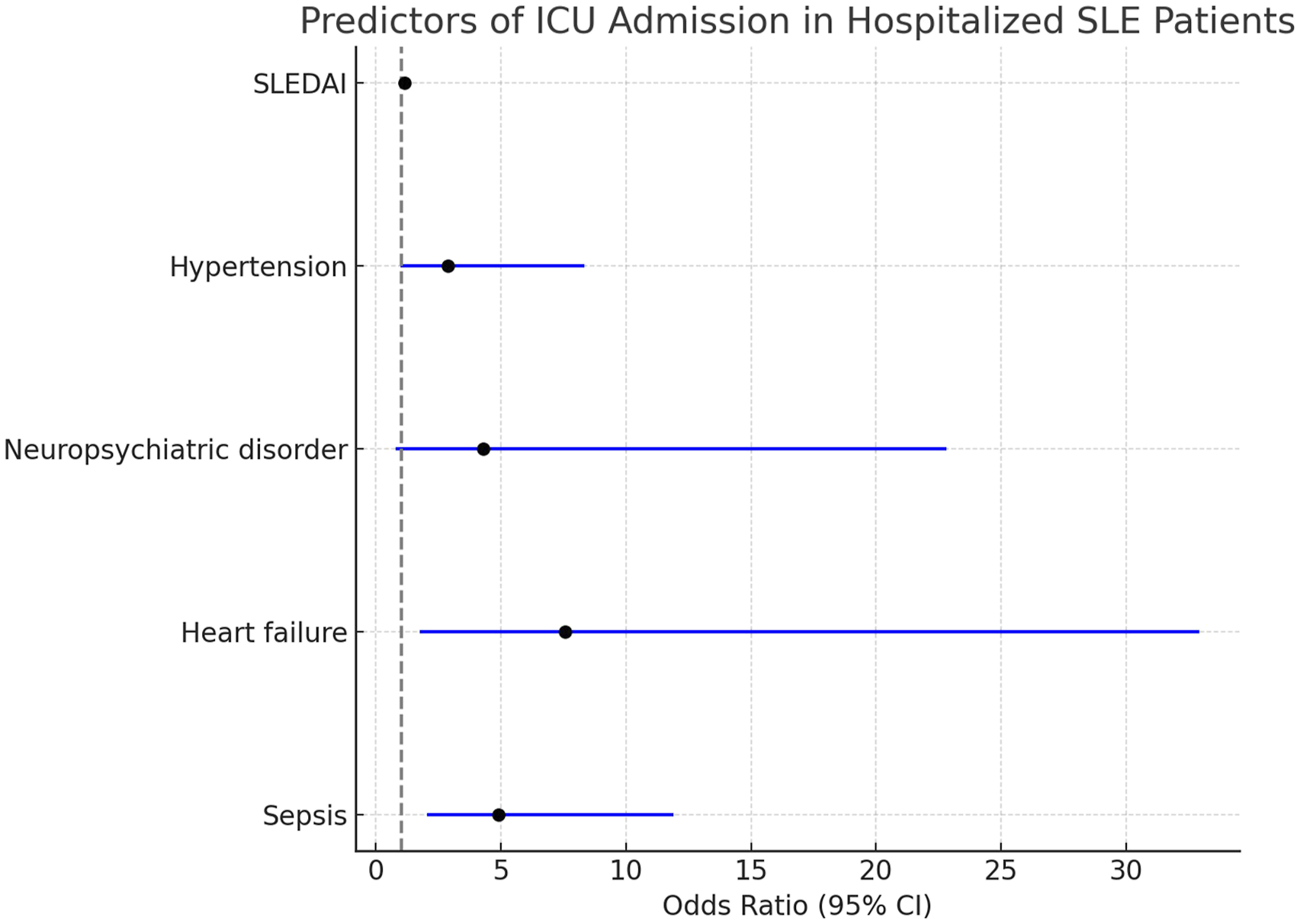
Predictors of ICU admission in patients with SLE.
Discussion
In this retrospective analysis of 281 hospital admissions among 153 patients with SLE, disease flares and infections emerged as the principal causes of hospitalisation. Nearly half of the patients had multiple admissions, and 17% required intensive care. Admission to the ICU was associated with prolonged hospital stay, the need for more intensive treatment, and substantially higher mortality. Elevated disease activity, sepsis, and cardiovascular complications were significant predictors of ICU admission.
Our data highlight the substantial burden of lupus flares, renal (28%), haematological (38%), and articular (20%) manifestations, together with infections (20%) as the predominant triggers for hospitalisation. Although haematological flares were the most common cause of lupus-related hospitalisation, severe leukopenia and other cytopenias in some admissions may have been multifactorial and related not only to lupus activity itself but also to treatment-related immunosuppression. Admissions clearly attributable to medication toxicity were classified separately as adverse drug reactions whenever this could be reliably determined from the medical records. Furthermore, only a minority of haematological flare admissions involved patients receiving intensive immunosuppressive therapies, including rituximab (4.7%) or cyclophosphamide (1.9%), suggesting that treatment-related cytopenia alone is unlikely to account for the predominance of haematological manifestations. Nevertheless, due to the retrospective design, definitive attribution of severe leukopenia to lupus activity versus medication-related marrow suppression was not always possible. These findings are consistent with regional reports from the UAE (24% flares and 20% infections), where pregnancy-related admissions were more frequent (29%) 16 , and from Saudi Arabia (68% flares and 20% infections) 15 . Global data from the US National Inpatient Sample similarly identified infections as the leading cause of SLE-related hospitalisation and in-hospital mortality 17 . In Qatar, patients with SLE are generally managed within a governmental healthcare system with access to national immunisation programs and international rheumatology guidelines, including influenza, pneumococcal, and COVID-19 vaccination, which may influence infection risk. 18 However, vaccination uptake was not assessed in this cohort. The LUMEN cohort further reported infections (24.6%), cardiovascular events (15.2%), and lupus flares (12.2%) as the principal reasons for hospital admission 4.
The median hospital stay in our cohort was 7 days (IQR: 4–12), comparable to reports from the UAE (5.9 days) 16 , Saudi Arabia (6.5 days) 15 , and Canada 9 . The ICU admission rate (17%) exceeded that of the Gulf countries (7%)15,16 and was slightly higher than the 13.8% reported in a Canadian SLE cohort 9 . ICU mortality in our cohort was 11%, which is lower than the rates documented in Saudi Arabia (29.2%) 19 and Iran (50%) 20 , and below the wide range described in a recent systematic review (20–80%) 21 . This comparatively low mortality rate, despite a higher admission rate, likely reflects advances in critical care and multidisciplinary management in Qatar.
Multivariate analysis identified sepsis, heart failure, and elevated SLEDAI scores as independent predictors of ICU admission. These results align with those of international reports. An Egyptian prospective cohort study demonstrated that high disease activity (SLEDAI), infection, and organ damage were significant predictors of ICU admission. 14 A 2025 systematic review further noted that infections, cardiovascular complications, and renal failure are the most common reasons for ICU admission across diverse populations with SLE 22 . Studies from Tunisia 23 , Korea 24 , and Catalonia 25 have also consistently reported these risk factors, underscoring the need for early recognition and intensive management in high-risk individuals. Unlike previous cohorts8,26,27, age and male sex were not predictors of poor outcomes in our study, likely reflecting the younger, predominantly female, composition of our population.
Antimalarial therapy was common in our cohort (65%), although its use was slightly lower in ICU patients. Although we did not assess antimalarial efficacy longitudinally, substantial evidence supports hydroxychloroquine’s protective role in preventing flares and reducing hospitalisations.28,29
More than half of the patients had two or more hospitalisations, consistent with findings from the Hopkins Lupus Cohort 7 , the Korean Lupus Network registry 24 , and Catalonian population-based data 25 . These recurrent admissions reflect the relapsing–remitting course of SLE. A US healthcare utilisation study similarly demonstrated frequent re-admissions, with annual hospital costs ranging from $21,000 to $53,000 per patient, depending on disease severity 30 . Our findings emphasise that SLE imposes a considerable burden on healthcare systems, particularly among patients with high disease activity and complications.
Strengths and limitations
This study is among the few comprehensive evaluations of hospitalisation due to lupus in the Gulf region, incorporating a heterogeneous, multinational cohort of patients and detailed hospital course data. Its relevance is strengthened by the use of validated disease activity indices (SLEDAI) and the availability of complete serological and therapeutic information. Nonetheless, several limitations of this study must be acknowledged. This was a single-centre retrospective study, which may limit the generalisability of the findings to other healthcare settings. Due to the retrospective design, the ability to establish causal attribution for certain reasons for admission, particularly cardiovascular and thrombotic events, was limited, and these may reflect both lupus-related and non–lupus-related processes. Additionally, several covariates, including vaccination status, long-term follow-up and post-discharge outcomes were not consistently available, limiting assessment of their impact on outcomes. Histopathological data, including lupus nephritis class, and detailed classification of renal impairment (e.g., CKD staging) were not consistently available, restricting further characterisation of renal involvement. Similarly, severity grading of arthritis flares (e.g., mild, moderate, or severe) and detailed information on steroid duration and cumulative dose prior to admission was not consistently documented limiting more comprehensive assessment of disease activity and treatment exposure. Microbiological data, including blood culture results and identification of causative organisms, were also incomplete, limiting further characterisation of sepsis. Missing data from some admissions may also have reduced the statistical power of the subgroup comparisons.
Implications and future directions
Our findings emphasise the importance of early flare control, infection prevention, and risk stratification in identifying patients at high risk of ICU admission and poor outcomes. Future studies should include long-term follow-up after discharge and evaluate targeted interventions aimed at reducing re-admissions and ICU utilisation.
Conclusion
Lupus flares and infections remain the predominant causes of hospitalisation in SLE. Sepsis, high disease activity, and cardiac involvement are principal predictors of poor outcomes. These results indicate that optimal disease control, infection prevention, and careful management of comorbidities are essential for improving hospitalisation outcomes and reducing morbidity and mortality.
Supplemental material
Supplemental material - Outcomes of systemic lupus erythematosus hospitalisations in Qatar: Insights from a multinational tertiary centre experience
Supplemental material for Outcomes of systemic lupus erythematosus hospitalisations in Qatar: Insights from a multinational tertiary centre experience by Miral H. Gharib, Karima Becetti, Hana J. Abukhadijah, Fiaz Alam, Aishwariya Padmakumari, Mohamed AL-Kahlout and Rawan Saleh in Lupus
Footnotes
Acknowledgment
Acknowledgments Medical Research Centre at Hamad Medical Corporation.as requested by our Medical research center for publications.
Ethical considerations
The study approval was obtained from the Institutional Review Board of the Medical Research Centre at Hamad General Hospital (Approval No. MRC-01-20-056). It adhered to the Declaration of Helsinki, Good Clinical Practice guidelines, and the regulations of the Ministry of Public Health, Qatar. Due to the retrospective nature of this study, which utilized only de-identified existing data, the requirement for informed consent was waived by the Institutional Review Board.
Author contributions
MHG, kB, and SAE contributed to the conception and design of the work and to the interpretation of data. AP, MAK, RS, and BJ contributed to the acquisition of clinical data. HJA performed the statistical analysis. MHG drafted the manuscript. SAE provided supervision, and SAE, KB, and FA provided critical revision of the manuscript for important intellectual content. All authors approved the final version for publication. MHG is the guarantor and takes overall responsibility for the content of the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a fund from the Medical Research Centre at Hamad Medical Corporation (MRC-01-20-056).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Patient and public involvement
Patients and the public were not involved in the design, conduct, reporting, or dissemination of this research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.