
Abstract
Background
Shrinking lung syndrome (SLS) is a rare manifestation of systemic lupus erythematosus (SLE) lacking standardized management. This systematic review summarizes the current evidence on therapeutic interventions and clinical outcomes.
Methods
Following PRISMA guidelines, we searched six databases (e.g., PubMed, Scopus, and Web of Science) for studies on adult SLS patients published up to January 2026. Methodological quality was assessed using JBI tools.
Results
Forty studies (111 patients) were included (30 case reports and 10 case series); 87.5% presented a low risk of bias. There was a marked female predominance (91%), with a mean age of 33.5 ± 9.8 years. All patients showed a restrictive pattern (forced vital capacity: 47–52%). Glucocorticoids were the mainstay of therapy (95–96%). Rituximab emerged as an effective primary biologic for refractory cases. Non-pharmacological interventions, such as inspiratory muscle training and non-invasive ventilation, improved diaphragmatic strength. Although symptomatic resolution occurred in 75–95% of patients, complete functional recovery (normalization of pulmonary function tests) was achieved in only 20–23% of patients. Mortality directly attributed to SLS was low (2–5.5%).
Conclusions
Early glucocorticoid therapy remains essential, but complete functional recovery is rare, with 80% of patients maintaining chronic restriction. For refractory cases, multidisciplinary care integrating rituximab and respiratory rehabilitation should be considered to optimize functional outcomes.
Keywords
Introduction
Shrinking lung syndrome (SLS) is a rare but debilitating pleuropulmonary manifestation of systemic lupus erythematosus (SLE).1–3 SLS is characterized by progressive exertional dyspnea, pleuritic chest pain, and a restrictive ventilatory pattern associated with diaphragmatic elevation, in the absence of parenchymal or vascular disease.4–6 Since its initial description in 1965, 7 the pathophysiology of SLS has been the subject of academic debate. Proposed hypotheses range from diaphragmatic myopathy and phrenic neuropathy to reflex inhibition of deep inspiration triggered by pleural inflammation.8–10
Despite its impact on patients’ quality of life, therapeutic management is hindered by the lack of an established gold standard. 11 While glucocorticoids are traditionally employed as first-line therapy, evidence for managing refractory cases remains purely empirical and lacks standardized protocols.5,12–14 Furthermore, complete functional recovery is achieved in only approximately 20% of patients,8,10,15,16 suggesting a significant gap in current long-term management strategies. As more than half of the available literature on SLS has emerged in the last decade,4,12,17–19 an updated, rigorous synthesis is required. The aim of this systematic review was to synthesize current evidence on pharmacological and non-pharmacological treatment modalities for SLS, aiming to provide a clearer clinical framework in the absence of formal guidelines.
Methods
Study design and research question
This systematic review was conducted in accordance with the PRISMA 2020 20 guidelines. The research question was anchored in the PICO framework 21 : (P) adults with SLE and SLS; (I) pharmacological and non-pharmacological interventions; (C) not applicable; and (O) clinical and pulmonary functional responses.
Search strategy
A systematic search was performed in PubMed, Lilacs, Scopus, Web of Science, PEDro, and SciELO for records published up to January 2026. The search string “shrinking lung*” AND “lupus” was used. Additionally, the reference lists of the included studies were manually screened to identify further relevant records.
Eligibility criteria
Inclusion criteria comprised clinical trials, observational studies, case series, and case reports describing therapeutic interventions and outcomes in adult patients. We excluded pediatric cases, SLS associated with other connective tissue diseases, purely diagnostic studies, narrative reviews, conference abstracts, and studies without full-text access.
Study Selection and data extraction
Two independent reviewers screened the titles and abstracts, followed by full-text assessment. Any disagreements were solved by consensus. Extracted data included demographics, treatment protocols and respiratory functional response.
Quality assessment
Methodological quality was assessed by two independent reviewers using JBI Critical Appraisal Tools for Case Reports and Case Series. 22 The risk of bias was categorized by the percentage of “yes” responses as follows: low (≥70%), moderate (50–69%), or high (<50%).
Data synthesis
Due to clinical rarity and methodological heterogeneity, a meta-analysis was not performed. Instead, a qualitative narrative synthesis was conducted to summarize the evidence.
Results
Study Selection and quality assessment
The initial search yielded 114 records. After screening, 40 studies involving 111 patients were included: 30 were case reports, and 10 were case series (Figure 1). Although two studies were prospective and interventional, they were classified as prospective non-randomized interventional studies due to the lack of randomization and control groups. The overall methodological quality was high. According to JBI criteria, 35 studies (87.5%) presented a low risk of bias (≥70%) and five (12.5%) a moderate risk (50–69%). No studies were excluded due to a high risk of bias. Detailed quality scores are provided in Supplemental Tables S2 and S3. Flowchart illustrating the details of the search strategy, screening of potentially qualifying reports (n), selection of the included articles, and reasons for study exclusion.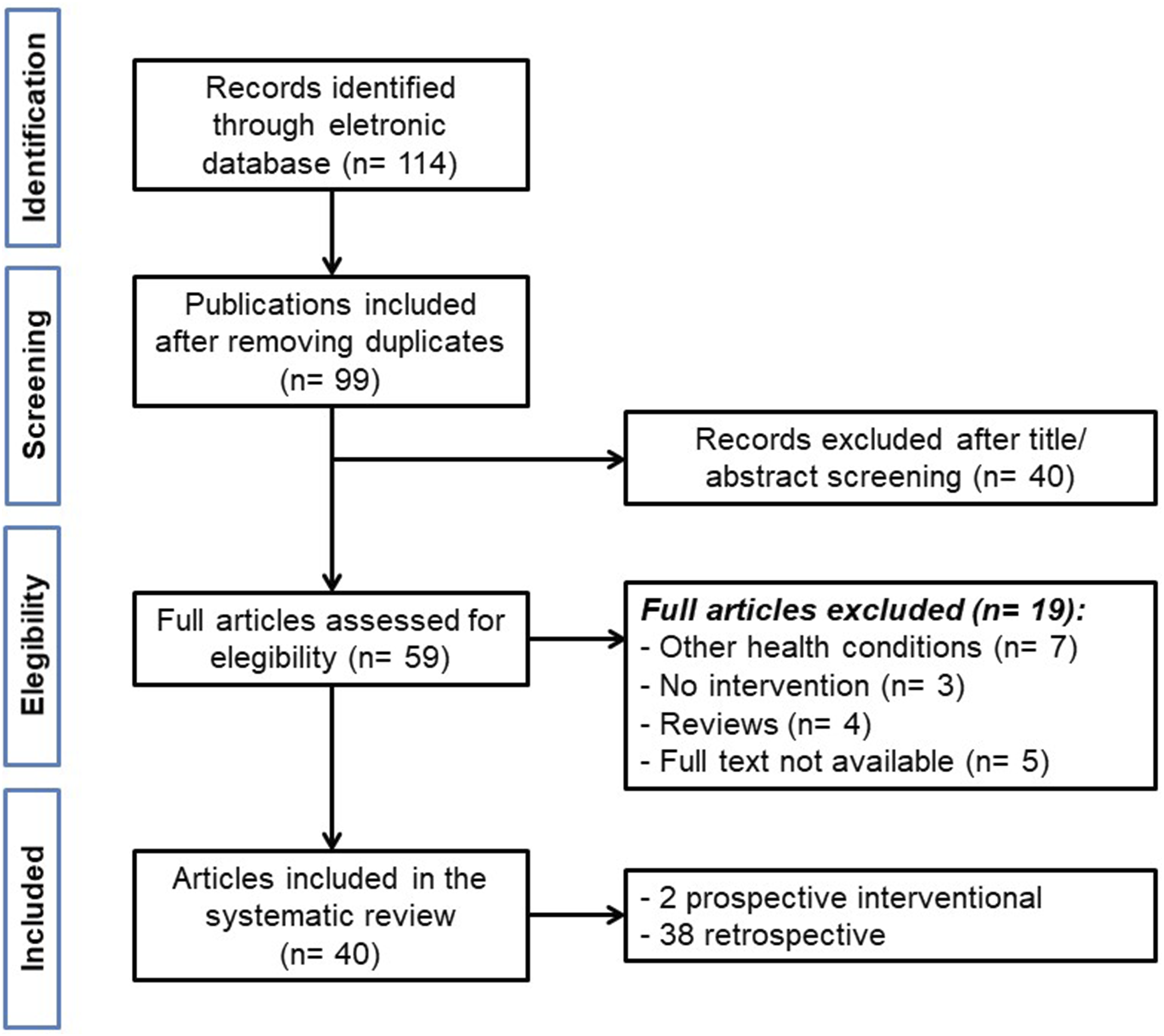
Patient characteristics
Demographic and epidemiological profile of patients with Shrinking Lung Syndrome in the included studies (N = 40).
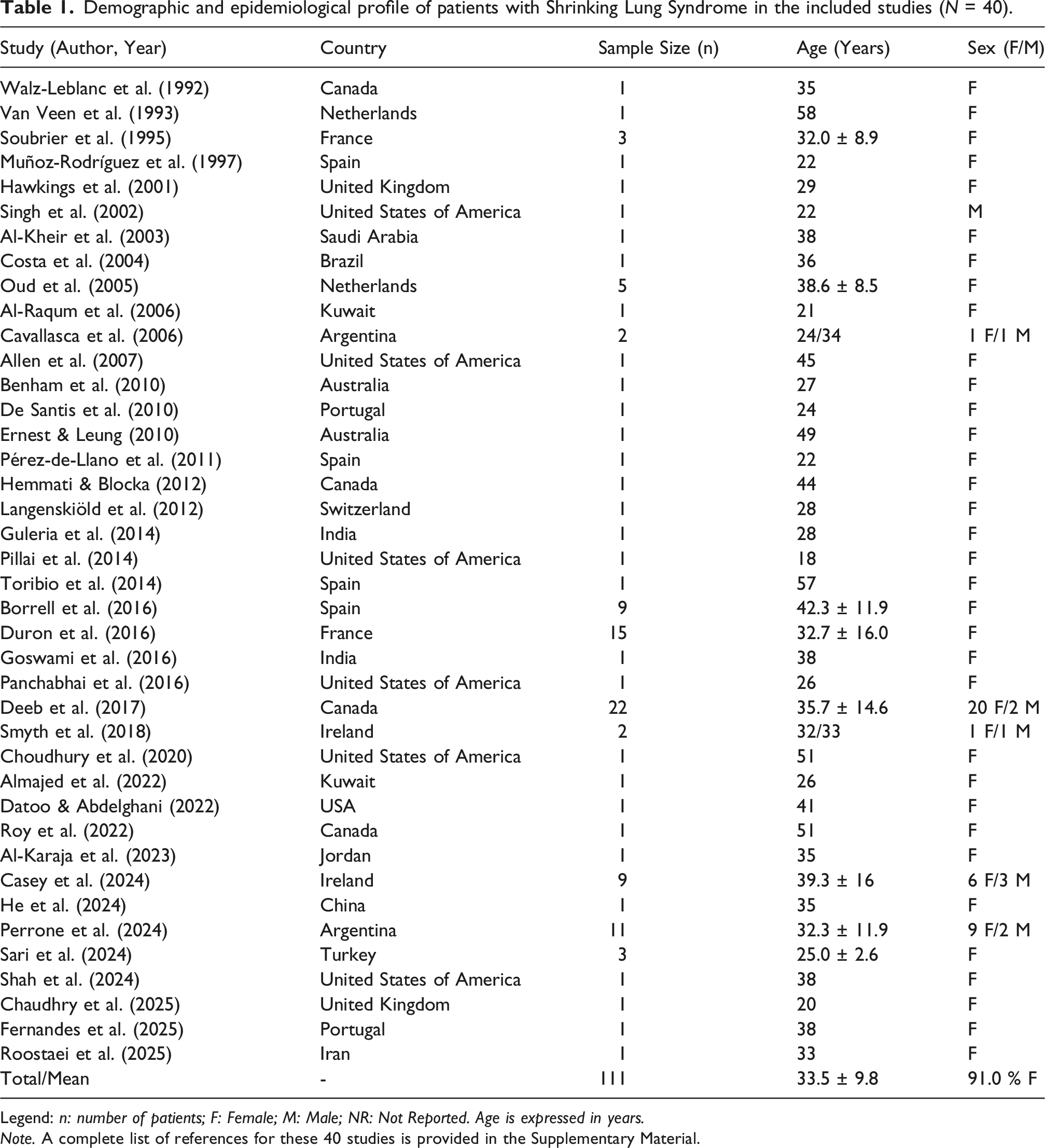
Legend: n: number of patients; F: Female; M: Male; NR: Not Reported. Age is expressed in years.
Note. A complete list of references for these 40 studies is provided in the Supplementary Material.
Clinical and diagnostic findings
Exertional dyspnea was nearly universal (95.5–100%), often accompanied by pleuritic chest pain (74–93%). Pulmonary function tests (PFT) revealed a restrictive pattern in 100% of patients (mean forced vital capacity [FVC]: 47–52%; mean total lung capacity: 54–60%). Diffusing capacity for carbon monoxide (DLCO) was reduced (48–49%) and diaphragmatic elevation was radiologically present in 60–96% of cases.
Therapeutic strategies and outcomes
Overview of treatment regimens and functional responses in representative studies.
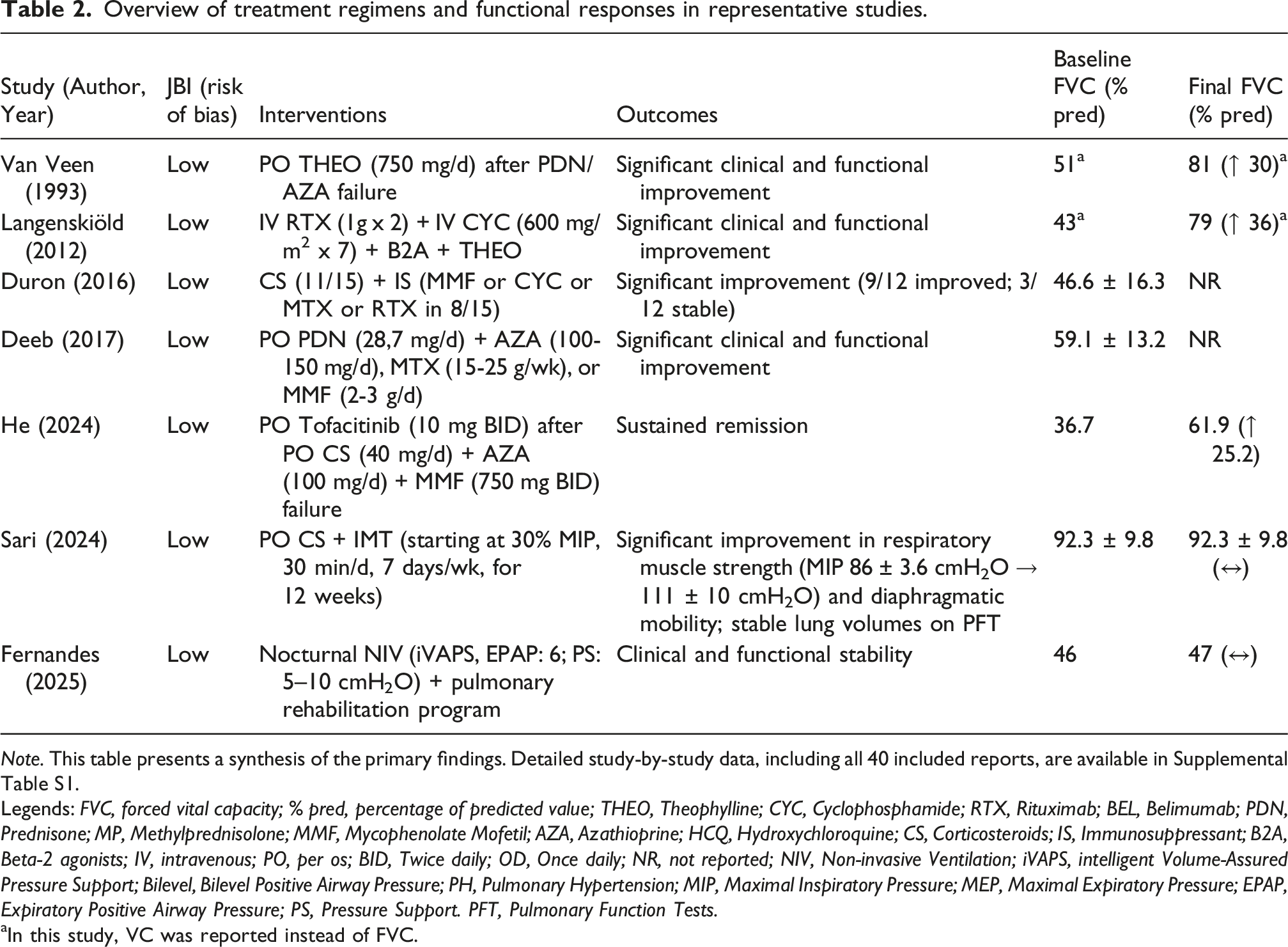
Note. This table presents a synthesis of the primary findings. Detailed study-by-study data, including all 40 included reports, are available in Supplemental Table S1.
Legends: FVC, forced vital capacity; % pred, percentage of predicted value; THEO, Theophylline; CYC, Cyclophosphamide; RTX, Rituximab; BEL, Belimumab; PDN, Prednisone; MP, Methylprednisolone; MMF, Mycophenolate Mofetil; AZA, Azathioprine; HCQ, Hydroxychloroquine; CS, Corticosteroids; IS, Immunosuppressant; B2A, Beta-2 agonists; IV, intravenous; PO, per os; BID, Twice daily; OD, Once daily; NR, not reported; NIV, Non-invasive Ventilation; iVAPS, intelligent Volume-Assured Pressure Support; Bilevel, Bilevel Positive Airway Pressure; PH, Pulmonary Hypertension; MIP, Maximal Inspiratory Pressure; MEP, Maximal Expiratory Pressure; EPAP, Expiratory Positive Airway Pressure; PS, Pressure Support. PFT, Pulmonary Function Tests.
aIn this study, VC was reported instead of FVC.
Regarding outcomes, clinical improvement, defined as resolution of dyspnea and pain, was achieved in 75–95% of patients. However, complete functional recovery, defined as normalization of PFT was rare, occurring in only 20–23% of the cohort. To facilitate a standardized comparison of therapeutic responses, the variation in FVC was consolidated in Table 2 and Supplemental Table S1. This approach was chosen to mitigate discrepancies in reporting styles and to provide a clearer overview of individual lung volume recovery across the included cohort.
Mortality directly attributed to SLS was low (2–5.5%). Notably, intravenous RXT consistently induced remission in cases failing conventional therapy, while inotropic agents (theophylline/beta-agonists) were effective when diaphragmatic weakness was the primary driver.
Discussion
This systematic review provides an updated, comprehensive analysis of SLS management, incorporating 111 patients. Notably, 51.3% of our sample (57 out of 111 patients) was reported within the last decade, reflecting modern clinical practices that were not captured in previous non-systematic reviews. Despite its rarity—with an estimated prevalence between 0.5% and 1.53%—SLS remains a critical manifestation of SLE that significantly impairs quality of life.
Demographics and pathophysiology
Our findings confirm a striking female predominance (91%), primarily affecting women of reproductive age (mean age 33.5 ± 9.8 years). Although SLS is traditionally associated with long-standing SLE, our analysis highlights that it can present as the initial manifestation in approximately 9–10% of cases. Understanding of its pathogenesis has evolved from simple surfactant deficiency theories to a complex multifactorial model involving diaphragmatic myopathy, phrenic neuropathy, and reflex inhibition of deep inspiration triggered by pleural inflammation. The universal restrictive pattern observed in PFT, coupled with significant reductions in Maximal Inspiratory Pressure (MIP) and Maximal Expiratory Pressure (MEP; 80–89% of cases), reinforces the hypothesis that respiratory muscle weakness is the primary functional driver of the syndrome.
Diagnostic and therapeutic challenges
Diagnosis remains a process of exclusion, in which high-resolution computed tomography is essential for ruling out interstitial lung disease or pulmonary vascular involvement. While glucocorticoids remain the first-line therapy (95–96%), our review underscores the emergence of biologic therapies and non-pharmacological interventions. RXT has shown promise in refractory cases, consistently inducing functional recovery where conventional immunosuppressants have failed.9,15,23–25 Our analysis shows that RTX was effective both when used as a targeted rescue therapy for SLS and when administered for concomitant systemic flares, such as lupus nephritis. This superior response may be attributed to its ability to deplete B-cells involved in the underlying autoimmune-mediated diaphragmatic or neural inflammation, which often proves resistant to broad-spectrum agents. However, it is important to note that although symptomatic relief is often observed within the first two months, functional stabilization of PFT typically requires a longer period, often between 6 and 12 months. Furthermore, given the high rates of clinical improvement reported (75–95%), there is a strong likelihood of publication bias, whereby successful outcomes are overrepresented in the literature compared to therapeutic failures. This bias may potentially overstate the real-world efficacy of both glucocorticoids and RXT in this population.
While RXT presents the most robust body of evidence regarding clinical and functional success in refractory SLS, the role of alternative biological agents remains poorly defined.1,11,12 Belimumab, a B-lymphocyte stimulator inhibitor, has demonstrated clinical benefit in isolated case reports, yet its efficacy lacks validation in broader cohorts.1,12,18 Conversely, TNF-alpha inhibitors, such as infliximab, have been associated with unsatisfactory outcomes or even paradoxical respiratory deterioration.1,9,10 This disparity underscores that B-cell depletion therapy may target a more fundamental axis of the autoimmune-mediated diaphragmatic or neural inflammation, which is characteristic of SLS. Other pathways appear to be less reliable in reversing established restrictive patterns.
A significant finding of this review is the role of respiratory rehabilitation. Interventions such as IMT and NIV have demonstrated efficacy in improving muscle strength and quality of life. Studies by Sari et al. (2024) 17 and Fernandes et al. (2025), 26 although not classified as formal randomized trials, provide evidence that structured rehabilitation should be an integral part of multidisciplinary care.
Physiologically, IMT exerts benefits by applying a controlled resistive load to the diaphragm and accessory respiratory muscles. This triggers hypertrophy and enhances the recruitment of type I and type II muscle fibers.17,27 This targeted conditioning is particularly relevant in SLS, where diaphragmatic thinning and reflex inhibition lead to chronic disuse and reduced thoracic compliance. Furthermore, by improving MIP, structured rehabilitation helps overcome the mechanical disadvantage imposed by the elevated diaphragm, potentially reducing the neural drive for dyspnea and improving the ventilatory threshold during physical activity.17,27 These findings pave the way for larger clinical trials focusing on non-pharmacological interventions, which offer a favorable safety profile and cost-effectiveness, representing a viable adjunct to intensive immunosuppression.
Comparison with previous literature
A landmark review by Duron et al. (2016) 9 compiled 155 cases; however, it was primarily a literature review accompanying a case series and lacked a formal systematic methodology. Our study fills this gap by employing PRISMA guidelines and standardized JBI critical appraisal. Furthermore, our data suggest that, although symptomatic improvement is achieved in up to 95% of patients, complete functional recovery (PFT normalization) is rare (20–23%). This discrepancy suggests that long-standing SLS may lead to permanent diaphragmatic fibrosis or parenchymal reorganization. Thus, early intervention is crucial to prevent irreversible damage.
Limitations
This review has limitations inherent to the rarity of SLS, as evidence remains restricted to observational data with no randomized controlled trials identified. Reliance on case reports and small case series carries a risk of publication bias. Significant heterogeneity in reporting PFT and diaphragmatic mobility, along with inconsistent follow-up periods, precluded a meta-analysis and limits the assessment of long-term sustainability. Despite these constraints, this study provides a rigorous synthesis of a large, modern SLS cohort that followed strict methodological guidelines.
Conclusions
SLS is a complex manifestation of SLE with a multifaceted pathophysiology involving diaphragmatic dysfunction and pleural inflammation. Early diagnosis and the prompt initiation of moderate-to-high dose glucocorticoids therapy appear essential for symptom control. RXT and non-pharmacological strategies, such as NIV, IMT, and respiratory rehabilitation, emerge as promising adjuvant therapies for refractory cases. Although clinical resolution of dyspnea and pain is common, complete functional recovery is rare, with approximately 80% of patients maintaining a chronic restrictive defect. This persistent volume restriction necessitates long-term functional monitoring. Standardizing therapeutic protocols through prospective multicenter studies is essential to optimize outcomes and ensure that respiratory muscle rehabilitation is integrated early into the multidisciplinary care of SLE patients.
Supplemental material
Supplemental material - Treatment strategies and clinical outcomes in shrinking lung syndrome in systemic lupus erythematosus: An updated systematic review
Supplemental material for Treatment strategies and clinical outcomes in shrinking lung syndrome in systemic lupus erythematosus: An updated systematic review by Júlia Ribeiro Lemos, Agnaldo José Lopes and Patrícia dos Santos Vigário in Lupus.
Footnotes
Acknowledgements
The authors would like to sincerely thank Míriam Raquel Meira Mainenti and Leonardo Ribeiro Marques for their valuable contributions and support throughout the development of this study. This study was supported in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. The authors also acknowledge the financial support provided by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and the Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.