
Abstract
Objectives
Our aim was to evaluate clinical and renal histopathological variables associated with the diagnosis of Systemic Lupus Erythematosus (SLE) in a South American cohort with Full-House (FH) glomerulonephritis (GN) in order to distinguish it from other causes of FHGN.
Methods
Observational retrospective study. Kidney biopsies performed in our hospital between 2000 and 2019 were reviewed, identifying those with a FH pattern. Clinical, analytical, and histopathological data were collected. Patients were classified as SLE with Lupus - FHGN (if they met ACR 1997 and/or SLICC 2012 and/or ACR-EULAR 2019 SLE criteria) and as non-Lupus FH GN (idiopathic or secondary). Descriptive statistics, univariate and multivariate logistic regression analysis were performed to identify factors associated with Lupus- FHGN, and Kaplan-Meier survival curves were used to compare renal survival between both groups.
Results
181 patients with FHGN were included, 124 women (68.5%), with a mean age of 41.1 years (SD 16.0) and a median post-biopsy follow-up time of 2.9 years (IQR 0.4-6.8 years). 116 patients (64.1%) met SLE criteria (103 with extrarenal manifestations and 13 with renal-limited lupus), 52 patients presented identifiable secondary causes of FHGN and 13 remained idiopathic FHGN. Renal biopsies in Lupus - FHGN presented more frequently 3 or 4 crosses of IgG, C3 and C1q deposits (p < 0.001) and had less moderate/severe involvement of the tubulointerstitial compartment (p < 0.001), when compared with non-Lupus FHGN. In the multivariate analysis, the factors that remained associated with Lupus - FHGN were: female sex, younger age, positive ANA, anti-DNA, and 3 or 4 crosses of C1q deposits. Lupus - FHGN showed a protective effect for the development of End-Stage Renal Disease (ESRD) in the univariate analysis (HR 0.34, 95% CI 0.13-0.89) but this association was not significant in the multivariate analysis.
Conclusions
In this South American cohort, 35.9% of FHGN were not associated with SLE diagnosis. Female sex, younger age, positive ANA or anti-DNA antibodies and marked C1q deposits at renal biopsy were associated with SLE diagnosis.
Keywords
Introduction
Systemic lupus erythematosus (SLE) is a multiorgan autoimmune disease with various manifestations that are subject to relapse and remission. The incidence is estimated between 1.0 and 10.0/100,000 person-years, and a prevalence between 20 and 70/100,000. In Buenos Aires, Argentina, our estimated incidence and prevalence of lupus was 6.3/100 000 person-years and 58.6/100,000 people, respectively.1,2
Lupus nephritis (LN) is one of the most common manifestations of lupus, occurring in around 50% of patients at some point during the disease, being an important cause of morbidity and mortality. Lupus nephritis shows a heterogeneous course, ranging from mild forms to progression to ESRD in approximately 10% of patients. 3
Renal biopsy plays an essential role in the diagnosis of LN. Histologic findings provide the basis for treatment recommendations. Glomerular involvement is the most frequent finding in renal biopsies, but any renal structure could be affected in LN.
Most patients with LN have immune complex-mediated glomerular disease and immunoglobulin and/or complement deposits can be seen at the mesangial, subendothelial, and subepithelial levels. These deposits can be observed by immunofluorescence light microscopy or by electron micrography. A common finding in lupus renal biopsies is full-house glomerulonephritis (FHGN), defined as a positive simultaneous immunofluorescence staining for IgA, IgG, IgM, C3, and C1q, observed in various regions of the glomeruli.4–6
There are other diseases that can present with FHGN: membranous nephropathy, IgA nephropathy, infection-related glomerulonephritis, ANCA vasculitis, etc. In some cases, no associated diagnosis is made, being classified as idiopathic FHGN. 6
In clinical practice, a renal biopsy result with a full-house pattern suggests the diagnosis of SLE. We hypothesized that clinical and histopathological variables could distinguish lupus-associated FHGN from other etiologies and that lupus FHGN would show different renal outcomes.
Methods
Patients
Design: Observational, retrospective study performed at the Hospital Italiano de Buenos Aires, Argentina.
All patients, older than 18 years, with a FHGN pattern in a renal biopsy performed in our hospital between 2000 and 2019 were included. FHGN was defined as concurrent positive staining (≥1+) for IgA, IgG, IgM, C3, and C1q by immunofluorescence. Each patient was followed until the end of the study (December 31, 2019), lost to follow-up or death.
Variables
Demographic and clinical data were obtained from electronic medical records. Renal biopsies were initially reported by pathologists and subsequently reviewed jointly by rheumatologists and nephrologists involved in this study and histological data registered:
including light microscopy findings and immunofluorescence staining [location, number of glomeruli with IgA, IgG, IgM, C1q and C3 deposits and intensity of the deposits (number of crossings)]; Lupus Nephritis histological class according to the International Society of Nephrology (ISN)/Renal Pathology Society (RPS) for those patients with a diagnosis of Lupus.
Antinuclear antibodies (ANA) and anti-double-stranded DNA (anti-dsDNA) antibodies were determined using standard assays that were routinely used at our institution during the study period. ANA was tested using indirect immunofluorescence (IIF) with HEp-2 cells. Anti-dsDNA was tested using IIF on Crithidia luciliae substrate. Although laboratory methodologies evolved over time, internal quality control and standardized diagnostic thresholds were maintained.
End-Stage Renal Disease (ESRD
Patients were followed from biopsy until ESRD, death, loss to follow-up, or December 31, 2019.
Patients were classified as SLE if met the criteria for SLE at any point during follow-up according to the ACR 1997 8 and/or SLICC 2012 9 and/or EULAR-ACR 2019 10 criteria.
After carefully reviewing all clinical, laboratory, and biopsy data, FHGN patients were classified into 2 groups: I. II.
For each patient, the FHGN classification was reviewed at the time of renal biopsy and at the end of follow-up to see if they could be reclassified based on new data developed during follow-up.
Statistical analysis
Descriptive and analytical statistics were performed. Continuous variables were expressed as means and standard deviations (SDs) for normally distributed data or as medians and Interquartile Ranges (IQR) for non-normally distributed data.
Normality of distributions was assessed using visual inspection and standard normality tests. Comparisons between two groups (lupus-associated vs non-lupus full-house glomerulonephritis) were performed using the student’s t test or the Mann–Whitney U test, as appropriate. Categorical variables were compared using the chi-square (χ2) test for independence. When the assumptions for the chi-square test were not met—specifically, when the expected cell counts were <5 in more than 20% of the cells or when any expected count was <1comparisons were performed using Fisher’s exact test instead. This approach ensured valid inference for analyses involving small cell sizes or sparse contingency tables.
Univariate and multivariate logistic regression analyses were performed to identify factors associated with the diagnosis of SLE and renal survival curves comparing between patients with and without SLE. The dependent variable in the logistic regression model was the diagnosis of SLE-associated FHGN (yes/no). Independent variables considered included demographic variables (age, sex), serological markers (ANA, anti-dsDNA), complement levels, and histopathological features (immunofluorescence intensity and tubulointerstitial damage). Variables with p < 0.10 in univariate analysis were entered into the multivariate model, limiting the number of predictors to avoid overfitting. Multicollinearity among independent variables, particularly ANA and anti-dsDNA, was assessed using the Variance Inflation Factor (VIF), with a VIF <5 considered acceptable.
Renal survival was analyzed using Kaplan–Meier curves, with time zero defined as the date of renal biopsy. Patients were censored at the time of death, loss to follow-up, or end of the study period (December 31, 2019). Renal survival was estimated using the Kaplan–Meier method and compared between groups using the log-rank test. Additionally, sensitivity analyses for renal survival were conducted at pre-specified time points (1, 5, and 10 years) using the log-rank test to evaluate model stability over time. Data were analyzed with the STATA v.12 program (Stata Corp, 4905 Lakeway Drive, College Station, Texas 77845 USA).
Statement of ethics and consent
The study was conducted according to the principles of the Declaration of Helsinki for research in humans, and following local institutional review boards regulations. All patients included signed an informed consent before their inclusion.
Results
181 patients with FHGN were included, 124 women (68.5%), with a mean age at the time of biopsy of 41.1 years (SD 16.0) and a median post-biopsy follow-up of 2.9 years (IQR 0.4-6.8 years). 116 patients (64.1%) met the criteria for SLE. Within this group, 103 patients (88.8%) presented with at least one extrarenal manifestation, whereas 13 patients (11.2%) were classified as having SLE based solely on histological and serological findings (renal-limited lupus),52 (28.7%) had identifiable secondary causes of GMN (Figure 1) and 13 (7.2%) remained as idiopathic FHGN. Secondary causes of FHGN. Hepatitis C Virus (HCV), Hepatitis B Virus (HBV), Rheumatoid Arthritis (RA), Immune Complexes (IC), Hemolytic Uremic Syndrome (HUS), Type AA/AL Amyloidosis (AA/AL).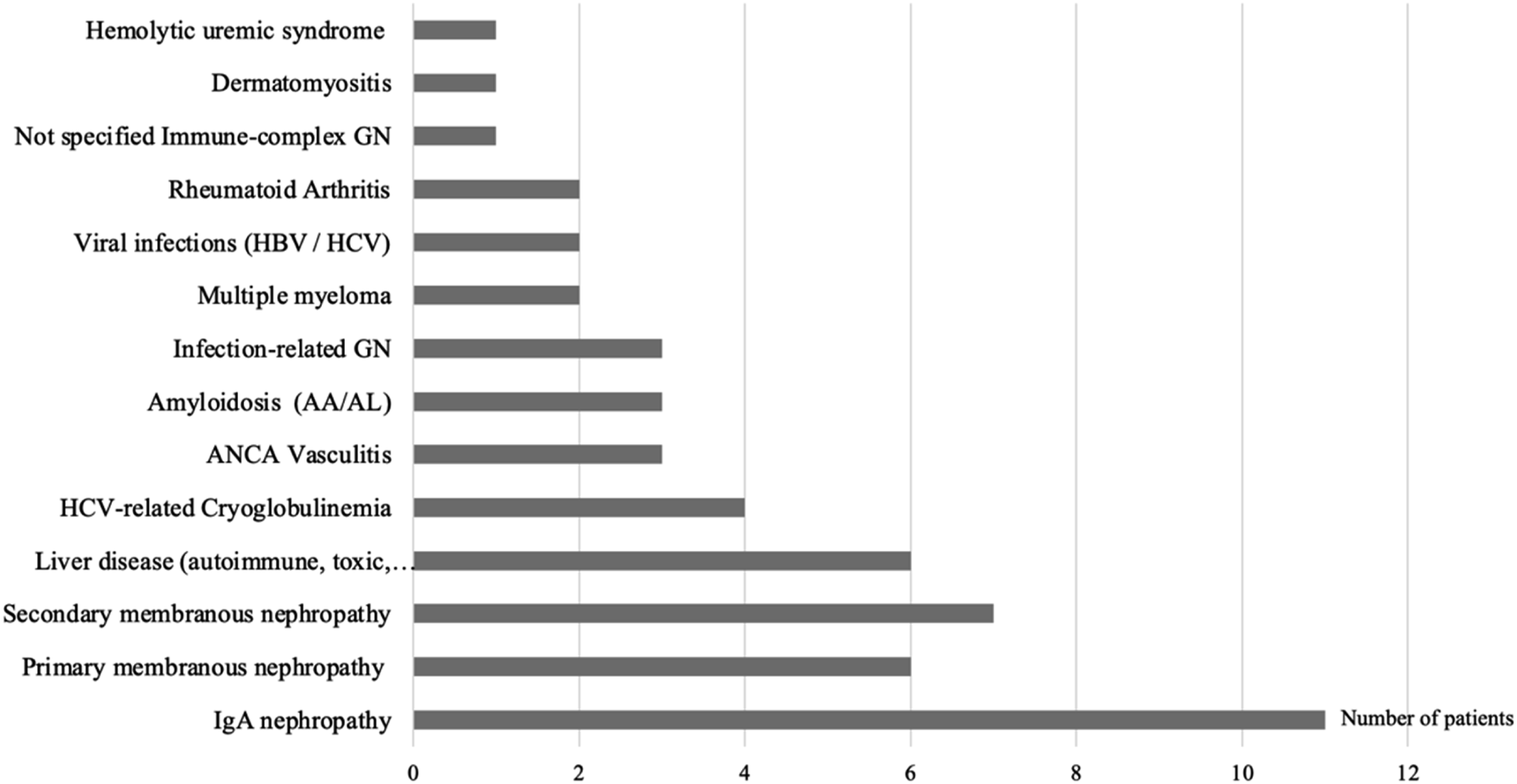
Notably, in our cohort, no patients from the non-lupus or idiopathic groups were reclassified as having SLE during the median follow-up of 2.9 years.
Baseline characteristics.
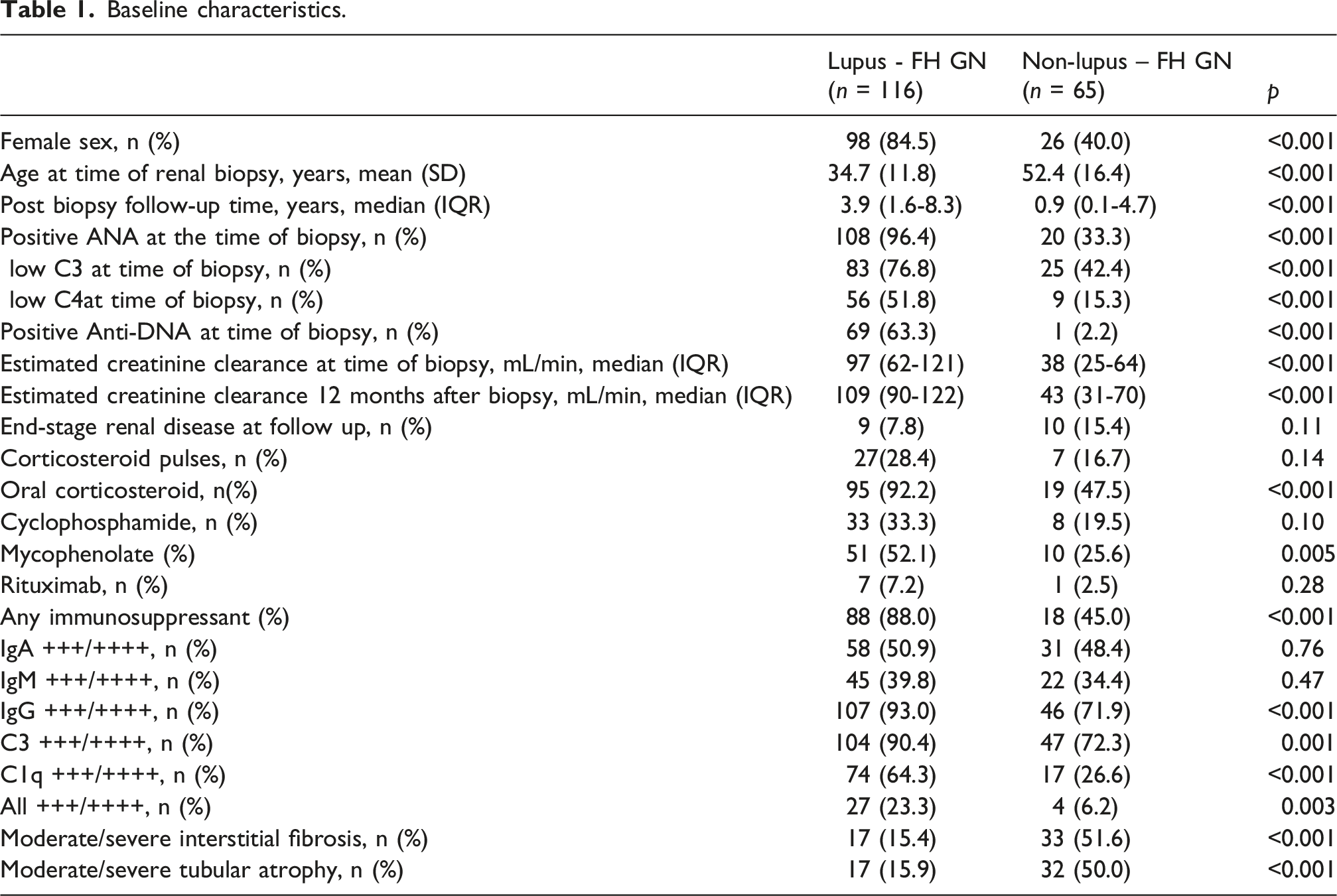
In the immunofluorescence analysis, patients with SLE more frequently presented 3+ or 4+ deposits for IgG, C3, and C1q compared with non-lupus patients (p < 0.001), and showed less moderate-to-severe tubulointerstitial involvement (p < 0.001) (Figure 2). Immunopathological findings.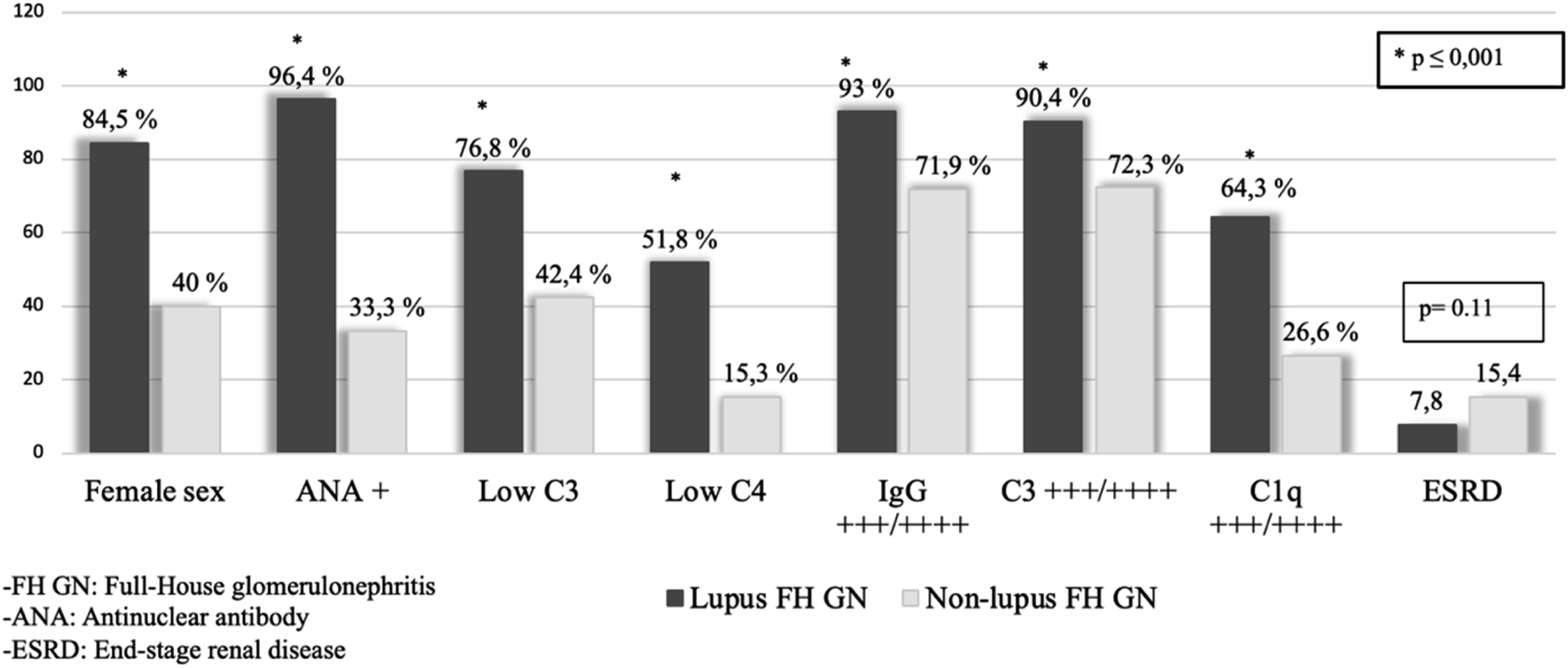
Patients with SLE had higher renal clearance at the time of biopsy (p < 0.001) and a higher proportion of them received treatment with corticosteroids (p < 0.001) and immunosuppressive therapy (p < 0.001). In the multivariate analysis, the factors independently associated with a diagnosis of Lupus as the cause of FHGN were: female sex (Odds Ratio [OR] 0.16; 95% CI 0.05–0.52; p = 0.002), age at diagnosis of GN (OR 0.95; 95% CI 0.91–0.99; p = 0.011), positive ANA at the time of biopsy (OR 1.002; 95% CI 1.000–1.003; p = 0.022), antidsDNA at the time of biopsy (OR 1.02; 95% CI 1.000–1.035; p = 0.043),and intensity of C1q immunofluorescence deposits graded as 3+ or 4+ on a scale of 0 to 4+ in the renal biopsy (OR 3.25; 95% CI 1.08–9.89; p = 0.037).
Intensity of C1q immunofluorescence deposits graded as 3+ or 4+ on a scale of 0 to 4+”. During follow-up, 19 patients developed ESRD, including 9 patients with lupus FHGN and 10 patients with non-lupus FHGN.
The fact of having a FHGN associated with Lupus was protective of ESRD in the univariate analysis (HR 0.34, 95% CI 0.13-0.89), but this association was not significant in the multivariate analysis when adjusting for the fact of having received treatment with corticosteroids or immunosuppressants (Figure 3). Additionally, a sensitivity analysis at 1, 5, and 10 years of follow-up confirmed a consistently lower renal survival rate in the non-lupus cohort across all pre-specified intervals (all p < 0.05). Renal survival. Although median follow-up was 2.9 years, a subset of patients had longer retrospective follow-up, allowing estimation of survival up to 17 years; however, the number at risk beyond 15 years was small.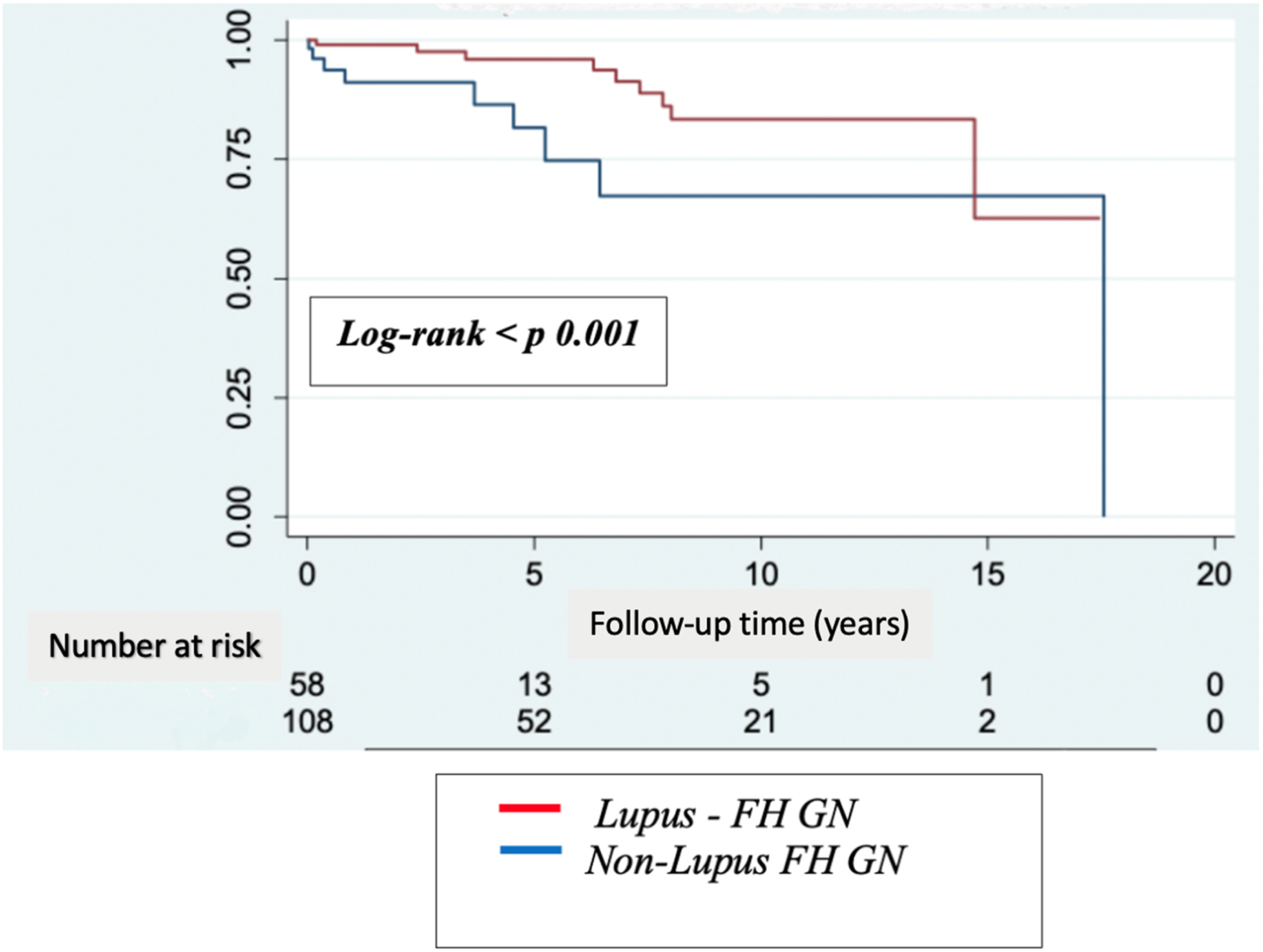
Discussion
In this South American cohort of patients with FHGN, approximately one third of cases were not associated with a diagnosis of SLE, underscoring that the full-house immunofluorescence pattern, although classically linked to lupus nephritis, is not pathognomonic for SLE. The proportion of non-lupus FHGN observed in our cohort (35.9%) is consistent with several previously reported series, in which non-lupus FHGN accounted for approximately 20–30% of cases. Rijnink et al. reported non-lupus FHGN in 22% of patients, while Wen and Chen and Mahanta et al. described frequencies ranging from 25% to 31%, closely aligning with our findings. In contrast, a recent study by Sciascia et al. reported a markedly lower prevalence of non-SLE FHGN. Differences in cohort composition, referral patterns, diagnostic strategies, and inclusion criteria may partially explain this discrepancy. Notably, our study derives from a joint rheumatology–nephrology evaluation in a tertiary referral center, which may facilitate more comprehensive systemic assessment and classification compared with cohorts derived primarily from nephrology settings.6,13–16
Recent evidence has further elucidated the clinical complexity of full-house glomerulonephritis (FHGN). A 2024 systematic review by Uzzo et al. emphasizes that FHGN represents a common immunopathological endpoint for diverse etiologies beyond SLE, a concept that aligns with our identification of various secondary causes in the non-lupus group. 17
Among secondary causes of non-lupus FHGN, IgA nephropathy was the most frequent diagnosis in our cohort, consistent with prior studies that have highlighted IgA nephropathy as a common contributor to the non-lupus full-house pattern. These findings reinforce the concept that FHGN represents a shared histopathological endpoint across heterogeneous immune-mediated renal diseases rather than a disease-specific signature. 6
The full-house histological pattern has always been associated with SLE. However, as seen in this study and in previous ones, there are other causes linked to this pattern in renal biopsy.6,13–15
The term non-lupus FHGN was first described in 24 patients by Wen and Chen. Of these patients, 2 developed systemic lupus erythematosus during follow-up (2-years follow-up period). 13
According to case reports, the frequency of development of SLE in patients diagnosed with non-lupus FHGN is very low.6,15In our patient cohort, none of the patients developed SLE during follow-up (2.9 years follow-up period).
As is well known, SLE can present with nephritis as the only manifestation of the disease, even preceding other clinical features. This has been acknowledged in both the 2012 SLICC and the 2019 ACR/EULAR classification criteria, which allow for the classification of a patient as having SLE if they have biopsy-proven lupus nephritis and positive ANA (according to both criteria) or anti–double-stranded DNA antibodies (according to SLICC), even in the absence of other clinical or serological manifestations.9,10
According to these criteria, there are patients who present with a form of lupus limited to the kidney. A notable finding in our cohort was the identification of a subgroup of patients classified as having SLE based on biopsy-proven lupus nephritis and positive ANA or anti-dsDNA antibodies, but without extrarenal manifestations during follow-up. This presentation corresponds to what has been described as “renal-limited lupus.” This entity was first reported by Jones and Magil in 1982, who described five patients with mesangioproliferative glomerulonephritis and a full-house immune deposition pattern on renal biopsy. The absence of systemic involvement during follow-up supported the concept of a renal-limited form of SLE. 11
In previous studies have reported that idiopathic non-lupus FHGN behaves more aggressively, representing an independent risk factor for ESRD when compared with lupus FHGN. One possible explanation for this is that the immunological profile of SLE along with exposure to immunosuppressive treatment, may modulate renal prognosis in patients with this histological pattern. 6
Taken together, these observations highlight the importance of distinguishing between lupus and non-lupus FHGN, as their clinical course and long-term renal outcomes appear to differ substantially.
In our cohort, possibly because the number of patients with other histopathologic patterns was small, we were unable to demonstrate a difference in these subgroups.
Finally, our observations on renal survival in a South American setting are supported by contemporary regional data, such as the longitudinal study by Polycarpo and Kirsztajn (2025), which underscores the importance of long-term monitoring in similar cohorts. 18
Some limitations should be mentioned. First, we acknowledge a degree of circularity in the analysis of factors associated with Systemic Lupus Erythematosus (SLE). Since variables such as ANA or anti-dsDNA positivity are integral components of the ACR, SLICC, and EULAR/ACR classification criteria, their strong association with the SLE-associated FHGN group was expected. However, our primary objective was to assess the relative contribution and diagnostic weight (represented by Odds Ratios) of these features within the specific and broader population of patients already presenting with a full-house pattern on renal biopsy. This approach allows for a better understanding of which clinical and histological markers—such as the intensity of C1q deposits—provide the most significant clues for differentiating SLE from non-lupus etiologies in daily practice.
The main weakness of our study is the relatively small sample size, which limits the ability to draw robust or definitive conclusions. In addition, it is a single-center study, and therefore the results may reflect the specific characteristics of our patient population and institutional practices limiting the generalizability of our results. Due to the retrospective nature of the analysis, there is also a possibility of underreporting of clinical data in the electronic medical records, which might have led to patient misclassification. However, we carefully reviewed all EMRs, and in general, there was a very complete description of the clinical manifestations, as all patients were hospitalized for kidney biopsy. Finally, since our hospital is a referral center, a selection bias toward more severe cases and patients with poorer treatment responses cannot be ruled out.
The main strengths of this study include the availability of all renal biopsy samples performed during the study period and the opportunity for joint review by rheumatologists, nephrologists, and pathologists. Previous studies on FHGN have often had a predominant renal focus, which may have limited the depth of the systemic autoimmune characterization. By contrast, our joint rheumatology-nephrology evaluation allowed for a more comprehensive systemic clinical assessment of SLE.
On the other hand, we would like to emphasize that this to our knowledge, this is the first Latin American cohort systematically comparing SLE and non-lupus FHGN with joint rheumatology-nephrology evaluation
In conclusion, in our cohort, a third of FHGN were not associated with SLE. Being a woman, younger age, with a positive ANA or with anti-DNA antibodies and with larger C1q deposits in the renal biopsy were associated with the diagnosis of SLE. Patients with Lupus-FHGN less frequently evolved to ESRD. The reason for this may be earlier diagnosis, more aggressive immunosuppression, or distinct immunologic mechanisms.
Footnotes
Ethical considerations
The study was conducted according to the principles of the Declaration of Helsinki for /research in humans, and following local institutional review boards regulations.
Consent to participate
All patients included signed an informed consent before their inclusion.
Author contributions
Study conception and design:
Acquisition of data: all the authors
Data analysis and interpretation and original draft preparation: RT,
All authors contributed to the critical revision of the manuscript and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.