
Abstract
Objective
We aimed to investigate the long-term thrombotic outcomes in patients with obstetric antiphospholipid syndrome (OAPS) who initially presented without thrombosis and to identify clinical features associated with late thrombotic events.
Methods
Female patients with antiphospholipid syndrome (APS) and obstetric manifestations diagnosed at Hokkaido University Hospital between 2004 and 2024 were retrospectively analyzed. Patients were first compared cross-sectionally according to the presence or absence of a history of thrombosis at diagnosis. Among those without prior thrombosis, individuals were further analyzed in a nested case-control study comparing patients who developed new thrombotic events with those who remained event-free for more than 10 years.
Results
Of 47 female APS patients complicated with obstetric manifestations, 23 had a history of thrombosis but not in 24 patients. The prevalence of SLE was higher in the thrombotic group (74%) compared with 40% in the non-thrombotic group (p = 0.019, Fisher’s exact test). During long-term follow-up, 4 of the 24 patients in the absence of prior thrombosis developed a first thrombotic event median of 16 years after the diagnosis. Of the remaining 20 OAPS patients, 9 patients who were observed for more than 10 years without any thrombotic events served as the control group and 11 patents with less than 10 years of follow-up were excluded. The presence of triple antiphospholipid antibodies (aPLs) and accumulation of conventional thrombotic risk factors were more frequent among the cases than the controls.
Conclusion
Thrombotic events may occur in OAPS patients even decades after diagnosis of OAPS, particularly in those with high-risk aPL profiles and conventional thrombotic risk factors. These findings underscore the importance of long-term vigilance and individualized prevention strategies in OAPS management.
Introduction
Antiphospholipid syndrome (APS) is an autoimmune thrombotic disorder characterized by vascular thrombosis and/or pregnancy morbidity in the presence of antiphospholipid antibodies (aPLs). 1 The risk of thrombosis in patients with APS is influenced by both the type and titer of aPLs at diagnosis, as well as the presence of conventional thrombotic risk factors. Obstetric APS (OAPS) is defined as a syndrome presenting solely with pregnancy morbidity and has traditionally been regarded as a lower-risk form than thrombotic APS. 2 However, emerging evidence suggests that aPL-positive individuals without thrombosis can ultimately develop thrombotic events, particularly those with persistent high aPL titers or multiple aPLs. 3 Furthermore, long-term follow-up may reveal changes in thrombotic risk that are not apparent at the time of diagnosis. 4
Long-term clinical data about OAPS extending beyond a decade remain scarce. We aimed to explore the clinical characteristics, risk factors and aPL profiles of OAPS patients, with particular focus on long-term thrombotic outcomes assessed by a nested case-control study.
Method
Study design and setting
Patients diagnosed with APS based on the revised Sapporo classification criteria 5 at Hokkaido University Hospital between April 2004 and September 2024 were analyzed. Male and female without obstetric manifestations were excluded. The study consisted of three parts: a cross-sectional comparison of OAPS patients with and without a history of thrombosis at diagnosis; a longitudinal follow-up of OAPS patients without prior thrombosis to assess the occurrence of late thrombotic events; and a nested case-control study: cases were defined as patients developing a new thrombotic event during follow-up and non-thrombotic groups were defined as patients remaining event-free for more than 10 years of observation. The present study was conducted in accordance with ethical principles of the Declaration of Helsinki and approved by the Hokkaido University Hospital ethics committee (approval number: 025–0438). Clinical data were retrospectively extracted from medical records at the time of diagnosis and during follow-up.
Determination of aPLs
Anticardiolipin (aCL) IgG/IgM and anti-β2 glycoprotein I antibodies (aβ2GPI) IgG and IgM were measured by enzyme-linked immunosorbent assay (ELISA) as previously reported. 6 Phosphatidylserine-dependent antiprothrombin antibodies (aPS/PT) IgG and IgM were measured by in-house ELISA as previously reported. 7 Lupus anticoagulant (LA) was detected based on the guidelines recommended by the Subcommittee for Standardization of the International Society of Thrombosis and Haemostasis. 8
The cut-off values for aPL positivity were established based on previously validated standardizations. Normal ranges of aCL IgG/IgM, aβ2GPI IgG/IgM and aPS/PT IgG/IgM with cut-off values of 99th percentile were established using healthy controls. 9
Definitions and outcomes
Obstetric manifestations were defined according to the revised Sapporo classification criteria. 5 Patients were categorized as those with a prior thrombotic event and those without. Thrombotic events were defined as objectively confirmed thrombosis documented by imaging studies. In the nested case-control analysis, the outcome was the first thrombotic event occurring among patients without prior thrombosis.
Statistical analysis
Continuous variables were expressed as median (interquartile range) and compared using the Mann-Whitney U test. Categorical variables were compared using Fisher’s exact test. A p-value <0.05 was considered statistically significant. All statistical analyses were performed using JMP pro 18 (SAS Institute Inc., Cary, NC, USA). Due to the small sample size, the nested case-control analysis was conducted as a descriptive assessment to avoid overinterpretation of the data.
Results
Baseline characteristics of obstetric antiphospholipid syndrome patients with and without a history of thrombosis at diagnosis.
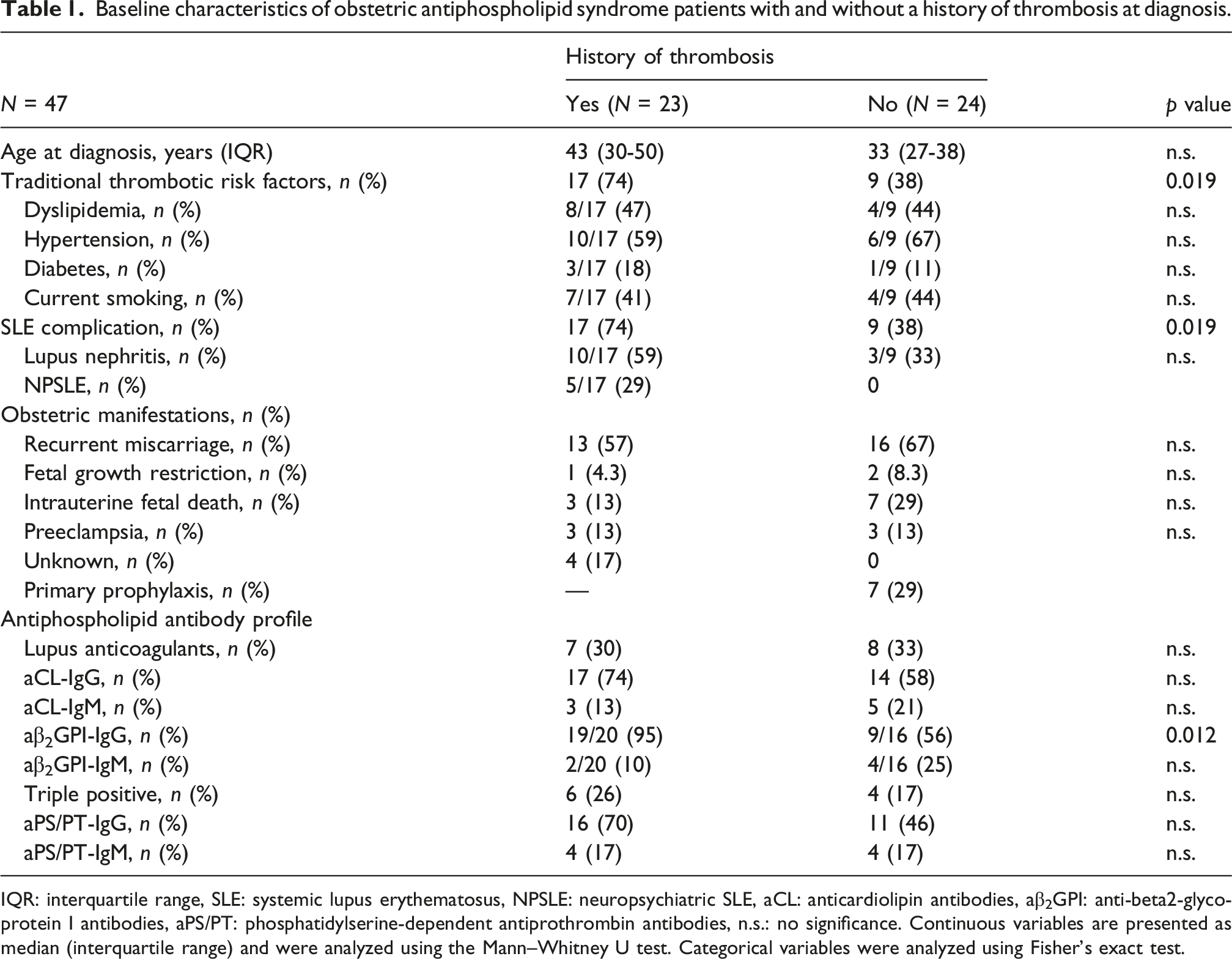
IQR: interquartile range, SLE: systemic lupus erythematosus, NPSLE: neuropsychiatric SLE, aCL: anticardiolipin antibodies, aβ2GPI: anti-beta2-glycoprotein I antibodies, aPS/PT: phosphatidylserine-dependent antiprothrombin antibodies, n.s.: no significance. Continuous variables are presented as median (interquartile range) and were analyzed using the Mann–Whitney U test. Categorical variables were analyzed using Fisher’s exact test.
Among the 24 OAPS patients without a history of thrombosis at diagnosis of APS (median age, 33 years [interquartile ranges (IQR), 27–38]; median observation period, 10 years [IQR, 5.5–18]), 4 patients developed a first thrombotic event after a median of 16 years, during a median observation period of 23.5 years. These patients comprised the case group. Of the remaining 20 OAPS patients, 9 patients who were observed for more than 10 years without any thrombotic events served as the control group (median age, 28 years [IQR, 25.5–35.5]; median observation period, 17 years [IQR, 11.5–19.5]) and 11 patents with less than 10 years of follow-up were excluded. (Supplemental Figure).
Case 1 was a 28-year-old woman with primary APS presented with fetal growth restriction. OAPS was diagnosed based on positive LA, aCL-IgG, aβ2GPI-IgG/IgM and aPS/PT-IgG. She developed dyslipidemia during follow-up and statin therapy was initiated. She experienced a left cerebellar infarction 15 years after diagnosis (at the age of 43), despite primary prophylaxis with LDA. Tests of aPLs showed persistently positive LA, aCL-IgG and aPS/PT-IgG at the time of the thrombotic event. Cilostazol was added, but she developed a right cerebellar infarction 19 years after OAPS diagnosis (at the age of 47). Following this event, we replaced LDA with prasugrel and introduced hydroxychloroquine (HCQ) because this patient did not accept taking warfarin. No further thrombotic events have occurred since the initiation of prasugrel and HCQ.
Case 2 was a 24-year-old woman with primary APS diagnosed following an intrauterine fetal death. OAPS was diagnosed according to positive LA, aCL-IgG/IgM and aPS/PT-IgG at the age of 27. Because she had neither conventional venous thromboembolism (VTE) nor cardiovascular diseases (CVD) risk factors, primary thromboprophylaxis was not given. Fifteen years after OAPS diagnosis (at the age of 42), she developed VTE in the lower extremity. No further thrombotic events have occurred since the initiation of warfarin.
Case 3 was a 25-year-old woman with primary APS presented with one miscarriage and one fetal growth restriction. OAPS was diagnosed based on positive LA, aCL-IgG, aβ2GPI-IgG and aPS/PT-IgG/IgM at the age of 32. She had no CVD risk factors, but she had taken primary prophylaxis with LDA due to elevated risk of thrombosis related to the initiation of starting hormone replacement therapy (HRT) 10 years after OAPS diagnosis. Twenty-three years after diagnosis (at the age of 56), she developed a pulmonary embolism following cessation of HRT. LDA was switched to warfarin with the international normalized ratio maintained between 2.0 and 3.0. No recurrent thrombotic events have been observed since then.
Case 4 was a 35-year-old woman with SLE-associated APS having a history of miscarriage and intrauterine fetal death. She had been treated with prednisolone and tacrolimus for SLE (skin lesions, arthritis, pleuritis) and she did not have either lupus nephritis or neuropsychiatric complications. She experienced a transient ischemic attack (TIA) six years after diagnosis (at the age of 41) and a DVT five years later (at the age of 46). Dyslipidemia was present with receiving no medication, and she underwent HRT. LA became newly positive at the time of first thrombosis with persistently positive aPS/PT-IgG. LDA was initiated after the TIA, and warfarin was added following the DVT. HCQ was introduced 14 years after the diagnosis.
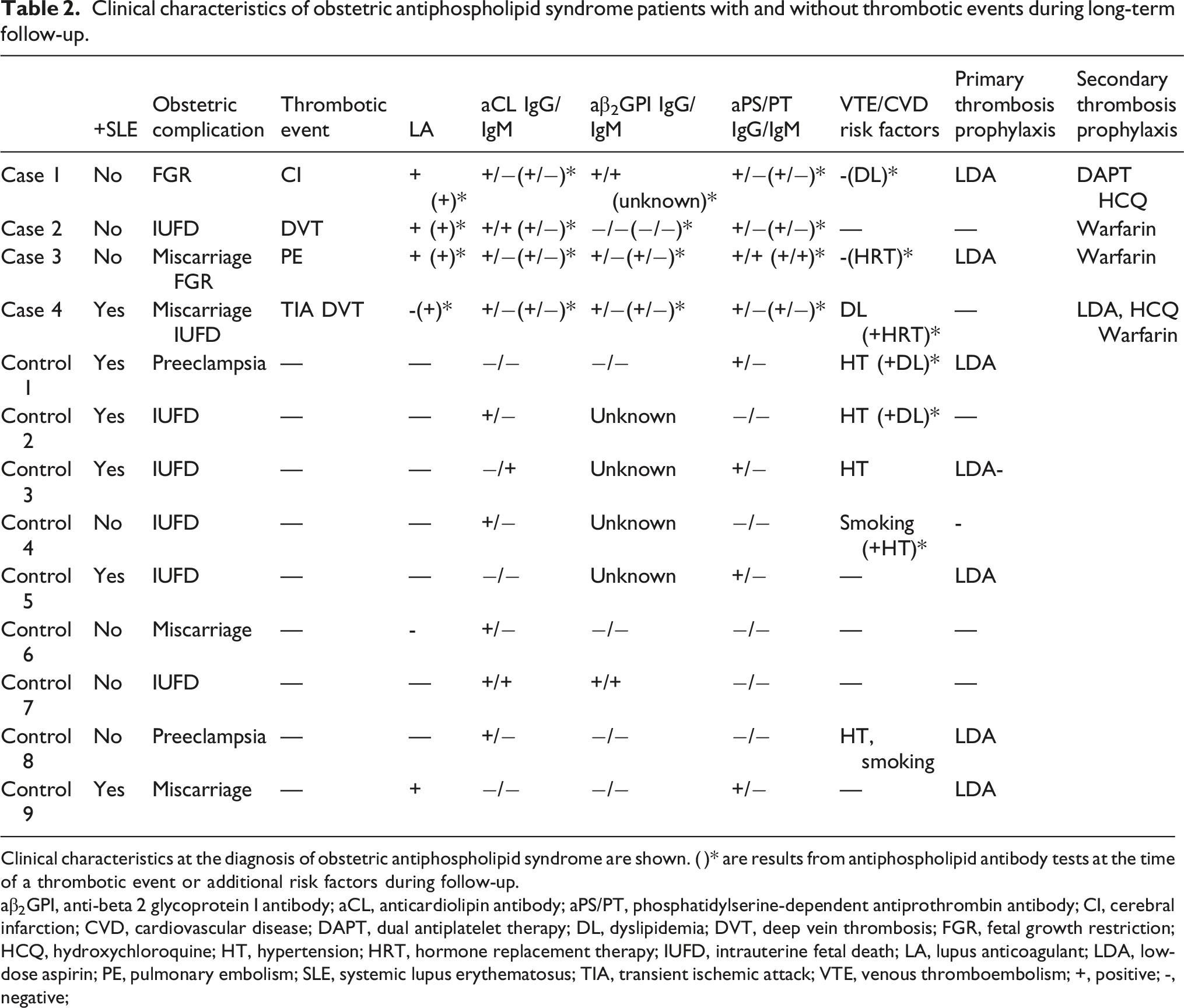
These four cases developed obstetric manifestations in their 20-30s and thrombotic events in their 40-50s even decades after the diagnosis of OAPS (Figure 1). In the nested case-control comparison, the presence of triple aPLs was observed in 3 of 4 cases (75%) but in none of the controls (0%). These aPLs were persistently positive in the four cases at the time of a thrombotic event. Conventional thrombotic risk factors increased over time in 3 of 4 cases (75%), whereas 3 of 9 controls (33%) acquired additional risk factors during follow-up. LDA was prescribed as primary prophylaxis in 2 of 4 cases (50%) and in 5 of 9 controls (56%). Detailed clinical features of cases and controls are summarized in Table 2. Specific antibody titers for the patients who developed thrombosis and the mean titers for the remaining patients are indicated in Supplemental Table. Age at each event and observation period of obstetric APS (OAPS) patients without a history of thrombosis. Scatter plot showing the age at obstetric complication, diagnosis and thrombotic events and duration of follow-up for 24 OAPS patients without prior thrombosis at baseline. Each arrow represents an individual patient. Patients who experienced thrombotic events during follow-up (cases) and those who remained event-free (controls) are distinguished. Clinical characteristics of obstetric antiphospholipid syndrome patients with and without thrombotic events during long-term follow-up. Clinical characteristics at the diagnosis of obstetric antiphospholipid syndrome are shown. ( )* are results from antiphospholipid antibody tests at the time of a thrombotic event or additional risk factors during follow-up. aβ2GPI, anti-beta 2 glycoprotein I antibody; aCL, anticardiolipin antibody; aPS/PT, phosphatidylserine-dependent antiprothrombin antibody; CI, cerebral infarction; CVD, cardiovascular disease; DAPT, dual antiplatelet therapy; DL, dyslipidemia; DVT, deep vein thrombosis; FGR, fetal growth restriction; HCQ, hydroxychloroquine; HT, hypertension; HRT, hormone replacement therapy; IUFD, intrauterine fetal death; LA, lupus anticoagulant; LDA, low-dose aspirin; PE, pulmonary embolism; SLE, systemic lupus erythematosus; TIA, transient ischemic attack; VTE, venous thromboembolism; +, positive; -, negative;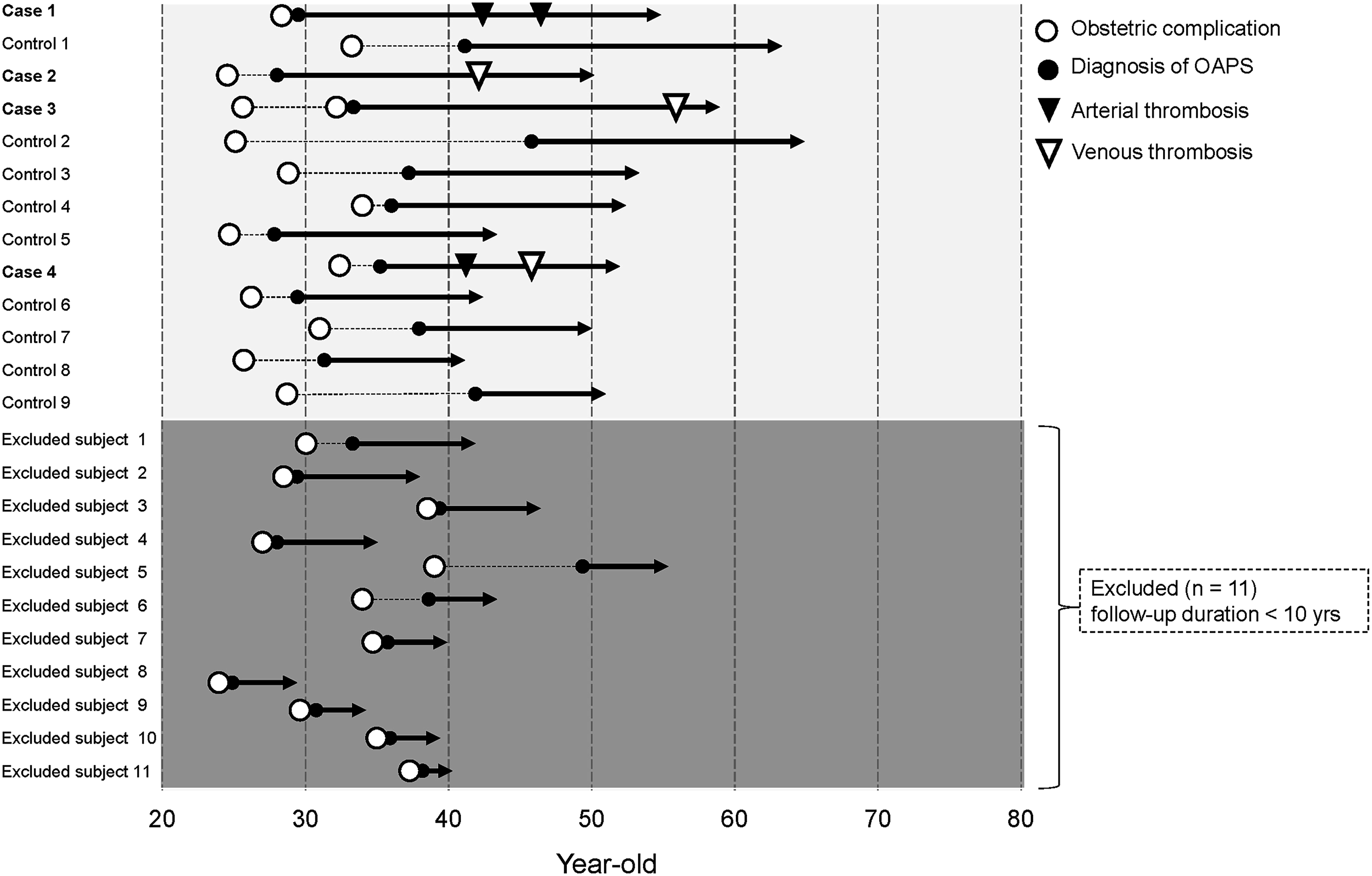
Discussion
OAPS has traditionally been considered to carry a lower thrombotic risk than thrombotic APS, particularly in patients without a prior history of thrombosis or comorbid autoimmune disease. 2 However, as illustrated by the present four cases, thrombotic events could occur after prolonged asymptomatic periods, even in patients initially considered to be at low risk. These findings suggest that OAPS should not be underestimated in terms of long-term thrombotic potential and warrant a more nuanced approach to risk assessment and monitoring.
Previous cohort studies have reported that OAPS patients without prior thrombosis but with high-risk aPL profiles, such as triple positive aPLs or hypocomplementemia, were more likely to experience a first thrombotic event within only a few years of OAPS diagnosis. 10 While their studies demonstrated risk over a relatively short timeframe (mean follow-up 5.4 years), our findings highlight that such thrombotic events can occur even decades after diagnosis, particularly in 40–50 s. Our findings therefore extend existing evidence, underscoring the need for sustained vigilance in long-term follow-up. Indeed, a recent analysis demonstrated that the frequency of thrombotic events as the initial APS manifestation progressively increases with age. 11 This suggests that the age-related accumulation of thrombotic risk factors over decades may subsequently trigger thrombosis in OAPS patients.
From a clinical perspective, these findings emphasize the importance of individualized long-term management strategies for OAPS patients, particularly regarding CVD and thrombotic risk modification. Recent findings support this concept, demonstrating traditional CVD risk factors such as hypertension and hyperlipidemia are independent predictors of organ damage even in non-thrombotic aPL-positive patients. 12 It is also crucial to perform regular reassessment of CVD risk throughout the disease course. Previous reports indicated that CVD risk management was suboptimal in APS patients compared with those with rheumatoid arthritis or diabetes mellitus. 13 Furthermore, de Jesús et al. revealed that incorporating objective tools like the adjusted Global Antiphospholipid Syndrome Score is highly valuable for risk stratification, as higher baseline scores significantly increase the risk of subsequent thrombosis. 14 Current recommendations suggest that LDA for primary prophylaxis should be considered in OAPS patients after adequate risk-benefit evaluation. 15 Our 2 patients who suffered thrombosis, did not receive LDA although one of them had triple aPLs, and the other had SLE and dyslipidemia. Quantification and management of modifiable risk factors, and appropriate primary prophylaxis with LDA could reduce early cardiovascular burden in this population.
This study has several limitations. First, it was conducted at a single tertiary center with a relatively small number of patients, which may limit the generalizability of the findings. Second, its retrospective design may have introduced selection and information biases, despite systematic data extraction from medical records. Third, the limited number of thrombotic events precluded multivariate analysis to identify independent predictors of long-term thrombosis. Finally, laboratory assays for aPLs were not fully standardized across the two-decade study period, which could have influenced aPL profiling.
Future studies with larger multicenter cohorts and standardized laboratory testing are warranted to validate our observations and to develop risk prediction models specific to OAPS. In addition, prospective designs incorporating longitudinal monitoring of both aPL profiles and modifiable CVD risk factors would help establish evidence-based strategies for primary prevention. Such efforts could ultimately improve individualized long-term management and outcomes in OAPS.
Conclusion
The present study highlighted that thrombotic events occurred in OAPS patients even after prolonged event-free intervals. Despite being traditionally viewed as a lower-risk subgroup, our findings underscore the need for individualized long-term monitoring and risk assessment in OAPS. Although limited by the small number of patients, our results would expand current knowledge by showing that the thrombotic potential of OAPS extends well beyond the early disease course.
Supplemental material
Supplemental material - Longitudinal observation of thrombotic events in patients with obstetric antiphospholipid syndrome
Supplemental material for Longitudinal observation of thrombotic events in patients with obstetric antiphospholipid syndrome by Yuta Inoue, Hiroyuki Nakamura, Yuichiro Fujieda, Mitsutaka Yasuda, Kohei Karino, Ryo Hisada, Michihito Kono, Olga Amengual, Tatsuya Atsumi, in Lupus
Supplemental material
Supplemental material - Longitudinal observation of thrombotic events in patients with obstetric antiphospholipid syndrome
Supplemental material for Longitudinal observation of thrombotic events in patients with obstetric antiphospholipid syndrome by Yuta Inoue, Hiroyuki Nakamura, Yuichiro Fujieda, Mitsutaka Yasuda, Kohei Karino, Ryo Hisada, Michihito Kono, Olga Amengual, Tatsuya Atsumi, in Lupus
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Hokkaido University.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Y.F. has received research grants from MEDICAL & BIOLOGICAL LABORATORIES Co., Ltd. and Taisho Pharmaceutical Co., Ltd.. R.H. has received speaking fees from AbbVie, Asahi-Kasei, Astellas, Ayumi, Bristol-Myers Squibb, Chugai, Daiichi Sankyo, Eisai, Janssen, Nippon Boehringer Ingelheim, Mitsubishi Tanabe, Otsuka and Pfizer. M. Kono reports grants and/or speaking fees from AbbVie, Asahi-Kasei, Astellas, AstraZeneca, Ayumi, Bristol-Myers Squibb, Chugai, Daiichi Sankyo, Eisai, Eli Lilly, Gilead Sciences, GlaxoSmithKline, Janssen, Kowa, Kissei, Kyocera, Kyowa Kirin, Lotte, Nippon Boehringer Ingelheim, Nippon Shinyaku, Mitsubishi Tanabe, Mochida, Pfizer, Sandoz, Taiju Life Social Welfare Foundation, Taisho, Takeda, Terumo, UCB Japan and Yamazaki Baking, outside the submitted work. T.A. has received research grants from GlaxoSmithKline, Bristol-Myers, Zenyaku Kogyo, Amgen, Kissei, AbbVie, Mitsubishi Tanabe, Eisai, Nippon, Otsuka and Chugai; consultant fees from AstraZeneca, Idorsia, Otsuka, Gilead Sciences, GlaxoSmithKline, Sanofi, Eli Lilly, Nippon Boehringer Ingelheim, Janssen, UCB Japan, Kissei and Novartis; and speaking fees from Bristol-Myers, Eli Lilly, Nippon Boehringer Ingelheim, Eisai, AbbVie, Pfizer and Gilead Sciences. The remaining authors have declared no conflicts of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.