
Abstract
Objective
This study aims to elucidate the novel role of serum receptor interacting protein kinase 3 (RIPK3)/mixed series of protein kinase-like domains (MLKL) levels in SLE and assess their correlation with clinical manifestations and serological parameters.
Methods
We employed enzyme-linked immune sorbent assay (ELISA) analysis to evaluate RIPK3/MLKL protein levels in serum from 90 SLE patients and 50 healthy controls (HC).
Results
Our findings reveal a significant elevation of serum RIPK3/MLKL protein levels in SLE patients compared to HC (p = 0.0004 and p = 0.0005, respectively). Notably, these levels were closely associated with the disease’s clinical manifestations, notably heightened in active SLE compared to stable cases (p = 0.0312 and p = 0.0096, respectively). Furthermore, while RIPK3 protein exhibited significant upregulation in patients with lupus nephritis (LN) compared to non-LN individuals (p = 0.0017). SLE patients with high anti-nuclear antibody (ANA) titers exhibited notably higher RIPK3 levels compared to those with low ANA titers (p < 0.0001). The receiver operating characteristic (ROC) curve demonstrated diagnostic potential for serum RIPK3/MLKL, with respective areas under the curve (AUCs) of 0.6319 (p = 0.0099) and 0.7374 (p < 0.0001).
Conclusions
Our study illuminate serum RIPK3/MLKL proteins are exploratory biomarker candidates for SLE and necroptosis may be involved in SLE pathogenesis.
Introduction
Systemic lupus erythematosus (SLE) represents a complex and multifaceted systemic autoimmune disorder, characterized by its heterogeneity and absence of curative treatments, thereby inflicting significant patient distress. Recent epidemiological data indicates an annual incidence rate of approximately 5.14 per 100,000 individuals, imposing substantial socioeconomic implications on both clinical practice and society. 1 The pathogenesis of SLE remains enigmatic, with pervasive chronic inflammation and excessive autoantibody production observed across the majority of SLE cases. 2 Within the context of SLE, uncontrolled programmed cell death culminates in the widespread release of intracellular components and damage-associated molecular patterns (DAMPs) into the bloodstream. This event acts as a stimulus, fostering the generation of autoantibodies, immune complexes, and inflammatory mediators. 3 While numerous studies have unveiled the roles of apoptosis, NETosis, and pyroptosis in the SLE and lupus nephritis (LN) contexts, limited attention has been dedicated to the role of necroptosis in SLE progression.
Necroptosis, a lytic form of cell death, hinges on the concerted action of receptor interacting protein kinase 3 (RIPK3) and its effector mixed series of protein kinase-like domains (MLKL). Necroptosis is initiated by a multitude of stimuli, encompassing tumor necrosis receptor (TNFR), death receptors, interferon receptors (INFR), toll-like receptors (TLR3 and TLR4), and intracellular RNA and DNA sensors binding to their respective ligands.4,5 Following RIPK3 activation, MLKL undergoes phosphorylation, orchestrating the formation of membrane pores that induce cellular lysis, thereby facilitating the release of cellular contents and exposing DAMPs, such as high-mobility group box-1 (HMGB-1). Our previous articles revealed that necroptosis activation was important in host anti-tumor immunity, bacterial infection and cancer metastasis.6,7 Additionally, both LN patients exhibit hyperactivated RIPK3/MLKL and SLE patients display elevated serum mRNA MLKL levels.8,9 While a conjectural link between necroptosis and SLE pathogenesis has been postulated, there exists a paucity of literature investigating the interaction between RIPK3 and MLKL proteins in the context of SLE. Accordingly, this study endeavors to explore the protein levels of RIPK3/MLKL within distinct subgroups of SLE patients and health controls (HC) using serum analysis.
In this paper, our observation showed the notable elevation of serum RIPK3/MLKL levels in SLE patients, which exhibited close associations with disease activity, the production of autoantibodies and renal involvement. Collectively, our findings underscore the potential involvement of necroptosis in the pathogenesis of SLE and the potential utility of RIPK3/MLKL as exploratory biomarker candidates for this condition.
Materials and methods
Study cohorts
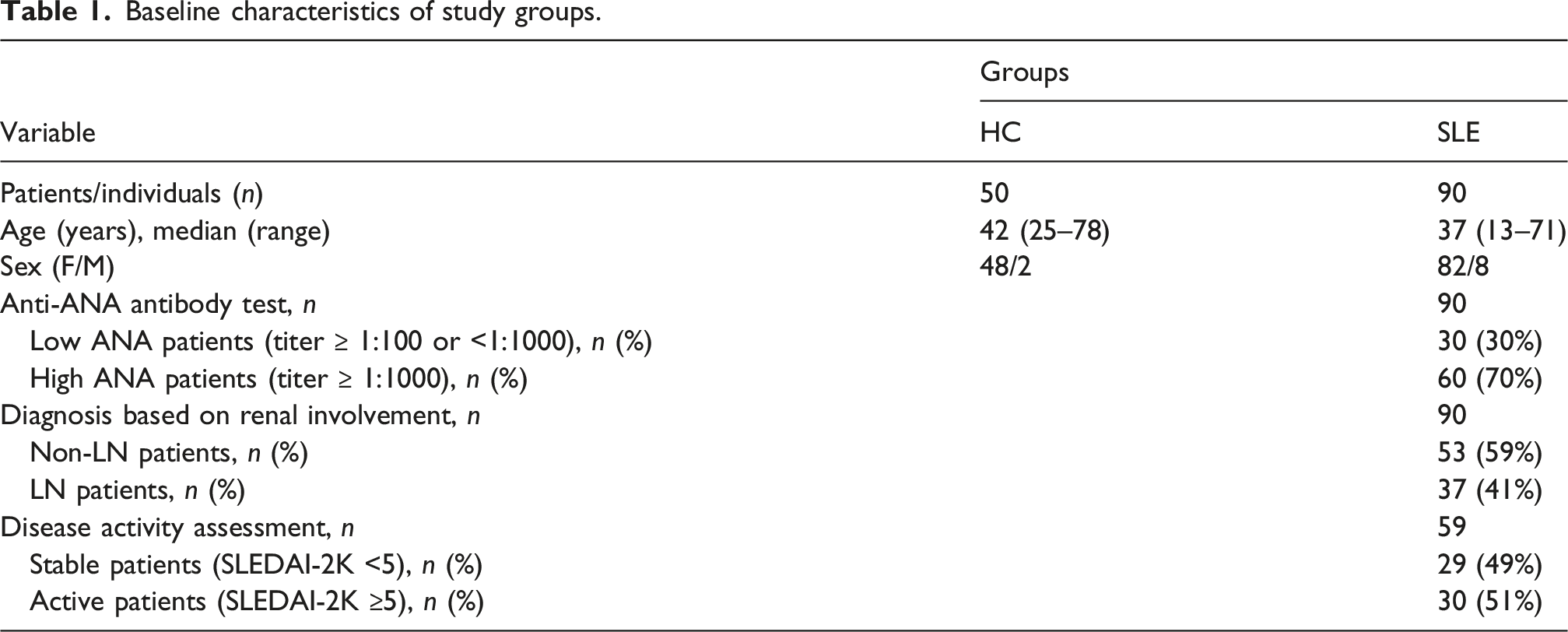
This is a cross-sectional observational study. SLEDAI-2 K scores assessment were started on the same day as blood collection. A cohort comprised 90 SLE patients and 50 HC individuals based on some criteria. Those patients met the 2019 European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR) classification criteria 10 and without other autoimmune diseases were included; those SLE patients coexisted with infections, chronic or malignant diseases were excluded. Those HC individuals with no history of SLE or other immune disorders were included and those who experienced chronic or malignant diseases were exclude. All enrollers recruited from the Yueyang People’s Hospital, during the period of March 2024–May 2025 following the ethical consent approved by human ethics committee. Comprehensive information pertaining to the study was communicated to all participants, and their consent was duly acquired. Subsequently, serum samples were procured, and clinical data, along with laboratory parameters, were systematically collected within the same time frame.
Baseline characteristics of study groups.
Enzyme-linked immunosorbent assay (ELISA)
Serum levels of RIPK3/MLKL and HMGB-1 were quantified using commercially available enzyme-linked immunosorbent assay (ELISA) kits according to the manufacturers’ instructions. The RIPK3/MLKL ELISA kit (Jonln, China) has a sensitivity of 0.08 ng/mL, a detection range of 0.156–10 ng/mL, and an intra-assay coefficient of variation (CV) of <10%. The HMGB-1 ELISA kit (Elabscience, China) has a sensitivity of 18.75 pg/mL, a detection range of 31.25–2000 pg/mL, and an intra-assay CV of <10%. All serum samples were collected under fasting conditions. Within 1 h after collection, the samples were centrifuged at low speed (1000 rpm for 10 min) to obtain the serum, which was then stored at −80°C and assayed within 1 month.
Statistical analysis of clinical data
Data were analyzed using GraphPad Prism 9 and SPSS and expressed as Mean ± SD for normally distributed variables. Normality was assessed by Shapiro-Wilk test. For two-group comparisons, Mann-Whitney U test was used for abnormally distributed variables and Unpaired t test was used for normally distributed variables. Correlations were assessed by Pearson correlation test. ROC curve analysis was carried out to evaluate diagnostic performance. Binary logistic regression analysis was performed to adjust for potential confounders including BMI, steroid use, hydroxychloroquine, mycophenolate mofetil, and belimumab, with SLEDAI-2K or proteinuria as independent variables. Pre-specified primary hypotheses included: SLE versus HC, active versus stable SLE (SLEDAI-2K ≥5 vs < 5), LN versus non-LN, and proteinuric versus non-proteinuric subgroups. All other subgroup analyses (e.g., autoantibody, CRP/ESR, complement subgroups) were considered exploratory. Given multiple comparisons, p-values in exploratory analyses are descriptive and risk of type I error is acknowledged; independent validation is required. Significance was set at p < 0.05.
Results
Characteristics of participates
Association of serum RIPK3/MLKL levels with clinical parameters and subgroups of SLE.
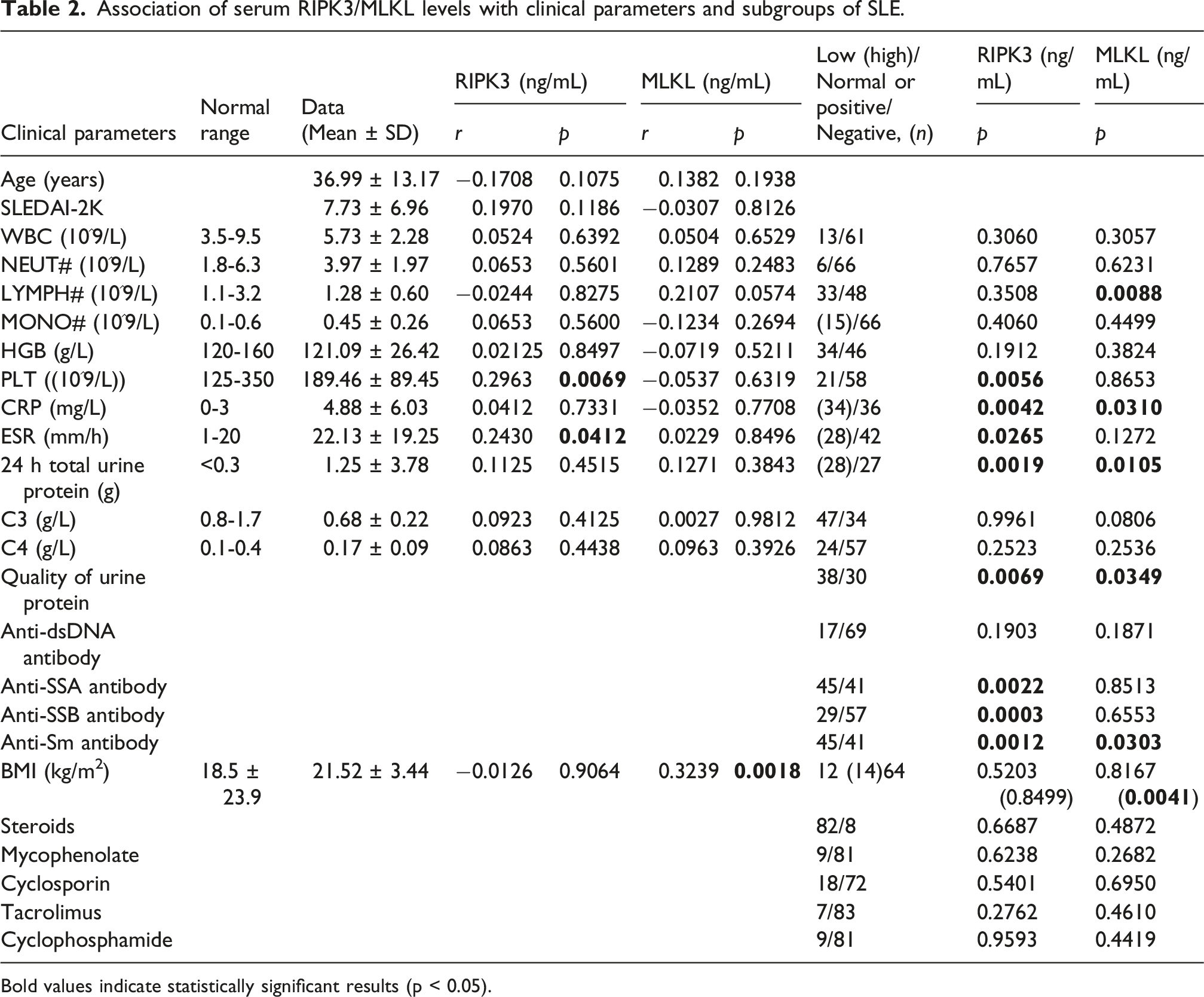
Bold values indicate statistically significant results (p < 0.05).
Serum RIPK3 and MLKL were upregulated in SLE patients
To elucidate the role of serum RIPK3/MLKL levels in SLE, we employed a specific quantitative diagnostic ELISA kit. Our findings demonstrated markedly elevated serum RIPK3 and MLKL protein levels in SLE patients compared to HC individuals (p = 0.0004 and p = 0.0005, respectively, Figure 1(a), (d)). Active SLE, characterized by more extensive systemic involvement and a less favorable prognosis, prompted us to explore these levels in distinct SLE patient subgroups.
11
Further analysis within these subgroups unveiled significantly higher RIPK3 and MLKL levels in active patients than in stable patients (p = 0.0312 and p = 0.0096, respectively) (Figure 1(b), (e)). Notably, the LN subgroup exhibited notably elevated RIPK3 levels compared to the non-LN subgroup (p = 0.0017) (Figure 1(c)), while no such difference was observed in MLKL (p = 0.4232) (Figure 1(f)). The differential concentrations of serum RIPK3/MLKL in HC and SLE and its two subgroups. (a/d) HC individuals (n = 50) versus SLE patients (n = 90). (b/e) stable (SLEDAI-2K <5, n = 29) versus active (SLEDAI-2K ≥5, n = 30) SLE patients. (c/f) Non-LN patients (n = 53) versus LN patients (n = 37). *p < 0.05; **p < 0.005; ***p < 0.001; ****p < 0.0001; ns: p ≥ 0.05.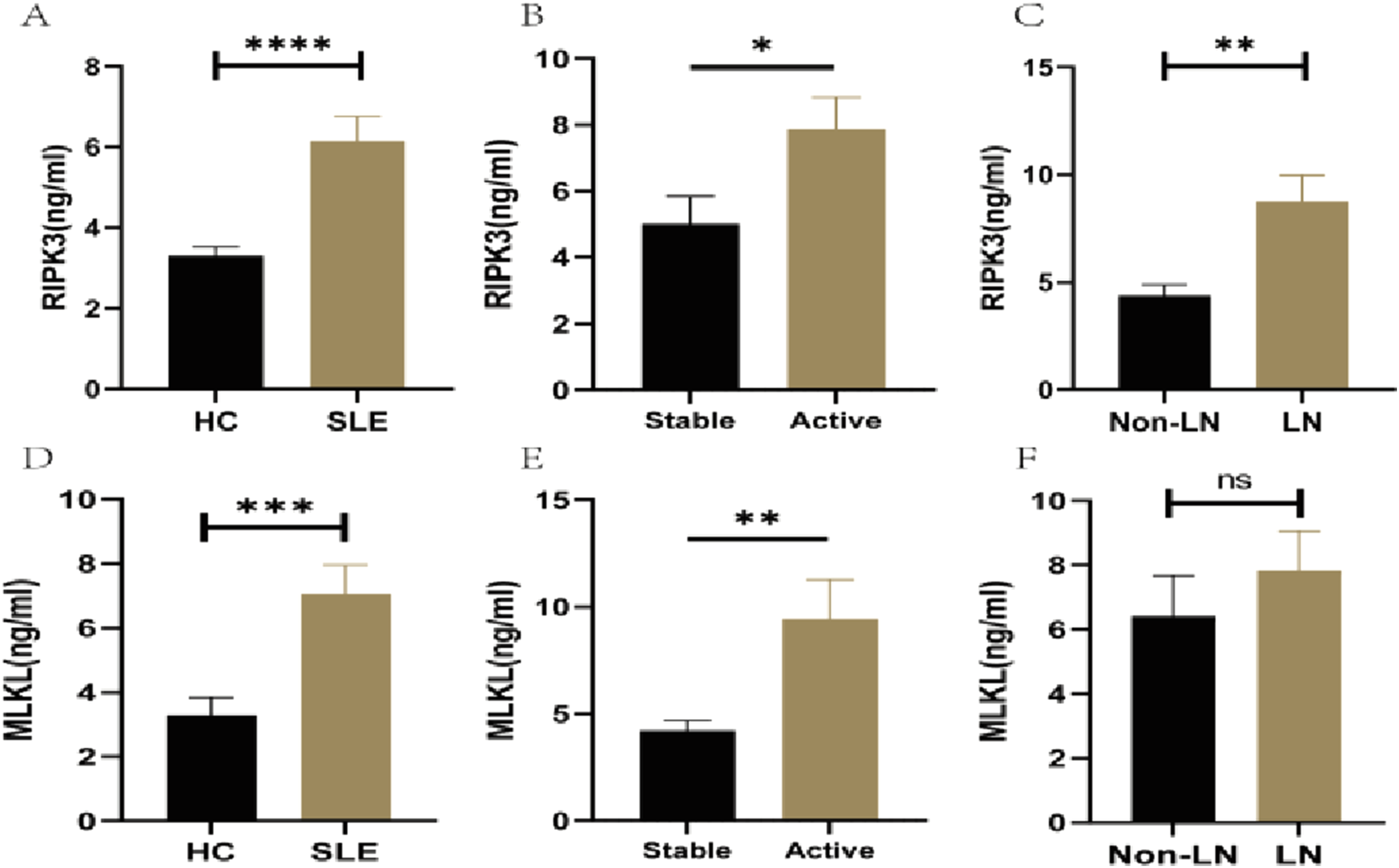
As exploratory analysis, the association between RPK3/MLKL and some variables related to SLE were explored. Elevated RIPK3 levels were detected in high ANA patients compared to their low ANA counterparts (p < 0.0001) (Figure 2(a)), whereas MLKL levels showed no such distinction (p = 0.3338) (Figure 2(b)). Moreover, a discernible pattern emerged in various antibody-positive subgroups, with significantly higher RIPK3 levels observed in anti-SSA (p = 0.0022), anti-SSB (p = 0.0003), and anti-Sm (p = 0.0012) subgroups (Figure 2(a)). However, this divergence was not evident in MLKL levels (Figure 2(b)). Furthermore, both RIPK3 and MLKL protein levels were more pronounced in subgroups with positive urine protein quality than in their negative counterparts (p = 0.0069 and p = 0.0349, respectively). Similarly, in subgroups with 24-h total urine protein exceeding 300 mg, both RIPK3 and MLKL protein levels were significantly elevated (p = 0.0019 and p = 0.0105, respectively) (Figure 2(c) and (d)). No significant differences in both RIPK3 and MLKL levels were noted between low and normal C3 level subgroups (Figure 2(c) and (d)). Detailed results are presented in Table 2. In sum, our results underscore a correlation between serum RIPK3/MLKL concentrations and SLE disease progression. Particularly, RIPK3 was significantly upregulated across various clinical classifications, providing insights into the pathogenesis of SLE. In multivariable analysis adjusting for gender, age, anti-ANA antibody, anti-dsDNA antibody, anti-Sm antibody, BMI and major immunosuppressive treatments (steroids, Mycophenolate, Cyclosporin, Tacrolimus), The results showed that the associations with active disease (OR = 1.055, 95% CI = 1.021–1.238, adjusted p = 0.049), LN (OR = 0.008, 95% CI = 1.045–1.333, adjusted p = 0.008) and proteinuria (OR = 1.238, 95% CI = 1.048–1.462, adjusted p = 0.012) remained significant for RIPK3 but not for MLKL. Details are shown in Supplemental Table S1. The differential concentrations of serum RIPK3/MLKL in other SLE subgroups. (a/b) autoantibodies subgroups; (c/d) routine laboratory results. *p < 0.05; **p < 0.005; ***p < 0.001; ****p < 0.0001.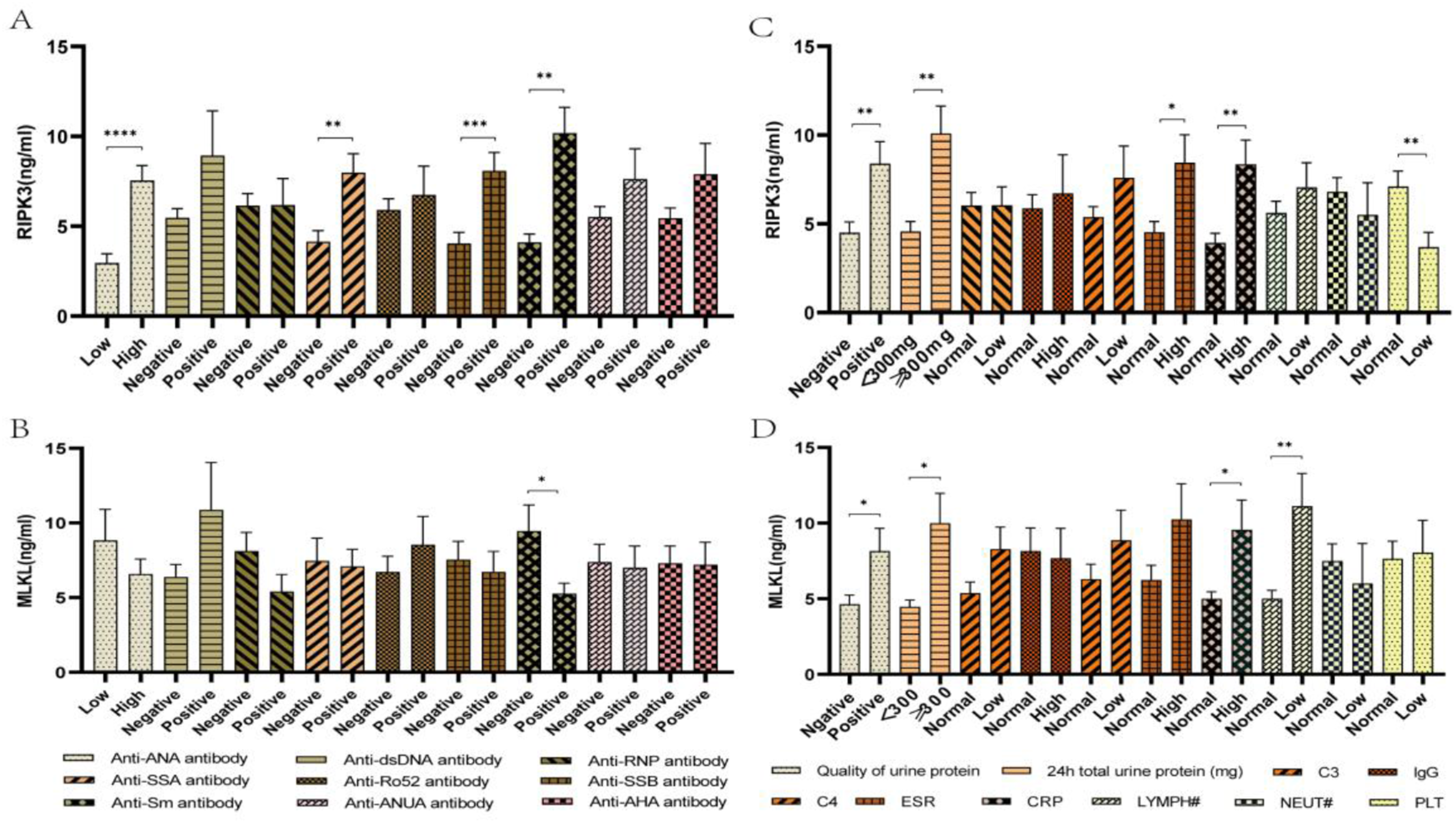
Serum RIPK3/MLKL levels were positively correlated with laboratory parameters of SLE
For a more comprehensive understanding of the correlation between elevated RIPK3/MLKL expression and SLE disease progression, an exploration of clinical laboratory parameters was undertaken. This investigation aimed to unravel the intricate relationship between these variables. Detailed results are presented in Table 2 and Supplemental Table 2. As exploratory analysis, serum MLKL levels exhibited a notable increase in subgroups with lower lymphocyte (LYMPH) counts (p = 0.0088) and RIPK3 levels significant upregulated in low platelet (PLT) count subgroups (p = 0.0056), compared to normal subgroups. Notably, both RIPK3 and MLKL levels were markedly elevated in subgroups with higher C-reactive protein (CRP) levels in contrast to normal subgroups (p = 0.042 and p = 0.0310, respectively). Elevated RIPK3 levels were also observed in subgroups characterized by higher erythrocyte sedimentation rate (ESR) values relative to normal subgroups (p = 0.0412), although this distinction was not evident in MLKL levels. Furthermore, both RIPK3 and MLKL levels displayed a significant correlation with renal damage markers, including 24-h total urine protein (p = 0.0019 and p = 0.0105, respectively) and the quality of urine protein (p = 0.0069 and p = 0.0349, respectively). Additionally, the MLKL levels were positively related to body mass index (BMI) of the patients (r = 0.3239, p = 0.0018). Neither the history of smoking or drinking nor the treatments of various medicines unshown the association with the level of RIPK3 or MLKL in our cohort.
Serum RIPK3/MLKL/HMGB1 levels were sensitive for the diagnosis of SLE
The concentration of RIPK3 demonstrated a positive correlation with ESR (r = 0.2430, p = 0.0412) (Figure 3(a)) and PLT count (r = 0.2963, p = 0.0069) (Figure 3(b)). HMGB-1 as a kind of DAMPs is a nuclear non-histone protein, which is released from lytic cell death and closely connected with SLE progression.
12
To further uncover the relationship between necroptosis and SLE, the level of HMGB-1 was detected from participator serum involving 16 HC individuals and 24 SLE patients using ELISA. The concentration of HMGB-1 displayed a significantly increase in SLE compared to HC (p < 0.0001) (Figure 3(c)) and exhibited a positive correlation with RIPK3 and MLKL concentrations (r = 0.4931, p = 0.0014 and r = 0.4762, p = 0.0029, respectively) (Figure 3(d) and (e)), besides, it demonstrated potentially diagnostic value for SLE (AUC = 0.9948, p < 0.0001) in this exploratory analysis (Figure F). However, this result was derived from a small subset and should be interpreted with caution; overfitting is possible. Employing ROC analysis, the diagnostic potential of serum RIPK3 and MLKL protein levels for identifying SLE patients was assessed. Both proteins showed modest diagnostic capacity in this cohort (AUC = 0.6319, p = 0.0099 and AUC = 0.7374, p < 0.0001, respectively) (Figure 3(h) and (i)). Consequently, our findings suggest that serum RIPK3/MLKL concentrations hold promise as exploratory biomarker candidates for SLE. Correlations of serum RIPK3/MLKL levels with SLE clinical parameters, serum HMGB-1 levels and ROC analysis of them for SLE patients. ****p < 0.0001.
Discussion
In this paper, we embarked on a comprehensive exploration, uncovering novel insights into the augmented serum concentrations of RIPK3/MLKL/HMGB-1 in SLE patients. Particularly noteworthy is their pronounced elevation in subjects exhibiting active disease and renal involvement. These associations were corroborated by their interrelation with clinical laboratory parameters and demonstrated diagnostic potential through ROC curve analysis. Given the cross-sectional design, these associations do not imply causality; elevated RIPK3/MLKL levels may reflect disease activity or secondary phenomena rather than a direct pathogenic role in SLE initiation.
SLE is a chronic autoimmune disorder characterized by elevated levels of autoantibodies and Interferon Type I (IFN-I) in serum.13,14 Excessive cell death and impaired dead cell clearance contribute to an accumulation of intracellular components, thus serving as a major source of autoantigens. 15 Concurrently, aberrant cell death exacerbates the release of DAMPs, intensifying the IFN-I release. 16 Importantly, necroptosis, a form of lytic cell death, is triggered or heightened not only by free nucleic acids but also by IFN-I.4,5 Notably, IgG, both from lupus mice and SLE patients, can activate the necroptosis pathway.9 Furthermore, IFN-I not only sustains the activation of RIPK3 but also maintains MLKL expression, thereby amplifying necroptosis.4,17 This intricate relationship between necroptosis and IFN-I/autoantibodies forms a self-perpetuating loop. Despite the compelling indications of necroptosis’s involvement in SLE, few articles have thoroughly explored this connection. While certain studies have suggested the activation of the RIP3-dependent NLRP3 inflammasome pathway in podocytes during LN and the significant upregulation of MLKL mRNA in PBMCs of SLE patients, the serum levels of RIPK3 in SLE patients have not been investigated. Filling this gap, our study focuses on unraveling the link between serum levels of RIPK3 and MLKL proteins in SLE patients and their association with disease characteristics. Quantifying protein levels provides more immediate insights compared to mRNA levels, which are subject to various transcriptional fluctuations. Our findings, akin to those of MJ Zhang, demonstrate a significant increase in serum RIPK3/MLKL levels in SLE. These results notably advance our comprehension of necroptosis’s role in SLE pathogenesis.
As known to all, SLE is a chronic, systemic inflammatory disorder affecting multiple organs, renal impairment stands as one of the most prevalent manifestations. 18 The significance of necroptosis in various kidney diseases has been substantiated in existing literature. 19 Demonstrative of this, research by CH Guo et al.8,9 illustrated the activation of both RIPK3 and MLKL in LN patients as well as MRL/lpr SLE mice. Our study presents an interesting finding: the serum level of RIPK3 protein was notably elevated in the LN patient subgroup compared to those without LN. Although the serum level of MLKL protein didn’t exhibit a significant difference between these subgroups, it did correlate with urine protein excretion. Central to the pathogenesis of SLE is the breakdown of immune tolerance and the consequent sustained production of autoantibodies. 20 Additionally, a plethora of reports have underscored the relationship between necroptosis in immune cells and the production of autoantibodies. 15 Studies by H Fan demonstrated the overexpression of necroptosis-related genes in B cells from SLE patients as compared to healthy individuals. Furthermore, the co-activation of TLR7 and BCR pathways promoted B cell hyperactivation and eventual necroptosis. Equally relevant, research by David Salem revealed that necroptotic cells augment the antigenic presentation of autoantigen β2-glycoprotein I (β2GPI) to CD4+ T cells by dendritic cells. And mice immunized with β2GPI and deficient in RIPK3 or MLKL exhibited reduced SLE autoantibody production. 21 Our study offers a novel perspective by demonstrating that the serum level of RIPK3, rather than MLKL protein, is significantly heightened in subgroups with positive antibodies, as opposed to those with negative antibodies. This observation diverges from the findings of MJ Zhang et al. 8 We also observed a positive correlation between MLKL and BMI (r = 0.3239, p = 0.0018), suggesting that metabolic status might influence serum MLKL levels. This could limit the specificity of MLKL as a SLE-specific biomarker, and future studies should carefully match for BMI or adjust for it in analyses. Additionally, although we did not find significant associations with individual medications, the possibility of treatment confounding cannot be fully excluded due to the observational design and small numbers in some treatment subgroups. Extracellular HMGB-1 as a primary DAMP was released from dying cell and involved in the pathogenesis of SLE.12,22 Aking to numerous reports, our study exhibits HMGB-1 significantly elevated in SLE patients compared to HC individuals, while our study further displays the level of serum HMGB-1 closely and positively correlated with the level of serum RIPK3/MLKL, which also maybe imply necrosis is mainly forms of lytic cell death in SLE.
Nevertheless, there were some limitations in our study. First, this is a single-center study with a relatively modest sample size, which may limit generalizability and increase the risk of type II error. Independent multi-center validation with larger cohorts is needed. Second, most SLE patients were receiving immunosuppressive treatments at the time of sampling. Although we did not detect significant associations between individual medications and RIPK3/MLKL levels in univariate analyses, confounding by indication and disease severity cannot be ruled out. Our multivariable analyses adjusted for major treatments, but residual confounding may persist. The influence of treatment on circulating necroptosis markers warrants further investigation in longitudinal study. Third, SLEDAI-2K scores were missing for 31 SLE patients, which may introduce bias, although baseline characteristics were comparable between groups. Four, SLEDAI-2K scores were missing for 31 SLE patients, which may introduce bias, although baseline characteristics were comparable between groups. Last, we did not measure the level of RIPK3/MLKL mRNA of peripheral blood mononuclear cells in participants, which could enhance our conclusion. Of note, the high AUC for HMGB-1 (0.9948) was based on a limited sample size and requires confirmation in larger independent cohorts. Furthermore, the added value of RIPK3/MLKL beyond conventional markers (e.g., complement, anti-dsDNA) was not assessed and should be explored in future study.
Conclusion
In summary, our investigation has unveiled the discernible variations in serum levels of RIPK3/MLKL proteins, closely interlinking necroptosis, among patients with stable, active SLE, and healthy controls. These findings offer compelling evidence for the involvement of necroptosis in the pathogenesis of SLE. Moreover, the serum levels of RIPK3/MLKL proteins hold the potential to serve as exploratory biomarker candidates for SLE, which warrant further validation.
Supplemental material
Supplemental material - Serum RIPK3/MLKL as exploratory biomarker candidates for systemic lupus erythematosus
Supplemental material for Serum RIPK3/MLKL as exploratory biomarker candidates for systemic lupus erythematosus by Guowang Zhao, Mingjun Li, Jianghong Lin, Qintong Xiao, Liu Wang, Qi Huang, Man Xiong, Yuanyuan Yang and Xiangming Yi in Lupus
Footnotes
Ethical considerations
This study has been approved by the Ethics Committee of the Yueyang People’s Hospital (No.: 2025015).
Author contributions
Conceptualization: G.Z. and X.Y.; Writing-original draft preparation: G.Z. and M.L.; Methodology M.L. and Q.X.; Resources: L.W., Q.H., M.X. and Y.Y.; Supervision: X.Y.; Revising-review and editing: G.Z. and M.L.; All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.