
Abstract
Background
Systemic lupus erythematosus is a chronic autoimmune disease associated with heightened cardiovascular risk. Data on the impact of systemic lupus erythematosus on outcomes following heart failure hospitalization remain limited. This study aimed to evaluate whether systemic lupus erythematosus is independently associated with 90-days readmission and other clinical outcomes among patients hospitalized with heart failure.
Methods
We conducted a retrospective cohort study using the 2016–2017 Nationwide Readmissions Database to evaluate the association of systemic lupus erythematosus with 90-days readmission after heart failure hospitalization. Adults ≥18 years with an index admission for heart failure were included. The primary outcome was 90-days all-cause readmission. Secondary outcomes included in-hospital mortality, median length of stay, and hospitalization costs. Multivariable Cox proportional hazards were used to identify independent predictors of outcomes.
Results
Among 1,625,731 patients hospitalized with heart failure, 9096 had comorbid systemic lupus erythematosus. Compared with non-systemic lupus erythematosus patients, those with systemic lupus erythematosus were younger (mean age 61 vs 72 years), predominantly female, and more likely to have socioeconomic disadvantage and a higher comorbidity burden. The 90-days readmission rate was significantly higher in the systemic lupus erythematosus cohort (41%) versus the non-systemic lupus erythematosus cohort (34%) (HR: 1.07; 95% CI: 1.02–1.12; p = 0.010). In-hospital mortality did not differ significantly between groups; however, mortality during readmissions was nearly doubled compared with index admissions (5.4% vs 2.9%). SLE patients had a median length of stay of 4 days (vs 4 days in non-SLE) and incurred median hospitalization costs of USD 32,872 (13% higher than non-SLE patients). Independent predictors of readmission included Medicaid insurance, weekend admission, renal failure, myocardial infarction, and discharge to a non-home setting, whereas female sex, treatment at metropolitan teaching hospitals, and comorbid hypertension or diabetes were associated with a lower risk of readmission.
Conclusion
Systemic lupus erythematosus is independently associated with an increased risk of 90-days readmission following heart failure hospitalization, contributing to greater healthcare utilization and costs. These findings highlight the need for tailored strategies for transitional care, multidisciplinary follow-up, and socioeconomic support.
Keywords
Introduction
Heart failure (HF) remains one of the leading causes of hospitalizations and rehospitalizations in the United States (US), with early readmissions contributing significantly to healthcare costs and patient morbidity. Identifying high-risk subgroups is therefore essential for developing targeted strategies to reduce preventable readmissions. Systemic lupus erythematosus (SLE), a chronic autoimmune disease with multi-organ involvement, has emerged as a notable comorbidity in cardiovascular disease, particularly among young and middle-aged women. 1
Globally, HF affects more than 64 million people, with recent estimates placing prevalence at over 37.7 million. 2 In the US, more than 5.7 million individuals live with HF, and nearly 870,000 new cases are diagnosed each year. 3 While incidence rates in high-income countries have plateaued, HF prevalence continues to rise due to population aging and improved survival from ischemic heart disease. Consequently, reducing HF-related hospitalizations and readmissions has become a major public health priority.
Patients with SLE face an increased risk of cardiovascular complications, including accelerated atherosclerosis, myocarditis, pericardial effusion, and HF.2,4 Prior studies have shown that SLE is associated with worse short- and long-term outcomes in HF admissions. For example, an analysis of the National Readmission Database in 2018 demonstrated significantly higher 30-days readmission rates among HF patients with SLE compared to those without SLE. 5 Moreover, HF itself has been identified as an independent predictor of hospital readmission in patients with SLE. 6
Given the chronic inflammatory state and multi-systemic burden of SLE, these patients may remain vulnerable to adverse outcomes well beyond the conventional 30-days post-discharge period. However, the impact of SLE on 90-days readmission risk following HF hospitalization has not been systematically examined.
The objective of this study is to evaluate the association between SLE and 90-days readmission rates among patients discharged after HF hospitalization and to identify key clinical predictors of readmission in this population. By leveraging a nationally representative cohort, we aim to determine whether SLE independently contributes to post-discharge complications beyond traditional cardiovascular risk factors. Findings from this study may highlight important gaps in post-hospital care and inform the development of targeted interventions to optimize outcomes and reduce preventable readmissions in this high-risk group.
Methods
Study design
We conducted a retrospective cohort study to evaluate the association between SLE and 90-days all-cause hospital readmission following an index hospitalization for HF in U.S. adults. Secondary aims included examining differences in patient demographics, clinical characteristics, and hospital features by SLE status, as well as identifying predictors of readmission risk. This study was conducted in accordance with the reporting of studies Conducted using Observational Routinely-collected Data (RECORD) guidelines.
Data source
Data were obtained from the Nationwide Readmissions Database (NRD) for 2016 and 2017, which is part of the Healthcare Cost and Utilization Project (HCUP). The NRD is a nationally representative, all-payer inpatient database containing discharge records from participating states. Each patient is assigned a unique linkage number, allowing readmissions to be tracked within the same calendar year, although cross-year tracking is not possible. The 2017 NRD included approximately 18 million discharges from 28 states, representing about 60% of the U.S. population. The years 2016–2017 were specifically chosen as they represent the most recent period prior to the onset of the COVID-19 pandemic. Post-2019 NRD data are substantially confounded by pandemic-related care avoidance, deferred elective procedures, and altered readmission thresholds. Therefore, pre-pandemic data provide a more clinically stable backdrop and are more appropriate for estimating the inherent biological association between SLE and HF readmission risk.
Ethical considerations
Because the NRD contains de-identified patient information, this study was exempt from institutional review board oversight.
Study population
The cohort included adult patients aged 18 years or older who were hospitalized with a principal diagnosis of HF during the study period. To qualify as an index admission, hospitalizations had to be non-elective and occur before October 1, ensuring a full 90-days follow-up period. Patients were excluded if they were transferred to another acute care facility, if key demographic information (age or sex) was missing, or if mortality data were unavailable. Readmissions within 90 days of discharge were identified using NRD linkage variables, and only the first unplanned readmission was analyzed, with planned readmissions excluded. Patients with SLE were identified using ICD-10-CM diagnosis codes M32.10–M32.19, M32.8, and M32.9, while those with drug-induced lupus (M32.0) were excluded, consistent with prior studies. 7
Outcomes and covariates
The primary outcome was 90-days all-cause readmission after an index HF hospitalization, identified using NRD linkage variables. Secondary outcomes included in-hospital mortality, length of stay (LOS), total hospitalization charges, and non-home discharge following the index admission. Readmissions were defined according to HCUP NRD methodology, with trauma-related readmissions excluded to avoid unrelated admissions. In-hospital mortality was defined as death occurring during either the index hospitalization or a subsequent readmission. LOS was measured as the number of calendar days between admission and discharge, with single-day stays coded as zero. Total hospitalization charges were obtained from the NRD’s TOTCHG variable and adjusted to 2017 U.S. dollars using Consumer Price Index data. Non-home discharge was defined as discharge to any destination other than home or self-care, including transfers to other hospitals, skilled nursing facilities, intermediate facilities, discharge against medical advice, or discharge alive with unknown destination.
Covariates included demographics (age, sex, primary expected payer, median income quartile by ZIP code, and weekend admission), clinical comorbidities, and hospital-level factors. Comorbidities such as diabetes mellitus (DM), hypertension (HTN), renal failure, myocardial infarction (MI), chronic obstructive pulmonary disease (COPD), cardiac arrhythmia, depression, and deficiency anemia were identified using ICD-10 codes. The overall burden of comorbidities was quantified using the Elixhauser and Charlson Comorbidity Index (CCI).8,9 Hospital-level variables included teaching status (metropolitan teaching, metropolitan non-teaching, or non-metropolitan) and hospital bed size (small, medium, or large). The ICD-10 codes used to define all variables are provided in Table 1 of the supplementary material.
Statistical analysis
Baseline characteristics of patients with and without SLE were summarized using survey-weighted means and proportions. Comparisons between groups were conducted using the Rao–Scott chi-square test for categorical variables and the design-based Kruskal–Wallis test for continuous variables. A multivariable, survey-weighted Cox proportional hazards model was then applied to assess the association between SLE and time to 90-days readmission, adjusting for demographic, clinical, hospital-level, and index-stay covariates. Results were reported as hazard ratios (HRs) with 95% confidence intervals (CIs).
A subgroup analysis among patients who experienced 90-days readmission was performed to describe readmission characteristics using survey-weighted methods. All analyses accounted for the NRD’s complex survey design, including weights, strata, and clustering. Statistical analyses were conducted using R version 4.5.0 (R Foundation for Statistical Computing, Vienna, Austria) with the survey and srvyr packages.
Results
Clinical and demographic characteristics
Baseline characteristics of patients evaluated for 90-day readmissions.
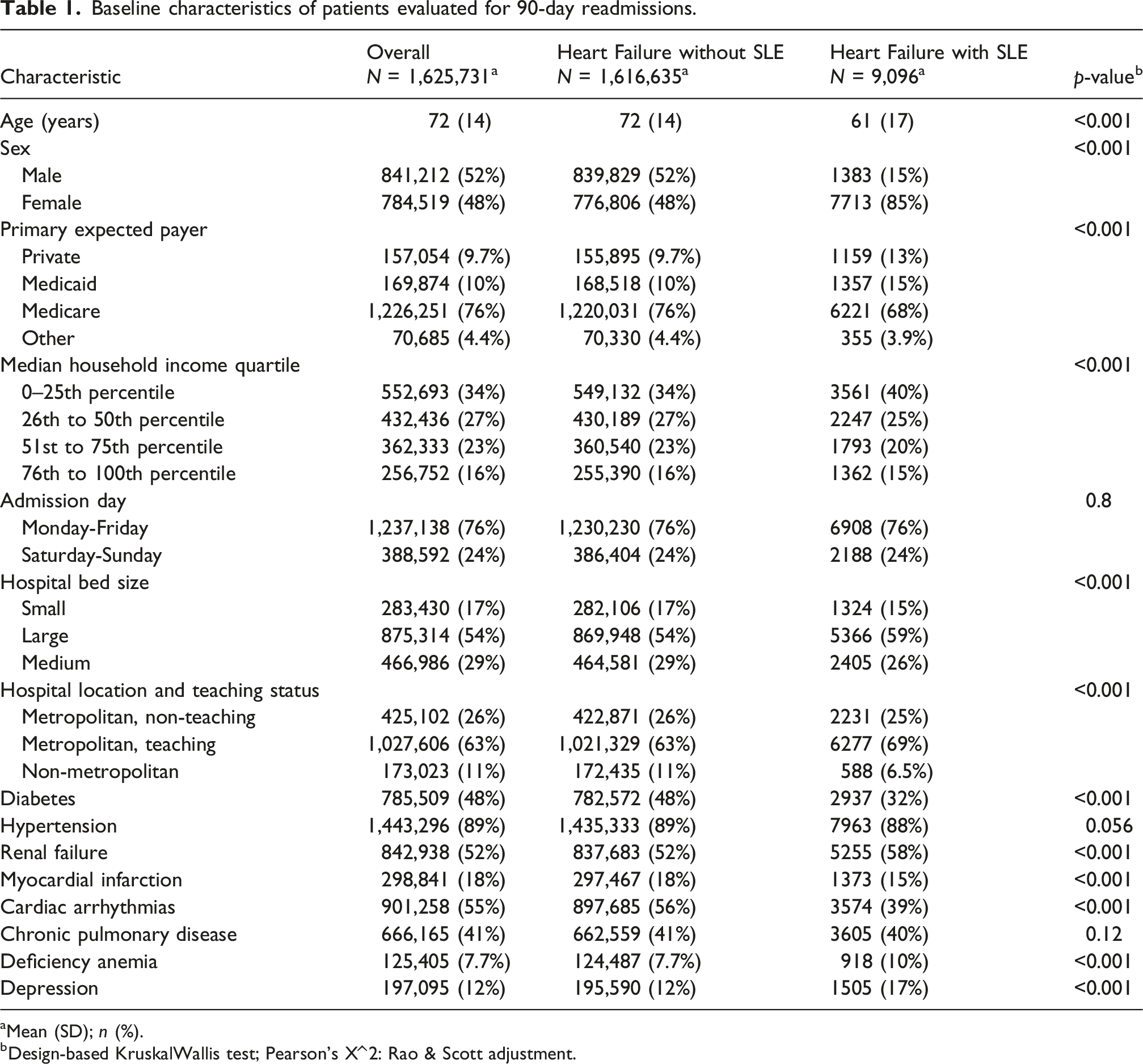
aMean (SD); n (%).
bDesign-based KruskalWallis test; Pearson’s X^2: Rao & Scott adjustment.
Insurance coverage also differed between groups: a higher proportion of patients with SLE were covered by Medicaid (15% vs 10%) or private insurance (13% vs 9.7%) as their primary payer, whereas Medicare was more common among those without SLE (76% vs 68%). Socioeconomic disparities were evident, with 40% of patients with SLE residing in the lowest income quartile compared to 34% of non-SLE patients.
Hospitalization characteristics varied as well. Patients with SLE were more frequently admitted to large hospitals (59% vs 54%) and metropolitan teaching hospitals (69% vs 63%). Comorbid conditions were also more prevalent in the SLE cohort, including renal failure (58% vs 52%), deficiency anemia (10% vs 7.7%), and depression (17% vs 12%). These baseline demographic, socioeconomic, hospital, and clinical characteristics are summarized in Table 1.
Index hospitalization outcomes
During the index hospitalization, the 90-days readmission rate was significantly higher among patients with SLE (41%) compared to those without SLE (34%). In-hospital mortality was slightly higher in the non-SLE group (2.9% vs 2.6%), although this difference did not reach statistical significance (p = 0.078).
Outcomes of index hospitalizations.
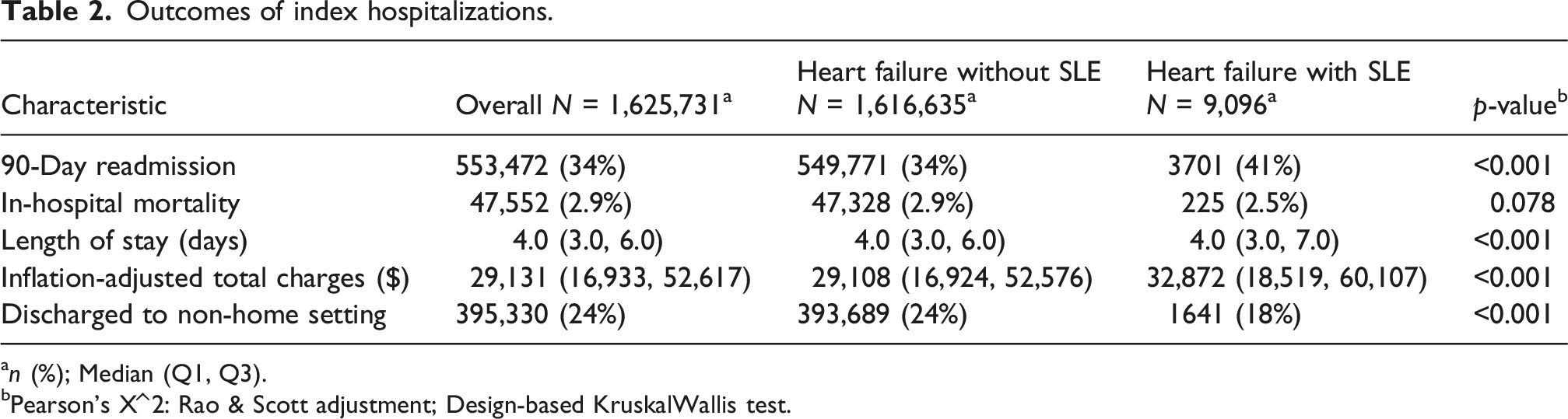
an (%); Median (Q1, Q3).
bPearson’s X^2: Rao & Scott adjustment; Design-based KruskalWallis test.
Readmission outcomes
Multivariable predictors of 90-day readmission.
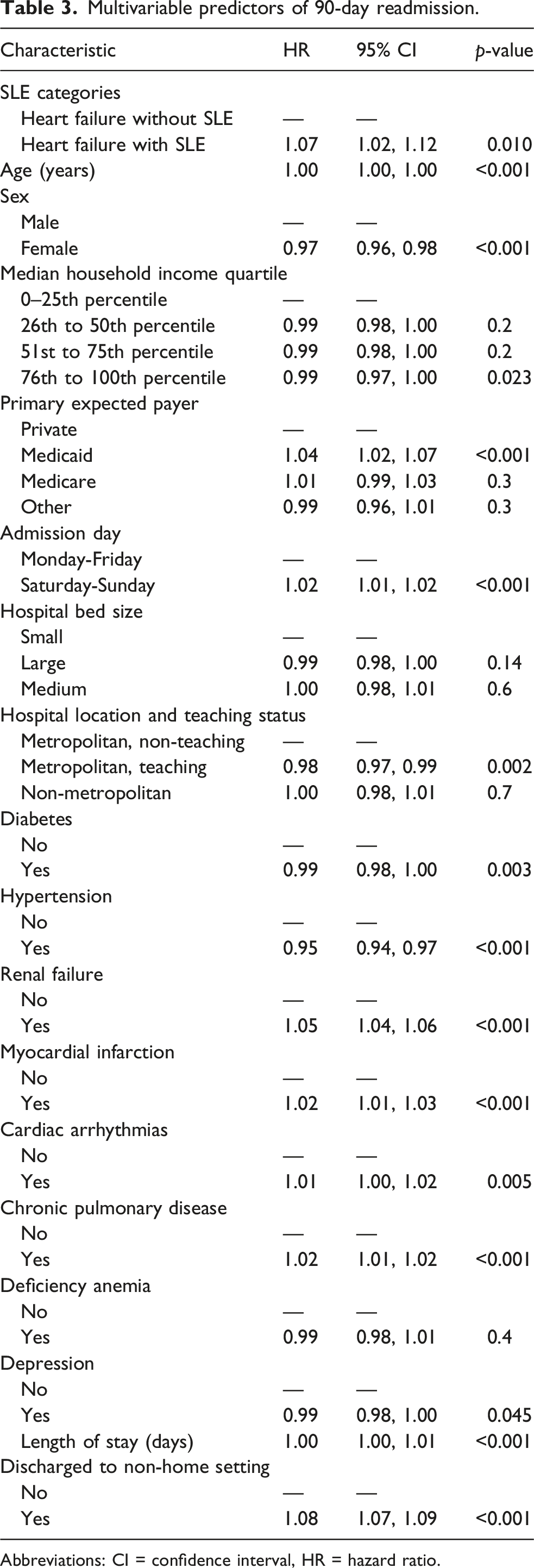
Abbreviations: CI = confidence interval, HR = hazard ratio.
Additional predictors of higher readmission risk included Medicaid insurance (HR: 1.04; 95% CI: 1.02–1.07; p < 0.001), weekend admission (HR: 1.02; 95% CI: 1.01–1.02; p < 0.001), renal failure (HR: 1.05; 95% CI: 1.04–1.06; p < 0.001), myocardial infarction (HR: 1.02; 95% CI: 1.01–1.03; p < 0.001), cardiac arrhythmias (HR: 1.01; 95% CI: 1.00–1.02; p = 0.005), chronic pulmonary disease (HR: 1.02; 95% CI: 1.01–1.02; p < 0.001), and discharge to a non-home setting (HR: 1.08; 95% CI: 1.07–1.09; p < 0.001). Weekend admissions (Saturday–Sunday) were associated with a modestly higher risk of 90-days readmission compared with weekday admissions (HR: 1.02; 95% CI: 1.01–1.02; p < 0.001).
In contrast, female sex (HR: 0.97; 95% CI: 0.96–0.98; p < 0.001), treatment at metropolitan teaching hospitals (HR: 0.98; 95% CI: 0.97–0.99; p = 0.002), hypertension (HR: 0.95; 95% CI: 0.94–0.97; p < 0.001), and diabetes (HR: 0.99; 95% CI: 0.98–1.00; p = 0.003) were associated with a lower risk of readmission. Patients residing in the highest income quartile (76th to 100th percentile) also had a slightly reduced risk of readmission compared to those in the lowest quartile (HR: 0.99; 95% CI: 0.97–1.00; p = 0.023). Although the hazard ratio for age was 1.00, the association was statistically significant (p < 0.001), indicating that each additional year of age contributed a small but consistent increase in readmission risk.
To determine whether readmissions in the SLE cohort were driven primarily by cardiac decompensation or other complications, we conducted an analysis of the top 10 principal diagnoses at the 90-days readmission stage. This analysis was restricted exclusively to the heart failure patients with SLE (n = 3701 90-days readmissions). The weighted counts and standard errors for each diagnosis are detailed in Figure 1 of the supplementary material.
Discussion
In this large, nationally representative cohort of patients hospitalized with HF, we found that comorbid SLE was independently associated with a higher risk of 90-days readmission. Although in-hospital mortality did not differ between groups, SLE patients incurred greater healthcare utilization, as evidenced by higher readmission rates and hospitalization costs, despite similar LOS. These findings underscore the disproportionate burden of SLE in the context of HF and highlight important clinical and policy implications.
Our results build on prior literature demonstrating that SLE is associated with adverse cardiovascular outcomes and an increased risk of hospitalization. The elevated cardiovascular risk in SLE is likely multifactorial, reflecting chronic systemic inflammation, autoantibody activity (e.g., antiphospholipid antibodies), abnormal platelet activation, complement-mediated endothelial injury, and dysregulated lipid metabolism.10–13 In addition, common therapies such as glucocorticoids and hydroxychloroquine may worsen cardiometabolic risk through effects on glucose regulation, adiposity, and lipid profiles, further complicating outcomes. 14 Together, these biological and treatment-related mechanisms provide a plausible explanation for the increased risk of readmission observed in our SLE-HF population.
Demographic differences may also contribute. Prior studies have shown that SLE-related HF often develops at a younger age, with early onset reported in up to 50–60% of pediatric and young adult patients and in nearly one-third of adults under 45 years. 15 Population data from Europe similarly suggest earlier onset in women (ages 30–50) compared with men (ages 50–70).16,17 Consistent with these reports, our cohort showed that HF patients with SLE were younger and predominantly female.
We also observed that in-hospital mortality was almost doubled during readmissions compared with index HF admissions (5.4% vs 2.9%), suggesting that recurrent hospitalizations represent a more vulnerable and advanced stage of HF. Prior observational studies from the United States and Canada have identified recurrent hospitalizations as strong predictors of mortality,18,19 and analyses from the CHARM trial similarly showed that a prior history of HF admission portends higher cardiovascular mortality and recurrent HF events. 20 In the context of SLE, this risk may be further amplified. 21 Strategies aimed at preventing the first readmission such as early post-discharge follow-up, structured transitional care, and home health support have been shown to improve outcomes in high-risk HF populations. 22 Our findings suggest that implementing such interventions specifically in SLE-HF patients could meaningfully reduce mortality and resource use.
We also found that SLE patients incurred 13% higher hospitalization costs than non-SLE patients, despite similar LOS (median: 4 days). This likely reflects greater complexity of care, including additional diagnostic evaluations and more intensive medication requirements. Prior work has similarly linked higher SLE disease activity with increased healthcare costs. 23
Our analysis identified several independent predictors of readmission, including Medicaid insurance, weekend admission, renal failure, myocardial infarction, and discharge to a non-home setting. Patients with Medicaid coverage had higher readmission risks, likely reflecting socioeconomic vulnerability such as reduced access to medications, limited follow-up, and lower continuity of care. 24 This was reinforced by our finding that residence in the highest income quartile was modestly protective against readmission. Weekend admissions were also associated with slightly elevated risk, consistent with the “weekend effect,” in which reduced staffing and resource availability may delay treatment or discharge planning. 25 Discharge to a non-home setting emerged as one of the strongest predictors of readmission, consistent with prior work linking such discharges to worse outcomes due to greater frailty and fragmented continuity of care. 26 For patients with SLE, who often require coordinated subspecialty follow-up, transitions to post-acute facilities without structured care may further heighten the risk of rehospitalization.
Interestingly, female sex, treatment in metropolitan teaching hospitals, and comorbid hypertension and diabetes mellitus were each associated with a modest reduction in readmission risk. Female patients may experience lower readmission risk due to stronger adherence and health-seeking behaviors. 27 Metropolitan teaching hospitals likely achieve better outcomes due to access to multidisciplinary expertise, advanced diagnostics, and high-volume care. 28 The lower readmission risk associated with hypertension and diabetes should not be interpreted as a biological protective effect. Rather, this paradoxical finding is a statistical artifact—specifically, index event bias (or collider bias)—which occurs because our cohort is restricted exclusively to patients who have already experienced the index event of a heart failure hospitalization. Taken together, our findings have important clinical implications. HF patients with SLE represent a high-risk subgroup that may benefit from enhanced transitional care, multidisciplinary management involving rheumatology and cardiology, and structured post-discharge follow-up. Interventions such as early clinic visits, care coordination, and optimization of comorbid conditions could reduce preventable readmissions in this population. From a policy perspective, addressing socioeconomic barriers, expanding access to outpatient care, and strengthening continuity across care settings may help mitigate disparities and improve outcomes in this vulnerable group.
Limitations
This study has many important limitations. First, considering that the NRD is an observational, administrative database, our results show associations instead of proving causation. Notably, NRD lacks critical clinical markers such as Left Ventricular Ejection Fraction (LVEF), BNP/NT-proBNP levels, and baseline medications (e.g., steroids or hydroxychloroquine). Without LVEF, we are unable to distinguish between heart failure phenotypes. This is particularly relevant in SLE populations, where Heart Failure with Preserved Ejection Fraction (HFpEF) may predominate. Second, the NRD only includes event data during the time of hospitalization, which is why we cannot look at deaths outside the hospital or details about post-discharge follow-up, like clinic or specialist visits, which may influence readmission risk after index hospitalization. This database also excludes non-community hospitals, such as Long-Term Acute Care (LTAC) and rehabilitation facilities; SLE patients, who are often younger but more frail and comorbid, frequently require these settings following a complex heart failure hospitalization, readmissions to these facilities are not captured. Consequently, our study likely underestimates the true rate of 90-days healthcare utilization and complications.
Third, our identification of HF, SLE, and comorbidities relied on ICD-10 codes. While a single inpatient code has good specificity and prediction value, the sensitivity is lower, which means that some cases may have been missed. Such inaccuracy typically shifts results toward the null, meaning the reported estimates may be lower than the true values. Future analyses in datasets that require two or more SLE codes, as is common in outpatient research, could improve the accuracy. Regarding our definition of baseline renal failure, we deliberately excluded the primary ICD-10-CM code for acute kidney injury (N17. x) to capture established chronic disease rather than acute in-hospital events. However, we acknowledge that the code for unspecified kidney failure (N19. x) remains in our definition. This carries residual ambiguity, as it may capture a small subset of acute-onset renal failure which could act as a mediator rather than a true baseline confounder.
Fourth, the NRD does not track patients across state lines or between calendar years, which may underestimate readmissions, especially for those admitted in a different state or after year-end. It also represents about 60% of the U.S. population, compared with over 97% for the National Inpatient Sample, so generalizability may be limited.
Fifth, although changes in coding systems and the addition of new states over time could affect the absolute number of heart failure hospitalizations, these shifts are unlikely to meaningfully change proportional readmission estimates because calculations are based on index admissions followed within the same year.
Finally, because NRD only records in-hospital deaths, we could not assess total mortality, which is a key outcome for patients with HF, particularly those with SLE who may remain at high risk after discharge. Future studies linking inpatient, outpatient, and mortality data could give us a more complete picture of long-term outcomes in our population.
Furthermore, in heart failure populations, death acts as a competing risk that precludes the possibility of readmission. Our use of a cause-specific Cox proportional hazards model treats death as a censoring event, which assumes non-informative censoring. We acknowledge that this approach may not fully account for competing risks; censoring may disproportionately remove higher-risk patients and potentially lead to an underestimation of the readmission risk. Future studies utilizing alternative approaches, such as the Fine-Gray subdistribution hazard model, could provide complementary estimates of cumulative incidence.
Conclusion
The goal of this study was to assess the impact of SLE on 90-days readmission rates in heart failure patients. The results demonstrate that SLE was an independent risk factor for increased readmission risk for HF patients. The SLE cohort had younger ages, was mostly female, socioeconomically disadvantaged, had a higher burden of comorbidities, and increased readmission rates. More importantly, patients with SLE exhibited a significantly higher 90-days readmission rate (41%) compared to those without SLE (34%) after index hospitalization for heart failure, with multivariate analysis confirming SLE’s independent association with this elevated risk (HR: 1.07; 95% CI: 1.02–1.12; p = 0.010). These findings highlight the need for tailored and intensive follow-up management to improve clinical outcomes of discharged HF patients with SLE. Efforts should be made to develop and implement strategies to decrease unnecessary readmissions in this population by managing their complex and multifaceted healthcare needs.
Supplemental material
Supplemental material - Association of systemic lupus erythematosus with 90-day readmission following heart failure hospitalization: A national readmission database (NRD) analysis, 2016–2017
Supplemental material for Association of systemic lupus erythematosus with 90-day readmission following heart failure hospitalization: A national readmission database (NRD) analysis, 2016–2017 by Farheen Malik, Muhammad Saad, Minahil Javaid, Fatima Gul, Meerub Fatima Zafar, Rai Muhammad Umar Khan, Syed Nosherwan Ali, Rija Tahir, Ishba Manal, Saba Fatima, Sunny Kumar, Komal Saleem, Komal Kumari and Jawad Ahmed in Lupus
Footnotes
Acknowledgments
The authors acknowledge the Agency for Healthcare Research and Quality (AHRQ) and the HCUP State Partners for providing the NRD used in this study.
Consent to participate
Informed consent was not required, as the study utilized de-identified, publicly available data from the National Readmission Database.
Author contributions
Conceptualization: Jawad Ahmed, Minahil Javaid; Formal Analysis, Data Curation: Muhammad Saad, Jawad Ahmed; Methodology: Minahil Javaid, Jawad Ahmed, Muhammad Saad, Fatima Gul; Validation: Komal Kumari, Komal Saleem, Sunny Kumar; Writing – Original Draft: Saba Fatima, Ishba Manal, Rija Tahir, Syed Nosherwan Ali, Rai Muhammad Umar Khan, Meerub Fatima Zafar; Writing – Review & Editing: Jawad Ahmed, Muhammad Saad, Minahil Javaid; Supervision: Jawad Ahmed, Muhammad Saad.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.