
Abstract
Objective
This study aimed to investigate belimumab continuation and identify clinical parameters predicting belimumab continuation in patients with systemic lupus erythematosus (SLE) in a real-world setting.
Methods
A total of 38 consecutive patients with SLE who were newly treated with belimumab at our institution from 2018 to 2024 were retrospectively analyzed. The data were censored when belimumab was discontinued or the observation period ended. Clinical and laboratory data were retrospectively collected.
Results
The median follow-up time after starting belimumab was 37 months (IQR 12–52). The 1-year belimumab continuation rate was 29/38 (76%). During the entire observation period, 15 (39%) patients discontinued belimumab. Among the 10 patients who discontinued belimumab due to lack of efficacy, seven were switched to other biologics. The overall discontinuation rate was 13.4 per 100 person-years. Absence of serological activity (increased anti-dsDNA and/or hypocomplementemia) at baseline was a significant risk factor for belimumab discontinuation within 1 year (p = 0.034), with a relative risk of 3.43 (95% CI, 1.01–11.6). The glucocorticoid dosage was significantly reduced in the 29 patients treated with belimumab for ≥12 months (p < 0.001). Among the 33 patients who were not in the low disease activity state (LLDAS) at baseline, 19 (58%) were in the LLDAS at their final visit (p < 0.001). Belimumab was temporarily discontinued in six patients due to infection, but all patients resumed it.
Conclusion
The belimumab continuation rate was high among patients with SLE in real-world settings; however, the absence of serological activity at belimumab initiation was a significant risk factor for discontinuation within 1 year.
Introduction
Systemic lupus erythematosus (SLE) is a multisystemic autoimmune disease characterized by chronic inflammation of classic target organs such as the skin, joints, and kidneys. 1 Despite substantial advances in SLE diagnosis and management, the disease burden remains high. Add-on treatment with conventional and/or biological immunosuppressive therapies, including belimumab, is usually recommended for patients with SLE who do not respond to combinations of hydroxychloroquine and glucocorticoids (GCs). However, the best use of belimumab remains to be elucidated, and the situation has become more complicated since the approval of anifrolumab for the treatment of extrarenal SLE (in Japan in 2021).
Drug continuation is a comprehensive outcome that encompasses effectiveness, safety, and patient and physician preferences 2 . Drug continuation rates reflect both efficacy and safety and may be influenced by the availability of alternative treatment options. 3 It is particularly suitable for chronic diseases, such as SLE, requiring long-term treatment. However, reports on drug continuation in SLE are limited. This study aimed to investigate belimumab continuation and identify clinical parameters predicting belimumab continuation in patients with SLE in a real-world setting.
Methods
Study population
Clinical data from all consecutive adult (≥18 years old) patients with SLE who were newly treated with belimumab in our hospital from 2018 to 2024 were retrospectively analyzed. SLE was diagnosed according to the 2019 European Alliance of Associations for Rheumatology/American College of Rheumatology classification criteria for SLE. 4 Patients initiated on belimumab within 1 year of data collection were excluded. The observation period began on the first day of belimumab administration. The data were censored when belimumab was discontinued or the observation period ended (December 2024). This study was approved by the ethics committee of Tokyo Women’s Medical University (registration numbers 4086 and 2023-0206) and was conducted in accordance with the principles of the Declaration of Helsinki.
Data collection
Clinical and laboratory data on the following occasions were retrospectively collected: upon initiation of belimumab, at 3, 6, and 12 months after initiation, and annually until the last visit. Clinical, radiological, and laboratory data and information on adverse events were collected from the electronic medical records. Serious adverse event was defined as an adverse event that resulted in death, was life-threatening, required hospitalization or prolongation of existing hospitalization, resulted in persistent or significant disability or incapacity, or was a birth defect. Treating physicians assessed disease activity and damage using the SLE Disease Activity Index 2000 (SLEDAI-2K), 5 and Physician Global Assessment (PGA). 6 Attainment of the Lupus low disease activity state (LLDAS) 7 and the definition of remission in SLE (DORIS) 8 were evaluated on a per-visit basis. LLDAS was defined using the definition published by Golder et al. 7 as meeting all of the following conditions: SLEDAI-2K ≤4, excluding major organ activity; absence of new SLEDAI-2K activity compared with the preceding visit; PGA score of ≤1 (scale 0–3); and daily prednisolone dose of ≤7.5 mg, with the use of antimalarials and immunosuppressants permitted. DORIS was defined as meeting all of the following conditions: clinical SLEDAI = 0; PGA score of <0.5 (scale 0–3); and daily prednisolone dose of ≤5 mg, with the use of stable antimalarials, immunosuppressants, and biologics permitted. 8
Treatment
Belimumab was administered at the discretion of the treating physician. Other treatments, including tapers for GCs, were also decided by the treating physicians. All patients received COVID-19 vaccination during the pandemic.
Outcomes
The primary outcome was the 1-year drug continuation rate for belimumab. The secondary outcomes included the overall discontinuation rate of belimumab, reduction in the dosage of prednisolone (PSL)-equivalent GC, attainment of LLDAS and DORIS, and adverse events.
Statistical analyses
Missing data were handled using available-case analysis; each analysis was based on subjects with available data for the included variables. Continuous variables are presented as median (range or interquartile range [IQR]), whereas categorical variables are expressed as counts and proportions (%). For categorical variables, two-group comparisons were performed using the chi-square test. Time-to-event analyses were performed using Kaplan–Meier analysis with the log-rank test. The Wilcoxon signed-rank test was used to compare the glucocorticoid dosages at baseline and 12 months after treatment. Two-sided p-values of <0.05 were considered statistically significant. No correction for multiple comparisons was made, and p-values were interpreted as exploratory results, except for the primary outcome: the 1-year continuation rate for belimumab. Owing to the limited sample size, the comparisons were performed using only univariate analyses. Statistical analyses were performed using Microsoft Excel (version 2021; Microsoft, Redmond, WA, USA) and JMP Pro statistical software (version 17.0.0; SAS Institute, Cary, NC).
Results
Clinical characteristics of patients with SLE
Baseline characteristics of patients with systemic lupus erythematosus who had been treated with belimumab (n = 38).
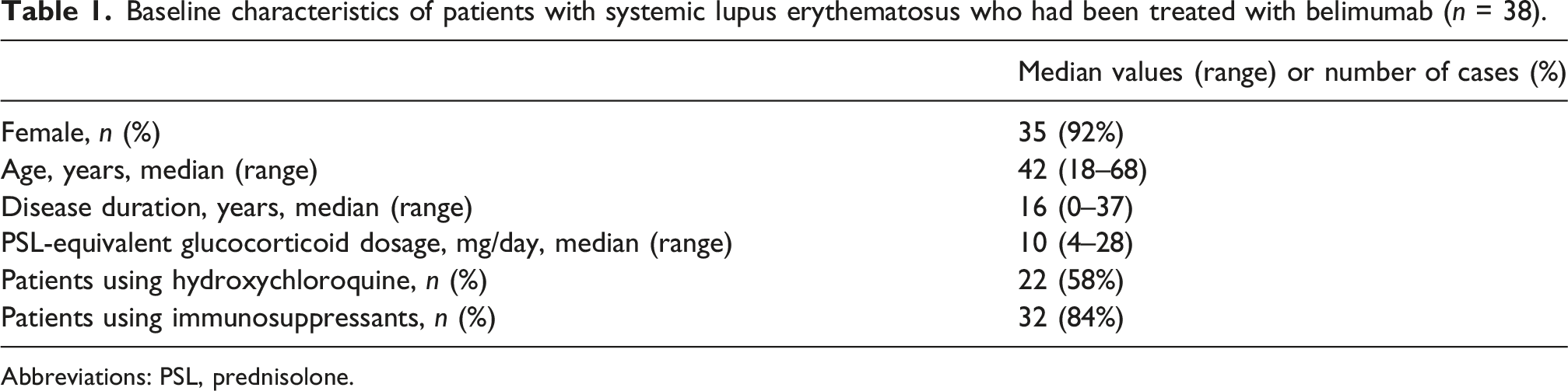
Abbreviations: PSL, prednisolone.
Belimumab continuation/discontinuation
The 1-year continuation rate for belimumab was 29/38 (76%). During the entire observation period, 15 (39%) patients discontinued belimumab, and 4 discontinued the drug after only one infusion. The reasons for discontinuation were as follows: lack of efficacy in 10, patient preference in 4, and pregnancy in 1. Among the 10 patients who discontinued belimumab because of its lack of efficacy, seven patients were switched to other biologics, including anifrolumab (n = 5). The overall discontinuation rate was 13.4 per 100 person-years.
Risk factor for belimumab discontinuation
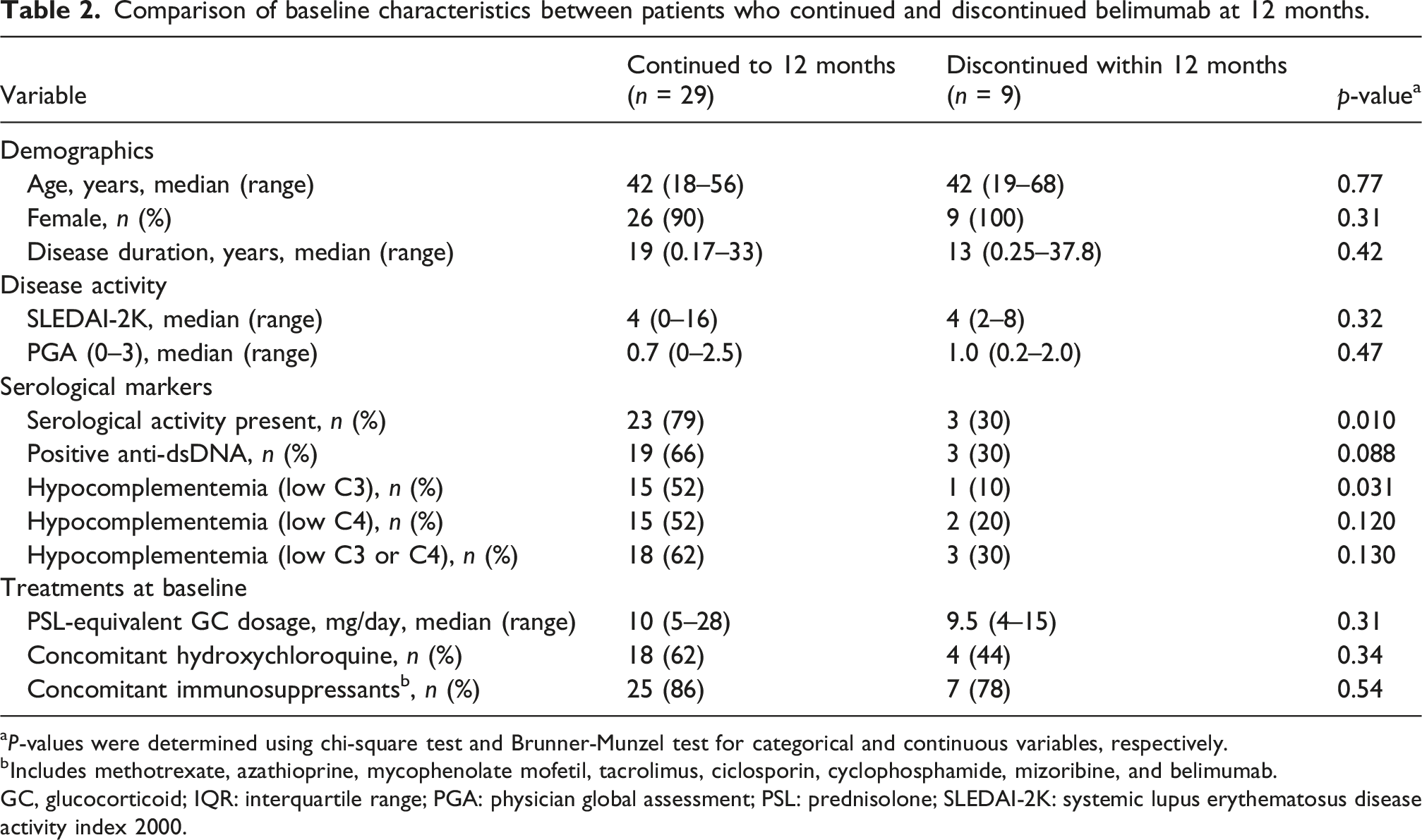
Absence of serological activity (increased anti-dsDNA and/or hypocomplementemia) at baseline was a significant risk factor for belimumab discontinuation within 1 year (p = 0.034), with a relative risk of 3.43 (95% CI, 1.01 to 11.6). When serological activity was broken down, positivity for serum anti-dsDNA antibodies and a decrease in baseline serum C3 levels were each significantly associated with 1-year belimumab continuation (p = 0.045 and 0.021, respectively). As shown in Figure 1, the time-to-event analysis also indicated that baseline serological activity was significantly associated with 1-year belimumab continuation (p = 0.022 by the log-rank test). The following factors were not significantly associated with 1-year drug continuation for belimumab (p > 0.05 in all assessments): baseline SLEDAI-2K, PGA, PSL-equivalent GC dosage, and concomitant use of immunosuppressants or hydroxychloroquine; attainment of LLDAS at 3 or 6 months; decrease in SLEDAI-2K scores, serum anti-dsDNA antibody titers, and PSL-equivalent GC dosages at 3 or 6 months; and increase in serum C3 or C4 levels at 3 or 6 months. Baseline characteristics between patients who continued belimumab for at least 12 months and those who discontinued it earlier are shown in Table 2. Continuation rates of belimumab with or without baseline serological activity within 1 year in patients with systemic lupus erythematosus. Kaplan–Meier plot of time to belimumab cessation from any cause. The p-value was determined using the log-rank test. Comparison of baseline characteristics between patients who continued and discontinued belimumab at 12 months. aP-values were determined using chi-square test and Brunner-Munzel test for categorical and continuous variables, respectively. bIncludes methotrexate, azathioprine, mycophenolate mofetil, tacrolimus, ciclosporin, cyclophosphamide, mizoribine, and belimumab. GC, glucocorticoid; IQR: interquartile range; PGA: physician global assessment; PSL: prednisolone; SLEDAI-2K: systemic lupus erythematosus disease activity index 2000.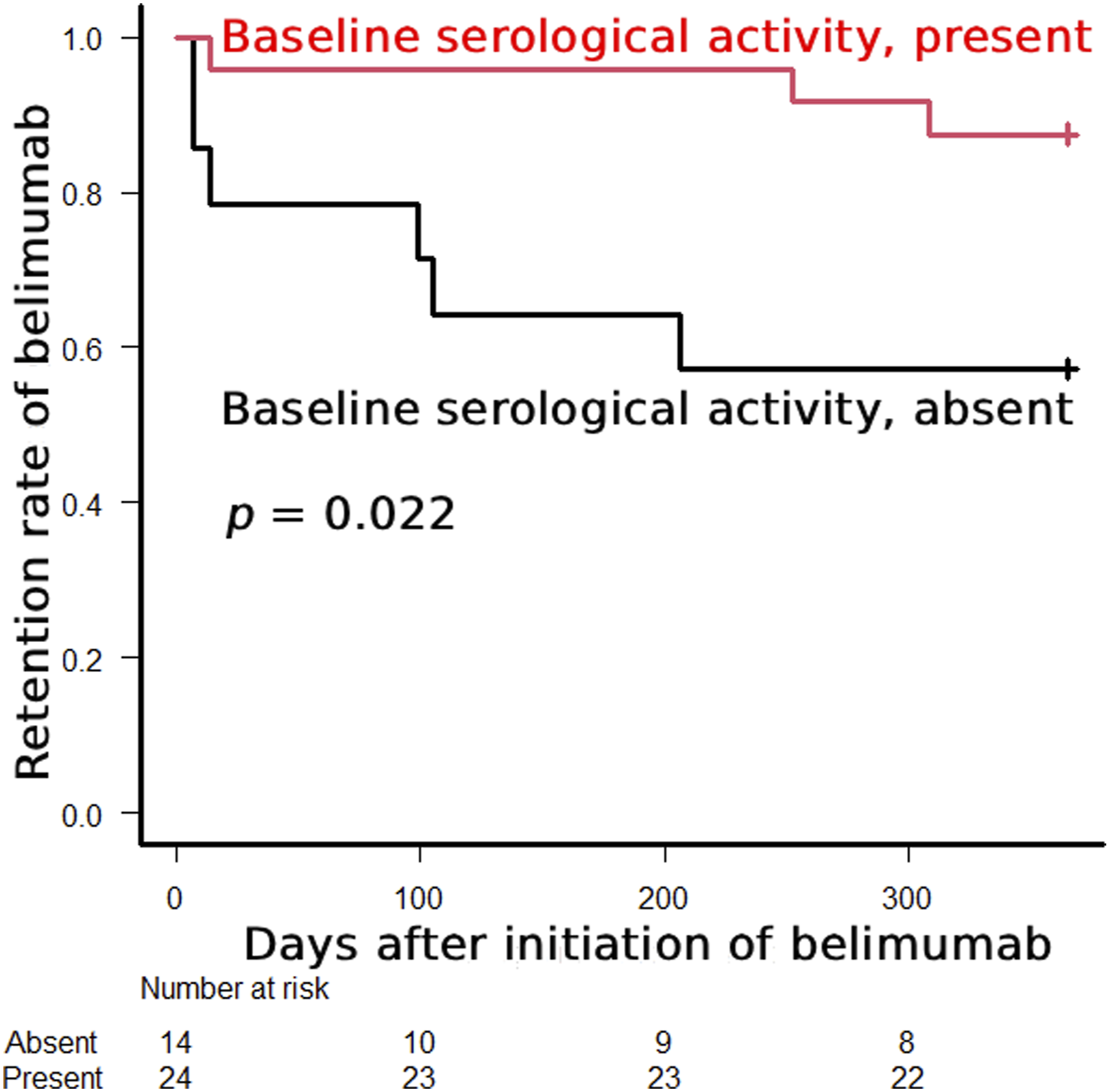
GC dosage
As shown in Figure 2(a), the GC dosage was significantly reduced among the 29 patients treated with belimumab for ≥12 months (p < 0.001). The PSL-equivalent GC dosage was reduced in 19 (66%) patients, with a median reduction of 3.0 mg at 1 year after the initiation of belimumab. Temporal changes in GC dosages among patients who continued and discontinued belimumab within 1 year are shown in Figure 2(b). (a) Temporal changes in GC dosages among patients with systemic lupus erythematosus who had been treated with belimumab ≥12 months (n = 29). GC dosages at baseline and 12 months were compared using the Wilcoxon signed-rank test. (b) Box plots of GC dosages among patients who continued (dark gray) and discontinued (light gray) belimumab within 1 year. GC, glucocorticoid; PSL, prednisolone.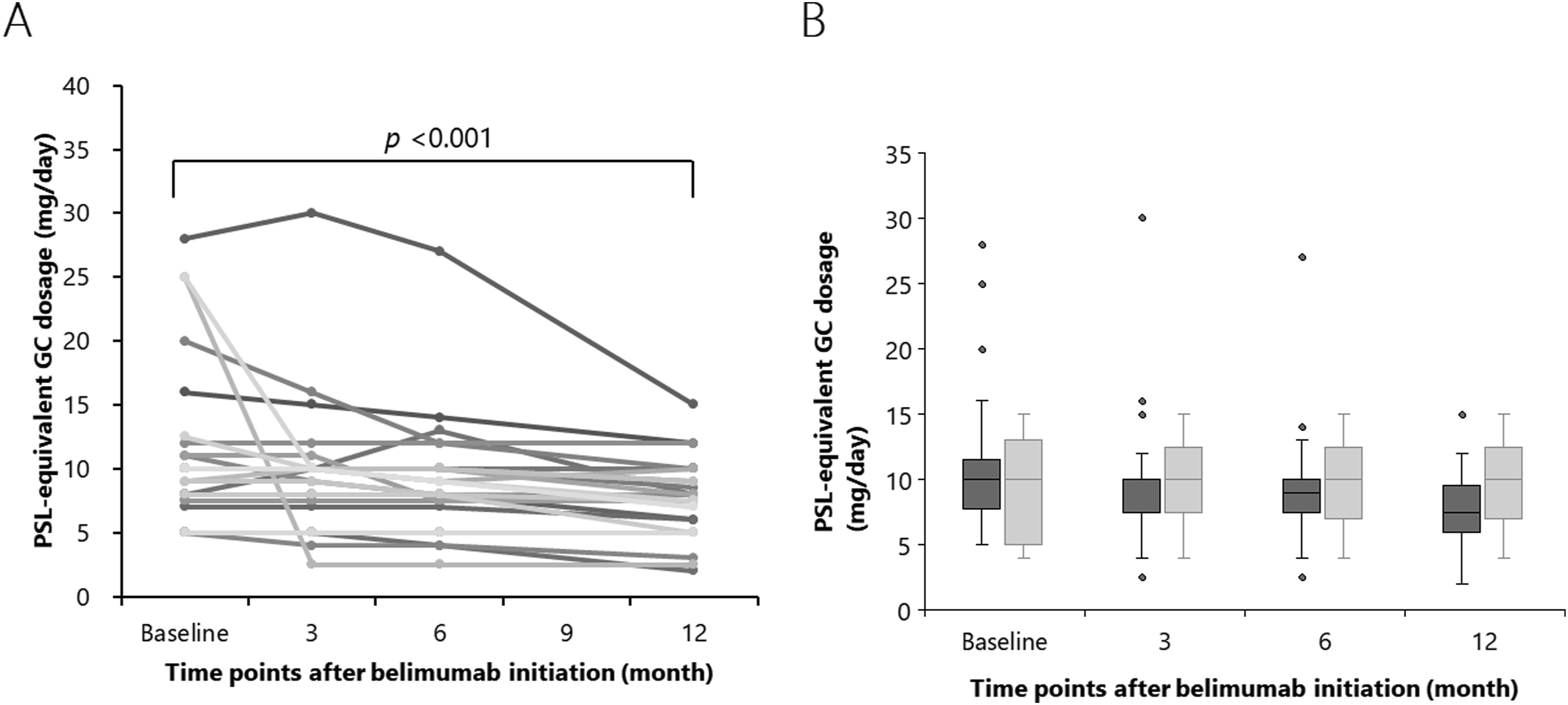
Attainment of LLDAS and DORIS
Among the 33 patients who were not in LLDAS at baseline, 19 (58%) were in LLDAS at their final visit (p < 0.001). 9 and 11 patients newly attained LLDAS at 12 months and thereafter, respectively: one patient, who attained LLDAS at 12 months, was not in LLDAS at her last visit. Five patients attained LLDAS at baseline but did not attain DORIS. Belimumab was initiated to ameliorate residual minor disease activity and/or reduce glucocorticoid dosages in these five patients. Although no patient was in DORIS at baseline, 12 patients were in DORIS at their final visit.
Adverse events
Belimumab was temporarily discontinued in six patients due to infection: herpes zoster in 4 and other infections in 2; however, all were restarted on belimumab and continued until the last visit. No other serious adverse events or adverse events resulting in the permanent discontinuation of belimumab were observed.
Discussion
This study demonstrated that the belimumab continuation rate was high in patients with SLE in real-world settings. Similarly, an integrated analysis of 11 prospective Italian cohorts reported a 1-year belimumab continuation rate of 76.9% in the clinical practice setting. 9 Another Italian multicenter, retrospective cohort study reported a 1-year belimumab continuation rate of 85.2%. 10 A prospective observational study from three centers in Greece reported a 1-year belimumab continuation rate of approximately 70% (estimated on a graph: the precise percentage was not mentioned in the article). 11 The studies from the LOOPS registry reported 1-year belimumab continuation rates of 90%–99% in real-world settings; however, the study subjects were selected based on some criteria, such as “patients with biopsy-proven lupus nephritis 12 ” and “patients with SLE during maintenance therapy 13 ”.
This study showed that the absence of serological activity at belimumab initiation was a significant risk factor for discontinuation within 1 year. While our finding that the absence of baseline serological activity predicts earlier discontinuation is based on a limited cohort, it is highly consistent with the cumulative evidence from post hoc analyses of randomized controlled trials robustly supports the conclusion that baseline serological activity is associated with enhanced belimumab efficacy in SLE.14–16 In addition, in a post hoc analysis of randomized controlled trials, treatment differences between belimumab and placebo were numerically greater in the baseline serum B-cell activating factor (BAFF) levels ≥2 ng/mL group than in the baseline serum BAFF levels <2 ng/mL group, and high anti-dsDNA and low complement levels were associated with baseline serum BAFF levels ≥2 ng/mL 17 . In contrast, reports on serological activity as a predictor of belimumab continuation in SLE in real-world settings are limited. Inconsistent with our findings, a Greek study reported that only baseline PGA and early PGA improvement were significantly associated with belimumab efficacy-related continuation. 11
This study has several limitations. First, the small sample size of 38 patients is a major limitation of this study. This small cohort size limits the statistical power to perform multivariate analyses and may affect the generalizability of our findings regarding serological activity as a predictor of drug continuation. Consequently, our results should be interpreted as exploratory and as a prompt for larger, multi-center longitudinal studies to confirm these associations in the Japanese population such as the MOONLIGHT (post-Marketed effectiveness of belimumab cOhOrt and JapaN Lupus NatIonwide ReGistry coHorT) study. 18 Second, the study’s reliance on an uncontrolled design and retrospective data, with a limited number of study subjects, raises concerns about potential confounding factors and selection biases that may influence the reported outcomes, warranting cautious interpretation of the results and the conclusions drawn. Nevertheless, all consecutive previously untreated patients hospitalized at our hospital during the study period were included in the analyses, and all data were collected on time as per routine clinical practice. Third, treatment was decided and arranged by attending physicians, although a general treatment strategy based on recent clinical guidelines had been shared in our division. Fourth, selection bias may exist because the participants were followed up at a university hospital, although patients with SLE are usually seen at university or tertiary hospitals in Japan. Fifth, hydroxychloroquine was first approved in Japan in 2015; thus, it was newly administered to only a limited number of patients. Sixth, subcutaneous (SC) belimumab has been available in Japan since 2017. In our cohort, 11 patients received intravenous (IV) belimumab, and 7 of these patients had IV switched to SC. Because only four patients were treated solely with IV therapy, subanalyses by mode of administration could not be performed. Finally, because the subjects of this study were of Japanese ethnicity only and conducted in Japan, the generalizability of the results must be confirmed in patients with different ethnic backgrounds and those from other countries.
In conclusion, this study showed that the belimumab continuation rate was high among patients with SLE in real-world settings, although the absence of serological activity at belimumab initiation was a significant risk factor for discontinuation within 1 year. Belimumab was well-tolerated and exhibited a glucocorticoid-sparing effect. Some studies, particularly in real-world settings, have found no significant association between baseline serological activity and clinical response or drug continuation, underscoring the need to consider serological activity alongside overall disease activity and other clinical factors. Further longitudinal studies are needed to elucidate belimumab drug continuation in patients with SLE in real-world settings.
Footnotes
Acknowledgments
We thank all the physicians who treated the enrolled patients for their engagement in data collection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JSPS KAKENHI [grant numbers JP20K08783, JP20K08810, JP23K07911, JP24K11395].
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: YK received honoraria from Asahi Kasei Pharma, Astellas Pharma Inc., AstraZeneca K.K., Chugai Pharmaceutical Co., Ltd., GlaxoSmithKline K.K., Janssen Pharmaceutical K.K., Mitsubishi Tanabe Pharma Corporation, Pfizer Japan Inc., Sanofi K.K. NH and YO declare no conflicts of interest.